")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 18
Hyaluronic Acid Combined with Diluted and Hyperdiluted Calcium Hydroxylapatite to Treat the Periocular Area
Authors Spada J, Van Loghem J
Received 20 January 2025
Accepted for publication 18 June 2025
Published 17 July 2025 Volume 2025:18 Pages 1741—1752
DOI https://doi.org/10.2147/CCID.S518475
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Monica K. Li
Julieta Spada,1 Jani Van Loghem2
1Spada. Dermatología y Estética, Buenos Aires, Argentina; 2Uma Clinic, Amsterdam, Netherlands
Correspondence: Julieta Spada, Spada. Dermatología y Estética, Echeverria 1515, 4B, C1428DQS, Ciudad Autónoma de Buenos Aires, Argentina, Email [email protected]
Purpose: A combination of fillers and other modalities is often required to address all signs of periorbital aging. Patients are injected for volume loss, and for hyperpigmentation are treated with a combination treatments with chemical peels and lasers, but multiple visits can be burdensome. To streamline the current treatment approach for the periocular area, the current study investigated the benefit of the treatment with a blend of Hyaluronic Acid (HA) and Calcium Hydroxylapatite (CaHA). This dual-filler strategy is designed to utilize the rheological and volume replacement capabilities of HA alongside the bioregenerative effects of CaHA while avoiding excessive edema and/or delayed swelling that may occur when HA is injected alone.
Methods: One hundred and six adults were treated with a blend of crosslinked HA (22.5 mg/mL) and diluted/hyperdiluted CaHA. The filler ratio was chosen based on individual skin thickness and depth of palpebro-malar groove (PG) or supraorbital hollowness (SH). Assessments were performed at baseline (T0), 30, 60, 90, and 365 days. One patient underwent a comparative analysis of HA alone versus the HA-CaHA blend, evaluated through ultrasound, Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) scan post-injection.
Results: All treated patients presented natural-looking results, less pronounced PG and SH with minimal edema on D30, and skin quality improvement with less laxity, wrinkling and pigmentation. No hyaluronidase injections for overcorrections were required. No severe complications were observed. For most patients, results varied according to the dilution of the blend; lower dilutions (1:1) lasted longer than higher dilution (1:4), even though results were still noticeable for patients treated with the latter (1:4) at the 1-year evaluation.
Conclusion: This study validates the use of a HA and CaHA blend (CaHA-CPM) for periocular rejuvenation, addressing various aging symptoms in this complex facial region.
Keywords: periocular, tear trough, sunken upper eyelids, supraorbital hollowness, A-frame deformity, superior sulcus syndrome, calcium hydroxylapatite, hyaluronic acid filler injection
Introduction
The periorbital skin is the thinnest skin on the face (<1mm),1 making it especially susceptible to environmental aging factors such as phototype, sun exposure, smoking, genetics among others.2–4 Furthermore, periorbital skin features a flattened dermal–epidermal interface, a thin dermis, and a low density of sebaceous glands.5 Over time, with increased laxity of the orbital septum, loss of subcutaneous collagen and deflation/herniation of orbital fat results in clinical manifestations of aging (eg, deepening of the supraorbital hollowness (SH), wrinkles, dermatochalasis of the upper and lower lids, worsening of palpebro-malar groove (PG), thinning of the skin, hyperpigmentation3,6). Eyes are an important and central facial feature, and these changes lead to a sad, fatigued, and unhealthy appearance.3–5
Periorbital rejuvenation aims to restore volume, soften rhytids, improve skin texture, and coloration.6 A broad array of periorbital anti-aging methods has been described, including topical medications, chemical peels, lasers, fillers, and surgery.1,2,7–9 However, the unique periorbital anatomy makes treatment challenging. Additionally, all therapies may have associated risks (eg, thermal necrosis or ectropion from excessive skin tightening) and may require multiple sessions to produce noticeable results.6 Treatment options are often designed to target specific clinical complaints. For instance, lasers and radiofrequency focus more on rhytids and skin tightening rather than on the clinical signs related to the deflated fat pads (eg, grooves and hollowness) which are addressed with injectable fillers alone or in combination with other therapies. Hyaluronic acid (HA) is the most commonly used filler type worldwide.6,10
The periocular area (especially the tear trough) may present injectors with the common challenge of dealing with edema, overcorrection, delayed edema and/or persistent inflammatory intermittent delayed swelling (PIDS).11 This manuscript describes our experience using 2 fillers with well-known efficacy and safety profile, Cohesive poly-densified matrix hyaluronic acid (CPM-HA; Belotero®, Anteis S.A., Lonay, Switzerland) and calcium hydroxylapatite-carboxymethylcellulose (CaHA; Radiesse (R), Merz Aesthetics, Raleigh, NC). This dual-filler strategy can address multiple patient concerns in a single multi-layered strategy; CaHA provides deep volume and structure while HA smoothen superficial lines and wrinkles.
Methods
This retrospective single-center study was approved by a centralized institutional review board (“Comité de Ética en Investigación Clínica (CEIC) – Stamboulian CEIC, Buenos Aires, Argentina”; Approval number: 2290/153/2024, approval date: January 16th, 2025) and was conducted in adherence to the Declaration of Helsinki (1996), and in accordance with regional laws and Good Clinical Practice for studies in human subjects. Written informed consent has been provided by all the patients for treatment, imaging and publication of case details and any accompanying images published.
Inclusion and Exclusion Criteria
Data from subjects treated from July 2022 to February 2024 were included in the study. Inclusion criteria comprised: 18 years or older, of any gender with mild-to-moderate palpebro-malar groove or supraorbital hollowness, preferably accompanied by hyperpigmentation. Exclusion criteria included: pregnancy, breastfeeding, auto-immune diseases, permanent filler injection, treatment in the periorbital area within 12 months.
Technique
CPM stands for Cohesive Polydensified Matrix, so when we refer to hybrids, we usually call them CaHA-CPM. For Belotero Balance, for example, we refer to it as CaHA-CPMB. In this treatment approach, a blend (CaHA-CPMB) of 0.8mL of CPM-HA B 22.5 mg/mL (Belotero® Balance; Merz Aesthetics, Raleigh, NC) and 0.2 mL of CaHA (Radiesse®; Merz Aesthetics, Raleigh, NC) either in diluted (1:1) or hyperdiluted form (1:2 or 1:4) was used.
For the 1:1 dilution, 1.5mL CaHA was diluted with 1.5mL of 2% lidocaine. For the 1:2 dilution, 1.5mL of CaHA was diluted with 1.5mL of 2% lidocaine and 1.5 mL of 0.9% saline. For the 1:4 dilution, 1.5mL CaHA was diluted with 1.5mL of 2% lidocaine and 4.5mL of 0.9% saline. After the initial dilution, 0.2 mL of the preparation was taken and blended with 0.8 mL of CPM 22.5 using Luer Lock syringes with 20 thorough passes to obtain a final homogeneous hybrid solution before injection, preventing needle clogging by CaHA particles.
The dilution ratio of CaHA was determined by the patient’s skin thickness. Dilution ratios ranged from 1:1 for thicker skin to 1:4 for thinner skin, tailored to minimize the risk formation of CaHA lumps and pseudoxanthelasma.
Palpebromalar Groove
Micro droplets of the blend were retro-injected using a 31G Becton Dickinson (BD) syringe needle in the supraperiosteal plane along the orbital rim for the palpebromalar groove.12 The same supraperiosteal technique described previously was used.10
The dose used ranged from 0.2 to 0.3 mL per side, per visit, depending on the depth, with an established frequency at the time of the first application (T0) and 30 days later, for a total of two treatment cycles.
Supraorbital Hollowness
For the supra orbital hollowness, we used the Softfil cannula (25G; 40 mm), which has a blunt tip and reduces the risk of bruising and vascular damage. The blend (CaHA-CPMB) was retro-injected along the supraorbital rim at the pre-septal plane, superficial to the orbital septum, and deep to the orbicularis oculi muscle. The plane of the injection for the supraorbital hollowness depended on the objective. For patients seeking an improvement in their skin quality (tension, hyperpigmentation) or treatment of a post-blepharoplasty scar, the pre-septal plane was suggested. A high cohesivity product that integrates seamlessly upon injection was recommended to avoid lumps. The retroseptal plane is recommended in cases where volume replacement of the supraorbital fat pads is needed and the product of choice is HA only; therefore, it was not included in this study.
The blunt cannula was preferred over a sharp needle for the supraorbital region, due to its lower risk of vascular occlusions, as well as higher precision to predict injection in the correct anatomical target layer from a remote entry point.13 We used a specific entry point between the lateral canthus and the distal edge of the eyebrow tail to access both the medial and the lateral part of the supraorbital rim. This point is in a line between the lateral canthus and the lateral eyebrow edge, at approximately 1.5 cm from the lateral canthus.14 Generally, it coincides with the upper orbital edge.
Care was taken to avoid injection within 1cm of the lateral canthus to prevent lymphatic obstruction as many deep lymphatic collectors are found in this area.15 The total volume of the blend varied from 0.2–0.25mL/side per visit. The procedure was fractionated in 2 to 3 visits, with a 30-day interval between visits (30, 60 and 90 days).
One patient was injected on the right side with HA alone (CPM-HA B 22.5 mg/mL) and on the left side with the blend (0.8mL of CPM-HA B 22.5 mg/mL + 0.2 mL of CaHA (1:1)) and ultrasound (US), Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) scan were performed to compare both sides.
Imaging
Images (2D) were captured with a standard camera (Sony A73) and Vectra H2 (Canfield) before the procedure and at days T0, T30, T60 (if needed), T90 (if needed) and 365 days.
Magnetic resonance imaging (MRI, General Electric Signa Explorer 1.5 Tesla MRI), CT scan (GE Brightspeed Elite, GE Healthcare, USA) and Ultrasound (US, Linear, Clarius; probes of 15 and 20 MHz) imaging to illustrate the location and filler integration was performed for 1 subject.
MRI was performed using highly specific face-oriented sequences with high resolution and a small field of view (voxel size: 0.3*0.3*3.0 mm). Thin slices (1.6 mm) across axial, sagittal, and coronal planes were acquired using the following sequences: 3D Bravo fast spin echo (FSE) sequence non-contrast (TR 7283 ms, TE 102 ms, Flip angle 160 degrees), with and without FS, STIR fast spin echo non-contrast (TR 3748 ms, TE 45 ms, Flip angle 160 degrees), with and without FS, T2 Cube (TR 2500 ms, TE 99 ms), with and without FS. Axial, coronal, and sagittal acquisitions).
Assessment
Investigator assessment
Post-treatment 2D and Vectra images (T30 and T60) were assessed by the investigator using a 5-point Global Aesthetic Improvement Scale (GAIS) (“worse, −1”; “no change, 0”; “improved, 1”; “much improved, 2”; and “very much improved, 3”). Moreover, the investigator scored the severity of the palpebro-malar groove depth, hyperpigmentation, the extent venous pooling, the amount of malar fat pad descent, and the visibility of lower eyelid rhytids using the Modified Sadick Scale16 (minimum score 4; maximum score 14 points) at baseline (T0) and post-treatment (T30, T60).
Patient Evaluation
Patients completed a 6-question questionnaire of satisfaction to evaluate their holistic experience throughout the treatment (“Is it the first time you treat the periocular area?”; What is your overall satisfaction with the treatment?”; “Did you have HA injection previously for the periocular area?”; “Was there any difference when you were treated with HA compared to the current treatment with the blend?”; “Did you notice improvement of skin quality with the current treatment with the blend?”; “Did you go back for re-evaluation consultation?”). Those who, prior to the study were treated with HA only, were asked to compare results with HA alone and with the blend.
Face MRI
Imaging evaluation and clinical correlation were evaluated by one independent radiologist who had over least 25 years of experience in the field. This reviewer was unaware of the injected substance on each side. The radiologist described the appearance of the dermal filler distribution pattern on each side on the MRI images.
Results
The study involved 106 participants, all Caucasian, predominantly female (94 patients and 12 male patients), ranging in age from 25 to 76 years (median 47 yrs), with a median modified Sadick score of 7 at baseline. Hyperpigmentation was present in 67.6% of the patients (71/106) at baseline as per investigator assessment. The final dilution of CaHA varied among subjects: 1:1 for 29 patients, 1:2 for 8 patients, and 1:4 for 69 patients. Almost all patients were followed up for at least 30 days (103; 97.1%), with 32 patients followed up for 30 days, and 71 patients followed up for 60 days or more (14 patients for 60 days, 31 patients for 90 days and 26 patients for 1 year). Three patients were lost to follow-up. Notably, at the 30-day evaluation, at least 1-grade improvement as assessed per investigator via Global Aesthetic Improvement Scale (GAIS score) was observed in most of the patients (88%; 91/103 patients) and maintained in 85% of patients at 60 days (52/61 patients) (Figures 1 and2). Out of the 12 subjects with unchanged 30-day GAIS evaluation, half were injected with a 1:4 CaHA dilution.
 |
Figure 1 GAIS score at 30-day evaluation. |
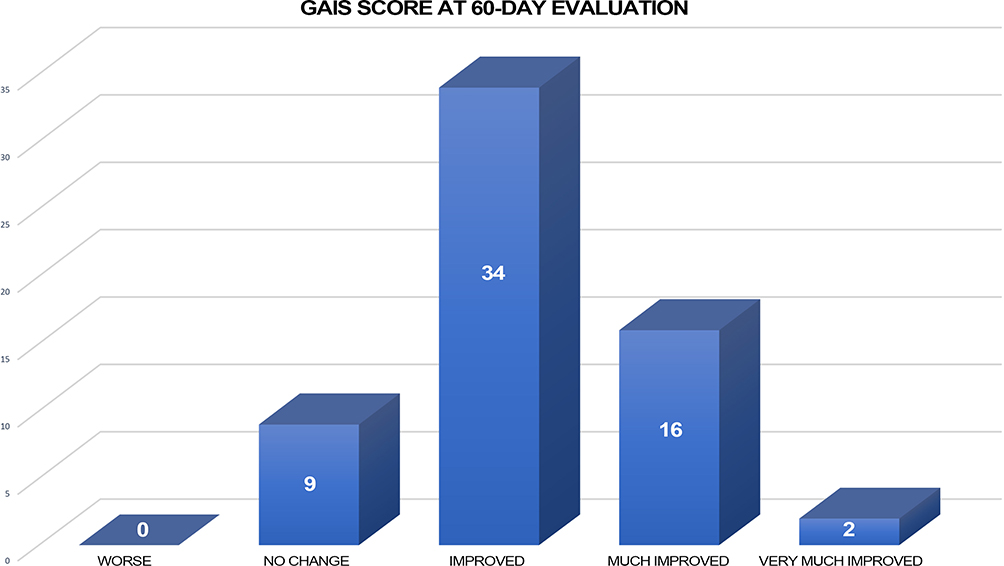 |
Figure 2 GAIS score at 60-day or more evaluation. Improvement. |
The modified Sadick Scale revealed substantial improvement in all patients in the appearance of the palpebro-malar groove and the sunken upper eyelids, alongside positive changes in skin laxity, wrinkles, and pigmentation score by the 60-day evaluation (Figure 3). Out of the 35 patients that completed the satisfaction questionnaire, 80% (28/35) referred improvement in skin quality. Sixteen (87%; 16/18) patients who had been previously treated with HA reported improvements to their skin quality and/or improvement of hyperpigmentation. None of the patients required hyaluronidase injections to dissolve overcorrection. One subject presented post-inflammatory hyperpigmentation after sun-exposure without proper care, which improved after topical treatment. Three patients presented transient edema, being one patient with a history of previous parotidectomy surgery with damaged lymphatic drainage that required treatment with hyaluronidase (15IU; one time injection) and antihistamine and betamethasone 0.6mg for 5 days. No severe complications were observed.
 |
Figure 3 Modified Sadick Scale scores at baseline, 30 and 60 days. |
 |
Figure 4 46 yo. Female received treatment for the palpebromalar groove with CaHA-CPMB blend (with CaHA with 1:4 dilution). (A) Before. (B) 30 days after 1st injection. (C) 60 days after 1st injection. (D) 1yr after injection. (E) 60 days after 2nd injection CaHA-CPMB (CaHa with 1:1 dilution). (F) 5 months after 2nd injection. |
 |
Figure 5 38 yo. Female received treatment for the sunken upper eyelids and palpebromalar groove with CaHA-CPMB blend (CaHA with 1:4 dilution). (A) Before. (B) 30 days after 1st injection. (C) 60 days after 1st injection. (D) 8 months after injection. (E) 30 days after 2nd injection CaHA-CPMB blend (CaHA with 1:1 dilution). (F) 1yr and 7 months after 2nd injection. |
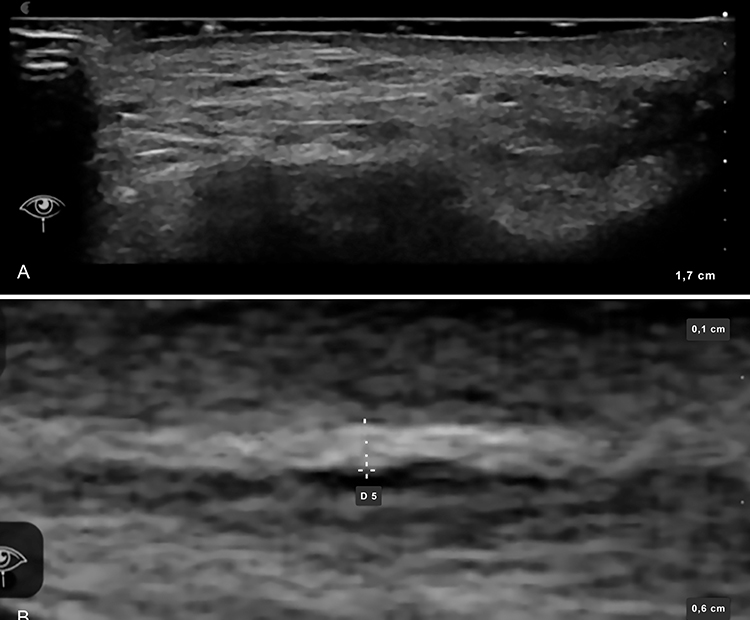 |
Figure 6 38 yo. Female received treatment on right side with CPM-HA B 22.5 mg/mL and left side with a CaHA-CPMB blend (CaHA with 1:1 dilution). US images performed 14 days after injection. (A) Right side, CMP-HA 22.5 mg/mL. (B) Left side CaHA-CPMB blend (CaHA with 1:1 dilution). |
 |
Figure 7 38 yo. Female received treatment on right side with CPM-HA B 22.5 mg/mL and left side with a CaHA-CPMB blend (CaHA with 1:1 dilution). CT scan 3D reconstruction image showing microdeposits of calcium in a linear trajectory in the left tear trough (black arrow). |
 |
Figure 8 38 yo. Female received treatment on right side with CPM-HA B 22.5 mg/mL and left side with a CaHA-CPMB blend (CaHA with 1:1 dilution). MR image showing microdeposits of hydrophilic filler were evidenced in the tear troughs in the supraperiosteal plane, predominantly on the right side. |
 |
Figure 9 38 yo. Female received treatment on right side with CPM-HA B 22.5 mg/mL and left side with a CaHA-CPMB blend (CaHA with 1:1 dilution). (A) Before. (B) 30 days after. (C) 60 days after. (D) 5 months after. |
For the 26 patients (24.5%; 26/106) followed for 1 year, results remained stable on day 365 (Figures 4 and 5). Three patients treated with the blend with the 1:4 dilution required a new treatment before day 365 (in 6 months), possibly due to the need of volume.
Imaging
Ultrasound
Facial ultrasound scanning was performed by a radiologist with linear probes of 15 and 20 MHz on both infraorbital regions. In the subdermal fat plane, ovoid microdeposits with regular contours of anechoic hydrophilic filler, averaging 1 mm in diameter, were visible, distributed diffusely, and uniformly without noticeable clusters. On the left side, a presence of focal hyperechogenic signal was noticeable in the deep dermis measuring 18 × 0.8 mm in diameter. This hyperechoic area could correspond to the presence of CaHA microspheres in the mentioned area (Figure 6). No hyperechoic clusters or ultrasound attenuation artifacts were seen in the area. No other noteworthy features were evident.
CT Scan
Thin axial cuts were taken from the trichion to the inferior border of the chin and reconstructed to create a 3D representation. Microdeposits of CaHA in the left tear trough, in the form of two linear trajectories, were seen predominantly according to the achieved images (Figure 7). No other noteworthy features were evident.
MRI
A series of multiplanar thin cuts were taken from the trichion to the inferior border of the chin and reconstructed to create a 3D reconstruction representation. T2 and STIR sequences were used. Microdeposits of hydrophilic filler were evidenced in the tear troughs in a supraperiosteal plane, predominantly on the right side (Figure 8). No other noteworthy features were evident.
Discussion
The desire for rejuvenation and the popularity of non-surgical solutions to treat the periocular area have increased. In a study examining the preferences of aesthetically oriented women, most respondents considered tear troughs among the most bothersome facial areas.17 The periorbital region has a complex anatomy,5 concurrent deformities, and a high risk of complications, and therefore remains one of the most complex and challenging regions of the face to be treated.1,18,19 Injecting in this area should therefore be reserved for advanced and experienced injectors only. Moreover, infraorbital hollowing is multifactorial in etiology (eg, preexisting maxillary bone hypoplasia, age-related loss of subcutaneous fat, descent of superficial fat pads, laxity of orbital retaining ligament, thinning of the skin overlying the fixed orbital rim, and/or orbital bone resorption1), meaning multiple treatment modalities are often required to adequately address all variables.3,19,20 For instance, in a study with non-ablative fractional laser, bipolar radiofrequency, and intense pulsed light, all light-based methods resulted in the reduction of the amount and depth of wrinkles as per subjects’ assessment, with no significant impact on skin aging, including discolorations, bags, dark circles (vascular/pigmentary) and oedema.20 Additionally, traditional surgical approaches related to removal of fat and tissue may cause more hollowness and result in loss of eyelid support.3
Minimally invasive HA injection has already been demonstrated to be a safe, effective, and reproducible procedure for the periorbital area.21,22 HA injections risk the formation of nodules, visible lumps, swelling, overcorrection, delayed edema, and persistent inflammatory intermittent delayed swelling (PIDS), particularly in the tear trough area, the “Tyndall effect”, among other undesirable effects.11 In a systematic review of the delayed complications described after dermal fillers ‘treatment, swelling, lumps, and nodules were among the most common, with the majority of the swelling cases being related to HA.23 In general, clinical evaluation of patients who received the blend treatment showed less edema compared to our usual patients who are treated with HA alone. A total of 3 patients experienced transient edema, including one patient with a history of periocular surgery (which could have damaged lymphatic drainage), presented a post-injection edema that required treatment. The surgical patient was treated with hyaluronidase (15IU; one time injection) and antihistamine and betamethasone 0.6mg for 5 days and edema had completely resolved after 1 month. Parotidectomy in the pre-auricular area can lead to scar formation and damaging of lymphatic vessels in that area and therefore altering the lymphatic drainage from the infraorbital area, as the lymphatics drain from the lateral periorbital area via the preauricular area to venous system.24
Patients with translucent skin (due to loss of dermal collagen, fat, and elastin allowing visualization of the orbicularis oculi muscle, for example), skin laxity, and/or hyperpigmentation may benefit less from HA injection alone.23 Skin laxity may predispose patients to develop significant lower eyelid rhytids16 and if skin is deeply pigmented, it may become more evident once the contour correction improved. Finally, moreover, aging is an ongoing process, and many patients may need to repeat HA treatment after determined intervals. Patients who prefer a single treatment with a more permanent substance would be candidates for blend injections which have extended treatment intervals. Finally, since some patients exhibit pigmented SH while others have dyschromia, scars, retractions, and fibrosis after blepharoplasties, a procedure that both fills and bioregenerates the area is needed.25 In our study, the majority of the patients that had been treated previously with HA referred improvement of skin quality and/or hyperpigmentation with the blend compared to HA alone.
HA and CaHA have complementary mechanisms of action, as HA provides an immediate effect and compensates for the early volume loss secondary to the resorption of the CMC gel carrier,26 whilst CaHA can enhance neocollagenesis properties thereby extending the duration of the filler treatment.27 Although HA may induce neocollagenesis, CaHA presented a more active, physiologic remodeling of the extracellular matrix (ECM) when compared to HA,27 with increase in proteoglycans, elastin and collagen synthesis,28 indicating it can induce remodeling of several aspects of the ECM.29 The collagen type I synthesis observed in immunohistochemistry was corroborated clinically by the increase in dermal thickness, as assessed by ultrasound.30 Furthermore, CaHA rheology can be tailored to achieve either filling and contouring or optimal regenerative effects, according to patient’s needs.31 Even when hyperdiluted, CaHA (1:2, 1:4, and 1:6) demonstrated significant increase in synthesis of collagen Types I and III four months after treatment30 and clinical improvement of necklines, neck laxity, and dermal thickness in adult women with mild and moderate cervical aging.32 It also possesses regenerative properties as it induces senescent fibroblasts to become active.33 Thus, based on the well-known properties and safety profiles of HA and CaHA, the authors opted to combine the 2 fillers in one injection to target multiple variables at a time (ie, improve skin laxity, quality, pigmentation, and thickness, with CaHA’s induced neocollagenesis and remodelling of the ECM and address fat pad deflation and improve ORL support with HA), improve patient’s experience by avoiding multiple treatments, and increase the duration of the treatment. CaHA also exhibits limited hygroscopic power in addition to the regenerative properties, which helps to minimize the risk of frequent edema in the area when HA is injected alone.34 This clinical observation was consistent with the MRI and CT readings comparing HA only and CaHA/HA injection sites; the right side (which received HA only) had greater amount of water, while on the left side (which received CaHA/HA) had less water and only filler substance (Figures 7–9).
CaHA has already been used for periocular rejuvenation.22,35,36 In the periorbital area, CaHA has been shown to improve hyperpigmentation, skin tone, color and thickness at week 16, with continuous improvement of skin quality beyond 4 months.16 Bernardini et al reported high patient satisfaction (overall satisfaction rate of 92%), with associated dark circles being satisfactorily treated in 68% of the patients,34 with lower rate of complications and no case of skin necrosis, visual loss, persistent pre-malar edema, or granuloma observed. In our study, improvement of eyelid hyperpigmentation was observed in 67.6% (71/106) of the patients with mild and transient adverse events (2.8%; 3/105;) and results remained stable in the 1-year follow-up. Nevertheless, it is important to highlight that the use of lower dilutions (eg, 1:4) may require smaller treatment intervals as seen in 3 of our patients. If the aim is to promote bioregeneration, the 1:4 dilution would suffice, while if volumization is desired (to address deep grooves), a 1:1 dilution would be more suitable. Furthermore, for patients with thinner skin, smaller intervals between injections of a blend with HA and hyperdiluted CaHa should be recommended, as their thin skin makes complications easier to notice.
The use of a premixed combination of the two products26,37 has been reported as safe, effective, with increased dermal collagen bundles without development of inflammation.25,26 Although areas with increased mobility may be at higher risk of nodule formation,38 by blending of CaHA and HA in our study, the final CaHA volume ends up more diluted in the final solution (HA + CaHA), reducing the risk of nodules development. In our study, no nodule formation was observed up to the 1-year follow-up. The regenerative capacity as well as elastic modulus of CaHA changes with various dilutions of saline. It is unknown to what extent our periocular hybrid filler is exactly influenced in rheology and regenerative capacity.31
The limitations of this study largely relate to its retrospective design, single evaluator, small population and lack of HA control group. These exploratory studies require follow-up using studies with comparative designs and conducted in a larger patient cohort for increased power, as well as blinded evaluation. This study does, however, highlights the need to consider this advanced blend injection technique for the periorbital region, especially for more experienced doctors.
Conclusion
We present a unique blend of CaHA and HA for the periocular area that has not been described previously. Given the high patient satisfaction, the long-lasting results and the lack of another procedure that treats many of the variables that affect this area, our presented approach of using a blend of a cohesive HA and diluted or hyperdiluted CaHA may represent a more effective and lower risk treatment strategy for the periocular area.
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Medical writing and editorial assistance were provided by Dr Danielle Shitara (Private Practice), and was supported by Medical Affairs of Merz Aesthetics LATAM, through its affiliate Merz Argentina in accordance with Good Publication Practice guidelines. The authors thank Dr Karina Ravera, radiologist from Sanatorio de la Trinidad Mitre, Argentina, who evaluated the radiology images.
Funding
Merz Aesthetics LATAM funded medical writing assistance and provided products to this study through its affiliate in Argentina. Despite this support, this study was conducted with autonomy and independence by the investigators, and Merz had any participation or influence on design, conduct, collection, assessment and evaluation of the presented data.
Disclosure
Dr Spada and Dr Van Loghem are global speakers for Merz Aesthetics. The authors report no other conflicts of interest in this work.
References
1. Woodward J, Cox SE, Kato K, Urdiales-Galvez F, Boyd C, Ashourian N. Infraorbital hollow rejuvenation: considerations, complications, and the contributions of midface volumization. Aesthet Surg J Open Forum. 2023;5:ojad016. doi:10.1093/asjof/ojad016
2. Aruan RR, Hutabarat H, Widodo AA, Firdiyono M, Wirawanty C, Double-blind FL. Randomized trial on the effectiveness of acetylhexapeptide-3 cream and palmitoyl pentapeptide-4 cream for crow’s feet. J Clin Aesthetic Dermatol. 2023;16(2):37–43.
3. Lee S, Yen MT. Nonsurgical rejuvenation of the eyelids with hyaluronic acid gel injections. Semin Plast Surg. 2017;31(1):17–21. doi:10.1055/s-0037-1598189
4. Kuruoglu D, Salinas CA, Kirk DS, Wong CH, Sharaf BA. Brow and eyelid rejuvenation: trends from the 100 most cited articles over 30 years. Medicina. 2023;59(2). doi:10.3390/medicina59020230
5. Love LP, Farrior EH. Periocular anatomy and aging. Facial Plast Surg Clin North Am. 2010;18(3):411–417. doi:10.1016/j.fsc.2010.05.001
6. Russel SM, Clark JM. Periorbital rejuvenation in the clinic: a state-of-the-art review. World J Otorhinolaryngol Head Neck Surg. 2023;9(3):242–248. doi:10.1002/wjo2.124
7. Pascali M, Quarato D, Pagnoni M, Carinci F. Tear trough deformity: study of filling procedures for its correction. J Craniofac Surg. 2017;28(8):2012–2015. doi:10.1097/SCS.0000000000003835
8. Lipp M, Weiss E. Nonsurgical treatments for infraorbital rejuvenation: a review. Dermatol Surg. 2019;45(5):700–710. doi:10.1097/DSS.0000000000001897
9. Kassir M, Kroumpouzos G, Puja P, et al. Update in minimally invasive periorbital rejuvenation with a focus on platelet-rich plasma: a narrative review. J Cosmet Dermatol. 2020;19(5):1057–1062. doi:10.1111/jocd.13376
10. Spada J, Ravera K, Schneider C. Needle versus cannula to treat tear trough: a prospective study comparing both methods. Plast Reconstr Surg Glob Open. 2023;11(11):e5327. doi:10.1097/GOX.0000000000005327
11. Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Invest Dermatol. 2013;6:295–316. doi:10.2147/CCID.S50546
12. Wong CH, Mendelson B. Newer understanding of specific anatomic targets in the aging face as applied to injectables: aging changes in the craniofacial skeleton and facial ligaments. Plastic Reconst Surg. 2015;136(5 Suppl):44S–48S. doi:10.1097/PRS.0000000000001752
13. Cotofana S, Lachman N. Anatomy of the facial fat compartments and their relevance in aesthetic surgery. J der Deutschen Dermatologischen Gesellschaft. 2019;17(4):399–413. doi:10.1111/ddg.13737
14. Spada J. Treating sunken upper eyelid with hyaluronic acid: recommendations and results. J Drugs Dermatol. 2022;21(9):1002–1008. doi:10.36849/JDD.6745
15. Bourgeois P, Peters E, Van Mieghem A, Vrancken A, Giacalone G, Zeltzer A. Edemas of the face and lymphoscintigraphic examination. Sci Rep. 2021;11(1):6444. doi:10.1038/s41598-021-85835-w
16. Corduff N. An alternative periorbital treatment option using calcium hydroxyapatite for hyperpigmentation associated with the tear trough deformity. Plast Reconstr Surg Glob Open. 2020;8(2):e2633. doi:10.1097/GOX.0000000000002633
17. Narurkar V, Shamban A, Sissins P, Stonehouse A, Gallagher C. Facial treatment preferences in aesthetically aware women. Dermatol surg. 2015;41 Suppl 1:S153–60. doi:10.1097/DSS.0000000000000293
18. Kolodziejczak A, Rotsztejn H. The eye area as the most difficult area of activity for esthetic treatment. J Dermatolog Treatment. 2022;33(3):1257–1264. doi:10.1080/09546634.2020.1832189
19. Anido J, Fernandez JM, Genol I, Ribe N, Perez Sevilla G. Recommendations for the treatment of tear trough deformity with cross-linked hyaluronic acid filler. J Cosmet Dermatol. 2021;20(1):6–17. doi:10.1111/jocd.13475
20. Kolodziejczak A, Rotsztejn H. Efficacy of fractional laser, radiofrequency and IPL rejuvenation of periorbital region. Lasers Med Sci. 2022;37(2):895–903. doi:10.1007/s10103-021-03329-7
21. Berguiga M, Galatoire O. Tear trough rejuvenation: a safety evaluation of the treatment by a semi-cross-linked hyaluronic acid filler. Orbit. 2017;36(1):22–26. doi:10.1080/01676830.2017.1279641
22. Hevia O, Cohen BH, Howell DJ. Safety and efficacy of a cohesive polydensified matrix hyaluronic acid for the correction of infraorbital hollow: an observational study with results at 40 weeks. J Drugs Dermatol. 2014;13(9):1030–1036.
23. Trinh LN, McGuigan KC, Gupta A. Delayed complications following dermal filler for tear trough augmentation: a systematic review. Facial Plast Surg. 2022;38(3):250–259. doi:10.1055/s-0041-1736390
24. Guisantes E, Beut J. Periorbital anatomy: avoiding complications with tear trough fillers. 2016.
25. Fakih-Gomez N, Kadouch J. Combining calcium hydroxylapatite and hyaluronic acid fillers for aesthetic indications: efficacy of an innovative hybrid filler. Aesthetic Plast Surg. 2022;46(1):373–381. doi:10.1007/s00266-021-02479-x
26. Chang JW, Koo WY, Kim EK, Lee SW, Lee JH. Facial rejuvenation using a mixture of calcium hydroxylapatite filler and hyaluronic acid filler. J Craniofac Surg. 2020;31(1):e18–e21. doi:10.1097/SCS.0000000000005809
27. Yutskovskaya Y, Kogan E, Leshunov E. A randomized, split-face, histomorphologic study comparing a volumetric calcium hydroxylapatite and a hyaluronic acid-based dermal filler. J Drugs Dermatol. 2014;13(9):1047–1052.
28. Gonzalez N, Goldberg DJ. Evaluating the effects of injected calcium hydroxylapatite on changes in human skin elastin and proteoglycan formation. Dermatol surg. 2019;45(4):547–551. doi:10.1097/DSS.0000000000001809
29. Corduff N. Introducing aesthetic regenerative scaffolds: an immunological perspective. J Cosmet Dermatol. 2023;22 Suppl 1:8–14. doi:10.1111/jocd.15702
30. Yutskovskaya YA, Kogan EA. Improved neocollagenesis and skin mechanical properties after injection of diluted calcium hydroxylapatite in the neck and decolletage: a pilot study. J Drugs Dermatol. 2017;16(1):68–74.
31. McCarthy AD, Soares DJ, Chandawarkar A, El-Banna R, Hagedorn N. Dilutional rheology of Radiesse: implications for regeneration and vascular safety. J Cosmet Dermatol. 2024;23(6):1973–1984. doi:10.1111/jocd.16216
32. de de Almeida AR T, Marques E, Contin LA, Trindade de Almeida C, Muniz M. Efficacy and tolerability of hyperdiluted calcium hydroxylapatite (Radiesse) for neck rejuvenation: clinical and ultrasonographic assessment. Clin Cosmet Invest Dermatol. 2023;16:1341–1349. doi:10.2147/CCID.S407561
33. Courderot-Masuyer C, Robin S, Tauzin H, Humbert P. Evaluation of lifting and antiwrinkle effects of calcium hydroxylapatite filler. In vitro quantification of contractile forces of human wrinkle and normal aged fibroblasts treated with calcium hydroxylapatite. J Cosmet Dermatol. 2016;15(3):260–268. doi:10.1111/jocd.12215
34. Bernardini FP, Cetinkaya A, Devoto MH, Zambelli A. Calcium hydroxyl-apatite (Radiesse) for the correction of periorbital hollows, dark circles, and lower eyelid bags. Ophthalmic Plast Reconstr Surg. 2014;30(1):34–39. doi:10.1097/IOP.0000000000000001
35. Wollina U. Improvement of tear trough by monophasic hyaluronic Acid and calcium hydroxylapatite. J Clin Aesthetic Dermatol. 2014;7(10):38–43.
36. Jacovella PF, Peiretti CB, Cunille D, Salzamendi M, Schechtel SA. Long-lasting results with hydroxylapatite (Radiesse) facial filler. Plastic Reconst Surg. 2006;118(3 Suppl):15S–21S. doi:10.1097/01.prs.0000234902.61284.c9
37. Yutskovskaya YA, Kogan EA, Koroleva AY. Clinical and histopathological evaluation of skin changes following intradermal injection of hybrid products combining calcium hydroxyapatite with various density hyaluronic acid. Madridge J Dermatol Res. 2024;6(1):126–139.
38. Emer J, Sundaram H. Aesthetic applications of calcium hydroxylapatite volumizing filler: an evidence-based review and discussion of current concepts: (part 1 of 2). J Drugs Dermatol. 2013;12(12):1345–1354.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.