")
Back to Journals » Clinical Ophthalmology » Volume 19
Hydrophobic and Hydrophilic IOLs in Patients with Uveitis – A Randomised Clinical Trial
Authors Pålsson S, Schuborg C, Sterner B, Andersson Grönlund M, Zetterberg M
Received 3 September 2024
Accepted for publication 16 December 2024
Published 4 February 2025 Volume 2025:19 Pages 373—383
DOI https://doi.org/10.2147/OPTH.S493398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sara Pålsson,1,2 Claes Schuborg,2,3 Bertil Sterner,1,2 Marita Andersson Grönlund,1,4 Madeleine Zetterberg1,2
1Department of Clinical Neuroscience/Ophthalmology, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 2Region Västra Götaland, Sahlgrenska University Hospital, Department of Ophthalmology, Mölndal, Sweden; 3Guldhedskliniken, Gothenburg, Sweden; 4Department of Ophthalmology, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
Correspondence: Madeleine Zetterberg, Sahlgrenska University Hospital, Department of Ophthalmology, Mölndal, SE 431 80, Sweden, Tel +46 31 33 43 31 50, Fax +46 31 41 29 04, Email [email protected]
Purpose: To compare inflammatory response, visual acuity, and complications of two intraocular lenses (IOLs) in patients with and without uveitis.
Setting: Tertiary referral centre at Sahlgrenska University Hospital/Mölndal, Sweden.
Design: Prospective randomised controlled trial.
Patients and Methods: Patients with and without uveitis eligible for cataract surgery were randomised to receive a hydrophobic or a hydrophilic square-edged intraocular lens (IOL). Patients undergoing bilateral surgery received a hydrophobic IOL in one eye and a hydrophilic in the other. Visual acuity, flare, and central foveal thickness were used as outcome measures.
Results: In total, 34 (61%) patients (52 eyes) with uveitis and 22 (39%) non-uveitic patients (38 eyes) were included in the study. Comparable corrected distance visual acuity (CDVA) was seen, regardless of IOL material. Flare, six months postoperatively, for those undergoing bilateral surgery, showed no significant difference between eyes receiving a hydrophilic IOL or a hydrophobic IOL; mean difference was − 3.2 (SD ± 20.7) ph/ms between eyes with uveitis (p = 0.53) and − 0.6 SD ± 7.5 ph/ms between eyes without uveitis (p = 0.77). No significant difference in cystoid macular edema (CME) was seen for uveitic patients receiving a hydrophobic IOL (n = 2; 8.0%) and those receiving a hydrophilic IOL (n = 6; 22.2%; p = 0.25).
Conclusion: No significant differences in postoperative inflammatory reaction or rate of CME were seen regardless of using a hydrophobic or a hydrophilic IOL. In general, an improvement in CDVA was seen after cataract surgery with both types of IOLs. Thus, the present study did not support either of the IOL materials as advantageous in patients with uveitis.
Plain Language Summary: Uveitis, an inflammatory eye condition, often leads to patients needing cataract surgery. The surgery involves removing the eye’s clouded lens and typically replacing it with an artificial lens known as an intraocular lens. Improvement in vision and possible complications vary depending on the type of replacement lens used. This randomised controlled trial compares inflammation, improvement in vision, and possible complications in patients that received two differing types of intraocular lenses. Improvement in vision was seen in both lens types yet neither lens type was superior in terms of inflammation.
Keywords: biocompatibility, cataract, complications, implant, inflammation
Introduction
Cataract surgery in the setting of uveitis is challenging and requires meticulous planning.1 Surgical technique, timing of surgery as well as anti-inflammatory treatment and postoperative controls need to be more carefully addressed in patients with uveitis, than in cases with age-related cataract only, in order to prevent complications and achieve optimal visual acuity.
Inflammation is associated with increased risk of developing postoperative complications such as cystoid macular edema (CME), posterior capsule opacification (PCO), glaucoma, and hypotony.2–4 Therefore, planning of cataract surgery in patients with uveitis is focused on how to perform surgery with inducing as little inflammation as possible and employing optimised anti-inflammatory treatment perioperatively. In general, at least two months of quiescent inflammation before surgery is considered eligible.5 However, evidence regarding preferable medical and surgical methods is lacking and considerable differences are seen between centres. Intraocular lens (IOL) material has been shown to influence the surgical results including differences due to capsular and uveal biocompatibility.6 Hydrophilic acrylic IOLs have shown better uveal biocompatibility and may therefore induce a milder inflammatory reaction compared to hydrophobic IOLs.7 On the other hand, an increased risk of developing PCO has been associated with hydrophilic acrylic IOLs,8 possibly due to less favourable capsular biocompatibility. However, optic edge design in addition to IOL material influences the risk of developing PCO, and Koshy et al showed no significant difference in PCO development comparing a hydrophobic and hydrophilic IOL, both with sharp edges.9
The purpose of the present randomised controlled trial was to compare inflammatory response, postoperative complications, and visual outcome after cataract surgery in uveitic and non-uveitic patients receiving either a sharp edged acrylic hydrophilic IOL or a sharp edged acrylic hydrophobic IOL.
Materials and Methods
Data Collection
This prospective randomised controlled study was approved by the Swedish Ethical Review Authority (DNR 787–13) and all procedures were performed in accordance with the Declaration of Helsinki. Patients with uveitis planned for cataract surgery at Sahlgrenska University Hospital, Mölndal, January 2017 to December 2019, were given oral and written study information and asked for participation. Patients without uveitis and in need of cataract surgery, during the same period, were also included in the study after informed consent in order to compare the effect of IOL material in non-uveitic eyes with that of eyes with uveitis. Patients < 18 years at surgery, unable to give informed consent, having large corneal opacities, other eye surgery within three months, active uveitis, or uncontrolled glaucoma preoperatively, were excluded as well as those with intraoperative posterior capsule rupture with/without vitreous loss.
Study Population
All patients who gave written consent and were considered capable to participate in follow-ups were included. All types of uveitic entities were included in the uveitic group and patients without uveitis were selected as controls. Three patients with uveitis and two without uveitis were excluded prior to surgery. One of the patients without uveitis did not appear at surgery despite several calls and in the other case, the procedure was performed by a surgeon other than the two study surgeons (MZ and CS). Two of the patients with uveitis chose surgery in a private practice and one of the patients with uveitis was managed by another surgeon. In cases where bilateral surgery was indicated both eyes were included.
IOL Specifications
The participants were randomised to receive either a hydrophilic IOL (INCISE® Bausch & Lomb, Rochester, N.Y., USA; a single-piece IOL with 360° sharp optic edge of hydrophilic acrylic material) or a hydrophobic IOL (VivinexTM iSert® [XC1], Hoya surgical optics, Tokyo, Japan; a single-piece IOL with a square, thin, and textured edge of hydrophobic acrylic material).
Randomisation
The study was registered on ClinicalTrials.com (ID: 031-6). Randomisation was achieved in a blockwise manner using a web-based online system (www.jerrydallal.com/random/randomize.html). Patients with uveitis and controls were randomised separately to receive either a hydrophobic or a hydrophilic IOL in the first eye undergoing cataract surgery. If the other eye was in need of surgery, the other type of IOL was then chosen. Patients with previous cataract surgery in one eye were randomised in the same manner as patients undergoing unilateral surgery.
Surgery
Standard clear corneal phacoemulsification using topical anaesthesia was performed. The anterior chamber was maintained with ophthalmic viscosurgical device (OVD). Small pupils and posterior synechiae were managed with OVD and iris retractors (iris hooks) as needed. Trypan blue (VisionBlue, D.O.R.C. Dutch Ophthalmic Research Center, The Netherlands; or Monoblue, Arcadophta, France) was used to stain the anterior capsule in dense cataracts. An anterior continuous curvilinear capsulorhexis (ACCC) was created followed by hydrodissection, phacoemulsification and IOL implantation. All surgeries were performed by one of two experienced surgeons (CS, MZ).
Pre- and Postoperative Protocol
Participants underwent a dilated slit lamp examination by an ophthalmologist (SP) prior to surgery. Details on anatomic localisation and uveitic entity were noted as well as ocular comorbidity, systemic diseases and ongoing topical or systemic anti-inflammatory treatment. The degree of cataract was classified according to the Lens Opacities Classification System (LOCSIII).10 Grading of inflammation was performed according to the Standardization of uveitis nomenclature (SUN) criteria11 and measurements with a flare meter were performed. In addition optical coherence tomography (OCT) was performed preoperatively to assess central foveal thickness (CFT) as well as excluding preoperative CME. At least three months of non-existing or stable inflammation was confirmed before surgery by reviewing charts and asking patients if any deterioration of inflammation or increase in anti-inflammatory treatment had occurred.
All patients with uveitis were examined seven to fourteen days preoperatively to establish that no deterioration of inflammation had occurred and the perioperative treatment was reviewed with the patient. Standard anti-inflammatory treatment with Dexamethasone (Isopto-Maxidex®) 1mg/mL, three times daily, and Nepafenak (Nevanac®) 3 mg/mL, once daily, was given in all cases and adjusted due to the inflammatory response if needed. Patients with a history of uveitis were prompted to start treatment one week prior to surgery and if no flare-ups were seen, treatment was terminated six weeks postoperatively. Non-uveitic patients started anti-inflammatory treatment after surgery and continued three weeks postoperatively. In cases with uveitis, except in Fuchs uveitis and in cases with a single episode of iritis and no systemic association, adjunctive 30 mg of oral steroids Prednisolone (Prednisolone®) was given once a day three days preoperatively, three days postoperatively and thereafter tapered with 5 mg every third day.
Follow-up visits were planned at two weeks, two months, and six months for all patients. Patients with uveitis were also seen on day one and five after surgery. At these visits, corrected distance visual acuity (CDVA), intraocular pressure (IOP), slit lamp examination including degree of inflammation, were controlled by an experienced optometrist (BS) or either of two ophthalmologists (MZ or SP). In addition, measurements with a flare meter (KOWA Laser Flare Meter FM-600, Tokyo, Japan) and OCT (Topcon 3D OCT-Maestro, Topcon 3D-OCT-200 or Topcon DRI OCT-1 Triton Plus, Tokyo, Japan) were performed. Eyes presenting with intraretinal cysts on OCT during the follow-up period were assessed as presenting with CME and included in CME analysis. The time of presentation was noted.
Statistics
Descriptive statistics included mean ± standard deviation (SD), or median with range or interquartile range, as appropriate. Continuous variables were analysed with Student´s t-test and/or Mann–Whitney U-test whereas categorical parameters were analysed using Chi-squared test. To assess the difference in flare between eyes undergoing bilateral surgery, paired t-test was used. Binary logistic regression was performed using a backwards stepwise procedure with flare as the dependent variable and age at surgery, gender, uveitis, IOL-type, mechanical pupil dilation, pseudoexfoliations, and staining of the anterior lens capsule as covariates. For this purpose, the parameter flare was dichotomised using 9.4 ph/ms, which was the mean flare at six months for the entire cohort. Snellen visual acuity was converted to Logarithm of the Minimum Angle of Resolution (logMAR) prior to analysis. P < 0.05 was considered statistically significant. IBM SPSS statistics, version 27 for Mac (SPSS Inc., Chicago, IL, USA) was used for statistical analysis.
Results
Study Population
In total, 34 patients with uveitis (52 eyes) and 22 non-uveitic patients (38 eyes) were included in the study (Table 1). Patients with uveitis were younger at surgery with a mean age, as calculated for each surgical procedure, ie per eye, of 66 years (SD ± 10) compared with non-uveitic patients; 74 years (SD ± 8; p < 0.001). However, no difference in gender distribution was seen; 21 (61.8%) female patients with uveitis and 16 (72.7%; p = 0.56) without uveitis were included. Posterior subcapsular cataract was more frequent in patients with uveitis with a median LOCS III of 2.5 (IQR=1.5–3.5) compared with 1.5 (IQR = 1.0–2.5) in patients without uveitis, p = 0.003 (Table 1). Other types of cataract were equally distributed between groups. The most common systemic conditions associated with uveitis were ankylosing spondylitis with nine eyes (17%) and idiopathic uveitis, 20 eyes (38%) (Table 2). Anatomically, anterior localisation of uveitis was most frequently seen, 49 eyes (94%). The remaining patients were heterogenous with infectious as well as inflammatory causes of uveitis. Three eyes (6%) showed intermediate uveitis and no eye had posterior engagement. Immunomodulatory treatment (IMT) was used in eight patients (24%) to control uveitis.
 |
Table 1 Baseline Characteristics of the Study Population, Surgical Details and IOL Material |
 |
Table 2 Uveitic Localisation and Associated Systemic Diseases |
Surgical Management
All surgical challenges; staining of the anterior lens capsule, mechanical pupil dilation and iris hooks at capsulorhexis margin, were more commonly seen in patients with uveitis, except the use of capsular tension ring. However, a significant difference was only seen with mechanical pupil dilation which was used in 15 eyes (28.8%) with uveitis and in none of the non-uveitic eyes (p < 0.001). In eyes with uveitis, 36 (69.2%) of procedures were performed as bilateral surgery compared with 32 (84.2%) of eyes without uveitis (p = 0.14) (Table 1).
Visual Acuity
Eyes with uveitis presented with worse mean CDVA preoperatively, 0.44 ± 0.44 logMAR (0.36 Snellen decimal [dec]) compared with those without uveitis, 0.30 ± 0.18 logMAR, (0.5 dec), (p = 0.04). Two weeks postoperatively, mean CDVA was improved and maintained at equal levels at six months postoperatively, where mean CDVA in uveitic eyes with a hydrophilic IOLs was 0.09 ± 0.17 (0.81 dec) and for those with a hydrophobic IOL 0.08 ± 0.23 (0.83 dec) (p = 0.88). Corresponding values in the group without uveitis was 0.03 ± 0.07 logMAR (0.93 dec) for those with a hydrophilic IOL and 0.06 ± 0.11 (0.87 dec) for those with a hydrophobic IOL (p = 0.45). (Supplement Table 1). No significant difference in visual improvement at six months compared to preoperatively was seen between groups.
Flare
Mean flare preoperatively in eyes with uveitis receiving a hydrophilic IOL was 35.0 ± 84.8 ph/ms and 20.0 ± 28.0 ph/ms in those receiving a hydrophobic IOL (p = 0.41). In eyes without uveitis receiving a hydrophilic IOL, mean flare preoperatively was 9.7 SD ± 4.5 ph/ms and in those receiving a hydrophobic IOL 9.1 SD ± 4.2 ph/ms (p = 0.70) (Table 3). Figure 1 shows the change in flare over time. Comparing flare, at six months, between eyes in patients undergoing bilateral surgery, showed no significant difference between the eye receiving a hydrophilic IOL and the eye receiving a hydrophobic IOL with a mean difference in flare of −3.2, SD ± 20.7 ph/ms (p = 0.53) in eyes with uveitis and −0.6 SD ± 7.5 ph/ms (p = 0.77) in eyes without uveitis. SUN grading showed similar levels of flare, anterior chamber cells and vitreous cells for hydrophobic and hydrophilic IOLs at all time points (Supplement Table 2). Performing binary logistic regression with flare > 9.4 ph/ms at six months as the dependent factor showed significant correlations with gender, age at surgery, mechanical pupil dilation and pseudoexfoliations (Table 4). The risk of high flare decreased with ageing and was lower for women.
 |
Table 3 Flare Preoperatively and Six Months Postoperatively |
 |
Table 4 Logistic Regression of Potential Risk Factors of Flare >9.4 ph/ms Six Months Postoperatively in Patients Receiving Hydrophobic and Hydrophilic IOLs |
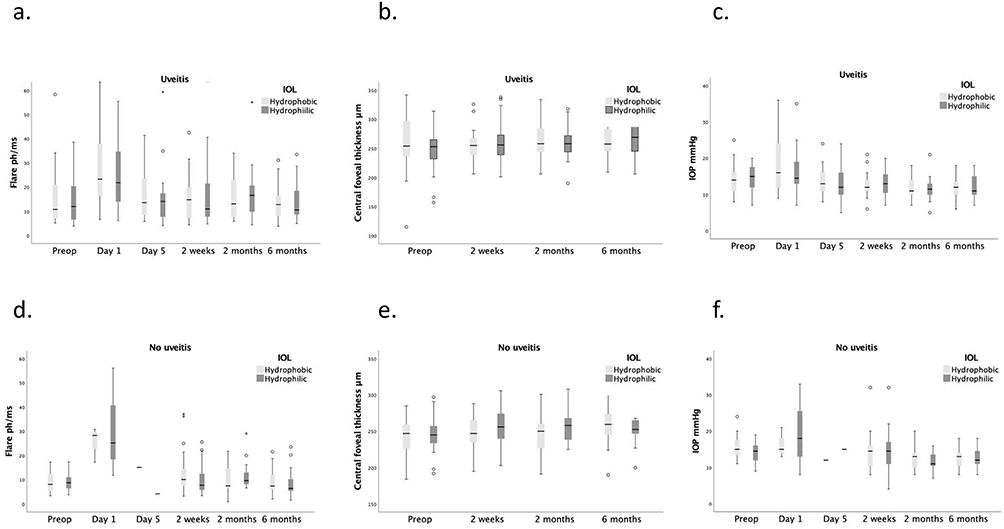 |
Figure 1 Difference in flare (ph/ms, a and d), central foveal thickness (CFT [µm], b and e) and intraocular pressure (IOP [mmHg], c and f) between eyes with a hydrophobic and hydrophilic intraocular lens (IOP) over time. Box plot shows interquartile range (IQR) with median and the whiskers indicate the minimum and maximum values. Circles represent outliers. |
Central Foveal Thickness
Mean change of CFT at six months compared to preoperatively in uveitic patients receiving a hydrophilic IOL was 22 ± 47µm and for those receiving a hydrophobic IOL 9 ± 37µm (p = 0.33) (Table 5). Corresponding values for those without uveitis was 6 ± 23µm with the hydrophilic IOL and 15 ± 27µm with the hydrophobic IOL (p = 0.28). Mean difference between the eye receiving a hydrophilic and the eye receiving a hydrophobic IOL at six months for those undergoing bilateral surgery was −0.8 ± 36.4µm for patients with uveitis and 9.5 ± 38.6µm for those without uveitis. Mean time to CME diagnosis was 63.5 ± 54.4 days for uveitic patients receiving a hydrophilic IOL and 78.5 ± 89.8 (p = 0.85) days for those receiving a hydrophobic IOL. No significant difference in incidence of CME with hydrophobic IOLs (n = 2; 8.0%) and hydrophilic IOLs (n = 6; 22.2%) (p = 0.25) or time after surgery were seen in patients with uveitis.
 |
Table 5 Central Foveal Thickness (CFT) Preoperatively and Six Months Postoperatively |
Discussion
There are many types of IOLs with different characteristics. In this study, we compared a square edged hydrophilic and a hydrophobic IOL in patients with and without uveitis, focusing on the postoperative inflammatory response and its related complications.
In line with previous studies12,13 patients with uveitis were younger at surgery than non-uveitic patients. Although uveitic etiology was heterogenic in our group, a great majority showed anterior uveitis (94.2%) most commonly idiopathic or associated with ankylosing spondylitis. When comparing with the epidemiologic study by Bro et al14 the patients in the present study had a similar distribution of uveitic patients with a rather large group of anterior uveitis. However, the study by Bro et al was community-based, ie not describing the situation at a referral centre as in the present study. Comparing the uveitic distribution to referral centres in Italy and Germany, 51.2%15 and 45.4%16 respectively, of their patients showed anterior uveitis and one would have expected a higher incidence of intermediate and posterior uveitis in our group. However, in the present study, in contrast to the two latter, children were not included. Also, the present study only included patients subjected to cataract surgery alone, hence excluding those who went through combined procedures (ie cataract surgery and vitrectomy), which may have been the case for some patients with intermediate and posterior uveitis.
In the present study, as well as in previous reports, cataract surgery in patients with uveitis was associated with more surgical difficulties.17,18 Mechanical pupil dilation in particular was more commonly seen in patients with uveitis, possibly due to posterior synechiae. Difficulties at surgery commonly leads to more traumatic and time-consuming surgery, which in turn increases the risk of severe inflammatory reaction postoperatively.19 Patients with uveitis already prone to developing inflammation may consequently develop a particularly severe postoperative inflammation which partly might explain the increased risk of complications such as CME.20
Visual acuity preoperatively was worse in patients with uveitis, probably indicating more pronounced cataract which in turn implies more difficult surgery. However, low CDVA preoperatively did not correspond to poorer visual acuity postoperatively and equal visual acuity was achieved in patients with and without uveitis. Visual acuity was maintained at six months postoperatively and improvement of visual acuity seen in eyes with uveitis supporting the benefit of cataract surgery in spite of increased perioperative risks and other comorbidities. None of the IOLs tested showed superior results to the other regarding visual outcome at any timepoint.
As previously shown, patients with uveitis have a higher degree of flare than patients without uveitis, preoperatively as well as postoperatively.21 However, no difference in flare related to IOL type was seen at six months and a similar course of inflammatory reaction with increased flare immediately postoperatively and early return to preoperative values regardless of IOL-type was seen. Binary logistic regression with flare >9.4 ph/ms at six months as the dependent factor showed significant correlation with gender, age at surgery, mechanical pupil dilatation and pseudoexfoliations. Female gender showed a negative correlation to high flare indicating a less severe course of uveitis in females which has previously also been described by Young et al.22 As previously shown, older age was correlated to less severe inflammatory reaction and mechanical pupil dilatation showed positive correlation to higher flare postoperatively as shown by Taipale et al.23 Uveitic patients in general, as well as in the present study, are younger at cataract surgery than patients with age-related cataract only and in our cohort, mechanical pupil dilatation was only used in patients with uveitis. These factors may contribute to increased risk of a higher postoperative flare in patients with uveitis.
Most cases of CME were seen in patients with uveitis receiving a hydrophilic IOL. Even though no significant difference in flare or CME was evident related to IOL-type, patients with uveitis receiving a hydrophilic IOL had a slightly higher flare contradicting previous reports which have shown better biocompatibility with hydrophilic IOLs. The higher flare in turn may explain a higher occurrence of CME in this group as previously shown by Ersoy et al.24
Our study is limited by a relatively small cohort which can be due to patients with uveitis constituting a small group among those requiring cataract surgery. Also, a majority of our patients with uveitis showed anterior uveitis and there were few patients with intermediate and posterior uveitis thus constituting a cohort with less severe inflammatory disease. This in turn makes general conclusions including more severe cases of uveitis less feasible. However, all patients with uveitis were included during the recruitment period, hence demonstrating few patients with more severe uveitis eligible for cataract surgery during the current study period.
Another limitation of the study was that three different OCT devices were used throughout the study, making comparisons of macular thickness less accurate. However, since the OCT instrument used for each follow-up depended on what device was available, there was no systematic bias.
Conclusion
In conclusion, no significant differences in inflammatory reaction or rate of CME were seen regardless of using a hydrophobic or a hydrophilic IOL. In general, an improvement in CDVA, was seen after cataract surgery with both IOL-types tested in patients with and without uveitis. Although the present study did not support either of the IOL-materials as advantageous in patients with uveitis, it demonstrates the benefit of cataract surgery in eyes with uveitis.
Data Sharing Statement
The data from this research will not be made available for sharing in accordance with our hospital guidelines and Ethical Committee’s restrictions. However, as per local policy, research data is stored securely for 20 years should any follow-up be necessary. Following that, all research data is appropriately destructed.
Acknowledgments
The study was financed by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement (ALF-GBG-441721 and ALF-GBG-725041), Konung Gustav and Drottning Victorias Frimurarstiftelse (Swedish Order of Freemasons), and De Blindas Vänner. The sponsors or funding organisations had no role in the design or conduct of this research. None of the authors has a financial or proprietary interest in any material or method mentioned.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Llop SM, Papaliodis GN. Cataract surgery complications in uveitis patients: a review article. Semin Ophthalmol. 2018;33(1):64–69. doi:10.1080/08820538.2017.1353815
2. De Maria M, Coassin M, Mastrofilippo V, Cimino L, Iannetta D, Fontana L. Persistence of inflammation after uncomplicated cataract surgery: a 6-month laser flare photometry analysis. Adv Ther. 2020;37(7):3223–3233. doi:10.1007/s12325-020-01383-1
3. El-Harazi SM, Feldman RM. Control of intra-ocular inflammation associated with cataract surgery. Curr Opinion Ophthalmol. 2001;12(1):4–8. doi:10.1097/00055735-200102000-00002
4. Ozates S, Berker N, Cakar Ozdal P, Ozdamar Erol Y. Phacoemulsification in patients with uveitis: long-term outcomes. BMC Ophthalmol. 2020;20(1):109. doi:10.1186/s12886-020-01373-5
5. Mehta S, Linton MM, Kempen JH. Outcomes of cataract surgery in patients with uveitis: a systematic review and meta-analysis. Am J Ophthalmol. 2014;158(4):676–692.e7. doi:10.1016/j.ajo.2014.06.018
6. Lloyd AW, Faragher RG, Denyer SP. Ocular biomaterials and implants. Biomaterials. 2001;22(8):769–785. doi:10.1016/s0142-9612(00)00237-4
7. Abela-Formanek C, Amon M, Kahraman G, Schauersberger J, Dunavoelgyi R. Biocompatibility of hydrophilic acrylic, hydrophobic acrylic, and silicone intraocular lenses in eyes with uveitis having cataract surgery: long-term follow-up. J Cataract Refract Surg. 2011;37(1):104–112. doi:10.1016/j.jcrs.2010.07.038
8. Chang A, Kugelberg M. Posterior capsule opacification 9 years after phacoemulsification with a hydrophobic and a hydrophilic intraocular lens. Eur J Ophthalmol. 2017;27(2):164–168. doi:10.5301/ejo.5000831
9. Koshy J, Hirnschall N, Vyas AKV, et al. Comparing capsular bag performance of a hydrophilic and a hydrophobic intraocular lens: a randomised two-centre study. Eur J Ophthalmol. 2018;28(6):639–644. doi:10.1177/1120672117752133
10. Chylack LT Jr, Wolfe JK, Singer DM, et al. The lens opacities classification system iii. the longitudinal study of cataract study group. Arch Ophthalmol. 1993;111(6):831–836. doi:10.1001/archopht.1993.01090060119035
11. Trusko B, Thorne J, Jabs D, et al. The Standardization of Uveitis Nomenclature (SUN) project. Development of a clinical evidence base utilizing informatics tools and techniques. Method Inform Med. 2013;52(3):259–65, S1–6. doi:10.3414/me12-01-0063
12. Chu CJ, Dick AD, Johnston RL, Yang YC, Denniston AK. Cataract surgery in uveitis: a multicentre database study. Br J Ophthalmol. 2017;101(8):1132–1137. doi:10.1136/bjophthalmol-2016-309047
13. Dana MR, Chatzistefanou K, Schaumberg DA, Foster CS. Posterior capsule opacification after cataract surgery in patients with uveitis. Ophthalmology. 1997;104(9):1387–1393;discussion1393–4. doi:10.1016/s0161-6420(97)30126-2
14. Bro T, Tallstedt L. Epidemiology of uveitis in a region of southern Sweden. Acta Ophthalmol. 2020;98(1):32–35. doi:10.1111/aos.14130
15. Cimino L, Aldigeri R, Salvarani C, et al. The causes of uveitis in a referral centre of Northern Italy. Intl Ophthalmol. 2010;30(5):521–529. doi:10.1007/s10792-010-9359-y
16. Jakob E, Reuland MS, Mackensen F, et al. Uveitis subtypes in a German interdisciplinary uveitis center--analysis of 1916 patients. J Rheumatol. 2009;36(1):127–136. doi:10.3899/jrheum.080102
17. Chan NS, Ti SE, Chee SP. Decision-making and management of uveitic cataract. Indian J Ophthalmol. 2017;65(12):1329–1339. doi:10.4103/ijo.IJO_740_17
18. Elgohary MA, McCluskey PJ, Towler HM, et al. Outcome of phacoemulsification in patients with uveitis. Br J Ophthalmol. 2007;91(7):916–921. doi:10.1136/bjo.2007.114801
19. Ursell PG, Spalton DJ, Tilling K. Relation between postoperative blood-aqueous barrier damage and LOCS III cataract gradings following routine phacoemulsification surgery. Br J Ophthalmol. 1997;81(7):544–547. doi:10.1136/bjo.81.7.544
20. De Maria M, Coassin M, Iannetta D, Fontana L. Laser flare and cell photometry to measure inflammation after cataract surgery: a tool to predict the risk of cystoid macular edema. Int Ophthalmol. 2021;41(6):2293–2300. doi:10.1007/s10792-021-01779-0
21. Shoughy SS, Elkum N, Tabbara KF. Aqueous protein level and flare grading. Acta Ophthalmol. 2015;93(2):e173–4. doi:10.1111/aos.12522
22. Yeung IY, Popp NA, Chan CC. The role of sex in uveitis and ocular inflammation. Int Ophthalmol Clin. 2015;55(3):111–131. doi:10.1097/iio.0000000000000072
23. Taipale C, Holmström EJ, Ilveskoski L, Tuuminen R. Incidence of pseudophakic cystoid macular edema in eyes with and without pupil expansion device. Acta Ophthalmol. 2019;97(7):688–694. doi:10.1111/aos.14007
24. Ersoy L, Caramoy A, Ristau T, Kirchhof B, Fauser S. Aqueous flare is increased in patients with clinically significant cystoid macular oedema after cataract surgery. Br J Ophthalmol. 2013;97(7):862–865. doi:10.1136/bjophthalmol-2012-302995
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.