")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Hyper-Relapse Disease is a Special Pattern of Relapse of Hepatocellular Carcinoma After Curative Hepatectomy: A Retrospective Cohort Study
Authors Yang ZL, Gan YX, Xu JX, Tang YH, Ouyang LY, Qi LN , Xu L
Received 16 January 2025
Accepted for publication 28 June 2025
Published 5 July 2025 Volume 2025:12 Pages 1301—1314
DOI https://doi.org/10.2147/JHC.S507437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Zi-Liang Yang,1,* Yi-Xiang Gan,1,* Jing-Xuan Xu,2,* Yu-Hao Tang,1 Li-Ying Ouyang,3 Lu-Nan Qi,2,* Li Xu1,*
1Department of Liver Surgery, Sun Yat-Sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China; 2Department of Hepatobiliary Surgery, Guangxi Medical University Cancer Hospital, Nanning, Guangxi, People’s Republic of China; 3Intensive Care Unit, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Xu, Department of Liver Surgery, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, 651 E. Dongfeng Road, Guangzhou, 510060, People’s Republic of China, Tel +86 20-87343115, Fax +86 20-87343585, Email [email protected]
Background: While hepatectomy is the major curative treatment of hepatocellular carcinoma (HCC), high relapsing rates were observed. Of note, quite a few cases of tumor relapses were characterized by very quick appearance and disseminated lesions. This study aims to identify a special pattern of tumor relapse and to evaluate the prognostic significance of it for HCC patients after curative hepatectomy.
Methods: Medical records of HCC patients who underwent curative hepatectomy from January 1st 2018 to December 31st 2019 at Sun Yat-sen University Cancer Center (SYSUCC) were reviewed. Patients (n = 217) identified with tumor relapse during follow-up were included for analyses. Hyper-relapse disease (HRD) is defined as tumor relapse within 6 months from surgery, multiple intrahepatic lesions, as well as macrovascular invasion and/or extrahepatic metastasis. Kaplan–Meier method and Cox regression model were used to analyze overall survival (OS). Risk factors for HRD were explored using logistic regression analysis. External validation was performed using data from another center (n = 270).
Results: In SYSUCC cohort, 66 (30%) encountered HRD, 118 (54%) had non-HRD early recurrence (ER), and 33 (16%) had late recurrence (LR). The HRD group had shorter OS than the non-HRD ER and the LR groups (P < 0.001). COX analysis identified HRD and PIVKA-II > 1000 mAU/mL as risk factors of poorer OS. Intriguingly, local therapy (HR [95% CI]: 0.528 [0.290– 0.961]) was associated with better OS in contrast to systemic therapies (HR [95% CI]: 1.120 [0.596– 2.107]) after tumor relapse (p = 0.001). Logistic regression analysis identified microvascular invasion and HBV infection as independent factors associated with HRD. The worse outcome of the HRD group was validated in the external cohort, compared with the non-HRD ER group (P < 0.001).
Conclusion: HRD is a special pattern of HCC relapse with poor prognosis after curative hepatectomy. Appropriate local therapy might improve patient survival after tumor relapse.
Keywords: hyper-relapse disease, HRD, hepatocellular carcinoma, HCC, curative hepatectomy, prognosis
Introduction
Liver cancer is the sixth most common cancer and the third cause of cancer-related death worldwide. As the most common type in liver cancer, hepatocellular carcinoma (HCC) accounts for 75–85% of cases of primary liver cancer.1 For early-stage HCC, Surgical treatment is preferentially recommended, including hepatectomy, orthotopic liver transplantation, and ablation.2–4
Although hepatectomy is thought to be a mainstream curative option, tumor relapse is quite common after surgery.5 Generally, tumors relapses of HCC are divided into early recurrence (ER) and late recurrence (LR), using 2 years after hepatectomy as the demarcation point.6 Previous studies reported that patients with ER had better survival than those with LR.7–9 A mainstream account for this phenomenon is occult micro-metastasis derived from the original tumor, which is associated with aggressive cancer features such as larger tumor size, multiclonality, microvascular invasion and poor histopathological differentiation.10
However, a demarcation point of two years seems to be insufficient to level out some extremely malignant cases. In clinical practices, we have noticed that quite a few HCC relapses are featured by super rapidity (within 6 months after LR) and multifocality (intrahepatic and/or extrahepatic), in spite of radical excision confirmed by pathological and post-operative imaging. Empirically, this type of patients are prone to have an even worse prognosis.
Here, we proposed hyper-relapse disease (HRD) as a new pattern of HCC relapse. We aimed to identify and validate the impact of HRD on patient outcome, and to screen out factors associated with HRD and long-term survival.
Materials and Methods
Study Population
This study was approved by the SYSUCC ethics committee (B2023-579-01) and conducted according to ethical guidelines of the Declaration of Helsinki. This study is a retrospective study, and the exemption of informed consent has been applied. The exemption of informed consent will not have adverse effects on the health and interests of the subjects. Medical records of patients who underwent curative LR as initial treatment of HCC between January 1st 2018 and December 31st 2019 at the Sun Yat-sen University Cancer Center (SYSUCC) were reviewed, and patients identified with tumor relapse during follow-up were included for analyses (SYSUCC cohort).
The inclusion criteria of patients were as follows: (1) age 18–80 years; (2) clinically diagnosed as liver cancer, according to AASLD and CNLC guidelines;3,4 (3) Barcelona Clinic Liver Cancer (BCLC) stage 0 to B; (4) underwent curative hepatectomy. Hepatectomy was considered to be curative according to the following criteria:11 (1) no local or distant metastasis based on pre- and intra-operative evaluation; (2) resection margin >1 cm or no residual tumor cells were found histologically at resected cross section; (3) no new lesion was identified by at least two scans of ultrasound scan, CT scan or MRI within 2 months after surgery; (4) serum alpha-fetoprotein (AFP) levels were restored to normal within 2 months after surgery. The exclusion criteria of patients were as follows: (1) not pathologically diagnosed as HCC; (2) combined with other malignancies; (3) previously received anti-tumor therapy before hepatectomy; (4) data insufficiency. Patients’ demographic characteristics, pathological findings, laboratory results and imaging data were obtained from the medical record system and database of SYSUCC.
External validation was conducted using dataset of patients with ER from Guangxi Medical University Cancer Hospital between January 1st 2018 and December 31st 2019. Of which, 270 patients who met the inclusion and exclusion criteria of our study were collected as the validation cohort. The identical dataset of Guangxi Medical University Cancer Hospital was once reported in a study analyzing the different types of recurrent HCC.12
Definition of HRD
The definition of HRD must meet the following conditions at the same time: (1) relapses occurred within 6 months since radical hepatectomy; (2) relapse appeared as multiple intrahepatic lesions (n ≥ 3); (3) relapse appeared with macrovascular invasion and/or extrahepatic metastasis. All the above criteria are based on imaging diagnosis and patients with tumor relapse were then divided into the HRD and the non-HRD groups (Figure 1).
 |
Figure 1 Flowchart of patient inclusion in initial cohort and validation cohort. |
Study Outcomes
The primary outcome was overall survival (OS), which was defined as the time from liver resection to death of any cause or the last follow-up. The secondary outcome was post-relapse survival, which was defined as the time from tumor relapse to death of any cause or the last follow-up.
Follow-Up
Patients were monitored after hospital discharge with routine blood test, serum AFP and PIVKA-II, liver function tests, HBV-DNA load and imaging examinations, including contrast-enhanced computed tomography (CT) and/or magnetic resonance imaging (MRI) regularly. Generally, patients were followed up firstly during 4–6 weeks since hepatectomy to confirm the radical of surgery, then every 2–3 months for the following 2 years, and then every 3–6 months. Tumor relapse was defined by the appearance of new intrahepatic and/or extrahepatic tumor(s) possessing classical imaging features consistent with HCC on surveillance contrast-enhanced CT and/or MRI. For those who had uncertain findings on surveillance imaging examinations, histopathological biopsy would be performed to confirm a final diagnosis.
Statistics
Continuous variables were expressed as median (interquartile range [IQR]). Categorical variables were presented as number (n) with frequency (%). Comparison of continuous variables was performed with Student’s t test when applicable; otherwise, the Mann–Whitney U-test was adopted. Categorical variables were compared with chi-square test or the Fisher’s exact test, as appropriate. Propensity scores were computed based on a logistic regression model including, MVI, tumor size, AFP, ALBI. Patients of the HRD and the non-HRD groups were then matched in a 1:2 ratio using the Matching algorithm with a caliper of 0.02 without replacement. Overall survival (OS) curves of the patients were calculated using the Kaplan–Meier method and differences of the curves were compared with the Log rank test. Univariable and multivariable Cox proportional hazard regression analyses were performed to assess predictors of OS among the whole studied population. Clinicopathological factors potentially contributing to HRD following LR were evaluated by means of logistic regression analysis. All data analyses were carried out using IBM SPSS software version 24.0. Statistical plots were produced using ggplot package, R version 4.1.2. A two-tailed P value less than 0.05 was considered to be statistically significant.
STROCSS Criteria Statement
This work has been reported in line with the strengthening the reporting of cohort, cross-sectional and case–control studies in surgery (STROCSS) criteria.13
Results
The Prevalence of HRD
Overall, 579 patients met the criteria. With a median follow-up time of 59.4 months (range: 57.3 to 61.5 months), 217 (37.5%) were observed with tumor relapse (Figure 1). Specifically, 66 (30.4%) patients were categorized into the HRD group, while 118 (54.4%) cases had non-HRD ER and 33 (15.2%) had LR. The prevalence of HRD was 11.4% (66/579) after curative hepatectomy.
Patient Characteristics
Characteristics of SYSUCC cohort are shown in Table 1. Before propensity score matching (PSM), the HRD group were characterized by higher ratio of female, MVI and HBV positivity, larger tumor size, elevated baseline AST and AFP levels than the non-HRD arm. After PSM, 61 patients from the HRD group and 89 patients from the non-HRD group were successfully matched. Patient Characteristics of the two groups were then well balanced (Table 1).
 |
Table 1 Baseline Characteristics of the Study Population |
In the validation cohort, the HRD group was characterized by higher ratio of MVI, increased tendency of blood transfusion, larger tumor size, elevated baseline AST and AFP levels, as well as larger proportion of advanced cases than the non-HRD arm. After PSM, 31 patients from the HRD group and 55 patients from the non-HRD group were successfully matched (Table S1).
Patient Survival
In SYSUCC cohort, the HRD group had significantly poorer OS than the non-HRD group (before PSM: the 1-year, 3-year and 5-year OS rates were 81.5% vs 97.5%, 63.1% vs 80.9%, 50.2% vs 68.9%, P = 0.003; after PSM: the 1-year, 3-year and 5-year OS rates were 81.7% vs 97.8%, 63.5% vs 79.4%, 49.6% vs 66.6%, P = 0.015), as demonstrated in Figure 2. The LR group had an even better OS than the non-HRD ER group (the 1-year, 3-year and 5-year survival rates are 97%, 97%, 90.8%, respectively, Figure 2A).
 |
Figure 2 Kaplan–Meier curves depicting the comparison of overall survival between patients with and without hyper-relapse disease (HRD) in initial cohort. (A) before propensity scores matching (PSM). (B) after PSM. |
In the validation cohort, the 1-year, 3-year and 5-year OS rates of HRD group were also significantly inferior to the non-HRD group (before PSM: 56.4% vs 88.7%, 20.2% vs 55.9%, 0% vs 49.4%, P < 0.001; after PSM: 67.7% vs 88.9%, 22.1% vs 53.7%, 0% vs 51%, P < 0.001), seen in Figure 3.
 |
Figure 3 Kaplan–Meier curves depicting the comparison of overall survival between patients with and without hyper-relapse disease (HRD) in validation cohort. (A) before propensity scores matching (PSM). (B) after PSM. |
Cox Regression Analyses
In SYSUCC cohort, multivariate COX analyses identified HRD and PIVKA-II >1000 as independent risk factors associated with poorer OS (HRD: hazard ratio [HR], 2.300; 95% CI, 1.351–3.916; p = 0.002, PIVKA-II >1000: HR, 1.628; 95% CI, 1.015–2.786; p = 0.044). Of note, post-relapse local therapy was associated with better OS (HR, 0.528; 95% CI, 0.290–0.961), in contrast to systemic therapy (HR [95% CI]: 1.747 [0.861–3.544], P = 0.001), seen in Table 2.
 |
Table 2 Univariate and Multivariate Cox Analyses for Overall Survival |
In the validation cohort, multivariate COX analyses revealed HRD, MVI and age <60yr were associated with poor OS (HRD: hazard ratio [HR], 2.349; 95% CI, 1.510–3.656; p < 0.001, age <60yr: HR, 1.767; 95% CI, 1.150–2.715; p = 0.009; MVI: HR, 2.130; 95% CI, 1.071–4.235; p = 0.031), while post-relapse local therapy predicted better OS (HR, 0.630; 95% CI, 0.443–0.897; p = 0.010), shown in Table S2.
Post-HRD Treatment
As mentioned above, patterns of post-relapse treatment might lead to distinct outcomes. Thus, we made further analyses in the subset of HRD patients. Patients who received local therapy had better OS and PRS than non-treatment group (P = 0.047 and 0.047), while those who received systemic therapy had poorer OS and PRS (P = 0.650 and 0.480, Figure 4). The 3-year OS rates are 36.4%, 50% and 72.3% for patients who received systemic treatment, no treatment and local treatment, respectively (overall P = 0.004). The 3-year PRS rates were 27.3%, 0% and 69.3% for patients who received systemic treatment, no treatment and local treatment, respectively (overall P = 0.004).
 |
Figure 4 Kaplan–Meier curves depicting the comparison of overall survival and post relapse survival among HRD patients who received different post-relapse management in initial cohort. (A) overall survival. (B) post relapse survival. |
In the validation cohort, only one patient received systemic therapy. Patients who received local therapy had better PRS than those received no treatment (P = 0.042). Although there is no difference on OS, a trend towards longer overall survival was observed in patients with local therapy (P = 0.430, shown in Figure 5). The 3-year PRS rates are 23.5% and 0% for patients who received local treatment and no treatment, respectively (Figure 5). The 3-year OS rates are 31.6% and 5.3% for patients who received local treatment and no treatment, respectively.
 |
Figure 5 Kaplan–Meier curves depicting the comparison of overall survival and post relapse survival between HRD patients who received different post-relapse management in validation cohort. (A) overall survival. (B) post relapse survival. |
Predictors for HRD
In SYSUCC cohort, multivariate logistic regression analyses revealed that MVI (odds ratio [OR], 3.054; 95% CI, 1.545–6.063; P = 0.001) and increasing preoperative AST (OR, 1.024; 95% CI, 1.008–1.040; P = 0.003) were independent factors associated with HRD (Table 3). Conversely, HBV positivity (OR, 0.290; 95% CI, 0.135–0.626; P = 0.002) was associated with lower risk of HRD.
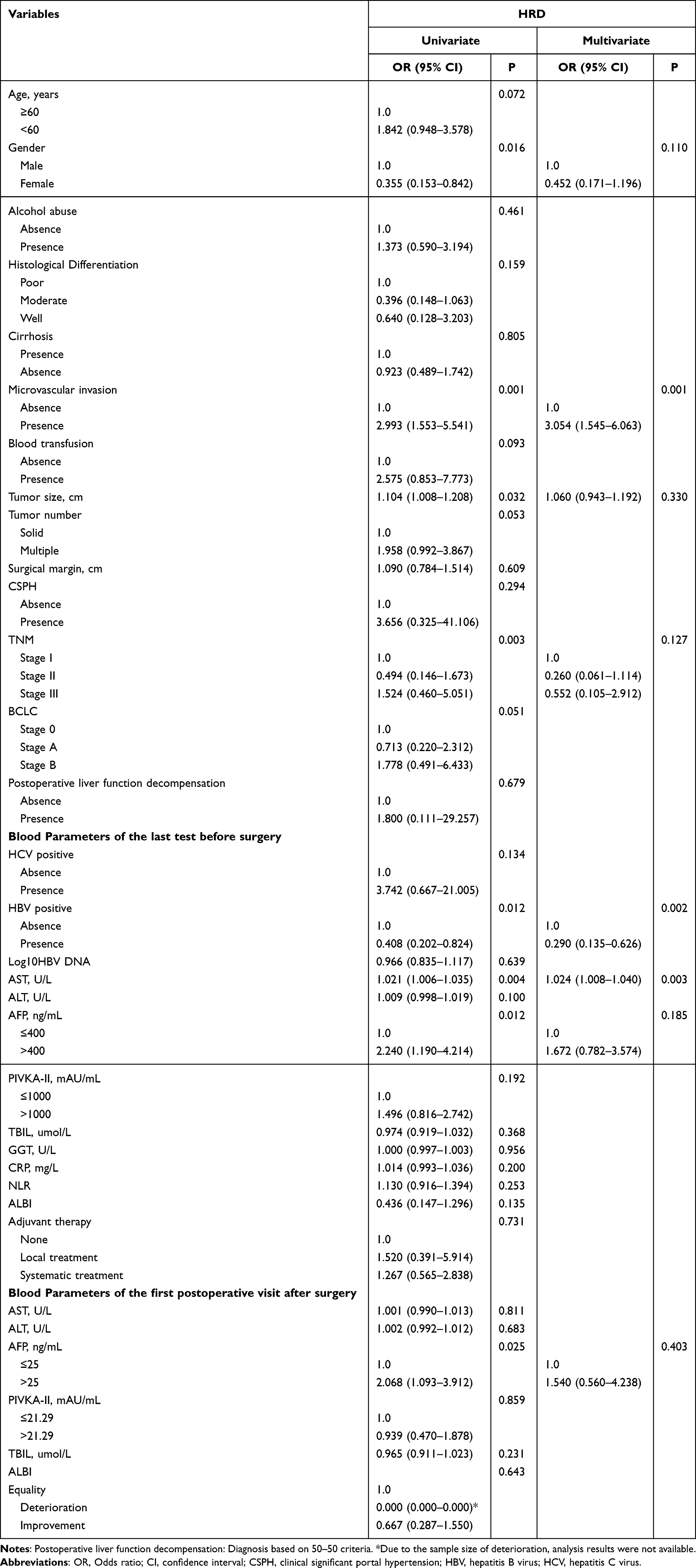 |
Table 3 Logistic Regression Analyses for Hyper-Relapse Disease (HRD) |
In the validation cohort, MVI (odds ratio [OR], 3.660; 95% CI, 1.441–9.300; P = 0.006) and lager tumor size (OR, 1.149; 95% CI, 1.058–1.247; P = 0.001) were independent factors associated with HRD (Table S3).
Discussion
Here, we proposed a novel concept, hyper-relapse disease (HRD), for the identification of a specific group of HCC patients who were susceptible to rapid tumor relapses leading to poor prognosis. Prior to the present study, there were already some recognitions which depicted refractory and rapid-developing characteristics of HCC, including early recurrence and hyper-progressive disease (HPD).7–10,14 Although early recurrence was known as a predictor for lower OS and extensively used in clinical practices, the conventional cut-off value of 2 years still has deficiencies because a small minority of relapses occurred much earlier following curative hepatectomy.7,8,15 Recently, the concept of very early recurrence (VER) was introduced to ICC, which is defined as recurrence within 6 months after initial resection.16 The study determined 6 months as the threshold based on their previous study, which noted that approximately one-quarter of patients with ICC had VER. Referring to this standard, it is estimated that approximately one-fifth of HCC patients developed VER after curative LR, albeit the inherently shorter recurrence-free period of ICC than HCC.15 Previous study document that a similar concept of hyper-progression recurrence (HPR) is correlated with the worst survival benefits, which is characterized by multinodular early recurrence (within 2 years) together with higher biological malignancy.12 The study defined HPR based on the quantity and location of recurrent nodules (numerous >5 intrahepatic nodules with macrovascular invasion and/or extrahepatic recurrence). However, the definition is limited as more importance is attached to the spatial distribution of tumor relapse, while temporal rapidity is not considered. In this case, it is difficult to screen out those patients with extremely malignant tumors who tend to recur both temporally and spatially aggressively. Another study proposed a definition of early explosive recurrence (EER), which refers to the appearance of more than 3 tumors involving more than 3 segments of the liver within 6 months after surgery.17 The median overall survival time of EER patients was 16.9 months, and tumor size, number, MVI, and high expression of GPC3 were important risk factors for EER. However, this definition only focuses on intrahepatic recurrence but does not refer to extrahepatic metastasis. Of note, we noticed that a fraction of HCC relapses was featured with both temporal rapidity and spatial multifocality, which were nightmare of both surgeons and patients. Henceforth, it is of great potential to explore effective predictor factors to indicate HRD for timely and tailored therapeutic regimen designing.
In this study, among 579 HCC cases who had BCLC stage 0-B disease and underwent curative hepatectomy, 11.4% suffered from HRD. To our knowledge, it is the first to report the prevalence of HRD in early and intermediate stage of HCC who received curative hepatectomy. To validate the prognostic value of HRD from other early recurrence cases, we set those who had non-HRD early relapse as the control group instead of patients with no relapse. Not surprisingly, patients of the HRD group indeed had the significantly poorest OS, and the patients of late recurrence group had best prognosis (Figure 2A and B).
Multivariate Cox regression analyses revealed that patients with HRD and PIVKA-II >1000 were the only predictors for worse OS, while post-relapse local therapy was the only independent protective factor, with HR of 2.300, 1.628 and 0.528, respectively. While in the validation cohort, patients with HRD, MVI and age <60yr were the only predictors for worse OS, and post-relapse local therapy was the only independent protective factor, with HR of 2.349, 2.130, 1.767 and 0.630, respectively. Although tumor size and serum AFP level are known as important prognostic factors for HCC patients’ survival,15,18 they were not identified as independent factors for OS in this study. Instead, the independent risk factors for HRD only included MVI, absence of HBV and elevated AST in SYSCC cohort. However, considering that the OR of AST is only 1.024, we think it has no clinical significance, and there is no correlation between AST, HBV and MVI (P = 0.078 and 0.381, respectively) that would affect the outcome. While in validation cohort, the independent risk factors for HRD only included MVI, and lager tumor size. However, MVI as an expected risk factor has limited utility for preoperative patient selection. Thus, there is an urgent need on more preoperative indicators and more depth to the molecular mechanism research of HRD. In addition, the conclusions in our initial cohort and validation cohort were slightly different, which may be due to the difference in baseline between the two groups of patients. Meanwhile, as a retrospective study, the conclusions need to be further verified.
In subgroup analyses of both cohort, post-relapse local therapy were significantly associated with improved PRS of HRD patients, the patients who received local treatment had better survival compared with those treated with basic supportive care. However, post-relapse systemic therapy could not significantly affect prognosis of HRD patients, and the prognosis of post-relapse systemic therapy was even worse than that of with just basic supportive care in the early stage. This might be attributed to the fact that tumors with HRD are highly aggressive, while systemic treatments typically take effect slowly. Thus, when patients present with HRD, local treatment should be administered actively. The reasons some patients receive only supportive care after relapse can be attributed to the following factors: (1) The relapse is more extensive, leading patients and their families to lose confidence in further treatment and opt to discontinue it; (2) Many liver cancer patients in China face financial difficulties and cannot afford the cost of additional treatment; (3) Relapsed patients often have impaired liver function, making them unable to tolerate aggressive treatment; (4) It is a common challenge across various patient groups in China, not unique to liver cancer patients.
Furthermore, we speculate that some extremely aggressive phenotypes of HCC cells and/or microenvironment underlying the occurrence of HRD, which calls for in-depth investigation of mechanisms and translation into therapeutic strategy. Additionally, surgery as a stress may activate or aggravate the genetic abnormalities of underline HRD, resulting in insensitivity to subsequent treatment. Although the current data is not sufficient to instruct clinical practice, it holds great appeals for further exploration regarding its underlying molecular mechanisms, which may provide profound insights into distinguishing patients with this pattern.
Limitations
First, this is a retrospective study, and most patients were HBV-related HCC. Our findings need to be verified in patients with other etiology. Second, a relatively small sample size hurts the reliability of subgroup analysis, and different treatment strategies for HCC with HRD or non-HRD need further investigation.
Conclusion
Patients with HRD are a refractory subtype of HCC with poor prognosis after curative hepatectomy. MVI and absence of HBV were predictors of HRD, and post-relapse local therapy was associated with better OS in patients with recurrent HCC.
Provenance and Peer Review
Not commissioned, externally peer-reviewed.
Funding
This work was funded by the National Natural Science Foundation of China (82372981); Cancer Innovative Research Program of Sun Yat-sen University Cancer Center (CIRP-SYSUCC-0030).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Galle PR, Forner A, Llovet JM. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
3. Xie D-Y, Ren Z-G, Zhou J, Fan J, Gao Q. 2019 Chinese clinical guidelines for the management of hepatocellular carcinoma: updates and insights. Hepatobiliary Surg Nutr. 2020;9(4):452–463. doi:10.21037/hbsn-20-480
4. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
5. Okada S, Shimada K, Yamamoto J. Predictive factors for postoperative recurrence of hepatocellular carcinoma. Gastroenterology. 1994;106(6):1618–1624. doi:10.1016/0016-5085(94)90419-7
6. Ding X, He M, Chan AWH, et al. Genomic and epigenomic features of primary and recurrent hepatocellular carcinomas. Gastroenterology. 2019;157(6):1630–1645.e1636. doi:10.1053/j.gastro.2019.09.005
7. Portolani N, Coniglio A, Ghidoni S, et al. Early and late recurrence after liver resection for hepatocellular carcinoma: prognostic and therapeutic implications. Ann Surg. 2006;243(2):229–235. doi:10.1097/01.sla.0000197706.21803.a1
8. Wang MD, Li C, Liang L, et al. Early and late recurrence of hepatitis B virus-associated hepatocellular carcinoma. Oncologist. 2020;25(10):e1541–e1551. doi:10.1634/theoncologist.2019-0944
9. Kobayashi T, Aikata H, Kobayashi T, Ohdan H, Arihiro K, Chayama K. Patients with early recurrence of hepatocellular carcinoma have poor prognosis. Hepatobiliary Pancreat Dis Int. 2017;16(3):279–288. doi:10.1016/S1499-3872(16)60181-9
10. Wu JC, Huang YH, Chau GY, et al. Risk factors for early and late recurrence in hepatitis B-related hepatocellular carcinoma. J Hepatol. 2009;51(5):890–897. doi:10.1016/j.jhep.2009.07.009
11. Wen T, Jin C, Facciorusso A, et al. Multidisciplinary management of recurrent and metastatic hepatocellular carcinoma after resection: an international expert consensus. Hepatobiliary Surg Nutr. 2018;7(5):353–371. doi:10.21037/hbsn.2018.08.01
12. Qi LN, Ma L, Wu FX, et al. Clinical implications and biological features of a novel postoperative recurrent HCC classification: a multi‐centre study. Liver Int. 2022;42(10):2283–2298. doi:10.1111/liv.15363
13. Mathew G, Agha R, Albrecht J, et al. STROCSS 2021: strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int J Surg. 2021;96:1.
14. Champiat S, Dercle L, Ammari S, et al. Hyperprogressive disease is a new pattern of progression in cancer patients treated by Anti-PD-1/PD-L1. Clin Cancer Res. 2017;23(8):1920–1928. doi:10.1158/1078-0432.CCR-16-1741
15. Tabrizian P, Jibara G, Shrager B, Schwartz M, Roayaie S. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Annals Surg. 2015;261(5):947–955. doi:10.1097/SLA.0000000000000710
16. Tsilimigras DI, Sahara K, Wu L, et al. Very early recurrence after liver resection for intrahepatic cholangiocarcinoma: considering alternative treatment approaches. JAMA Surg. 2020;155(9):823–831. doi:10.1001/jamasurg.2020.1973
17. Yan K, Dong W, Li X, et al. Early explosive recurrence of hepatocellular carcinoma after radical resection: risk factors and clinical significance. Cancer Screen Prevent. 2023;2(4):238–249. doi:10.14218/CSP.2023.00037
18. Liang L, Wang MD, Zhang YM, et al. Association of postoperative biomarker response with recurrence and survival in patients with hepatocellular carcinoma and high alpha-fetoprotein expressions (>400 ng/mL). J Hepatocell Carcinoma. 2021;8:103–118. doi:10.2147/JHC.S289840
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systemic Inflammation Response Score for Prognostic Prediction in Hepatocellular Carcinoma Patients After Hepatectomy
Zhang D, Huo L, Pan Y, Yang Z, Zeng H, Wang X, Chen J, Wang J, Zhang Y, Zhou Z, Chen M, Hu D
Journal of Inflammation Research 2022, 15:6869-6881
Published Date: 29 December 2022
Liver Regeneration-Related Genes of Nontumor Liver Tissues Predict the Prognosis of Patients with Hepatocellular Carcinoma
Xu Y, Li Y, Lu Y, Wang W, Lian Z, Wu Z, Li B, Yu D
Journal of Hepatocellular Carcinoma 2023, 10:2197-2209
Published Date: 7 December 2023