")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 17
Illness Burden and Unmet Patient Needs in Giant Cell Arteritis: Current State and Future Prospects
Authors Sattui SE, Corral M, O'Donnell DC
Received 15 January 2025
Accepted for publication 28 May 2025
Published 1 July 2025 Volume 2025:17 Pages 117—134
DOI https://doi.org/10.2147/OARRR.S517664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Sebastian E Sattui,1 Mitra Corral,2 Dannielle C O’Donnell2
1Division of Rheumatology and Clinical Immunology, University of Pittsburgh, Pittsburgh, PA, USA; 2Genentech, Inc, South San Francisco, CA, USA
Correspondence: Dannielle C O’Donnell, Genentech, Inc, South San Francisco, CA, USA, Email [email protected]
Abstract: Giant cell arteritis (GCA) is the most common form of primary systemic vasculitis and primarily affects large- and medium-sized vessels. Diagnostic delay can occur from underrecognition of symptoms, and optimal treatment duration remains unclear. Patients with GCA can experience significant burdens related to adverse outcomes of GCA, including risk of vision impairment/loss and stroke, which can result in permanent disability. Glucocorticoids, which remain the first line of treatment, are often associated with adverse effects, and emerging glucocorticoid-sparing agents represent an important option for the treatment of this relapsing disease. Moreover, GCA is a costly illness in terms of both direct healthcare spending and healthcare resource utilization. This narrative review summarizes the clinical, psychosocial, and economic burdens of illness as well as the unmet needs of patients with GCA in terms of diagnosis, treatment, and healthcare resource utilization and spending. Reducing delays in diagnosis and making informed treatment decisions that optimize patient response, while minimizing exposure to potential adverse events, can lead to significant improvement in patient care and outcomes.
Keywords: giant cell arteritis, large vessel vasculitis, glucocorticoids, healthcare costs, quality of life
Background
The pathophysiology of giant cell arteritis (GCA) is complex and multifactorial, involving a predisposing genetic background, the role of immune aging, and the activation of vascular dendritic cells by an unknown trigger (Figure 1).1 GCA, a chronic inflammatory disease affecting large and medium-sized arteries, is believed to be an autoimmune disorder where the body’s immune system mistakenly attacks healthy blood vessels, leading to inflammation and potential complications like vision loss.1 GCA involves a predilection for the cranial branches of the carotid artery as well as the subclavian and axillary branches of the aorta and is the most common form of primary systemic vasculitis.1 Inflammation of the arterial wall leads to vascular remodeling, which can result in narrowing of the blood vessels and subsequent ischemia or increase the risk for aneurysm formation. Ischemic events such as optic neuropathy, scalp necrosis, stroke, and (if untreated) potentially irreversible vision loss can result, making accurate and timely diagnosis and treatment crucial.1,2 Polymyalgia rheumatica (PMR), an inflammatory disease characterized by shoulder and pelvic girdle pain and stiffness, can be associated with GCA, and both conditions may be manifestations of a common disease spectrum.3 Patients with GCA are also at a higher risk of myocardial infarction, aortic aneurysm, and peripheral artery disease.4
 |
Figure 1 Pathophysiology of giant cell arthritis. |
GCA primarily occurs in individuals aged 50 years and older, with peak prevalence occurring in individuals between 70 and 80 years of age.4,5 The pooled incidence has been reported at 10.00 cases per 100,000 people over age 50, and the pooled prevalence at 51.74 cases per 100,000 people over age 50.6 Although a higher prevalence has been reported in Caucasians of Scandinavian ancestry,6 GCA has been reported in all ethnic and racial groups globally.7
For almost 70 years, GCA was treated primarily with glucocorticoids. For uncomplicated GCA, the glucocorticoid starting dose recommended by the American College of Rheumatology is 1 mg/kg (up to 80 mg/day)8 and the starting dose recommended by the European Alliance of Associations for Rheumatology is 40–60 mg/day.9 Despite these recommendations, patients with uncomplicated GCA are prescribed higher doses of glucocorticoids at initial treatment.4,5,8,10 The advent of novel biologic and nonbiologic agents represents new treatment options that could minimize patient exposure to glucocorticoids and their potential adverse effects such as weight gain, skin atrophy, glaucoma, and osteoporosis as well as cardiometabolic and neuropsychiatric complications.4,11
Despite advances in treatment, GCA is associated with a significant illness and economic burden, and several unmet needs remain to date (Figure 2). To that end, this narrative review aims to summarize the clinical, psychosocial, and economic burden of illness and unmet needs of patients with GCA by exploring aspects of diagnostic delay, treatments, costs of complications, health insurance implications, and healthcare resource utilization (HCRU) findings.
 |
Figure 2 Burden of giant cell arteritis and unmet needs. |
For this narrative review, a search was conducted in PubMed and the Cochrane Library (including the Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, and Health Technology Assessments) from the inception of each database through August 2023. In addition, a manual search was conducted and a bibliography of selected publications was reviewed as part of a comprehensive search on the topic.
The search was conducted to address the clinical, psychosocial, and economic burden of GCA. The targeted search was conducted using key search terms related to GCA, clinical burden, epidemiology, mortality, treatments, economics, cost, and quality of life. Titles and abstracts were initially screened by one reviewer to determine their suitability for inclusion. A full-text review was then conducted to select the final list of articles to be included in the review. For topics addressing the burden of GCA, observational studies were considered for review. For topics addressing treatment options, randomized controlled trials (RCTs) were included. When RCTs were not available, observational studies (cohort and case‐control studies) that reported on patient‐important outcomes for the interventions were included. In the absence of comparative data, case series that presented patient outcomes for the interventions were considered.
Excluded studies included those with an irrelevant population, intervention, or outcome; studies that had no primary data (eg, letters, opinion pieces, and commentaries); and narrative reviews. Further, only English-language studies were considered in this review.
Findings
Patient Burden of Illness
Mortality
The burden of illness for patients with GCA is significant given its high morbidity (particularly the risk of vision impairment/loss and stroke) and the adverse effects that result from treatment, specifically the long-term exposure to high-dose glucocorticoids. The worldwide disease burden of GCA is predicted to be sizable by the year 2050, with a global prevalence estimated at 3 million people, including approximately 500,000 who will experience vision impairment.2 In the United States (US), the estimated age- and sex-adjusted prevalence is 204 per 100,000 persons aged 50 and older, with a predicted total number of 943,690 incident cases by 2050.2,12 By 2050, US expenditures on GCA are estimated to be more than $76 billion for the management of vision impairment and approximately $6 billion for the management of glucocorticoid-induced fractures.2
Patients with GCA have an elevated risk of death compared with individuals without GCA. To date, findings on the life expectancy of patients with GCA are conflicting. A population-based cohort study in Denmark found that, compared with the general population, patients with GCA had an almost 50% increased risk of mortality (relative risk [RR] 1.49, 95% CI 1.36–1.46) during the 1 year following the index date (ie, date of the third prednisolone prescription).13 A similar trend was observed in a Canadian cohort, where mortality rates of patients with GCA increased over a 19-year period, while mortality rates in the general population fell significantly.14 Further, a retrospective analysis of more than 7000 patients with GCA found an elevated risk of mortality in the first 2 years postdiagnosis (hazard ratio [HR] 1.14, 95% CI 1.04–1.25) and more than a decade after diagnosis (HR 1.14 [95% CI 1.02–1.30]).15 However, a cohort study using the United Kingdom (UK) primary care database showed that, in comparison with age-matched controls, patients with GCA had increased mortality during the first year following diagnosis (adjusted HR 1.51, 95% CI 1.40–1.64) and marginally increased mortality between 1 and 5 years after the diagnosis (adjusted HR 1.16, 95% CI 1.09–1.23) but not >5 years after the diagnosis.16 A systematic literature review comprising 17 studies reported that long-term mortality was not increased in patients with GCA ascertained from a population base (mortality ratio, 1.03, 95% CI 0.96–1.10) but was increased in patients ascertained from a hospital setting (mortality ratio, 1.61, 95% CI 1.19–2.19).17
Disease and Treatment-Related Comorbidities
Patients with GCA are burdened by an increased vulnerability to significant adverse outcomes and comorbid conditions that are potentially disabling, often chronic, and require intervention (and thus increase HCRU and spending). These adverse outcomes primarily include vision impairment, including blindness (potentially irreversible); stroke, aortic dissections, and other ischemic events; and serious infections.5,11,18 The most common comorbidities in a large cohort of Medicare (n=734) and commercial insurance beneficiaries (n=1022) with GCA were hypertension (80% and 72%), hyperlipidemia (71% and 61%), cancer (38% and 24%), coronary artery disease (34% and 25%), and diabetes (34% and 31%), respectively.19
Up to 30% of patients with GCA experience permanent vision loss, usually related to arteritic anterior ischemic optic neuropathy.20,21 Patients with GCA also have an elevated risk of cardiovascular disease.5,22 An observational cohort study using the UK primary care database reported that compared with age- and sex-matched reference participants, GCA patients had an increased risk [incidence rates per 1000 person-years] of myocardial infarction [10.0 vs 4.9], cerebrovascular accident (CVA) [8.0 vs 6.3], and peripheral vascular disease [4.2 vs 2.0].23 Further, a meta-analysis reported a significantly increased risk of CVA among patients with GCA; the pooled risk ratio of CVA in patients with GCA versus non-GCA controls was 1.40 (95% CI: 1.27–1.56).24 However, an increased risk of coronary artery disease among patients with GCA was not observed.25
Arterial dilation and aneurysms are long-term complications of GCA, and patients with GCA have a higher risk of developing aneurysms and aortic dissections than the general population.18 Further, patients with GCA who develop vascular complications are at increased risk of mortality compared with the general population or with patients with GCA without vascular complications.18
Patients with GCA also have an elevated risk of serious infections. A study among individuals with GCA reported that the incidence rate of serious infections (defined as bacterial or viral infections requiring hospitalization based on primary inpatient diagnosis code) per 100 person-years was 10.7 for the Medicare beneficiaries and 6.3 for the commercial insurance beneficiaries.19 Despite improved treatment of patients with GCA, a large analysis of claims data using the National Inpatient Sample from 1998 to 2016 in the US has shown that the incidence of serious infections, including sepsis, has increased over time in patients with GCA.26
Many patients with GCA require ongoing treatment with high-dose glucocorticoids for disease control. Most patients receive at least 2 years of glucocorticoid treatment and can taper off medication by 5 years postdiagnosis, although relapse—and thus reinitiation of glucocorticoid treatment—is common.11 As patients with long-term GCA are increasingly exposed to accumulating doses of glucocorticoids, their risk of treatment-related side effects/adverse effects also increases. As many as 86% of patients with GCA who rely on glucocorticoids for the long term to maintain disease will develop a glucocorticoid-related adverse event.2,11 These adverse events include increased risk of cardiovascular events (eg, hypertension), osteoporotic events, infectious complications, diabetes, weight gain, cataracts, and neuropsychiatric events (eg, cognitive impairment).2,11,27 Complications leading to loss of autonomy, including falls and fractures, have been frequently observed within the first 2 years after initiation of treatment for GCA.27 In a retrospective claims analysis of newly diagnosed patients with GCA (N=2497) from 2003 to 2012,28 the risk of adverse events increased by 3% for every 1000 mg of glucocorticoids prescribed, and for adverse events such as fracture, osteoporosis, cataracts, and glaucoma, the risk increased 3% to 5%. For patients previously undiagnosed with diabetes, every 1000 mg increase of glucocorticoids increased the risk of diabetes by 5%.28
Disease Recurrence
Because GCA is a relapsing and remitting condition—with relapse occurring in 34% to 84% of patients in clinical trials and 36% to 64% of patients in nonclinical, prospective, observational studies—patients require ongoing disease monitoring and management of side effects/adverse effects and complications, primarily in the first 2 years of initial treatment.29 Higher relapse rates have been observed in clinical trials that included a rapid glucocorticoid tapering schedule as part of the study design.20 Further, a population-based study showed that 40.8% of patients with GCA experienced relapses or recurrences.30 Relapse is difficult to predict and manage and requires further investigation, and questions remain surrounding relapse and the resultant higher cumulative doses of glucocorticoids. It is also unknown whether repeated relapses lead to greater morbidity, such as vascular stenoses or aortic aneurysms.29
Diagnostic Delays
With prompt and appropriate diagnosis, the risk of damage from GCA complications can be ameliorated. However, diagnosis of GCA can be challenging, and diagnostic delays increase the risk of devastating consequences such as permanent vision loss.31 While most patients with GCA experience systemic symptoms (80%), interpreting them can be challenging. Although most patients with GCA-related vision loss exhibit typical symptoms such as headache or jaw claudication, about one-fifth of patients with GCA who present with visual complications do not exhibit systemic symptoms, and even when patients do, they may have atypical features, such as normal inflammatory markers.32 Primary care physicians—who are the clinicians routinely seeing these patients—may not have a high level of suspicion for GCA, in part because the disease is relatively uncommon and also because symptoms such as weakness, headache, vision disturbance, and musculoskeletal dysfunction are prevalent in the primary care older adult population and can be secondary to other etiologies.33–35 Although cranial manifestations such as temporal headaches and scalp tenderness are the classic symptoms of GCA, some patients develop extracranial disease and atypical, nonspecific, or asymptomatic presentations that could be easily overlooked.33 Consequently, patients without cranial manifestations may experience an even greater delay in diagnosis than patients with the “classic” presentation.33 In one meta-analysis,35 the mean diagnostic delay from symptom onset to GCA diagnosis was 9 weeks, but the delay was nearly double (17.6 weeks; P < 0.001) in patients with extracranial involvement. Further, GCA shares pathophysiologic and clinical features with PMR, resulting in an overlap or mimicking of the 2 disorders that can make it difficult to disentangle these conditions.33
Age and Care of Older Adults with GCA
Patient age presents another challenge in terms of timely diagnosis and patient outcomes. GCA is primarily a disease of older individuals; patients are generally older than 50 years, with the average age of onset around 77 years and the risk of disease increasing with age.36–38 A meta-analysis showed that the mean diagnostic delay between symptom onset and GCA diagnosis was 9.0 weeks (95% CI, 6.5 to 11.4).35 In one of the few studies to examine the experience of GCA in adults 80 years and older, patients demonstrated signs and symptoms generally comparable to those seen in younger populations with GCA, such as vision disturbance, headache, jaw claudication, and scalp tenderness.34 However, older adults with GCA may experience a delay in diagnosis when symptoms are incorrectly attributed to normal aging.34 Another study reported a higher risk of ophthalmologic complications in adults with GCA 75 years and older.39 In a recent multicenter Italian study of 1004 patients with GCA, patients 80 years and older had a higher frequency of cranial symptoms and ischemic complications as well as an increased risk for blindness compared with younger patients.40 Blindness was observed in 37% of patients with GCA 80 years and older, compared with 18.2% of patients between 65 and 79 years old and 6.2% of patients 64 years and younger. Despite a higher incidence of complications, adults over 80 years received fewer immunosuppressive drugs.
Even when diagnosed accurately, older adults with GCA may manifest significant comorbidities requiring clinical intervention. In one retrospective study of publicly and commercially insured patients with GCA, rates of serious infection were significantly more common in a Medicare cohort than a MarketScan cohort (27.9% vs 7.2%), with older age at time of diagnosis (HR 1.03 [95% CI 1.01–1.05] and HR 1.04 [95% CI 1.02–1.06], respectively) and moderate/severe frailty (HR 2.51 [95% CI 1.38–4.57] and HR 4.54 [95% CI 1.44–14.29], respectively) at diagnosis being the highest risk factors for infections during follow-up.19 Similar observations were made in a recent multicenter Italian cohort where the risk of serious infections during the first year of follow-up was higher in patients 80 years and older (odds ratio [OR] 13.71 [95% CI 1.59–117.91]) and between 65 and 79 years (OR 11.90 [95% CI 1.69–83.63]) when compared with patients 64 years and younger.40 This increased risk of infections persisted even at 5-year follow-up.
Impact on Quality of Life
Patient-reported outcomes have shown the negative impact GCA can have on patient well-being and functioning. In a survey of nearly 700 patients with various types of systemic vasculitis, most patients with GCA reported experiencing depression (55%) and sleep disturbances (62%), and many also reported negative perceptions about their illness.41 In an analysis of 72 patients with GCA,42 about one-third had either probable anxiety or probable depression; older age was an independent predictor of higher scores for depression, and glucocorticoid use was an independent predictor of higher scores for anxiety.42 Further, increasing age was correlated with higher scores on the Hospital Anxiety and Depression Scale.42
Research from the UK and Australia suggests that GCA can exact a significant toll on patients’ lives, leading to difficulties maintaining functioning and/or activities of daily living in those with symptoms like pain and fatigue; substantial fears about future vision loss and other debilitating symptoms; impairments in social functioning and interpersonal relationships; and a negative sense of self, such as feeling guilty, anxious, and seeing oneself as not “normal”.43,44 However, treatment may improve quality of life (QOL) for some patients with GCA. Results from the Giant-Cell Arteritis Actemra (GiACTA) study showed a higher improvement in physical and mental domains of QOL (as measured by the 36-item Short-Form Health Survey Mental Component Summary [MCS] and Physical Component Summary scores) and decreases in fatigue among patients treated with tocilizumab (TCZ) plus prednisone (n=100) compared with those receiving placebo plus prednisone (n=101).45 Interestingly, scores from the treatment group were either comparable to or surpassed population age-matched norms by week 52. MCS-related QOL benefits were maintained in the 2-year long-term extension of GiACTA, where patients receiving TCZ demonstrated significantly better MCS scores at week 156 than patients taking placebo plus prednisone taper, even though all patients had reached clinical remission at week 52 and stopped receiving TCZ or glucocorticoid treatment.46
Economic Impact of GCA
Cost of GCA
To date, research on HCRU and costs among patients with GCA in the US is consistent, albeit limited, with the published literature indicating increased spending and resource use. One study of commercial and Medicare supplemental claims data (2008–2012 [before approval of TCZ]) from a cohort of patients with newly diagnosed GCA (n = 1293) found that the mean 1-year total inpatient, outpatient, and pharmacy costs for patients with GCA was $34,065, compared with $12,890 for controls—resulting in a $16,431 difference after adjusting for age, sex, comorbidity, health plan type, region, and calendar year.47 GCA was associated with more than $5000 in additional inpatient expenditures, more than $10,000 in additional outpatient expenditures, and $660 in additional pharmacy expenditures compared with matched controls.47 Data from outside the US are similar. In a sample from the French national healthcare system, the average first-year cost of incident GCA was estimated at €10,407.40.48 The incremental costs of GCA among patients in France have been largely attributed to expenses from inpatient care (40% of costs), medications (17%), and paramedical costs (16%).49
A population-based retrospective study of patients with GCA in Minnesota also found significantly greater HCRU with GCA versus matched controls over the first 5 years post-index (ie, each referent subject was assigned an index date corresponding to the GCA incidence date of their matched patient with GCA).50 Patients with GCA had more laboratory visit-days within the first 3 years post-index; more outpatient visit-days in years 0–1, 1–2, and 3–4; more radiology visit-days in years 0–1, 3–4, and 4–5; and more ophthalmologic procedures/surgery in years 0–1, 1–2, 2–3, and 4–5 versus matched controls.50 Spending was also higher; patients with GCA incurred higher total cumulative direct medical costs in the month immediately before diagnosis and annually for the first 4 years postdiagnosis compared with matched controls.50
Cost of Complications
In addition to the cost of clinic visits, radiologic evaluations, and medications to treat their GCA, these patients often incur significant expenses associated with the management of GCA complications and comorbidities such as stroke and cardiovascular disease. In Europe, the economic costs of blindness and moderate-to-severe vision impairment (broadly; not necessarily GCA-induced) among people aged 50 and older are substantial and thought to range from €25.83 billion to €56.52 billion.51 A recent meta-analysis estimated the cost of illness or stroke in the general population at $1809 to $325,108 in direct and indirect costs, mostly due to length of hospital stay.52 Stroke-related hospitalization in the general population has been suggested to cost patients between $20,396 and $43,652 on average.53 Other GCA comorbidities and complications that can result in significant spending include PMR, which incurs $2233 to $27,712 in annual direct medical costs in the general population;54 type 2 diabetes, which incurs $16,750 in annual direct medical costs in the general population;55 and cardiovascular disease, which incurs $18,953 per patient per year in direct medical care costs and $8114 per patient per year in inpatient costs in the general population.56 Data from the 2017 US National Readmission Database of adults aged 50 and older with GCA suggest that patients also may be susceptible to increased spending because of hospitalizations needed for reasons such as infection, cardiovascular disease, and glucocorticoid-related complications.57 Further, about one-third (34%) of patients may require readmission within 6 months of initial hospitalization.57
Healthcare spending associated with adverse events from glucocorticoid exposure also can be substantial.58 As noted previously, in the US the cost of managing GCA-related vision impairments is estimated to exceed $70 billion by 2050.2 Best et al (2019) found that among 1602 patients with GCA identified from MarketScan commercial and Medicare Supplemental databases who filled at least 1 prescription for glucocorticoids between 2009 and 2014, 36.5% experienced adverse events related to glucocorticoids; among patients taking the highest cumulative dose, 45.3% commercial beneficiaries experienced glucocorticoid-related adverse effects.58 The unadjusted mean 1-year potential costs related to treatment of glucocorticoid adverse events was $12,818.58 Increased cumulative glucocorticoid dose was associated with increased healthcare spending (P<0.001), with mean predicted costs rising from $4389 to $6609, depending on dose.58 For instance, patients taking a cumulative dose of glucocorticoids of >7200 mg over 1 year incurred $2220 more in adjusted mean costs than patients taking ≤ 2607 mg of glucocorticoids.58
Health Insurance Implications
The high cost of biologic therapy (eg, TCZ) may represent a significant healthcare access burden to most patients in countries without national healthcare (eg, the US), especially for patients who are uninsured or publicly insured.59 Cost burdens are particularly relevant to the population of patients with GCA because older adults often have limited incomes and may not be able to earn wages working outside the home (also potentially limiting their access to employer-provided insurance). For instance, in the US, TCZ with prednisone is substantially more expensive than treatment with glucocorticoids alone.60 The cost of TCZ 20 mg/mL IV solution ranges from $526.67 for 4 mL to $1302.42 for 10 mL to $2595.33 for 20 mL, whereas 162 mg/0.9 mL TCZ subcutaneous solution costs $1142.56.61 Even in countries with universal healthcare, patients with GCA may find themselves without resources to cover the costs of daily living—especially people who are not able to work and draw a livable income. A quantitative study of patients with GCA living in the UK noted patients’ difficulties with attaining government-funded disability payments (ie, Employment and Support Allowance) because the questionnaire used to determine eligibility does not sufficiently capture the symptoms of GCA and PMR.43
Cost burdens also result from polypharmacy,62 which is common in older adults.63 The 2017 Medical Expenditure Panel Survey found that among older adults with cardiovascular disease (N=1610), polypharmacy (ie, taking at least 5 medications) was associated with nearly double the total health care expenditures (198%) and triple the pharmacy-related costs (287%) as non-polypharmacy.64,65 Out-of-pocket costs can be high if multiple medications are required to treat hypertension, blood glucose dysregulation, dyslipidemia, and glaucoma that can result from glucocorticoid-induced adverse events. These costs not only burden individual patients, but also present an economic strain to the healthcare system and society.
Available Treatments and Unmet Treatment Needs
Some guideline-recommended treatments for patients with GCA, such as glucocorticoids, have good evidence for efficacy but may carry a high risk of adverse events.8 Other treatments are still preliminary or have largely been investigated only in case studies rather than RCTs (eg, leflunomide [LEF]). Consequently, an optimal treatment and treat-to-target disease management approach that maximizes symptom control and minimizes exposure to treatment-related adverse effects has remained elusive.66 There are also currently no US Food and Drug Administration (FDA)-approved monotherapies for GCA other than glucocorticoids.10
Glucocorticoids
Glucocorticoids have been the backbone of GCA management, mostly with prednisone 40 mg-60 mg/day, decreasing to 15 mg-20 mg/day for the first 2–3 months; with a goal of ≤5 mg/day after 1 year.4,5,10,11 In the setting of threatened vision loss, IV pulse glucocorticoids (ie, methylprednisolone 1000 mg) are still conditionally recommended.8 Glucocorticoids are highly effective at suppressing inflammation and preventing vision loss and ischemic organ damage.67 However, glucocorticoid use is associated with an elevated risk of cardiovascular, metabolic, and osteoporotic complications, as well as ocular toxicities, and this risk increases incrementally with exposure to higher doses and for a longer duration of treatment.2,11 Given the relapsing nature of GCA, repeated exposure to glucocorticoids for months or even years may be necessary to manage episodes of recurrence.28 Identifying an optimal treatment alternative to glucocorticoids, and educating healthcare providers about such alternative treatments, is critical in part because patient-reported outcomes suggest that patients with GCA often do not receive information about other treatment options.68 Moreover, patients report feeling uncomfortable, disempowered, and resigned about the adverse effects of glucocorticoids; some patients attempt to manage symptoms on their own rather than continue taking glucocorticoids.69
Glucocorticoid-Sparing Medications
There is a high level of interest in exploring glucocorticoid-sparing and immunosuppressive agents that could effectively treat GCA while minimizing glucocorticoid use and mitigating long-term glucocorticoid toxicity.4,5,10,11 Methotrexate is one of the potential disease-controlling therapeutics given its immunosuppressive effects and ability to reduce neutrophil adhesion to endothelial cells, thereby halting a key pathogenic mechanism of systemic vasculitis. The glucocorticoid-sparing effects of adjunctive methotrexate have been examined in 3 RCTs, albeit with mixed results.70–72 Further, a meta-analysis of these 3 randomized clinical trials found that the use of methotrexate was associated with a significant reduction (by 842 mg) in cumulative glucocorticoid dose within 48 weeks (P<0.001), a greater odds of achieving sustained discontinuation of glucocorticoids for at least 24 weeks (HR 2.84 [95% CI 1.52–5.28, P = 0.001]), and a reduced risk of first relapse by 35% and second relapse by 51% (HRs 0.65 [95% CI 0.44–0.98, P = 0.04] and 0.49 [95% CI 0.27–0.89, P = 0.02], respectively).73 More recently, a case-control study found that methotrexate plus glucocorticoids led to a significant decrease in relapse rate versus glucocorticoids alone (P = 0.004), but there were no group differences in cumulative glucocorticoid dose.74 Collectively, these data suggest that methotrexate requires further study to determine its effectiveness as a glucocorticoid-sparing adjunct to GCA treatment.
LEF has been evaluated as potentially providing a glucocorticoid-sparing effect in GCA. LEF is an immunomodulatory and immunosuppressive agent that inhibits pyrimidine synthesis75 and is thought to be effective in GCA because its active metabolite A771726 impairs dendritic cell maturation and function, which in turn reduces proinflammatory cytokine production and inhibits the T-cell stimulatory capacity of dendritic cells.76 Two case series studies among patients with GCA and/or PMR have shown that LEF was efficacious and generally well-tolerated.75,76 A more recent open-label study of LEF among 67 patients with GCA who were followed for ≥48 weeks found that those taking LEF had a significantly lower rate of relapse than patients taking glucocorticoids only (13.3% vs 39.1%, respectively, P = 0.02).77 More than half (56.7%) of the LEF patients were able to terminate glucocorticoid treatment by week 48, and their cumulative glucocorticoid dose was significantly lower than in the glucocorticoid-only patients (4390 mg vs 5340 mg, respectively, P=0.01).77
Targeted Biologic Therapies
Biologic drugs, including TCZ, abatacept, secukinumab, ustekinumab, sarilumab, and anakinra, are potentially attractive glucocorticoid-sparing alternatives for GCA.78 Many emerging biologic agents are focused on interleukin (IL)-6 blockade, but other mechanisms of action are being leveraged, such as IL-12 and IL-23 blockade, T-cell and T-helper cell activation, and B-cell depletion. Table 1 summarizes published RCTs of biologic and conventional (ie, nonbiologic) immunosuppressive medications for the treatment of GCA.79–85
 |
Table 1 Published Randomized Controlled Trials of Biologic and Nonbiologic Therapeutics in Patients with Giant Cell Arteritis |
TCZ is a recombinant humanized monoclonal antibody that blocks the IL-6 pathway—a validated biologic marker of disease activity in treated and untreated GCA—and reduces its proinflammatory activity.86 TCZ has been shown to improve remission rates and is associated with lower glucocorticoid doses in new and relapsed patients with GCA.79,80,86 Further, in a multicenter study of 471 patients, TCZ was shown to have a protective effect against the development of visual complications or new episodes of transient visual loss in GCA.87 The addition of conventional immunosuppressive agents to TCZ may offer additional benefits and could be a consideration in clinical practice. A multicenter study of 134 patients showed that TCZ as monotherapy or combined with conventional immunosuppressive agents is effective and safe in patients with GCA. Compared with TCZ monotherapy, the addition of immunosuppressive drugs, usually methotrexate, appeared to result in a higher rate of prolonged remission, even in patients with a longer GCA duration, more extracranial large-vessel vasculitis involvement, and higher acute-phase reactants.88 Further, TCZ with a shorter steroid taper has been shown to induce and maintain remission in patients with GCA.89,90 Some of the considerations for TCZ include dose optimization and route of administration for patients with GCA. Dosing optimization for TCZ may be necessary after remission in patients with GCA; a case series study of patients with GCA (n=231) in a real-world clinical practice setting reported that TCZ optimization by reducing the dose or increasing dosing interval after the achievement of complete remission was an effective and safe option.88 The route of administration of TCZ is another aspect to be considered given its impact on patient outcomes. Pharmacodynamic and pharmacokinetic effects, including mean trough steady-state exposure and change in biomarkers (ie, erythrocyte sedimentation rate and C-reactive protein), appear comparable between the subcutaneous (SC) and IV formulations.91 The evidence seems to indicate similar efficacy between IV and SC TCZ but a potential for a higher rate of adverse reactions with the IV formulation.92–94 On the other hand, patients taking SC TCZ who experience relapse may find better disease control after switching to the IV formulation.92
Given the complex pathogenesis of GCA,95 a diverse array of therapeutic targets other than IL-6 pathways are under consideration (eg, dendritic cells, T cells, T-helper cells, B cells), and therefore several other biologic agents with potential disease-controlling effects are being investigated, including in numerous active RCTs (Harrington et al, 2021).96 Additionally, new therapeutics are needed because IL-6 inhibition is not universally effective in all patients, as shown in GiACTA, and patients may have contraindications (eg, history of gastrointestinal bleed) to treatment.97 The selective costimulatory modulator abatacept has been evaluated in one multicenter RCT among patients with new-onset or relapsing GCA (n=41); abatacept plus prednisone was associated with greater relapse-free survival (48% vs 31%, respectively, P=0.049) and longer mean duration of remission (9.9 vs 3.9 months, respectively, P=0.023) than placebo plus prednisone.81 Ustekinumab is an immunoglobulin G (IgG) 1 monoclonal antibody98 that has demonstrated glucocorticoid-sparing effects among patients with refractory GCA (n=14), resulting in a decrease in average prednisone dose from 20 mg to 5 mg (P=0.001) over a median of 13.5 months.98 Secukinumab, a selective IL-17A monoclonal antibody, was investigated in a proof-of-concept phase 2 RCT which demonstrated that 70.1% of secukinumab-treated patients with new-onset or relapsing GCA were in sustained remission at week 28 versus 20.3% of placebo-treated patients (P < 0.05), and these patterns persisted at week 52 (59.3% vs 8.0%, respectively) with no new safety signals84,99 Anakinra, an IL-1 blocker, may have therapeutic glucocorticoid-sparing effects in patients with GCA, based on the findings of a small number of case studies.100,101 Sarilumab is an IL-6 receptor inhibitor evaluated in a phase 3 double-blind study; the study was terminated early and findings are inconclusive.102 Finally, mavrilimumab is an investigational fully human monoclonal antibody103 that blocks activity of granulocyte-macrophage colony-stimulating factor (GM-CSF) by specifically binding to the alpha subunit of the GM-CSF receptor. Mavrilimumab has been evaluated in a phase 2 RCT; this RCT demonstrated that mavrilimumab significantly reduces flare risk compared with placebo (HR 0.38 [95% CI 0.15–0.92, P = 0.026]).82
Novel nonbiologic anti-inflammatory agents are also being explored for the treatment of GCA and offer the potential for an oral glucocorticoid-sparing therapeutic option. Janus kinase (JAK) inhibitors, including upadacitinib104 and baricitinib,105 are being evaluated for GCA because of their ability to downregulate T-helper 1 and T-helper 17 pathways and block the effects of IL-6, IL-12, and IL-23.95,96 The Phase 3 SELECT-GCA study showed that upadacitinib at 15 mg, combined with a 26-week steroid taper, achieved a higher rate of sustained remission in patients with GCA compared to placebo with a 52-week steroid taper.85 Upadacitinib received approval from the US FDA for the treatment of GCA on April 29, 2025.106
Table 2 summarizes GCA-related RCTs currently underway to study biologic and nonbiologic agents.107–111
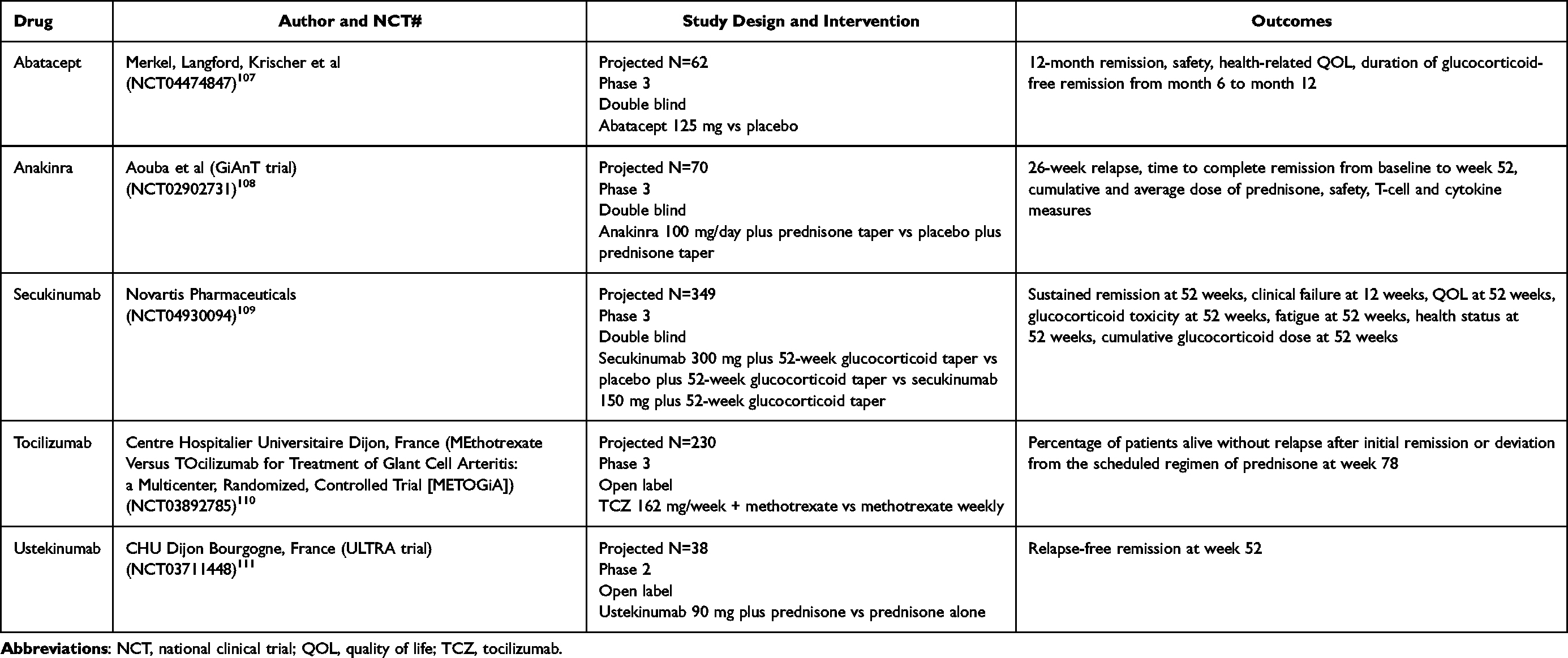 |
Table 2 Randomized Controlled Trials Currently Underway of Biologic and Nonbiologic Therapeutics in Patients with Giant Cell Arteritis |
Unmet Treatment Needs
Numerous unanswered questions remain about optimal GCA management. A multidisciplinary task force recently developed treat-to-target recommendations for GCA and PMR and also identified current gaps in research.66 Areas of uncertainty identified by the task force that must be addressed in future research include the lack of standardized definitions of disease states (eg, remission, response, relapse), the role of imaging and laboratory data in long-term patient care, differential effects of various treatment modalities on mortality, and the lack of research on patient-reported outcomes and their association with disease activity. There is currently a lack of consensus about what should be the primary target of treatment, although timely diagnosis and initiation of glucocorticoid treatment to help patients avoid potentially irreversible vision loss is generally considered among the most critical strategies.10,66,94,105 Reducing reliance on high-dose, long-term glucocorticoid treatment and preventing relapse are also considered urgent treatment goals, but a unanimous definition of relapse and remission is still lacking.10 Although minimizing the use of glucocorticoids can reduce the risk of glucocorticoid-related adverse events, their ability to protect against ischemic complications, including vision loss, is unquestionable and suggests there may always be a place for them in the treatment strategy. Trials of TCZ indicate that glucocorticoid tapering may be safely accomplished in as little as 6 months, or potentially less,112 without compromising clinical outcomes. However, not all patients can tolerate TCZ, and some experience disease recurrence while receiving treatment, underscoring the importance of identifying alternate effective glucocorticoid-sparing agents.
Whether glucocorticoids can be tapered more quickly and for how long is also unclear. The proof-of-concept GUSTO (GCA Treatment with Ultra-Short GC and TCZ) trial (n = 18) found that administration of TCZ monotherapy following a rapid 3-day taper of glucocorticoids in patients with new-onset GCA resulted in only 3 of 12 patients in the interim analysis achieving remission within 31 days and remaining relapse-free for up to 24 weeks.89 However, 14 of 18 patients recruited at the time of the interim analysis achieved remission at 24 weeks, and 13 of 18 were relapse-free for 52 weeks. Three of the 18 patients were treatment non-responders. Finally, in a single-arm, open-label study of 12 months of TCZ with only 8 weeks of prednisone (N=30), 77% of patients met the primary endpoint of prednisone-free remission at week 52, suggesting that 8 weeks of prednisone in combination with TCZ may be efficacious if upheld in larger samples.90
Given the population affected by GCA, there is a need for better characterization and study of the impact of GCA treatments and aging-related outcomes. In the study by Tedeschi et al,19 moderate-to-severe frailty at baseline was the highest risk factor for incident infections (MarketScan cohort adjusted HR 4.54 [95% CI 1.44–14.29]; Medicare cohort adjusted HR 2.51 [95% CI 1.38–4.57]). Frailty refers to a state of decline in physiologic reserve and homeostasis that is associated with an increased vulnerability to stressors and poor outcomes. Frailty provides a holistic assessment in older adults and is independently associated with several relevant outcomes, including other geriatric syndromes and mortality.113 Although data are scarce, a high prevalence of frailty and prefrailty has been described in patients living with multiple forms of vasculitis, including GCA.114 Studies on the impact of treatment and interventions in older adults with GCA and on other geriatric syndromes such as falls, polypharmacy, and functional status is also relevant, given the report of increased negative outcomes earlier in disease treatment.27 To better design appropriate interventions and to advance personalized care, studies must better identify the impact on these outcomes that are clinically relevant to patients affected by GCA.
Conclusions
GCA is the most common form of systemic vasculitis affecting older adults. If untreated, GCA can have devastating long-term effects on patient function and QOL, particularly in the form of potentially irreversible vision loss and stroke sequelae. Over the past 5 years, the treatment landscape for GCA has expanded beyond the mainstay of glucocorticoid therapy and has evolved to include glucocorticoid-sparing disease-modifying antirheumatic drugs and targeted therapies of both biologics and nonbiologic agents. Despite advances in GCA management, the burden of illness to patients is substantial, including decreased QOL, increased HCRU and spending, and a high risk of debilitating and expensive adverse effects due to long-term use of high-dose glucocorticoids. Research to develop glucocorticoid-sparing therapeutics that can prolong treatment-free remission from GCA is urgently needed. Clinicians should be aware of the many burdens of illness posed by GCA and its treatment and can improve patient care by reducing delays in diagnosis and making informed treatment decisions to optimize patient response while minimizing exposure to potential adverse events.
Acknowledgments
Medical writing and editing services were provided by Emily Kuhl, PhD, Ishveen Chopra, PhD, MBA, and Esther Tazartes, MS, of the Global Outcomes Group; these services were funded by Genentech, Inc. Dr. Rita De Castro and Dr. Fang Cai contributed to the review and editing of this manuscript, and both Dr. Castro and Dr. Cai are employees of Genentech, Inc.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Sponsorship for this review and the Rapid Service Fee were funded by Genentech Inc., South San Francisco, California.
Disclosure
SES is supported by the Rheumatology Research Foundation RISE Pilot Award and by the Bristol Myers Squibb Foundation Robert A. Winn Diversity in Clinical Trials Career Development Award. SES reports research support from AstraZeneca and GlaxoSmithKline (clinical trials). SES has consulted for Sanofi and participated in advisory boards for Sanofi and Amgen (all funds towards research support). SES reports speaker fees for Fresenius Kabi (funds towards research support). MC was an employee of Genentech during the development of this manuscript. DO is an employee of Genentech. The authors report no other conflicts of interest in this work.
References
1. Dua AB, Husainat NM, Kalot MA, et al. Giant cell arteritis: a systematic review and meta‐analysis of test accuracy and benefits and harms of common treatments. ACR Open Rheumatol. 2021;3(7):429–441. doi:10.1002/acr2.11226
2. De Smit E, Palmer AJ, Hewitt AW. Projected worldwide disease burden from giant cell arteritis by 2050. J Rheumatol. 2015;42(1):119–125. doi:10.3899/jrheum.140318
3. Dejaco C, Duftner C, Buttgereit F, Matteson EL, Dasgupta B. The spectrum of giant cell arteritis and polymyalgia rheumatica: revisiting the concept of the disease. Rheumatology. 2017;56(4):506–515. doi:10.1093/rheumatology/kew273
4. Lyons HS, Quick V, Sinclair AJ, Nagaraju S, Mollan SP. A new era for giant cell arteritis. Eye. 2020;34(6):1013–1026. doi:10.1038/s41433-019-0608-7
5. de Boysson H, Aouba A. An updated review of cardiovascular events in giant cell arteritis. J Clin Med. 2022;11(4):1005. doi:10.3390/jcm11041005
6. Li KJ, Semenov D, Turk M, Pope J. A meta-analysis of the epidemiology of giant cell arteritis across time and space. Arthritis Res Ther. 2021;23(1):82. doi:10.1186/s13075-021-02450-w
7. Gill T, Putman M, Sattui SE, et al. Giant cell arteritis can occur in people of colour. Lancet Rheumatol. 2023;5(4):e175–7. doi:10.1016/S2665-9913(23)00068-1
8. Maz M, Chung SA, Abril A, et al. 2021 American College of Rheumatology/Vasculitis Foundation guideline for the management of giant cell arteritis and Takayasu arteritis. Arthritis Rheumatol. 2021;73(8):1349–1365. doi:10.1002/art.41774
9. Hellmich B, Agueda A, Monti S, et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. 2020;79(1):19–30. doi:10.1136/annrheumdis-2019-215672
10. Bond M, Tomelleri A, Buttgereit F, Matteson EL, Dejaco C. Looking ahead: giant-cell arteritis in 10 years time. Ther Adv Musculoskelet Dis. 2022;14:1759720X221096366. doi:10.1177/1759720X221096366
11. Yu E, Chang JR. Giant cell arteritis: updates and controversies. Front Ophthalmol. 2022;2.
12. Crowson CS, Matteson EL. Contemporary prevalence estimates for giant cell arteritis and polymyalgia rheumatica, 2015. Semin Arthritis Rheum. 2017;47(2):253–256. doi:10.1016/j.semarthrit.2017.04.001
13. Therkildsen P, Nielsen BD, de Thurah A, Hansen IT, Norgaard M, Hauge EM. All-cause and cause-specific mortality in patients with giant cell arteritis: a nationwide, population-based cohort study. Rheumatology. 2022;61(3):1195–1203. doi:10.1093/rheumatology/keab507
14. Barra L, Pope JE, Pequeno P, Gatley JM, Widdifield J. Increased mortality for individuals with giant cell arteritis: a population-based study. Arthritis Care Res. 2022;74(8):1294–1299. doi:10.1002/acr.24573
15. Ben-Shabat N, Tiosano S, Shovman O, et al. Mortality among patients with giant cell arteritis: a large-scale population-based cohort study. J Rheumatol. 2020;47(9):1385–1391. doi:10.3899/jrheum.190927
16. Li L, Neogi T, Jick S. Mortality in patients with giant cell arteritis: a cohort study in UK primary care. Arthritis Care Res. 2018;70(8):1251–1256. doi:10.1002/acr.23538
17. Hill CL, Black RJ, Nossent JC, et al. Risk of mortality in patients with giant cell arteritis: a systematic review and meta-analysis. Semin Arthritis Rheum. 2017;46(4):513–519. doi:10.1016/j.semarthrit.2016.08.015
18. Camellino D, Matteson EL, Buttgereit F, Dejaco C. Monitoring and long-term management of giant cell arteritis and polymyalgia rheumatica. Nat Rev Rheumatol. 2020;16(9):481–495. doi:10.1038/s41584-020-0458-5
19. Tedeschi SK, Jin Y, Vine S, et al. Giant cell arteritis treatment patterns and rates of serious infections. Clin Exp Rheumatol. 2022;40(4):826–833. doi:10.55563/clinexprheumatol/uonz1p
20. Donaldson L, Margolin E. Vision loss in giant cell arteritis. Pract Neurol. 2022;22(2):138–140. doi:10.1136/practneurol-2021-002972
21. 138–140.
22. Vodopivec I, Rizzo JF. Ophthalmic manifestations of giant cell arteritis. Rheumatology. 2018;57(suppl_2):ii63–ii72. doi:10.1093/rheumatology/kex428
23. Clifford AH. Cardiovascular disease in large vessel vasculitis: risks, controversies, and management strategies. Rheum Dis Clin North Am. 2023;49(1):81–96. doi:10.1016/j.rdc.2022.08.004
24. Tomasson G, Peloquin C, Mohammad A, et al. Risk for cardiovascular disease early and late after a diagnosis of giant-cell arteritis: a cohort study. Ann Intern Med. 2014;160(2):73–80. doi:10.7326/M12-3046
25. Ungprasert P, Wijarnpreecha K, Koster MJ, Thongprayoon C, Warrington KJ. Cerebrovascular accident in patients with giant cell arteritis: a systematic review and meta-analysis of cohort studies. Semin Arthritis Rheum. 2016;46(3):361–366. doi:10.1016/j.semarthrit.2016.07.005
26. Ungprasert P, Koster MJ, Warrington KJ. Coronary artery disease in giant cell arteritis: a systematic review and meta-analysis. Semin Arthritis Rheum. 2015;44(5):586–591. doi:10.1016/j.semarthrit.2014.10.010
27. Singh JA, Cleveland JD. Serious infections in people with polymyalgia rheumatica (PMR) or giant cell arteritis (GCA): a time-trend national US study. Clin Rheumatol. 2020;39(11):3427–3438. doi:10.1007/s10067-020-05129-w
28. Castan P, Dumont A, Deshayes S, et al. Impact of glucocorticoid cumulative doses in a real-life cohort of patients affected by giant cell arteritis. J Clin Med. 2022;11(4):1034. doi:10.3390/jcm11041034
29. Broder MS, Sarsour K, Chang E, et al. Corticosteroid-related adverse events in patients with giant cell arteritis: a claims-based analysis. Semin Arthritis Rheum. 2016;46(2):246–252. doi:10.1016/j.semarthrit.2016.05.009
30. Cid MC, Alba MA. Sustained remission: an unmet need in patients with giant-cell arteritis. J Rheumatol. 2015;42(7):1081–1082. doi:10.3899/jrheum.150534
31. Martinez-Lado L, Calvino-Diaz C, Pineiro A, et al. Relapses and recurrences in giant cell arteritis: a population-based study of patients with biopsy-proven disease from northwestern Spain. Medicine. 2011;90(3):186–193. doi:10.1097/MD.0b013e31821c4fad
32. Baig IF, Pascoe AR, Kini A, Lee AG. Giant cell arteritis: early diagnosis is key. Eye Brain. 2019;11:1–12. doi:10.2147/EB.S170388
33. Heron E, Sedira N, Dahia O, Jamart C. Ocular complications of giant cell arteritis: an acute therapeutic emergency. J Clin Med. 2022;11(7):1997. doi:10.3390/jcm11071997
34. Gonzalez-Gay MA, Ortego-Jurado M, Ercole L, Ortego-Centeno N. Giant cell arteritis: is the clinical spectrum of the disease changing? BMC Geriatr. 2019;19(1):200. doi:10.1186/s12877-019-1225-9
35. Muller G, Devilliers H, Besancenot JF, Manckoundia P. Giant cell arteritis (Horton’s disease) in very elderly patients aged 80 years and older: a study of 25 cases. Geriatr Gerontol Int. 2016;16(6):679–685. doi:10.1111/ggi.12536
36. Prior JA, Ranjbar H, Belcher J, et al. Diagnostic delay for giant cell arteritis - a systematic review and meta-analysis. BMC Med. 2017;15(1):120. doi:10.1186/s12916-017-0871-z
37. Kermani TA, Schafer VS, Crowson CS, et al. Increase in age at onset of giant cell arteritis: a population-based study. Ann Rheum Dis. 2010;69(4):780–781. doi:10.1136/ard.2009.111005
38. Gonzalez-Gay MA, Miranda-Filloy JA, Lopez-Diaz MJ, et al. Giant cell arteritis in northwestern Spain: a 25-year epidemiologic study. Medicine. 2007;86(2):61–68. doi:10.1097/md.0b013e31803d1764
39. Salvarani C, Crowson CS, Wm O, Hunder GG, Gabriel SE. Reappraisal of the epidemiology of giant cell arteritis in Olmsted County, Minnesota, over a fifty-year period. Arthritis Rheum. 2004;51(2):264–268. doi:10.1002/art.20227
40. Daumas A, Bichon A, Rioland C, et al. Characteristics of giant cell arteritis patients under and over 75-years-old: a comparative study on 164 patients. Rev Med Interne. 2019;40(5):278–285. doi:10.1016/j.revmed.2018.11.004
41. Monti S, Milanesi A, Klersy C, et al. Age at diagnosis influences the clinical phenotype, treatment strategies and outcomes in patients with giant cell arteritis: results from the observational GCAGE study on a large cohort of 1004 patients. Ann Rheum Dis. 2023;82(8):1098–1106. doi:10.1136/ard-2023-223895
42. Grayson PC, Amudala NA, McAlear CA, et al. Illness perceptions and fatigue in systemic vasculitis. Arthritis Care Res. 2013;65(11):1835–1843. doi:10.1002/acr.22069
43. Martinho J, Ponte A, Dourado E, et al. Risk factors for anxiety and depression in patients with giant cell arteritis Abstract 1947. Am College Rheumatol Convergence. 2020.
44. Liddle J, Bartlam R, Mallen CD, et al. What is the impact of giant cell arteritis on patients’ lives? A UK qualitative study. BMJ Open. 2017;7(8):e017073. doi:10.1136/bmjopen-2017-017073
45. Robson JC, Almeida C, Dawson J, et al. Patient perceptions of health-related quality of life in giant cell arteritis: international development of a disease-specific patient-reported outcome measure. Rheumatology. 2021;60(10):4671–4680. doi:10.1093/rheumatology/keab076
46. Strand V, Dimonaco S, Tuckwell K, Klearman M, Collinson N, Stone JH. Health-related quality of life in patients with giant cell arteritis treated with tocilizumab in phase 3 randomized controlled trial. Arthritis Res Ther. 2019;21(1):64. doi:10.1186/s13075-019-1837-7
47. Stone JH, Han J, Unizony S, et al. SAT0275 maintained benefit in health-related quality of life of patients with giant cell arteritis treated with tocilizumab plus prednisone tapering: results from the open-label, long-term extension of a phase 3 randomized controlled trial. Ann Rheum Dis. 2020;79:1081–1082. doi:10.1136/annrheumdis-2020-eular.1541
48. Babigumira JB, Li M, Boudreau DM, Best JH, Garrison LP Jr. Estimating the cost of illness of giant cell arteritis in the United States. Rheumatol Ther. 2017;4(1):111–119. doi:10.1007/s40744-017-0052-8
49. Mahr A, Belhassen M, Paccalin M, et al. Characteristics and management of giant cell arteritis in France: a study based on national health insurance claims data. Rheumatology. 2020;59(1):120–128. doi:10.1093/rheumatology/kez251
50. Pugnet G, Costa N, Bouscaren N, et al. Incremental costs of giant cell arteritis in France. Value Health. 2015;18(3):A139. doi:10.1016/j.jval.2015.03.809
51. Koster MJ, Achenbach SJ, Crowson CS, Maradit-Kremers H, Matteson EL, Warrington KJ. Healthcare use and direct cost of giant cell arteritis: a population-based study. J Rheumatol. 2017;44(7):1044–1050. doi:10.3899/jrheum.161516
52. Chakravarthy U, Biundo E, Saka RO, Fasser C, Bourne R, Little JA. The economic impact of blindness in Europe. Ophthalmic Epidemiol. 2017;24(4):239–247. doi:10.1080/09286586.2017.1281426
53. Rochmah TN, Rahmawati IT, Dahlui M, Budiarto W, Bilqis N. Economic burden of stroke disease: a systematic review. Int J Environ Res Public Health. 2021;18(14):7552. doi:10.3390/ijerph18147552
54. Wang G, Zhang Z, Ayala C, Dunet DO, Fang J, George MG. Costs of hospitalization for stroke patients aged 18-64 years in the United States. J Stroke Cerebrovasc Dis. 2014;23(5):861–868. doi:10.1016/j.jstrokecerebrovasdis.2013.07.017
55. Kremers HM, Reinalda MS, Crowson CS, Zinsmeister AR, Hunder GG, Gabriel SE. Direct medical costs of polymyalgia rheumatica. Arthritis Rheum. 2005;53(4):578–584. doi:10.1002/art.21311
56. Centers for Disease Control and Prevention. How type 2 diabetes affects your workforce 2021. Available from: https://www.cdc.gov/diabetes/prevention/how-type2-affects-workforce.htm.
57. Nichols GA, Bell TJ, Pedula KL, O’Keeffe-Rosetti M. Medical care costs among patients with established cardiovascular disease. Am J Manag Care. 2010;16(3):e86–e93.
58. Goulabchand R, Qian AS, Nguyen NH, et al. Burden, causes, and outcomes of hospitalization in patients with giant cell arteritis: a US national cohort study. Arthritis Care Res. 2022.
59. Best JH, Kong AM, Smith DM, Abbass I, Michalska M. Healthcare costs of potential glucocorticoid-associated adverse events in patients with giant cell arteritis. Clinicoecon Outcomes Res. 2019;11:799–807. doi:10.2147/CEOR.S228400
60. Sheppard M, Laskou F, Stapleton PP, Hadavi S, Dasgupta B. Tocilizumab. Hum Vaccin Immunother. 2017;13(9):1972–1988. doi:10.1080/21645515.2017.1316909
61. Jogimahanti AV, Kini AT, Irwin LE, Lee AG. The cost-effectiveness of tocilizumab (Actemra) therapy in giant cell arteritis. J Neuroophthalmol. 2021;41(3):342–350. doi:10.1097/WNO.0000000000001220
62. Drugs.com. Actemra prices, coupons and patient assistance programs 2022. Available from: https://www.drugs.com/price-guide/actemra.
63. Kim J, Parish AL. Polypharmacy and medication management in older adults. Nurs Clin North Am. 2017;52(3):457–468. doi:10.1016/j.cnur.2017.04.007
64. Pazan F, Wehling M. Polypharmacy in older adults: a narrative review of definitions, epidemiology and consequences. Eur Geriatr Med. 2021;12(3):443–452. doi:10.1007/s41999-021-00479-3
65. Melillo G. Polypharmacy nearly doubles health care expenditures among older patients with CVD 2022. Available from: https://www.ajmc.com/view/polypharmacy-nearly-doubles-health-care-expenditures-among-older-patients-with-cvd.
66. Kwak MJ, Chang M, Chiadika S, et al. Healthcare expenditure associated with polypharmacy in older adults with cardiovascular diseases. Am J Cardiol. 2022;169:156–158. doi:10.1016/j.amjcard.2022.01.012
67. Dejaco C, Kerschbaumer A, Aletaha D, et al. Treat-to-target recommendations in giant cell arteritis and polymyalgia rheumatica. Ann Rheum Dis. 2024;83(1):48–57. doi:10.1136/ard-2022-223429
68. Dinkin M, Johnson E. One giant step for giant cell arteritis: updates in diagnosis and treatment. Curr Treat Options Neurol. 2021;23(2):6. doi:10.1007/s11940-020-00660-2
69. Best J, Nunez I, Woodburn K, Breyer A, Conway M, Michalska M. Patients’ journeys through giant cell arteritis: a qualitative study. 2019;71(suppl 10).
70. Spiera RF, Mitnick HJ, Kupersmith M, et al. A prospective, double-blind, randomized, placebo controlled trial of methotrexate in the treatment of giant cell arteritis (GCA). Clin Exp Rheumatol. 2001;19(5):495–501.
71. Hoffman GS, Cid MC, Hellmann DB, et al. A multicenter, randomized, double-blind, placebo-controlled trial of adjuvant methotrexate treatment for giant cell arteritis. Arthritis Rheum. 2002;46(5):1309–1318. doi:10.1002/art.10262
72. Jover JA, Hernandez-Garcia C, Morado IC, Vargas E, Banares A, Fernandez-Gutierrez B. Combined treatment of giant-cell arteritis with methotrexate and prednisone. a randomized, double-blind, placebo-controlled trial. Ann Intern Med. 2001;134(2):106–114. doi:10.7326/0003-4819-134-2-200101160-00010
73. Mahr AD, Jover JA, Spiera RF, et al. Adjunctive methotrexate for treatment of giant cell arteritis: an individual patient data meta-analysis. Arthritis Rheum. 2007;56(8):2789–2797. doi:10.1002/art.22754
74. Koster MJ, Yeruva K, Crowson CS, Muratore F, Labarca C, Warrington KJ. Efficacy of methotrexate in real-world management of giant cell arteritis: a case-control study. J Rheumatol. 2019;46(5):501–508. doi:10.3899/jrheum.180429
75. Diamantopoulos AP, Hetland H, Myklebust G. Leflunomide as a corticosteroid-sparing agent in giant cell arteritis and polymyalgia rheumatica: a case series. Biomed Res Int. 2013;2013:120638. doi:10.1155/2013/120638
76. Adizie T, Christidis D, Dharmapaliah C, Borg F, Dasgupta B. Efficacy and tolerability of leflunomide in difficult-to-treat polymyalgia rheumatica and giant cell arteritis: a case series. Int J Clin Pract. 2012;66(9):906–909. doi:10.1111/j.1742-1241.2012.02981.x
77. Hocevar A, Jese R, Rotar Z, Tomsic M. Does leflunomide have a role in giant cell arteritis? An open-label study. Clin Rheumatol. 2019;38(2):291–296. doi:10.1007/s10067-018-4232-x
78. Roberts J, Clifford A. Update on the management of giant cell arteritis. Ther Adv Chronic Dis. 2017;8(4–5):69–79. doi:10.1177/2040622317700089
79. Villiger PM, Adler S, Kuchen S, et al. Tocilizumab for induction and maintenance of remission in giant cell arteritis: a phase 2, randomised, double-blind, placebo-controlled trial. Lancet. 2016;387(10031):1921–1927. doi:10.1016/S0140-6736(16)00560-2
80. Stone JH, Han J, Aringer M, et al. Long-term effect of tocilizumab in patients with giant cell arteritis: open-label extension phase of the Giant Cell Arteritis Actemra (GiACTA) trial. Lancet Rheumatol. 2021;3(5):e328–36. doi:10.1016/S2665-9913(21)00038-2
81. Langford CA, Cuthbertson D, Ytterberg SR, et al. A randomized, double-blind trial of abatacept (CTLA-4Ig) for the treatment of giant cell arteritis. Arthritis Rheumatol. 2017;69(4):837–845. doi:10.1002/art.40044
82. Cid MC, Unizony SH, Blockmans D, et al. Efficacy and safety of mavrilimumab in giant cell arteritis: a phase 2, randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. 2022;81(5):653–661. doi:10.1136/annrheumdis-2021-221865
83. Matza MA, Fernandes AD, Stone JH, Unizony SH. Ustekinumab for the treatment of giant cell arteritis. Arthritis Care Res. 2021;73(6):893–897. doi:10.1002/acr.24200
84. Venhoff N, Schmidt WA, Bergner R, et al. Secukinumab in giant cell arteritis: a randomized, parallel-group, double-blind, placebo-controlled, multicenter phase 2 trial. Abstract L19. Am College Rheumatol Convergence. 2021.
85. Blockmans D, Penn SK, Setty AR, et al. SELECT-GCA Study Group. A phase 3 trial of upadacitinib for giant-cell arteritis. N Engl J Med. 2025;392;(20):2013–24
86. Stone JH, Tuckwell K, Dimonaco S, et al. Trial of tocilizumab in giant-cell arteritis. N Engl J Med. 2017;377(4):317–328. doi:10.1056/NEJMoa1613849
87. Calderon-Goercke M, Loricera J, Moriano C, et al. Optimisation of tocilizumab therapy in giant cell arteritis. a multicentre real-life study of 471 patients. Clin Exp Rheumatol. 2023;41(4):829–836. doi:10.55563/clinexprheumatol/oqs8u9
88. Calderon-Goercke M, Castaneda S, Aldasoro V, et al. Tocilizumab in refractory giant cell arteritis. Monotherapy versus combined therapy with conventional immunosuppressive drugs. Observational multicenter study of 134 patients. Semin Arthritis Rheum. 2021;51(2):387–394. doi:10.1016/j.semarthrit.2021.01.006
89. Christ L, Seitz L, Scholz G, et al. OP0061 A proof-of-concept study to assess the efficacy of tocilizumab monotherapy after ultra-short glucocorticoid administration to treat giant cell arteritis—The GUSTO trial. abstract 05015. Am College Rheumatol Convergence. 2020.
90. Unizony S, Matza MA, Jarvie A, O’Dea D, Fernandes AD, Stone JH. Treatment for giant cell arteritis with 8 weeks of prednisone in combination with tocilizumab: a single-arm, open-label, proof-of-concept study. Lancet Rheumatol. 2023;5(12):E736–E42. doi:10.1016/S2665-9913(23)00265-5
91. Mallalieu NL, Stone JH, Villiger PM, et al. A comparison of pharmacokinetic and pharmacodynamic outcomes of tocilizumab treatment in giant cell arteritis after subcutaneous and intravenous dosing. Abstract 2757. Am College Rheumatol. 2018.
92. Schmalzing M, Gadeholt O, Gernert M, Tony HP, Schwaneck EC. Tocilizumab in large vessel vasculitis - different routes of administration. Open Rheumatol J. 2018;12:152–159. doi:10.2174/1874312901812010152
93. Sanchez-Bilbao L, Loricera J, Castañeda S, et al. POS0272 Intravenous versus subcutaneous tocilizumab in a series of 471 patients with giant cell arteritis. Ann Rheum Dis. 2022;81(1).
94. Calderon-Goercke M, Loricera J, Prieto-Pena D, et al. Tocilizumab in giant cell arteritis: route of administration: intravenous or subcutaneous. Ann Rheum Dis. 2019;78(2).
95. Low C, Conway R. Current advances in the treatment of giant cell arteritis: the role of biologics. Ther Adv Musculoskelet Dis. 2019;11:1759720X19827222. doi:10.1177/1759720X19827222
96. Harrington R, Al Nokhatha SA, Conway R. Biologic therapies for giant cell arteritis. Biologics. 2021;15:17–29. doi:10.2147/BTT.S229662
97. Koster MJ, Warrington KJ. Giant cell arteritis: pathogenic mechanisms and new potential therapeutic targets. BMC Rheumatol. 2017;1:2. doi:10.1186/s41927-017-0004-5
98. Conway R, O’Neill L, O’Flynn E, et al. Ustekinumab for the treatment of refractory giant cell arteritis. Ann Rheum Dis. 2016;75(8):1578–1579. doi:10.1136/annrheumdis-2016-209351
99. Barnard C. IL-17A inhibition demonstrates potential for giant cell arteritis. Am College Rheumatol. 2021.
100. Ly KH, Stirnemann J, Liozon E, Michel M, Fain O, Fauchais AL. Interleukin-1 blockade in refractory giant cell arteritis. Joint Bone Spine. 2014;81(1):76–78. doi:10.1016/j.jbspin.2013.06.004
101. Deshayes S, Ly KH, Rieu V, et al. Steroid-sparing effect of anakinra in giant-cell arteritis: a case series with clinical, biological and iconographic long-term assessments. Rheumatology. 2021;61(1):400–406. doi:10.1093/rheumatology/keab280
102. Schmidt WA, Dasgupta B, Sloane J, et al. A phase 3 randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of sarilumab in patients with giant cell arteritis. Arthritis Res Ther. 2023;25(1):199.
103. Cid MC, Muralidharan S, Corbera-Bellalta M, et al. FRI0010 GM-CSFR pathway is implicated in pathogenic inflammatory mechanisms in giant cell arteritis. Ann Rheum Dis. 2020;79(1):19–30. doi:10.1136/annrheumdis-2020-eular.4984
104. Zhang H, Watanabe R, Berry GJ, Tian L, Goronzy JJ, Weyand CM. Inhibition of JAK-STAT signaling suppresses pathogenic immune responses in medium and large vessel vasculitis. Circulation. 2018;137(18):1934–1948. doi:10.1161/CIRCULATIONAHA.117.030423
105. Koster MJ, Crowson CS, Giblon RE, et al. Baricitinib for relapsing giant cell arteritis: a prospective open-label 52-week pilot study. Ann Rheum Dis. 2022;81(6):861–867. doi:10.1136/annrheumdis-2021-221961
106. AbbVie. RINVOQ®.(upadacitinib) Receives U.S. FDA approval for giant cell arteritis (GCA). 2025. Available fromhttps://news.abbvie.com/2025-04-29-RINVOQ-R-upadacitinib-Receives-U-S-FDA-Approval-for-Giant-Cell-ArteritisGCA#:~:text=NORTH%20CHICAGO%2C%20Ill.%2C%20April,giant%20cell%20arteritis%20%28GCA%29.
107. University of Pennsylvania. Abatacept for the treatment of giant cell arteritis. Available from: https://clinicaltrials.gov/study/NCT04474847.
108. University Hospital, Caen. Giant cell arteritis and anakinra trial (GiAnT). Available from: https://clinicaltrials.gov/study/NCT02902731.
109. Novartis Pharmaceuticals. Phase III Study of efficacy and safety of secukinumab versus placebo, in combination with glucocorticoid taper regimen, in patients with giant cell arteritis (GCA) (GCAptAIN). Available from: https://clinicaltrials.gov/study/NCT04930094.
110. Centre Hospitalier Universitaire Dijon. MEthotrexate versus TOcilizumab for treatment of giant cell arteritis: a multicenter, randomized, controlled trial (METOGiA). Available from: https://clinicaltrials.gov/study/NCT03892785.
111. Centre Hospitalier Universitaire Dijon. Ustekinumab for the treatment of relapse of refractory giant cell arteritis (ULTRA). Available from: https://clinicaltrials.gov/study/NCT03711448.
112. Camellino D, Dejaco C, Buttgereit F, Matteson EL. Treat to target: a valid concept for management of polymyalgia rheumatica and giant cell arteritis? Rheum Dis Clin North Am. 2019;45(4):549–567. doi:10.1016/j.rdc.2019.07.005
113. Vermeiren S, Vella-Azzopardi R, Beckwee D, et al. Frailty and the prediction of negative health outcomes: a meta-analysis. J Am Med Dir Assoc. 2016;17(12):1163e1–e17. doi:10.1016/j.jamda.2016.09.010
114. Sattui S, Stadler J, Burroughs C, et al. Prevalence of frailty and associated factors in patients with vasculitis. Arthritis Rheumatol. 2022;1(74).
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.