")
Back to Journals » Clinical Ophthalmology » Volume 19
Impact of Active Fluidics System on RNFL and GCL in Phacoemulsification
Authors Di Maria A , Ferraro V, Barone G, Vitali M, Tredici C, Gaeta A, Vinciguerra P, Confalonieri F
Received 28 March 2025
Accepted for publication 27 June 2025
Published 18 July 2025 Volume 2025:19 Pages 2383—2391
DOI https://doi.org/10.2147/OPTH.S526195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Alessandra Di Maria,1,2 Vanessa Ferraro,1,2 Gianmaria Barone,1,2 Massimo Vitali,1,2 Costanza Tredici,1,2 Alessandro Gaeta,3 Paolo Vinciguerra,1,2 Filippo Confalonieri4
1Department of Ophthalmology, IRCCS Humanitas Research Hospital, Milan, Italy; 2Department of Biomedical Sciences, Humanitas University, Milan, Italy; 3Department of Internal Medicine and Medical Specialties (DIMI), Università Di Genova, Genova GE, 16132, Italy; 4Department of Ophthalmology, Montecchi Hospital of Suzzara, Suzzara, 46029, Italy
Correspondence: Filippo Confalonieri, Department of Ophthalmology, Montecchi Hospital of Suzzara, via Generale Cantore 14/B, Suzzara, 46029, Italy, Email [email protected]
Purpose: The aim of this study was to evaluate whether cataract surgery performed using the Active Fluidics® system under low-pressure settings has any measurable impact on the retinal nerve fiber layer (RNFL) and ganglion cell layer (GCL), with particular attention to early postoperative structural changes and safety outcomes.
Materials and Methods: Inclusion criteria comprised age-related cataract N4 NC4, BCVA ≤ 0.6, and subjects aged > 18 years. Exclusion criteria encompassed glaucoma therapy, anatomical pathologies, or retinal history. Preoperatively, participants underwent comprehensive ophthalmological assessment. Macular GCL and peripapillary RNFL evaluations were conducted using the Heidelberg Spectralis® OCT. Visual field (VF) tests were performed with Zeiss Humphrey Field Analyzer 3. Phacoemulsification surgery was performed using the Alcon Centurion Vision System. A month later, participants underwent ophthalmological re-evaluation, repeating OCT and VF testing.
Results: No significant differences were found before and after surgery in GCL. Regarding RNFL thickness, a significant increase was observed in several sectors. Changes in the computerized VF test showed variations, but these were not statistically significant.
Conclusion: We found no significant changes in GCL nor retinal function. However, there was an increase in peripapillary RNFL, likely due to underestimation caused by lens opacification before surgery. Overall, the Alcon® system allows for safe surgery with reliable long-term results and minimal retinal damage.
Keywords: phacoemulsification, cataract, retinal nerve fiber layer, RNFL, ganglion cell layer, GCL, glaucoma
Introduction
Cataract surgery is a common and effective procedure to restore vision in patients with lens opacities. However, it is important to consider the potential effects of the procedure on the health of the surrounding ocular tissues, particularly the macular ganglion cells layer (GCL) and the peripapillary optic nerve fibers (RNFL).
While phacoemulsification is the standard method for cataract surgery worldwide, the optimal settings to enhance safety and efficiency have yet to be definitively established. Numerous attempts have been undertaken to optimize various phacoemulsification settings.1 Most phacoemulsification machines determine intraocular pressure (IOP) based on the bottle height, with the actual IOP varying based on the balance between inflow and outflow. One such endeavor involves a monitored forced infusion system, specifically the Centurion Vision System and Active Fluidics developed by Alcon Surgical, Inc., which was introduced in 2013.2 This system continuously monitors and controls IOP throughout the procedure by adjusting the compression of the saline infusion bag to accommodate varying pressures within the eye. The primary objective of this new setting is to minimize post-occlusion surge, a phenomenon characterized by the sudden collapse of the anterior chamber due to the rapid influx of fluid through the phaco tip following an occlusion event.3
While the majority of studies have concentrated on the corneal flare edema resulting from infusion in the early postoperative period, less attention has been devoted to the effects on the posterior segment.4,5
Macular GCL constitute an essential part of the retina involved in transmitting visual signals to the brain.6 During cataract surgery, temporary or, in some cases, permanent compromise of these fibers may occur. This compromise may result from surgical trauma, IOP fluctuations, or other factors. Clinical studies have demonstrated that the density and function of GCL can be influenced following cataract surgery, potentially leading to changes in central vision and detail perception.7
Peripapillary RNFL, extending from the optic nerve head to the surrounding retina, are equally susceptible to the effects of cataract surgery, as intraocular manipulation during surgery could induce mechanical distortion or pressure on the RNFL, causing potential damage that could result in alterations in the visual field or even deficits in color perception.8 It is important to emphasize that while cataract surgery is generally safe and effective, side effects such as those described above can occur, and the potential impact of controlled IOP on efficiency and safety remains uncertain. Despite certain innovative and unique aspects of this system, others (such as torsional power, vacuum, and suction settings) remain similar to those of previous platforms. Therefore, we conducted an optimization study to assess efficiency and safety using this system in the context of IOP control.
Materials and Methods
We conducted a prospective observational cohort study at the Department of Ophthalmology, IRCCS Humanitas Research Hospital, Rozzano, Milan, Italy. Institutional approval was obtained (Ethics Committee No. 4132), and written informed consent was collected from all participants in accordance with the Declaration of Helsinki (2013) and the Health Insurance Portability and Accountability Act.
A total of 100 patients (100 eyes) were enrolled, all diagnosed with age-related cataract graded N4 NC4,9 with BCVA ≤ 0.6 (Snellen scale), and aged over 18 years. Inclusion criteria also required patients to present with a maximum spherical refractive error of - 3.00 diopters for myopia and +3.00 diopters for hyperopia, with a cylindrical astigmatic component not exceeding - 0.75 diopters. Eligible eyes were further restricted to those with an axial length between 21 mm and 25 mm to ensure anatomical comparability and reduce variability in retinal layer measurements due to extreme ocular biometrics.
Exclusion criteria included current topical therapy for glaucoma or ocular hypertension, use of prostaglandin analogues due to their effect on tear film and epiphora, which may influence VF testing,10 congenital ocular anomalies (eg, microphthalmos, buphthalmos), history of intraocular surgery, and macular or other retinal pathologies. We excluded patients with any known ocular or systemic condition that may influence retinal structural parameters postoperatively. Specifically, patients with glaucoma, ocular hypertension, diabetic retinopathy and diabetes, optic neuropathies, carotid disease or neurodegenerative diseases (eg, multiple sclerosis) were excluded, as these conditions are known to induce pre-existing or progressive alterations in RNFL and GCL thickness that may obscure surgery-related effects.6–8 Additionally, any history of intraocular inflammation, retinal vein occlusion, or prior macular surgery was considered exclusionary for the same reasons. These criteria were applied to ensure that the observed changes in retinal morphology were attributable solely to the surgical intervention and not to underlying pathology.
Preoperative evaluation included BCVA, IOP measurement, slit-lamp and dilated fundus examination, and ocular biometry using the Anterion system (Heidelberg Engineering GmbH, Heidelberg, Germany), providing keratometry, corneal thickness, axial length, and anterior chamber depth. OCT was performed with Spectralis (Heidelberg Engineering GmbH) to assess macular GCL and peripapillary RNFL. RNFL thickness was measured in seven regions: central, nasal, temporal, superior-nasal, superior-temporal, inferior-nasal, and inferior-temporal. GCL analysis included central, para-macular, and peri-macular areas; the para- and peri-macular values were calculated as the arithmetic mean of superior, inferior, nasal, and temporal sectors. Visual field (VF) testing was conducted using the Humphrey Field Analyzer 3 (Carl Zeiss Meditec AG, Jena, Germany), and included evaluation of Visual Field Index (VFI), Mean Deviation (MD), and Pattern Standard Deviation (PSD). All thicknesses were expressed in micrometers.
The preoperative evaluation was followed by standard phacoemulsification surgery performed under topical anesthesia, administered using a combination of eye drops containing Novesin (proparacaine hydrochloride) and lidocaine. Two experienced surgeons (A.D.M. and F.C.) performed all procedures using the Centurion Vision System with Active Sentry (Alcon Laboratories, Inc.) Viscoat (Alcon Laboratories), a dispersive viscoelastic substance, was used intraoperatively to protect the corneal endothelium and maintain anterior chamber stability. After cataract extraction, a foldable Clareon intraocular lens (Alcon Inc.) was implanted in the capsular bag. The overall surgical mean time was 10.4 minutes, maximum infusion pressure was set at 50 mmHg intraoperatively, while the mean intraocular pressure maintained throughout the procedures was 19.6 mmHg. Ultrasound energy was set to 0%, and torsional mode was used at a setting of 60%.
Postoperatively, patients were treated with a fixed combination of tobramycin and prednisolone acetate ophthalmic suspension (Fidia Pharma Group) administered four times daily for one week. This was followed by bromfenac 0.09% ophthalmic solution (Bausch & Lomb), prescribed twice daily for three weeks to control postoperative inflammation and discomfort.
None of the Patients Had Complications
One month after the surgery, the patients underwent a comprehensive ophthalmological re-evaluation. In this context, the patients were once again subjected to OCT using Spectralis® and computerized visual field testing with the Zeiss Humphrey Field Analyzer 3. The assessed parameters remained consistent with those evaluated in the preoperative assessment.
During this investigation, all necessary institutional and regulatory standards regarding the ethical use of human participants were followed. It was authorized by the IRCCS Humanitas Research Hospital’s Institutional Review Board. The research was carried out in conformity with the Helsinki Declaration of 1964’s ethical principles.
For statistical analysis, a two-tailed paired t-test was used to analyze associations between categorical parameters while correlations between continuous variables were analyzed using Pearson correlation coefficient and linear regression. Data were analyzed using STATA: statistical software for data science. A p-value of 0.05 was used to declare statistically significant difference between values before and after surgery.
Results
A hundred patients participated in the study. They all underwent cataract surgery in one eye. The thickness of peripapillary RNFL and of macular GCL and the VF test were evaluated before and one month after cataract surgery.
The mean age at the day of surgery was 72 ± 16 years. 47 (47%) of them were men and 53 (53%) were women. Of the 100 eyes considered, 54 (54%) were right eyes and 46 (46%) were left eyes.
No IOP increase was observed in any patient. Regarding the thickness of GCL, no significant difference was observed between the pre- and post-surgery values in any of the three parameters considered (macular: 14.28±2.86 µm vs 14.17±3.36 µm, p=0.72; para-macular: 45.22±7.52 µm vs 48.82±7.39 µm, p=0.18; peri-macular: 32.46±5.16 µm vs 32.43±3.87 µm, p=0.14) (Figure 1).
 |
Figure 1 Representative macular GCL scans from the same patient before and one month after cataract surgery. Image quality markedly improves following removal of media opacity, enabling better delineation of retinal layers. Although a slight postoperative increase in GCL thickness is visible in this example, such changes were not statistically significant across the study population. The observed improvement is likely attributable to enhanced OCT signal penetration and segmentation accuracy rather than true anatomical variation. |
As for the thickness of peripapillary RNFL, an increase in thickness was observed in all sectors except one after one month, with some values being statistically significant (central: 95.72±11.01 µm vs 100.45±13.31 µm, p=0.003; supero-temporal: 118.44±16.37 µm vs 123.27±20.01 µm, p=0.02; supero-nasal: 109.83±15.65 µm vs 116.09±17.94 µm, p=0.01; temporal: 65.44±15.82 µm vs 71.09±19.34 µm, p=0.02; nasal: 80.61±16.23 µm vs 88.27±16.61 µm, p=0.02), while others were not statistically significant (infero-temporal: 141.39±18.15 µm vs 145.45±18.21 µm, p=0.33). A reduction in thickness of the fiber layer was observed in the inferior-nasal sector without statistical significance (113.67±26.81 µm vs 113.27±30.70 µm, p=0.23) (Figure 2).
 |
Figure 2 Peripapillary RNFL analysis in the same patient pre- and post-cataract surgery. Enhanced OCT signal quality following lens removal leads to improved delineation of the RNFL contour, contributing to a measurable increase in reported thickness values. The apparent thickening in the differential analysis is likely artifactual and reflects improved image penetration and segmentation fidelity, rather than true neuroretinal structural change. |
Regarding changes in computerized VF test, variations were observed before and after surgery without statistical significance (VFI: 95.69±5.48 vs 92.6±17.05, p=0.55; MD −2.86±3.18 vs −2.89±5.05, p=0.92; PSD 2.99±1.97 vs 3.37±3.19, p=0.49).
The statistical analysis between preoperative and postoperative values is displayed in Table 1.
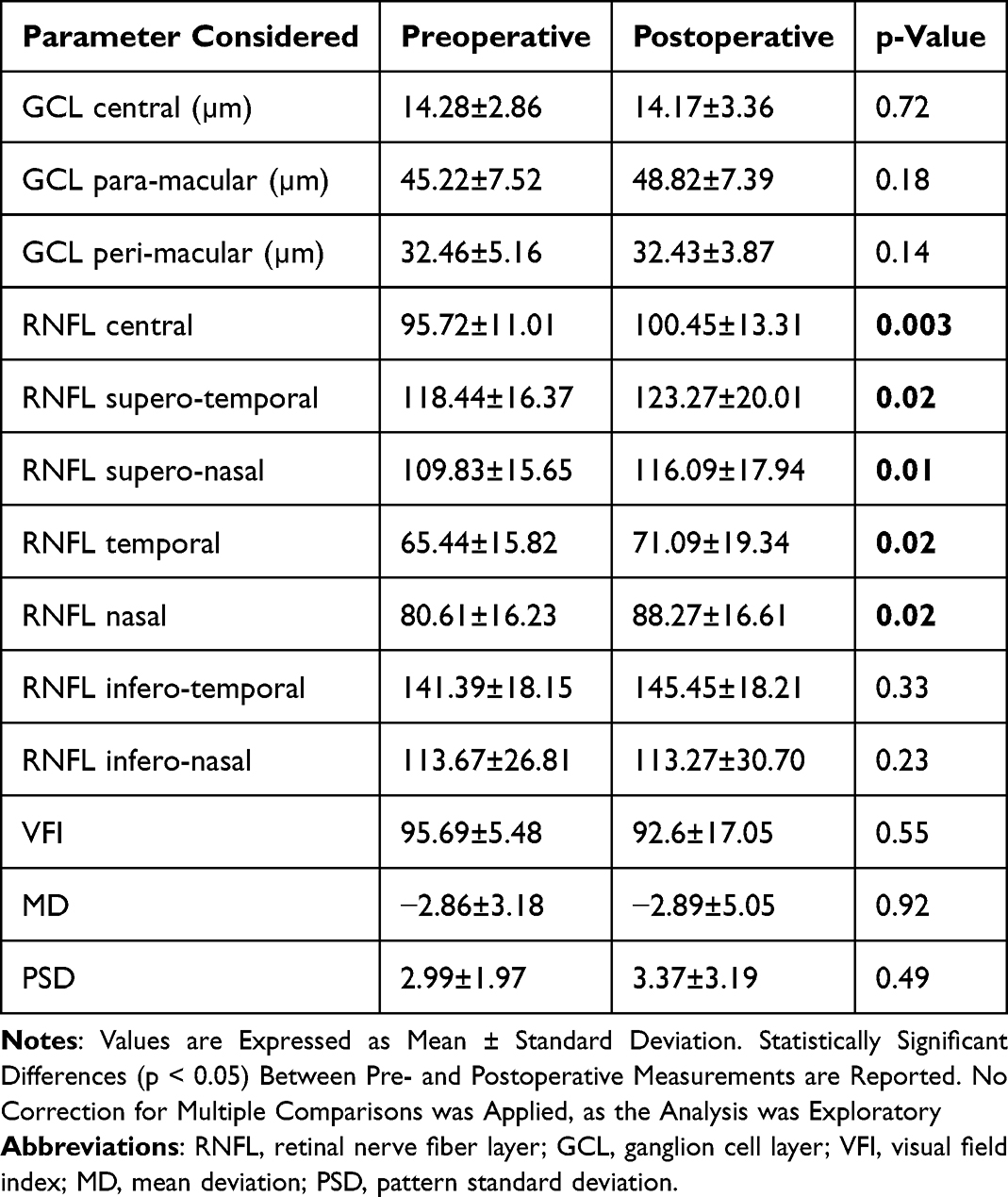 |
Table 1 Preoperative and Postoperative Measurements of GCL and RNFL Thickness, and Visual Field Parameters. |
Discussion
With the widespread utilization of cataract surgery, ophthalmologists have increasingly favored the utilization of augmented vacuum levels during phacoemulsification to enhance surgical efficiency. Nevertheless, elevated vacuum levels can lead to anterior chamber instability, necessitating heightened pressure infusion to uphold stability.11
Numerous studies have assessed IOP during cataract surgery, revealing significantly elevated IOP compared to central retinal artery pressure. This heightened IOP may compromise retinal blood flow, inducing retinal ischemia and subsequently impacting the cellular microenvironment, potentially triggering retinal ganglion cell apoptosis.12–14
Prior investigations have illustrated post-operative increases in macular GCL thickness as measured via OCT.15,16 Augmented macular thickness correlates with infusion duration under high simulated dynamic intraocular pressure (SDIOP).12
The fluidic system is a key component of phacoemulsification. It includes both gravitational and active fluidics systems, which are commonly used in clinical settings. The gravitational fluidics system’s irrigation pressure depends on bottle height and remains relatively constant. In contrast, the active fluidics system is paired with a cassette housing pressure sensors to constantly monitor intraocular pressure fluctuations. Recent advancements in phacoemulsification technology have introduced innovative strategies to address anterior chamber stability challenges in high-vacuum scenarios. Surgeons can now leverage sophisticated fluidics systems and real-time intraoperative monitoring to fine-tune vacuum levels and infusion pressures, thereby establishing a controlled and stable surgical milieu. The active fluidics system allows surgeons to preset and maintain a specific intraocular pressure by automatically replenishing fluids during surgery. Under these circumstances, stable intraocular pressure and anterior chamber volume values can be achieved. The CENTURION® Phacoemulsification System with ACTIVE SENTRY® technology is engineered with advanced features facilitating surgery at lower, physiological IOP and enhanced chamber stability.2 The incorporated pressure sensor in the ACTIVE SENTRY® Handpiece aids in mitigating post-occlusion swelling and sustaining anterior chamber stability by regulating IOP fluctuations. This innovation empowers surgeons to operate at reduced, physiological IOP levels alongside significantly elevated vacuum settings. The handpiece communicates with the system to adjust hardware and software parameters, ensuring stable intraocular pressure. The pressure sensor promptly identifies shifts in anterior chamber stability, prompting pressure plate adjustments in the balanced salt solution (BSS) irrigating bag, compensating for ocular changes. Maintaining a more physiological IOP during cataract surgery contributes to decreased corneal edema and diminished anterior segment inflammation (cells and flare) in the immediate postoperative period.13,17–20
In the scientific literature, there is limited investigation pertaining to the impact of this type of surgery on the optic nerve and macula.21–25
Similarly to what we found, Bambo et al, employing Spectralis® for OCT, observed an increase in peripapillary RNFL and GCL thickness. They attributed this outcome to improved transmission following cataract removal and artificial lens implantation, while dismissing the hypothesis that these changes have any pathological underpinnings.26
Parallel to our findings, also Dada et al, in their investigation of peripapillary RNFL thickness using scanning laser polarimetry with the Zeiss GDx VCC Retinal Scanner, also observed a statistically significant increase. They attributed this finding to an underestimation of fibers due to increased cataract birefringence.27
Even Kok et al, while studying retinal layers using different instruments than those employed in our study, arrived at the conclusion that lens opacity underestimates the thickness of retinal layers.28
Other authors have observed that even pupil size, which can undergo variations after cataract surgery, is capable of altering retinal thickness measurements detected by OCT.29,30
However, it is important to note that the presence of localized thickening in the peripapillary RNFL one month after surgery may have a logical basis in a phenomenon of fiber imbibition and edema, akin to what occurs at the macular level with postoperative cystoid macular edema (PCME).31 PCME is believed to result from the disruption of the blood-retinal barrier and the accumulation of inflammatory mediators in the macular region. Surgical trauma, release of prostaglandins, and the breakdown of the blood-aqueous barrier can trigger an inflammatory cascade, leading to increased vascular permeability and the leakage of fluid into the macular layers. Therefore, it is reasonable to hypothesize that such a phenomenon could also occur in the peripapillary RNFL.
An essential rationale underpinning our investigation was the need to assess whether cataract surgery conducted under controlled low-pressure settings—made possible by the Active Fluidics® technology—could truly minimize the risk of iatrogenic damage to the optic nerve head and adjacent neural structures. Given that both the RNFL and GCL are particularly sensitive to intraoperative IOP fluctuations, especially in vulnerable patient populations, determining the structural integrity of these tissues following surgery is of critical clinical interest.
Our findings suggest that low-pressure phacoemulsification maintains anatomical safety, as evidenced by the absence of significant changes in GCL thickness or functional alterations in the visual field. The observed postoperative increase in RNFL thickness is more plausibly linked to an underestimation of preoperative values due to lens-induced signal attenuation rather than true pathological change.
Nonetheless, one acknowledged limitation of the present study is its relatively short follow-up period of one month. While this timeframe is, in our opinion, the most biologically active and relevant for detecting early inflammatory or structural changes post-surgery, it does not exclude the possibility of late-onset alterations or long-term normalization of retinal parameters. The interpretation of RNFL thickening remains open-ended—potentially representing either transient fiber imbibition (analogous to postoperative macular edema) or improved optical resolution from media clarity.
To address these uncertainties, future studies with extended follow-up intervals are warranted. These would allow for a more granular understanding of the temporal dynamics of RNFL and GCL changes and offer insights into the long-term safety profile of low-pressure cataract surgery. Moreover, including patient populations with pre-existing glaucomatous damage could help determine whether such an approach also offers protective benefits in compromised optic nerves. We are currently planning prospective longitudinal studies to pursue these avenues.
It is important to note that in glaucomatous eyes, especially those with advanced optic disc cupping as well as in patients with systemic hypotension or carotid artery disease, even short-lasting intraoperative elevations in infusion pressure may pose a significant risk to optic nerve perfusion. In such cases, setting a maximum infusion pressure of 50 mmHg may be inappropriate, and substantially lower pressure targets should be considered to minimize potential harm to compromised optic nerves.
In any case, our study, featuring a notably large patient cohort, clearly highlights that both at RNFL and GCL levels, the utilization of the Centurion Vision System and Active Fluidics enables a safe surgical procedure in terms of potential retinal damage. Our findings underscore the efficacy of employing the Centurion Vision System and Active Fluidics to minimize the risk of retinal complications after surgery. The comprehensive patient data analyzed in our study emphasize the significant contribution of these advanced technologies to ensuring a secure and successful surgical outcome, particularly in safeguarding against the occurrence of retinal injuries.
It is important to highlight that some well consolidated method to preoperative reduce the IOP such as mannitol, thus creating space in the anterior chamber of short eyes, might be relevant in the modulation in the intraoperative infusion pressure.32
A notable limitation of this study is undoubtedly the restricted follow-up period. Indeed, if it were observed that the increase in RNFL thickness persists in the months following surgery, this could suggest an augmentation due to improved tomographic resolution. Conversely, if the fiber thickness were to return to values similar to pre-surgery levels as the months progress, this could be explained by a transient fiber imbibition that, akin to cystoid macular edema, diminishes over time. Hence, further extensive studies are imperative in this regard.
Additionally, all patients included in this study are without glaucoma; it would be valuable to assess whether the same safety profile exists in these patients who are known to have early damage to GCL and RNFL. This could lay the groundwork for a targeted surgical strategy in glaucomatous patients to minimize surgery-induced damage.
Conclusions
In this study concerning tomographic (OCT) and functional (VF test) alterations after cataract surgery using the Centurion Vision System and Active Fluidics, we observed that there are no significant alterations in GCL and retinal functionality. Simultaneously, we noted an increase in peripapillary RNFL, possibly due to the well-known mechanism of fiber underestimation reported in the literature, or to a potential transient fiber imbibition. Nonetheless, from the presented data, it is evident that the Alcon® system enables safe surgery with reliable long-term outcomes and without significant retinal damage.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Italian legislation and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical Approval was obtained from IRCCS Humanitas Research Hospital.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Funding
No funding was received for this research.
Disclosure
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
References
1. Chang VS, Gibbons A, Osigian C. Phacoemulsification in the setting of corneal endotheliopathies: a review. Int Ophthalmol Clin. 2020;60(3):71–89. PMID: 32576725; PMCID: PMC7360340. doi:10.1097/IIO.0000000000000315
2. Davison JA. Two-speed phacoemulsification for soft cataracts using optimized parameters and procedure step toolbar with the CENTURION vision system and balanced tip. Clin Ophthalmol. 2015;9:1563–1572. PMID: 26355695; PMCID: PMC4559244. doi:10.2147/OPTH.S90245
3. Sharif-Kashani P, Fanney D, Injev V. Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems. BMC Ophthalmol. 2014;14(1):96. PMID: 25074069; PMCID: PMC4134114. doi:10.1186/1471-2415-14-96
4. Sharma N, Singhal D, Nair SP, Sahay P, Sreeshankar SS, Maharana PK. Corneal edema after phacoemulsification. Indian J Ophthalmol. 2017;65(12):1381–1389. PMID: 29208818; PMCID: PMC5742966. doi:10.4103/Ijo.IJO_871_17
5. Yi DH, Dana MR. Corneal edema after cataract surgery: incidence and etiology. Semin Ophthalmol. 2002;17(3–4):110–114. PMID: 12759837. doi:10.1076/Soph.17.3.110.14783
6. Sihota R, Gupta S, Angmo D. Evaluation of macular ganglion cell analysis compared to retinal nerve fiber layer thickness for pre-perimetric glaucoma diagnosis. Indian J Ophthalmol. 2018;66(4):491–493. PMID: 29582806; PMCID: PMC5892048. doi:10.4103/Ijo.IJO_235_18
7. Roh HC, Park CY, Kim M. Changes of the macular ganglion cell-inner plexiform layer thickness after cataract surgery in glaucoma patients. J Ophthalmol. 2016;2016:9785939. PMID: 28101378; PMCID: PMC5214588. doi:10.1155/2016/9785939
8. Choi YJ, Seol BR. Effects of cataract on retinal nerve fiber layer and ganglion cell-inner plexiform layer thickness on swept source optical coherence tomography. Korean J Ophthalmol. 2023;37(1):12–22. PMID: 36281576; PMCID: PMC9935059. doi:10.3341/Kjo.2022.0097
9. The Longitudinal Study of Cataract Study Group; Chylack LT, Wolfe JK, Singer DM, et al. The lens opacities classification system III. Arch Ophthalmol. 1993;111(6):831–836. doi:10.1001/Archopht.1993.01090060119035
10. Di Maria A, Tredici C, Cozzupoli GM, Vinciguerra P, Confalonieri F. Effects of prostaglandin analogues on epiphora persistence after EN-DCR: a hypothesis-generating study. Eur J Ophthalmol. 2023;33(1):182–187. doi:10.1177/11206721221106138
11. Khng C, Packer M, Fine IH, Hoffman RS, Moreira FB. Intraocular Pressure during Phacoemulsification. J Cataract Refract Surg. 2006;32(2):301–308. doi:10.1016/j.jcrs.2005.08.062
12. Chen D, Zhu J, Li J, Ding XX, Lu F, Zhao YE. Effect of simulated dynamic intraocular pressure on retinal thickness measured by optical coherence tomography after cataract surgery. Int J Ophthalmol. 2012;5(6):687–693. doi:10.3980/j.issn.2222-3959.2012.06.07
13. Zhao Y, Li X, Tao A, Wang J, Lu F. Intraocular pressure and calculated diastolic ocular perfusion pressure during three simulated steps of phacoemulsification in vivo. Invest Ophthalmol Vis Sci. 2009;50(6):2927–2931. doi:10.1167/iovs.08-2996
14. Findl O, Strenn K, Wolzt M, et al. Effects of changes in intraocular pressure on human ocular haemodynamics. Curr Eye Res. 1997;16(10):1024–1029. doi:10.1076/ceyr.16.10.1024.9024
15. Celik E, Cakır B, Turkoglu EB, Doğan E, Alagoz G. Effect of cataract surgery on subfoveal choroidal and ganglion cell complex thicknesses measured by enhanced depth imaging optical coherence tomography. Clin Ophthalmol. 2016;10:2171–2177. doi:10.2147/OPTH.S105992
16. Pardianto G, Moeloek N, Reveny J, et al. Retinal thickness changes after phacoemulsification. Clin Ophthalmol. 2013;7:2207–2214. doi:10.2147/OPTH.S53223
17. Yesilirmak N, Diakonis VF, Sise A, et al. Differences in energy expenditure for conventional and femtosecond-assisted cataract surgery using 2 different phacoemulsification systems. J Cataract Refract Surg. 2017;43(1):16–21. doi:10.1016/j.jcrs.2016.11.037
18. Liu J, Liu Q, Yu H, et al. Microvascular changes in macular area after phacoemulsification and its influencing factors assessed by optical coherence tomography angiography. TCRM. 2021;17:405–414. doi:10.2147/TCRM.S309679
19. Yu S, Frueh BE, Steinmair D, et al. Cataract significantly influences quantitative measurements on swept-source optical coherence tomography angiography imaging. PLoS One. 2018;13(10):E0204501. doi:10.1371/journal.pone.0204501
20. Li T, Guadie A, Feng L, et al. Influence of cataract surgery on macular vascular density in patients with myopia using optical coherence tomography angiography. Exp Ther Med. 2020;20(6):1. doi:10.3892/etm.2020.9129
21. Krizanovic A, Bjelos M, Busic M, et al. Macular perfusion analysed by optical coherence tomography angiography after uncomplicated phacoemulsification. 1986
22. Luo Y, Bjeloš M, Bušić M, et al. Benefits beyond restoring vision. BMC Ophthalmol. 2021;21(1):71. doi:10.1186/s12886-021-01837-2
23. Hilton EJR, Hosking SL, Gherghel D, et al. Beneficial effects of small-incision cataract surgery in patients demonstrating reduced ocular blood flow characteris tics. Eye. 2005;19(6):670–675. doi:10.1038/sj.eye.6701620
24. Feng L, Azhati G, Li T, et al. Macular vascular density changes following cataract surgery in diabetic patients: an optical coherence tomography angiog raphy study. J Ophthalmol. 2021;2021:1–7. doi:10.1155/2021/4717996
25. Pilotto E, Leonardi F, Stefanon G, et al. Early retinal and choroidal OCT and OCT angiography signs of inflammation after uncomplicated cataract surgery. Br J Ophthalmol. 2019;103(7):1001–1007. doi:10.1136/bjophthalmol-2018-312461
26. Bambo MP, Garcia-Martin E, Otin S, et al. Influence of cataract surgery on repeatability and measurements of spectral domain optical coherence tomography. Br J Ophthalmol. 2014;98(1):52–58. PMID: 24174613. doi:10.1136/Bjophthalmol-2013-303752
27. Dada T, Behera G, Agarwal A, Kumar S, Sihota R, Panda A. Effect of cataract surgery on retinal nerve fiber layer thickness parameters using scanning laser polarimetry (GDxVCC). Indian J Ophthalmol. 2010;58(5):389–394. PMID: 20689193; PMCID: PMC2992913. doi:10.4103/0301-4738.67048
28. Kok PH, van Den Berg TJ, van Dijk HW, et al. The relationship between the optical density of cataract and its influence on retinal nerve fibre layer thickness measured with spectral domain optical coherence tomography. Acta Ophthalmol. 2013;91(5):418–424. PMID: 23106951. doi:10.1111/j.1755-3768.2012.02514.x
29. Savini G, Zanini M, Barboni P. Influence of pupil size and cataract on retinal nerve fiber layer thickness measurements by stratus OCT. J Glaucoma. 2006;15(4):336–340. PMID: 16865012. doi:10.1097/01.Ijg.0000212244.64584.C2
30. Savini G, Carbonelli M, Parisi V, et al. Effect of pupil dilation on retinal nerve fibre layer thickness measurements and their repeatability with cirrus HD-OCT. Eye. 2010;24(9):1503–1508. doi:10.1038/Eye.2010.66
31. Egger EG. The Irvine–Gass syndrome. Ophthalmologica. 1973;167(5):443–445. PMID: 4771495. doi:10.1159/000306992
32. Di Maria A, Ferraro V, Barone G, Gaeta A, Vinciguerra P, Confalonieri F. Preoperative intravenous mannitol administration and its rationale before cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2024. doi:10.1007/s00417-024-06589-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.