")
Back to Journals » Clinical Ophthalmology » Volume 19
Impact of Environmental Exposure on Ocular Surface Balance: A Comparative Study
Authors Alghamdi WM
Received 12 November 2024
Accepted for publication 7 February 2025
Published 3 March 2025 Volume 2025:19 Pages 747—752
DOI https://doi.org/10.2147/OPTH.S504021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Waleed M Alghamdi
Department of Optometry, College of Applied Medical Sciences, Qassim University, Buraydah, Saudi Arabia
Correspondence: Waleed M Alghamdi, Department of Optometry, College of Applied Medical Sciences, Qassim University, Qassim, Buraydah, Saudi Arabia, Tel +966503229636, Fax +966-16-3800050, Email [email protected]
Purpose: Environmental factors such as high temperatures, low humidity, ultraviolet radiation, wind, and dust can harm ocular surface health, increasing dry eye disease risk, especially in harsh climates like central Saudi Arabia. Thus, the purpose of this study is to investigate the impact of outdoor environmental exposure on ocular surface stability by comparing ocular surface parameters between participants exposed to harsh outdoor conditions and those in indoor environments in central Saudi Arabia.
Patients and Methods: A cross-sectional study was conducted in May 2024 with 40 male participants divided equally into two groups: those exposed to outdoor environments and those in indoor settings. Clinical assessments included Non-Invasive Keratographic Break-Up Time (NIKBUT) to evaluate tear film stability, lipid layer thickness measurement, meibomian gland evaluation using meiboscore and gland expressibility, Tear Meniscus Height (TMH), conjunctival redness grading, and the Ocular Surface Disease Index (OSDI) questionnaire. Data were analysed to identify the differences between the groups; a P-value less than 0.05 was considered statistically significant.
Results: Participants exposed to outdoor environments exhibited significantly shorter NIKBUT (12.35± ± 6.76 seconds) compared to indoor participants (18.50± ± 8.54 seconds), P = 0.016, indicating increased tear film instability. The outdoor group had higher lipid layer thickness (1.60± ± 0.50 units; P < 0.009), greater meiboscores (1.25± ± 0.44; P < 0.010), and increased conjunctival redness scores compared to those in indoor environments (P = 0.016). No significant differences were observed in TMH or meibomian gland expressibility between the groups. Although OSDI scores were higher in the outdoor-exposed group, this difference did not reach statistical significance.
Conclusion: Exposure to harsh outdoor environments adversely affects ocular surface health, increasing the risk of dry eye disease among individuals in central Saudi Arabia. Implementing protective measures like UV-protective eyewear and regular eye examinations can help mitigate these effects.
Keywords: dry eye disease, risk factors, public health, Outdoor activity, Saudi Arabia
Introduction
Dry eye disease (DED) is a prevalent, multifactorial disorder of the ocular surface that affects millions of people worldwide. It is characterized by symptoms such as ocular discomfort, visual disturbances, and tear film instability, potentially leading to inflammation and damage to the ocular surface.1,2 The global prevalence of DED varies widely, ranging from 5% to 50%, depending on factors such as the population studied, geographic location, and diagnostic criteria employed.1,3,4 In regions with harsh environmental conditions, such as the Middle East, the prevalence is notably higher. A recent systematic review and meta-analysis estimated the prevalence of DED and associated risk factors among the Middle East population. It showed that the prevalence was 28.33%, and the main risk factors were contact lens use, prolonged screen time, systemic disorders, glaucoma medications, allergies, and refractive surgery.5 A study conducted in Saudi Arabia reported that approximately 32% of the population experiences dry eye symptoms, indicating a significant public health concern.6
Central Saudi Arabia, including regions like Riyadh and Al-Qassim, experiences extreme weather conditions that potentially contribute to tear film instability and adversely affect ocular surface health. Temperatures can soar as high as 48 °C during the summer months and drop below 0 °C in winter, accompanied by low humidity levels often below 20%.6,7 This creates a dry environment that accelerates tear evaporation. Additionally, individuals working outdoors are exposed to high levels of ultraviolet (UV) radiation, wind, and dust, which can further disrupt the tear film and damage the ocular surface.8
Outdoor workers, such as construction workers, farmers, and traffic officers, are potentially more susceptible to DED due to prolonged exposure to these environmental stressors. Studies have shown that environmental factors like high temperature, low humidity, wind, and increased UV exposure can lead to increased tear film evaporation, resulting in tear film instability and lead to dry eye symptoms.9,10 Moreover, meibomian gland dysfunction (MGD), a leading cause of evaporative dry eye, may be exacerbated under these conditions. The increased tear evaporation reduces the protective lipid layer secreted by the meibomian glands, essential for tear film stability.11,12
Despite these environmental challenges, there is a paucity of research specifically addressing the impact of extreme weather conditions on DED among individuals exposed to outdoor environments in Saudi Arabia. Most studies focus on general populations without distinguishing between exposure to outdoor environments and control groups. The present study addresses a critical gap in research on how extreme outdoor environments in Saudi Arabia affect ocular surface balance compared to indoor conditions. By highlighting these environmental impacts, it underscores the importance of preventive measures, such as hydration, protective clothing, and activity scheduling, to protect the health and well-being of outdoor workers. This study aims to fill this gap by evaluating the effect of exposure to outdoor environments versus control conditions on tear film integrity, meibomian gland health, and ocular surface condition in individuals residing in central Saudi Arabia. By understanding how environmental factors contribute to DED among those exposed to outdoor environments, we can develop targeted clinical strategies and preventive measures to manage and reduce the incidence of DED in populations exposed to extreme weather conditions.
Material and Methods
Study Design
A cross-sectional study was conducted to examine tear film quality and meibomian gland dysfunction among individuals exposed to outdoor environments and a control group that remain indoors throughout the day in central Saudi Arabia. The study was conducted in May, when temperatures in Central Saudi Arabia soared as high as 48°C, with low humidity levels often below 20%.6,7
Sampling Technique
A non-probability sampling method was used to select 40 healthy male participants. The sample included 20 participants who engaged in outdoor activities for at least 4 hours per day and 20 participants who primarily engaged in indoor activities.
Participants
The study included 40 healthy male participants divided equally into two groups. The outdoor-exposed group consisted of individuals whose nature of work exposes them to at least 4 hours per day of outdoor environments (n = 20). The control group comprised individuals who predominantly remain indoors throughout the day (n = 20).
Eligibility Criteria
The study included male participants who were aged between 20 and 35 years, had no history of systemic or ocular diseases, were not using any medications known to cause dry eye, and had no previous ocular surgeries. Individuals were excluded if they had any ocular or systemic disease that may cause dry eye (including diabetes mellitus), had undergone refractive surgery, were over 35 years of age, were using medications that may induce dry eye, or had any previous eye surgery.
Data Collection Procedures
All participants underwent assessments categorized into three main areas:
Vision Assessment
Visual acuity was assessed using a standard Snellen chart to confirm normal or corrected-to-normal vision.
Symptoms Assessment
Participants completed the Ocular Surface Disease Index (OSDI) questionnaire prior to objective testing to assess subjective symptoms of dry eye disease. The questionnaire was translated into Arabic and culturally validated to ensure its relevance and accuracy for the population studied. The OSDI consists of 12 questions divided into three subscales: ocular symptoms, visual function, and environmental triggers. Each question is scored from 0 (none of the time) to 4 (all the time), and the overall score is calculated to determine the severity of dry eye symptoms.
Ocular Surface Assessment
The ocular surface and meibomian gland function were assessed using clinical examinations and advanced imaging techniques. The Oculus Keratograph 5M was utilized to assess parameters such as tear meniscus height (TMH), non-invasive keratograph break-up time (NIKBUT), meibography, tear film lipid layer quality, and scleral redness grading (R-Scan). Additionally, a slit-lamp biomicroscope was used to examine the ocular surface and eyelids, employing the Efron Grading Scale to grade the severity of conditions like bulbar redness, limbal redness, lid abnormalities, corneal staining, and meibomian gland dysfunction.
Ethical Considerations
Ethical permission was obtained from the Institutional Review Board of Al-Qassim University (approval number 23-60-04), and the study adhered to the Declaration of Helsinki guidelines. Written informed consent was obtained from all participants after explaining the study’s aim. Participants were able to withdraw from the study at any time, and no remuneration was offered for participation. Data were collected confidentially without any individual information being recorded.
Statistical Analysis
Data were entered into Microsoft Excel and analysed using Jamovi software (Version 2.3). Descriptive statistics, including means and standard deviations, were calculated for all continuous variables. An independent t-test was used to compare mean values between the indoor and outdoor groups, with a p-value of less than 0.05 considered statistically significant.
Results
A total of 40 male participants completed the study, with a mean age of 23.98 ± 2.25 years. Only males were included because it is uncommon in Saudi Arabia for females to work in outdoor environments, ensuring the study accurately reflects the population exposed to such conditions. Participants were equally divided into control and outdoor-exposed groups. The one-sample Kolmogorov–Smirnov test showed that the collected data were distributed normally with a p-value greater than 0.50.
Participants exposed to outdoor environments exhibited significant differences in several ocular surface parameters compared to the control group. Specifically, the Non-Invasive Keratographic Break-Up Time (NIKBUT) was significantly shorter in the outdoor group (mean ± SD: 12.35 ± 6.76 seconds) than in the control group (18.50 ± 8.54 seconds; p = 0.016), as shown in Figure 1.
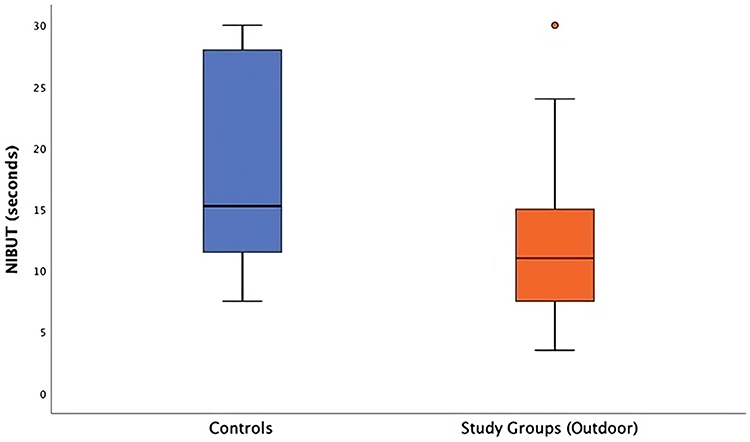 |
Figure 1 Box plot of Non-Invasive Keratographic Break-Up Time (NIBUT) comparing control and outdoor-exposed groups, showing a significantly shorter NIBUT in the outdoor group (p = 0.016). |
Additionally, the meiboscore, reflecting meibomian gland dropout assessed through meibography, was higher in the outdoor group (1.25 ± 0.44) compared to the control group (0.85 ± 0.49; p = 0.010). The lipid layer thickness was significantly higher in the outdoor group (1.60 ± 0.50 units) compared to the control group (1.20 ± 0.41 units; p = 0.009). Conjunctival redness scores were also significantly elevated in the outdoor group (1.25 ± 0.44) compared to the control group (1.00 ± 0.00; p = 0.016). Box plot of meiboscore values for control and outdoor-exposed groups, indicating a significantly higher meiboscore in the outdoor group (p = 0.010), as presented in Figure 2.
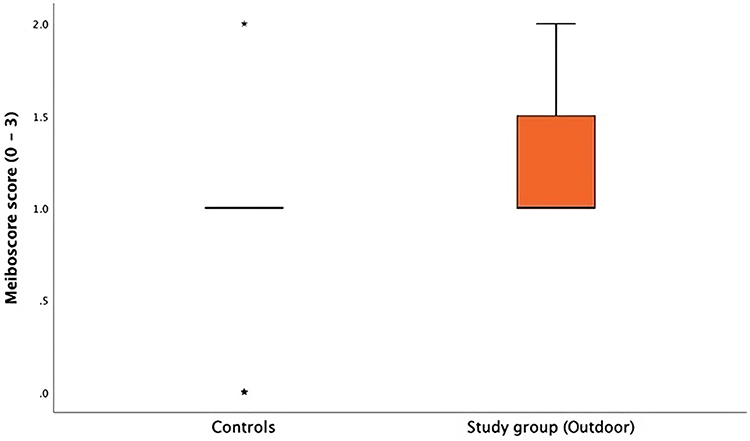 |
Figure 2 Box plot of meiboscore values for control and outdoor-exposed groups, indicating a significantly higher meiboscore in the outdoor group (p = 0.010). Outlier=*. |
In contrast, there were no significant differences between the groups in the Ocular Surface Disease Index (OSDI) scores, Tear Meniscus Height (TMH), and meibomian gland expressibility, as shown in Figure 3.
 |
Figure 3 Box plot comparing Ocular Surface Disease Index (OSDI) scores between control and outdoor-exposed groups, showing no significant difference between the groups (p = 0.256). Outlier=*. |
Discussion
The present study assessed the impact of harsh outdoor environmental exposure on ocular surface health by comparing young, healthy male participants exposed to outdoor conditions with those in indoor environments in central Saudi Arabia. The most significant findings were the higher meiboscores and shorter Non-Invasive Keratographic Break-Up Time (NIKBUT) in the outdoor-exposed group compared to the control group.
Although the meiboscore and NIKBUT values for the outdoor group were significantly different from those of the control group, they remained within normal clinical ranges. This suggests that environmental exposure is initiating early ocular surface changes that are subclinical at this stage. The elevated meiboscore indicates initial meibomian gland dropout, while the shortened NIKBUT reflects decreased tear film stability both are key factors in the development of evaporative dry eye disease.1,13 The lack of significant difference in the Ocular Surface Disease Index (OSDI) scores between the groups indicates that these early objective changes have not yet manifested as subjective symptoms. This discrepancy between clinical signs and symptoms is common in dry eye research and may be due to individual variability in symptom perception or the early stage of ocular surface alterations.14 As these subclinical changes progress, they may lead to significant discomfort and visual disturbances, highlighting the importance of early detection and intervention.
Increased conjunctival redness was also observed in the outdoor group, indicating heightened ocular surface inflammation. Exposure to ultraviolet (UV) radiation, wind, and dust prevalent in outdoor environments can induce oxidative stress and inflammatory responses in ocular tissues.15,16 Airborne particulates contribute to mechanical irritation, further exacerbating inflammation.14,17 These factors collectively contribute to ocular surface damage, increasing the risk of developing dry eye disease.
Interestingly, there were no significant differences between the groups in Tear Meniscus Height (TMH) and meibomian gland expressibility. This suggests that aqueous tear production and the functionality of remaining meibomian glands may not be compromised at this stage. It supports the notion that increased tear evaporation, rather than reduced tear secretion, is the primary issue affecting the outdoor-exposed participants.9 These findings imply that environmental exposure initiates early ocular surface changes that are not yet symptomatic but could progress over time. Recognizing these early alterations underscores the importance of implementing preventive strategies to preserve ocular surface health in individuals exposed to extreme environmental conditions.
The present study has the same limitations. The sample size was relatively small, comprising 40 participants, which may limit the generalizability of the findings. A larger sample size would enhance statistical power and provide more robust conclusions. The study was conducted over a short period, which may limit its ability to capture long-term or seasonal variations in ocular surface stability. Conducting longitudinal studies or including multiple seasons would provide more comprehensive data. Additionally, all participants were young, healthy males. While this homogeneity controls for age and gender-related variables, it limits the applicability of the results to other populations, including females and older individuals. Future studies should include females and older individuals to enhance generalizability. In Saudi Arabia, it is uncommon for females to work in outdoor environments, which justifies their exclusion; however, hormonal differences can influence ocular surface health and may yield different results in a more diverse population.11
Conclusion
The outdoor environmental exposure significantly impacts ocular surface health, increasing the risk of tear film instability, lipid layer dysfunction, meibomian gland dropout, and ocular surface inflammation, all of which are key factors in developing dry eye disease. However, meiboscore and NIKBUT changes are within normal ranges, and subjective symptoms were not significantly different; these early alterations may progress over time. Protective measures such as using UV-protective eyewear, adjusting exposure schedules, and encouraging hydration can help mitigate risks. Regular ocular assessments are essential for early detection and management of ocular surface changes in those exposed to harsh outdoor environments.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Craig JP, Nichols KK, Akpek EK. et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
2. Tsubota K, Yokoi N, Shimazaki J, et al. New Perspectives on Dry Eye Definition and Diagnosis: a Consensus Report by the Asia Dry Eye Society. Ocul Surf. 2017;15(1):65–76. doi:10.1016/j.jtos.2016.09.003
3. Papas EB. The global prevalence of dry eye disease: a Bayesian view. Ophthalmic Physiol Opt. 2021;41(6):1254–1266. doi:10.1111/opo.12888
4. Mohamed Z, Alrasheed SH. A Systematic Review and Meta-analysis of Convergence Insufficiency Prevalence and Management Options. Open Ophthalmol J. 2023;17:1–7.
5. Mohamed Z, Alrasheed S, Abdu M, et al. K. Dry Eye Disease Prevalence and Associated Risk Factors Among the Middle East Population: a Systematic Review and Meta-Analysis. Cureus. 2024;16:1–10.
6. Alshamrani AA, Almousa AS, Almulhim AA, et al. Prevalence and Risk Factors of Dry Eye Symptoms in a Saudi Arabian Population. Middle East Afr J Ophthalmol. 2017;24(2):67–73. doi:10.4103/meajo.MEAJO_281_16
7. Helayel HB, Al Abdulhadi HA, Aloqab A, et al. Prevalence and Risk Factors of Dry Eye Disease among Adults in Saudi Arabia. Saudi J Med Med Sci. 2023;11:242–249.
8. Uchino M, Schaumberg DA. Dry Eye Disease: impact on Quality of Life and Vision. Curr Ophthalmol Rep. 2013;2(2):
9. Alves M, Novaes P, Morraye Mde A, et al. Is dry eye an environmental disease? Arq Bras Oftalmol. 2014;77(3):193–200. doi:10.5935/0004-2749.20140050
10. Zhang X, Vj M, Qu Y, et al. Dry Eye Management: targeting the Ocular Surface Microenvironment. Int J mol Sci. 2017;18(7):1398–1400. doi:10.3390/ijms18071398
11. Schaumberg DA, Nichols JJ, Papas EB, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on the epidemiology of, and associated risk factors for, MGD. Invest Ophthalmol Vis Sci. 2011;52(4):1994–2005. doi:10.1167/iovs.10-6997e
12. Alghamdi WM, Alrasheed SH. Impact of an educational intervention using the 20/20/20 rule on Computer Vision Syndrome. Afr Vision Eye Health. 2020;79:1–6.
13. Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2011;52 (4):2050–2064. doi:10.1167/iovs.10-6997g
14. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
15. Parisi AV, Sabburg J, Kimlin MG. Scattered and filtered solar UV measurements. Springer Sci Bus Media. 2004;4:22.
16. Chen X, Utheim ØA, Xiao J, et al. Meibomian gland features in a Norwegian cohort of patients with primary Sjögren´s syndrome. PLoS One. 2017;12:1–8.
17. Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438–510. doi:10.1016/j.jtos.2017.05.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.