")
Back to Journals » Clinical Ophthalmology » Volume 18
Impact of Lipid Parameters on Visual Acuity Change in Non-Arteritic Anterior Ischemic Optic Neuropathy
Authors Kemchoknatee P , Arjkongharn N , Pongpirul K
Received 11 October 2024
Accepted for publication 8 December 2024
Published 16 December 2024 Volume 2024:18 Pages 3791—3800
DOI https://doi.org/10.2147/OPTH.S500368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Parinee Kemchoknatee,1 Niracha Arjkongharn,1 Krit Pongpirul2
1Department of Ophthalmology, Rajavithi Hospital, Bangkok, Thailand; 2Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Correspondence: Parinee Kemchoknatee, Department of Ophthalmology, Rajavithi Hospital, 2, Phayathai Road, Bangkok, 10400, Thailand, Email [email protected]
Purpose: To assess the potential influence of serum biochemical factors, specifically lipid profile parameters, on visual outcomes in patients with non-arteritic anterior ischemic optic neuropathy (NAION).
Patients and Methods: All patients diagnosed with NAION at Rajavithi Hospital between 1 January 2011 and 31 December 2020 were retrospectively reviewed. The primary outcome was defined as visual recovery, measured by an improvement of at least 0.2 logarithm of the minimal angle of resolution (logMAR) in their best-corrected visual acuity (BCVA) at the 12-weeks follow-up visit compared to the initial visit and determine whether those lipid profiles parameters are predictive of 12 weeks-visual outcomes. Factors of an initial poor VA were evaluated using logistic regression analysis.
Results: In this study, 84 patients with NAION were included to assess the impact of lipid parameters on visual outcomes. Majority of participants were male. The group with initial VA worse than 20/200 had significantly higher mean age of 58.3± 7.6 years and levels of total cholesterol (TC), triglycerides (TG), and low-density lipoprotein cholesterol (LDL) (all p < 0.05 respectively). Throughout 12 weeks, a significant difference in change of BCVA between the two groups of initial VA was observed (p< 0.001). Regarding lipid parameters on visual prognosis, lipid profile between the two groups of VA improvement of 0.2 logMAR was comparable different. The probability of VA improvement showed a weak association with TC levels. A gradual increase in probability slightly related to LDL parameter, while TG showed an inverse relationship. At elevated lipid levels, there was a greater degree of uncertainty in predicting visual outcomes.
Conclusion: While older age and elevated lipid levels, specifically TC, TGs, and LDL, were correlated with poorer initial visual acuity in NAION patients, no significant associations were identified between lipid parameters and long-term visual recovery. Early detection for individuals with dyslipidemia (DLP) and advanced age merit attention.
Keywords: non-arteritic anterior ischemic optic neuropathy, NAION, visual acuity, total cholesterol, triglycerides, LDL, TC, low-density lipoprotein, TG
Introduction
Non-Arteritic Ischemic Optic Neuropathy (NAION) is one of the most common optic neuropathies in patients with older than 50 years. An estimated annual incidence is 10.3 for all ages and 2.3 to 10.2 per every 100,000 persons for older age.1,2 Vision of affecting eyes has ranged from nearly normal to devastating vision.3 Visual recovery of the disease is approximately 40%, yet some patients may suffer from poor improvement resulting a devastating visual outcome.4 Presently, there is no effective treatment or promising improvement vision.5 Pathology of NAION is mostly believed due to vascular insufficiency of short posterior ciliary artery resulting in individual presented with painless visual loss, color vision impairment, and a disc swelling appearance.6
Several systemic vascular risk factors of NAION development have been investigated including diabetic mellitus, dyslipidemia (DLP), and hypertension in previous literatures.7,8 DLP has been established the atherogenesis development, vascular compromise, and vascular endothelial dysfunction from high level of total cholesterol (TC), triglyceride (TG), and low-density lipoprotein cholesterol (LDL), resulting in a decrease of vascular blood supply at optic nerve.9
The associations between systemic vascular diseases and visual outcomes of NAION have differed among previous studies.3,10,11 Hayreh et al observed no correlation among those systemic vascular diseases and visual status (VA, visual field) at 1 year-period.3 Similar to an Indian population, Patil et al also evaluated no association of those systemic vascular risks and the VA of 20/200.12 While Koçak et al proposed that atherogenic indices (ratio of TC, LDL to HDL) was notably higher in patients who failed to achieve VA of 20/200 in western populations; however, no investigations of trends in VA recovery based on lipid parameters, and these findings may have limited generalizability to other populations.13 Investigating the influence of DLP on the clinical course of NAION, particularly in mitigating initial visual loss, may offer a promising therapeutic approach in the future. With regard to Southeast Asia populations, no study has investigated the association of DLP, lipid parameters and visual prognosis or improvement of patients with NAION.
The purpose of the present study was to examine the association of lipid parameters, DLP on the visual outcome of patients with NAION at Rajavithi Hospital, Thailand.
Patients and Methods
Method and Data Collection
In this retrospective cohort study, the electronic medical records of 189 patients diagnosed with NAION between 1 January 2011 and 31 December 2020 were retrospectively reviewed.
The inclusion criteria were NAION patients diagnosed during the study period by ophthalmologists in our hospital which employed diagnostic criteria based on Sharma et al as follows: acute painless visual loss with the evidence of optic neuropathy including presence of relative afferent pupillary defect (RAPD); presenting a swelling disc morphology within one month; impaired color vision test; or nerve fiber layer defect pattern on visual field test.11
The exclusion criteria were patients with the following: 1) no data of serum lipid level after an initial diagnosis of NAION; 2) other optic neuropathy such as optic neuritis, compressive optic neuropathy; 3) other retinal diseases, for example proliferative diabetic retinopathy, macular edema; 4) other eye diseases affecting visual acuity or visual field assessments; 5) follow-up time of less than 3 months; 6) having an onset duration greater than 30 days; and 7) optic neuropathy with a history of previous intraocular surgery within 1 month.
Demographic and patient characteristics after diagnosed NAION were retrospectively reviewed including age and gender. Ophthalmic characteristic included best-corrected visual acuity (BCVA) which was converted to logarithm of the minimal angle of resolution (logMAR) as the follows; no light perception (NLP), light perception (LP), hand motion (HM), and counting finger (CF) to 3.4, 3.1, 2.9, and 2.6 respectively,14 color vision tested by Ishihara color plate, pupillary defect, fundus and optic disc examination. Visual field was tested with Humphrey Field Analyzer HFA II 750 (Carl Zeiss Meditec Inc, Dublin, CA) using a 24-2 threshold program with the Swedish Interactive Threshold Algorithm (SITA) Fast strategy. Biochemistry data of lipid profiles including serum of TC, TG, and LDL were retrospectively reviewed after diagnosed NAION.
In our study, the primary outcome was defined as visual recovery, measured by an improvement of at least 0.2 logMAR in BCVA at the 12-weeks follow-up visit compared to the initial visit. A change of BCVA in each visit of initial, 1-week, 4-weeks and 12-weeks period was also retrospectively reviewed.
Ethics Approval
The study was approved by Rajavithi Hospital Research Ethics Committee (EC number 123/2567), Chulalongkorn University (COA number of 0227/2024) and followed the tenet of the declaration of Helsinki. All the patients provided written informed consent before participating the study.
Statistical Analysis
All affected eyes which met the inclusion criteria were recruited in the present study. Categorical data were expressed as percentage. Continuous data were expressed as mean, and standard deviation (SD) for normal distributed data or expressed as median, interquartile range (IQR) for non-normal distributed data. The comparison of categorical data was employed Fisher exact, or Chi-square test. The difference of continuous data was employed student T test or Mann–Whitney U-test. Repeated measures analysis of variant (Repeated ANOVA) was employed for comparing the differences in baseline visual acuity and each visit of 1, 4, and 12 weeks-visit. Factors predictive of an initial poor VA were evaluated using logistic regression analysis. Statistical significance was considered when p-value<0.05.
Results
Clinical Characteristics of Patients with NAION
One hundred eighty-nine patients with NAION (189 eyes) were enrolled in our study (Figure 1). One hundred and five patients were excluded due to not fulfilling our inclusion criteria as follows: Twenty-one had a follow-up time less than 3 months; 26 had other optic neuropathy diseases; eighteen had a duration of onset greater than 30 days; 40 had no data of serum lipid profile after diagnosis. In case of sequential, concurrent or recurrence NAION, only the first affected eye was included in our analysis. None were presented with sequential, concurrent or recurrent NAION in the present study.
 |
Figure 1 STROBE study participant’s flow chart. Note: Improvement defined as improved 0.2 logMAR in BCVA from an initial visit to the 12-weeks period. |
Baseline Characteristics Between the Two Groups of Initial VA of 20/200
A total of 84 patients with NAION (84 eyes) were recruited in the present study. At Table 1, their mean age of the group of initial VA worse than 20/200 was 58.3±7.6 years with significantly older than that of the better VA group (p = 0.042). In both groups, the majority of participants were male. Notably, proportion of DLP as well as higher level of TC, TG, and LDL were significantly observed in the group with worse initial VA (all p<0.05 respectively). A comparable difference was seen between the two groups with respect to gender, presence of disc at risk, and systolic and diastolic blood pressure.
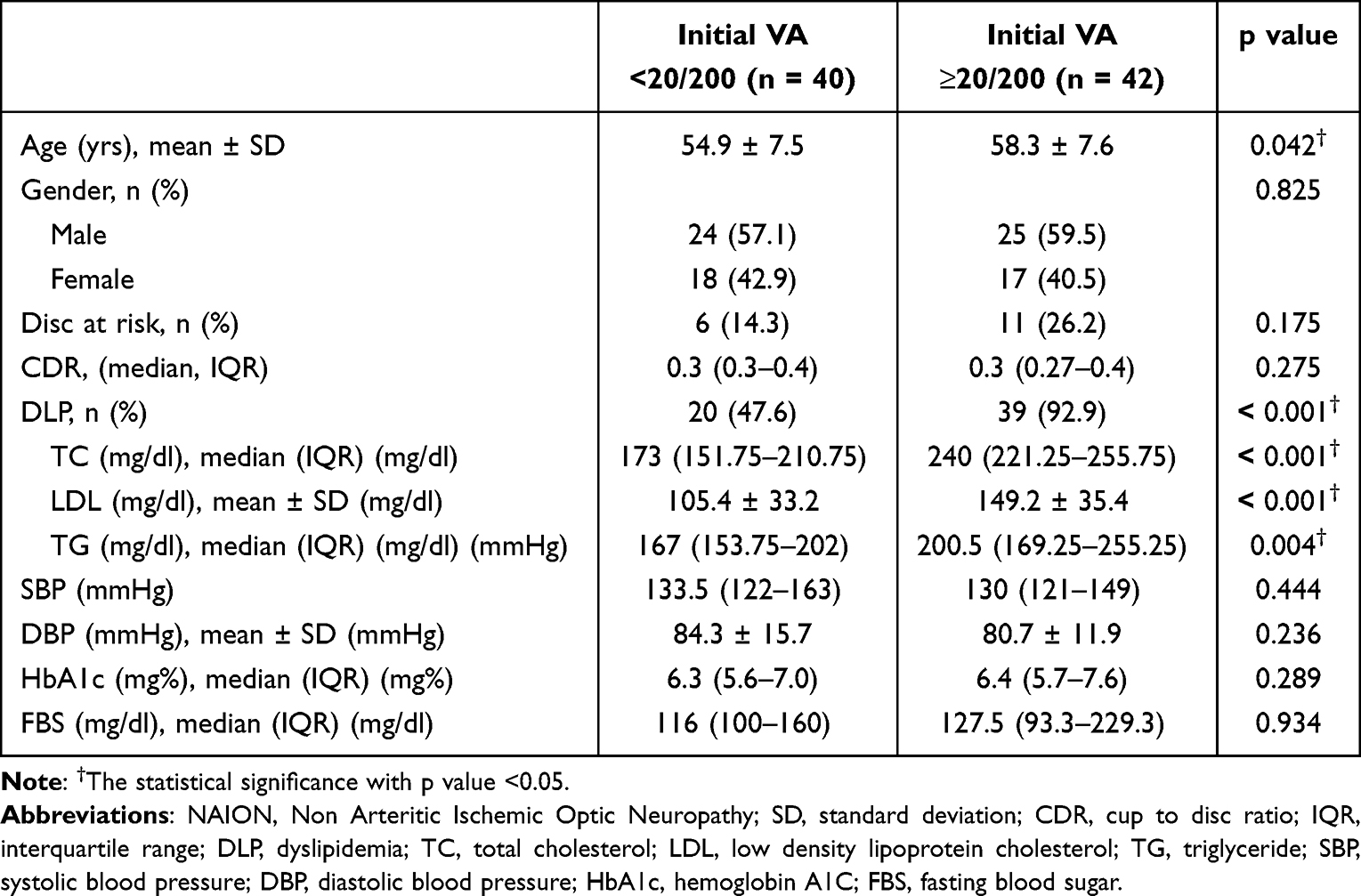 |
Table 1 Baseline Characteristics of NAION Patients of the Two Groups of Initial VA of 20/200 |
Baseline Characteristics Between the Two Groups of VA Improvement of 0.2 logMAR
Table 2 depicted baseline characteristics between the two groups of VA improvement of 0.2 logMAR at 12 weeks. No significant differences regarding of baseline demographic, characteristics or serum lipid parameters between the two groups were seen.
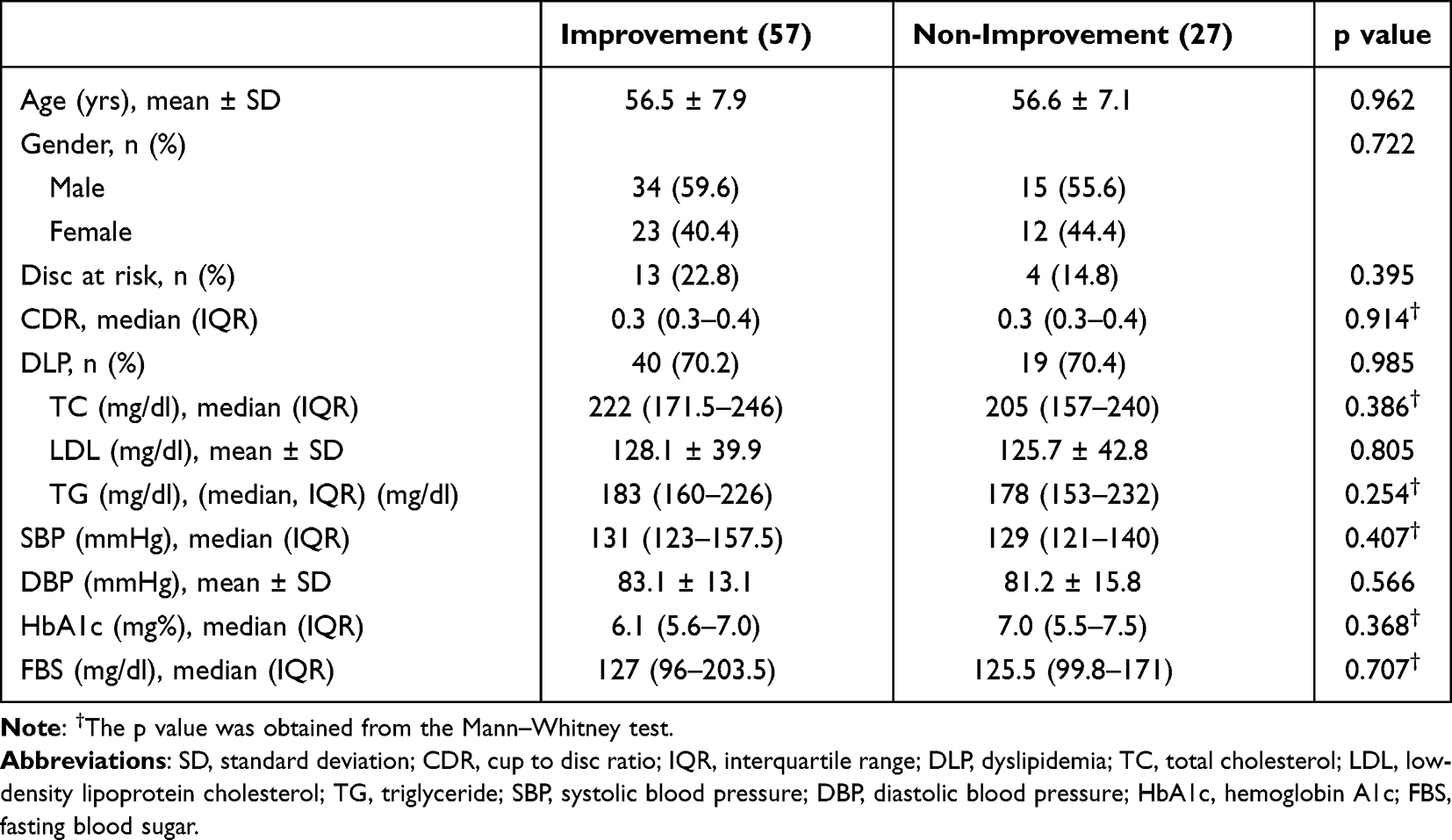 |
Table 2 Baseline Characteristics Based on the Two Groups of VA Improvement |
Determinates on Initial Visual Acuity
Table 3 depicted predictors of poor initial VA. In the multivariable model, higher age with an Odds ratio (OR) =1.118, (p = 0.014), and TC (OR: 1.034, p = 0.016) independently associated with worse initial VA. TG was significant only in the univariable analysis (p = 0.010).
 |
Table 3 Risk Factors for Initial Poor Visual Acuity |
Long Term Visual Outcomes Between the Two Groups of Initial VA of 20/200
Supplementary Table 1 and Figure 2 illustrated the changes in VA over the 12-weeks period for both groups. Those with good initial VA had a mean BCVA of 0.57±0.2 logMAR, improving to 0.49±0.44 logMAR at 12 weeks. While, the group with poor initial VA had a mean BCVA of 1.8±0.79 logMAR, which slightly worsened to 1.86±0.93 logMAR at 12 weeks. A statistically significant difference in mean BCVA between the two groups was observed throughout the 12-weeks follow-up period (p<0.001).
 |
Figure 2 Changes in visual acuity of the two groups of an initial VA 20/200 during the follow-up period. |
Long Term Visual Outcomes Between the Two Groups of VA Improvement of 0.2 logMAR
Supplementary Table 2 and Figure 3 illustrated the trend of VA change between the groups with and without a 0.2 logMAR improvement. Overall, at the 12-weeks period, a statistically significant difference in mean BCVA was observed between the groups (p = 0.017).
 |
Figure 3 Changes in visual acuity of the two groups of improvement during the follow-up period. |
Figure 4 demonstrated the overall probability of VA improvement based on serum lipid parameters. The probability of VA improvement 0.2 logMAR initially decreased slightly, stabilized, and then inclined sharply beyond 300 mg/dL, with greater uncertainty observed at extreme levels of TC. Similarly, an inverse relationship was noted between TG levels and predicted visual outcomes. LDL demonstrated a gradual increase in probability of visual acuity improvement was observed over the three months period, especially exceedingly closely 400 mg/dL. However, wider 95% confidence intervals (CI) at higher lipid levels suggest increased variability in the estimates, indicating greater uncertainty in prediction visual improvement based on those three lipid parameters.
 |
Figure 4 Probability of VA improvement based on serum lipid parameters during the follow-up period. Notes: Y axis in each figure (A–F) represents the linear prediction of probability of VA improvement at least 0.2 logMAR from an initial to the 12-weeks period; good initial VA, initial BCVA greater than VA of 20/200, poor initial VA, initial BCVA worse than or equal VA of 20/200. (A) Trend of VA improvement based on total cholesterol. (B) Trend of VA improvement based on triglyceride. (C) Trend of VA improvement based on low-density lipoprotein cholesterol. Comparison of VA improvement between the two groups of initial VA of 20/200. (D) Trend of BCVA change between the two groups based on total cholesterol. (E) Trend of BCVA change between the two groups based on triglyceride. (F) Trend of BCVA change between the two groups based on low-density lipoprotein cholesterol. Error bars represent 95% confidence intervals. |
Discussion
This study demonstrated that while DLP and elevated lipid profiles were significantly associated with worse initial visual status in patients with N AION, they do not appear to influence long-term visual recovery.
While pathophysiology of the disease is poorly understood, mostly believed due to hypo-perfusion of short posterior ciliary artery.6 DLP has influenced systemic vascular diseases by lowering anti-oxidant process, enhancing calcification or vascular endothelial dysfunction from high level of TC, |TG, LDL or low HDL level resulting in a decrease of vascular blood supply at optic nerve.9
Although DLP is a well-accepted risk factor of NAION development in several studies.7,8 The association of DLP and visual prognosis, or recovery has differed among studies. In western populations, Hayreh et al and The Ischemic Optic Neuropathy Decompression Trial group (The IONDT study) found no associations between DLP and either short-term or long-term VA.3,10 While some previous researchers reported their association. Dattilo et al revealed that several systemic vascular risk factors including DLP were seen in those presenting with poor VA of HM.15 Similarly, Eagling et al also reported a trend of attaining VA of 20/40 or better than in those without systemic vascular risks.16 Serum lipid parameters have been investigated in various eye diseases including retinal vein occlusion, diabetes retinopathy, and NAION.17,18 On the other hand, a ratio of TC/HDL and LDL/HDL had no benefit in predicting diabetic retinopathy development after adjustment all covariate factors in a study of Zhang et al.19 In a primate model, the worse ischemic process notably correlated with a poor visual status.20 A potential influence of non-perfusion area of blood flow at optic disc, capillary density and visual outcomes has been investigated in several recent studies.21,22 In western population, Koçak et al also reported that a high ratio of TC/HDL-c, LDL-c/HDL-c, and non-HDL-c/HDL were notably observed in the group of VA worse than 20/200 and higher probability of sequential NAION occurrence.13 Unfortunately, none of our NAION cases had concurrence or recurrence or sequential NAION, leading to no ability of evaluations of the association. A further study with large numbers of sequential NAION patients should be conducted for answering the hypothesis.
In the current study, we found a statistically significant association between poor presenting VA and high levels of TC, TG, and LDL. The findings may be explained as follows: first, lipid dysregulation or elevated cholesterol levels may lead to vascular constriction or narrowing, contributing to the development of non-perfused areas in the optic nerve. Second, it has been hypothesized that atherosclerosis may impair the vascularization of small blood vessels around the optic nerve, including the anastomoses of pial blood vessels, which could otherwise help preserve or protect against ischemic processes. Although serum lipid levels measured post-NAION diagnosis may not fully capture the 12-weeks visual status or prognosis in this study, it is notable that estimates of lipid parameters, particularly at higher or extreme values, demonstrated wider confidence intervals. This increased variability implies a degree of uncertainty regarding their prognostic significance for long-term visual outcomes. Consequently, these findings should be interpreted with caution when considering their potential role in predicting visual prognosis. Moreover, serum lipid levels were not consistently assessed at every follow-up visit, which limits the ability to draw definitive conclusions regarding the correlation between lipid levels and VA in each visit. A prospective study with regular lipid level assessments and visual status evaluations at each follow-up time would provide more robust insights into their potential association, enhancing our understanding of this relationship.
Aging has influenced optic nerve diseases in several aspects. First, there is a high neuroplasticity in young age compared to elderly leading to the preservation of retinal ganglion cells loss (RGC loss) or nerve axons after the optic neuropathy development.23 Second, the influences of microcirculation blood flow of retinal or optic nerve head and aging have differed in each study. Although Groh et al proposed that there was no significant correlation of optic nerve blood flow to patient age.24 Kobayashi et al proposed a notably lower blood flow at retinal or optic nerve in the older compared to the young age group.25 Similarly, Liu et al revealed that there is a stiffness or decreased ocular blood flow in the elderly Japanese populations.26 Third, age-related structural or mechanical change of optic nerve which might compensate RGC loss or enhance neurodegeneration.23
In our present study, while old age was notably observed in the poor initial VA of worse than 20/200. There was no influence on long-term visual recovery. The impact of patient age on visual outcome remains inconclusive in prior studies.3,11 Probably, due to systemic vascular diseases or ophthalmic factors; for example, a higher prevalence of multiple vascular diseases in the old age15 or a better initial VA in the young age.27 We found no correlation with age and the visual change at 12 weeks compared to the initial presentation. Initially, older age presented with worse VA. While, there was no association of this determinant at the 12-weeks period. Indeed, the natural disease of NAION has not been well understood yet. Although visual recovery was seen in approximately 40% of the western populations.3 It seems to be difficult for comparing our visual prognosis with other studies. Since we particularly aim at evaluating the association of lipid parameters on the visual prognosis, not for studying in all NAION cases.
Some limitations of our research should be addressed. First, A retrospective design posed inherent limitations, including sample size, potential incomplete or inconsistent data collection for example we could not evaluate the associations between serum lipid parameters and outcomes of visual field/ retinal thickness parameters or the impact of serum lipid profiles on visual status at each follow-up visit could not be assessed in this study and a reliance on smaller sample sizes, which may limit the generalizability of findings. Second, there is a potential for selection bias towards more severe cases, given the nature of the study being conducted at a referral hospital. Third, Although the therapeutic effect on visual outcomes in NAION cannot be entirely ruled out, there is currently no consensus on the proven efficacy of any specific therapies. In this study, the included NAION cases received supportive care, primarily focused on managing systemic vascular conditions, without any specific targeted treatments for NAION. With a follow up time of 12 weeks, that is enough to be a representative of a stability of visual change based on the previous literature.28 While, we believed that a trend of visual stabilization between an initial and the 12-weeks period has been investigated in the present study may provide an informative visual prognosis or its natural history in this specific population, Long-term follow-up studies are warranted to provide more comprehensive insights into the management and outcomes of NAION. Although lipid-lowering therapies, such as statins, have shown efficacy in reducing cardiovascular and cerebrovascular risks, their effect on NAION outcomes remains unclear. Future research should investigate whether DLP management influences the clinical course of NAION, particularly in preventing recurrence or mitigating initial visual loss.
To our knowledge, this is the first study in Southeast Asia population evaluating the association of initial visual status and long-term recovery among serum levels of TC, TG, and LDL.
Conclusions
While older age and elevated lipid levels, specifically TC, TGs, and LDL, were correlated with poorer initial visual acuity in NAION patients, no significant associations were identified between lipid parameters and long-term visual recovery. Early detection for individuals with DLP and advanced age merit attention.
Compliance with Ethical Standards
All participants gave written informed consent before the data collection process began.
Funding
No funding was received for this research.
Disclosure
None of the authors have any conflict of interest to disclose.
References
1. Hattenhauer MG, Leavitt JA, Hodge DO, Grill R, Gray DT. Incidence of nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol. 1997;123(1):103–107. doi:10.1016/s0002-9394(14)70999-7
2. Johnson LN, Arnold AC. Incidence of nonarteritic and arteritic anterior ischemic optic neuropathy. Population-based study in the state of Missouri and Los Angeles County, California. J Neuroophthalmol. 1994;14(1):38–44.
3. Hayreh SS, Zimmerman MB. Nonarteritic anterior ischemic optic neuropathy: natural history of visual outcome. Ophthalmology. 2008;115(2):298–305.e2. doi:10.1016/j.ophtha.2007.05.027
4. Borchert M, Lessell S. Progressive and recurrent nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol. 1988;106(4):443–449. doi:10.1016/0002-9394(88)90881-1
5. Katz DM, Trobe JD. Is there treatment for nonarteritic anterior ischemic optic neuropathy. Curr Opin Ophthalmol. 2015;26(6):458–463. doi:10.1097/icu.0000000000000199
6. Arnold AC, Hepler RS. Natural history of nonarteritic anterior ischemic optic neuropathy. J Neuroophthalmol. 1994;14(2):66–69.
7. Liu B, Yu Y, Liu W, Deng T, Xiang D. Risk factors for non-arteritic anterior ischemic optic neuropathy: a large scale meta-analysis. Front Med. 2021;8:618353. doi:10.3389/fmed.2021.618353
8. Kim DH, Shin GR, Choi YJ. Risk factors for non-arteritic anterior ischaemic optic neuropathy in a Korean population. Neuro-Ophthalmology. 2017;41(2):68–75. doi:10.1080/01658107.2016.1267771
9. Di Angelantonio E, Sarwar N, Perry P, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302(18):1993–2000. doi:10.1001/jama.2009.1619
10. Dickersin K, Everett D, Feldon S, et al. Optic nerve decompression surgery for nonarteritic anterior ischemic optic neuropathy (NAION) is not effective and may be harmful. JAMA. 1995;273(8):625–632.
11. Sharma S, Kwan S, Fallano KA, Wang J, Miller NR, Subramanian PS. Comparison of visual outcomes of nonarteritic anterior ischemic optic neuropathy in patients with and without diabetes mellitus. Ophthalmology. 2017;124(4):450–455. doi:10.1016/j.ophtha.2016.11.029
12. Patil A, Mahesh KV, Prabhat N, et al. Non-arteritic anterior ischaemic optic neuropathy - myths and misconceptions: experience from a Tertiary Care Centre in North India. Neuro-Ophthalmology. 2020;44(4):246–254. doi:10.1080/01658107.2019.1688356
13. Koçak N, Yeter V, Turunç M, Bayrambaş M, Eraydın B, Güngör İ. Atherogenic indices in non-arteritic ischemic optic neuropathy. Int J Ophthalmol. 2021;14(7):1041–1046. doi:10.18240/ijo.2021.07.12
14. Johnson LN, Guy ME, Krohel GB, Madsen RW. Levodopa may improve vision loss in recent-onset, nonarteritic anterior ischemic optic neuropathy. Ophthalmology. 2000;107(3):521–526. doi:10.1016/s0161-6420(99)00133-5
15. Dattilo M, Tian T, Peragallo JH, Newman NJ, Biousse V. Very poor visual acuity in non-arteritic anterior ischaemic optic neuropathy. Neuro-Ophthalmology. 2021;45(1):23–28. doi:10.1080/01658107.2020.1785509
16. Eagling EM, Sanders MD, Miller SJ. Ischaemic papillopathy. Clinical and fluorescein aniographic review of forty cases. Br J Ophthalmol. 1974;58(12):990–1008. doi:10.1136/bjo.58.12.990
17. Kohli D, Wu KY, White LJ, Hodge DO, Chen JJ, Roddy GW. Metabolic syndrome and its components are associated with non-arteritic anterior ischaemic optic neuropathy. BMJ Open Ophthalmol. 2022;7(1). doi:10.1136/bmjophth-2022-001111
18. O’Mahoney PR, Wong DT, Ray JG. Retinal vein occlusion and traditional risk factors for atherosclerosis. Arch Ophthalmol. 2008;126(5):692–699. doi:10.1001/archopht.126.5.692
19. Zhang J, Liu C, Peng Y, et al. Impact of baseline and trajectory of the atherogenic index of plasma on incident diabetic kidney disease and retinopathy in participants with type 2 diabetes: a longitudinal cohort study. Lipids Health Dis. 2024;23(1):11. doi:10.1186/s12944-024-02003-5
20. Johnson MA, Miller NR, Nolan T, Bernstein SL. Peripapillary retinal nerve fiber layer swelling predicts peripapillary atrophy in a primate model of nonarteritic anterior ischemic optic neuropathy. Invest Ophthalmol Vis Sci. 2016;57(2):527–532. doi:10.1167/iovs.15-17880
21. Gaier ED, Wang M, Gilbert AL, Rizzo JF, Cestari DM, Miller JB. Quantitative analysis of optical coherence tomographic angiography (OCT-A) in patients with non-arteritic anterior ischemic optic neuropathy (NAION) corresponds to visual function. PLoS One. 2018;13(6):e0199793. doi:10.1371/journal.pone.0199793
22. Ling JW, Yin X, Lu QY, Chen YY, Lu PR. Optical coherence tomography angiography of optic disc perfusion in non-arteritic anterior ischemic optic neuropathy. Int J Ophthalmol. 2017;10(9):1402–1406. doi:10.18240/ijo.2017.09.12
23. Coleman-Belin J, Harris A, Chen B, et al. Aging effects on optic nerve neurodegeneration. Int J Mol Sci. 2023;24(3). doi:10.3390/ijms24032573
24. Groh MJ, Michelson G, Langhans MJ, Harazny J. Influence of age on retinal and optic nerve head blood circulation. Ophthalmology. 1996;103(3):529–534. doi:10.1016/s0161-6420(96)30662-3
25. Kobayashi T, Shiba T, Kinoshita A, Matsumoto T, Hori Y. The influences of gender and aging on optic nerve head microcirculation in healthy adults. Sci Rep. 2019;9(1):15636. doi:10.1038/s41598-019-52145-1
26. Liu C, Kobayashi T, Shiba T, Hayashi N. Effects of aging and exercise habits on blood flow profile of the ocular circulation. PLoS One. 2022;17(4):e0266684. doi:10.1371/journal.pone.0266684
27. Behbehani R, Ali A, Al-Moosa A. Risk factors and visual outcome of Non-Arteritic Ischemic Optic Neuropathy (NAION): experience of a tertiary center in Kuwait. PLoS One. 2021;16(2):e0247126. doi:10.1371/journal.pone.0247126
28. Dotan G, Goldstein M, Kesler A, Skarf B. Long-term retinal nerve fiber layer changes following nonarteritic anterior ischemic optic neuropathy. Clin Ophthalmol. 2013;7:735–740. doi:10.2147/opth.S4252
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.