")
Back to Journals » Nature and Science of Sleep » Volume 17
Impact of Preoperative Daytime Sleepiness and Insomnia on Therapy Adherence and Neurostimulation Amplitude in Unilateral Hypoglossal Nerve Stimulation
Authors Pordzik J, Ludwig K , Ruckes C, Gouveris H
Received 7 September 2024
Accepted for publication 16 January 2025
Published 7 February 2025 Volume 2025:17 Pages 251—259
DOI https://doi.org/10.2147/NSS.S495106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Johannes Pordzik,1,* Katharina Ludwig,1,* Christian Ruckes,2 Haralampos Gouveris1
1Department of Otolaryngology/Head and Neck Surgery & Sleep Medicine Center, University Medical Center Mainz, Mainz, 55131, Germany; 2Interdisciplinary Center for Clinical Trials, University Medical Center Mainz, Mainz, 55131, Germany
*These authors contributed equally to this work
Correspondence: Haralampos Gouveris, Email [email protected]
Introduction: Average adherence to hypoglossal nerve stimulation (HGNS) therapy is more than 5 h/night. Reported data on HGNS therapy adherence is often based on studies that performed in-lab titration of the neurostimulation parameters and may therefore not represent real-world therapy outcomes. Adherence to HGNS therapy is a major determinant of success of this kind of therapy. Factors with the potential to influence adherence to HGNS therapy should be further elucidated. The aims of this study were to investigate 1) details regarding therapy adherence under HGNS therapy and 2) the possible association between age, insomnia, daytime sleepiness, polysomnography (PSG)-based metrics, neurostimulation parameters and HGNS-therapy adherence.
Methods: Forty-three consecutive patients with detailed information about therapy adherence time were included. About 225 ± 191 days after implantation, a PSG without any in-lab titration was performed. Adherence was assessed by interrogating the impulse generator’s data at that time. Patient-reported insomnia was assessed using the insomnia severity index (ISI) and the Epworth Sleepiness scale (ESS) was used to assess daytime sleepiness before and after HGNS treatment.
Results: An increased adherence in a real-world setting with 48.72 ± 14.74 hours per week (6.96 hours per night) was found. A strong negative correlation between preoperative ESS score and adherence time (r = - 0.43; p< 0.005) was found. Neither pre-operative insomnia nor sleepiness had any impact on neurostimulation amplitude. A positive association between preoperative age and therapeutic amplitude levels could be shown.
Discussion: In this cohort, average adherence was much higher than previously reported. We provide evidence that pre-operative excessive daytime sleepiness may seriously impair adherence to HGNS therapy.
Keywords: obstructive sleep apnea, hypoglossal nerve stimulation, adherence, sleepiness, insomnia, positive airway pressure therapy
Introduction
Hypoglossal nerve stimulation (HGNS) is a second-line therapy for patients not tolerating positive airway pressure therapy (PAP). Previously high success rates for polysomnography (PSG)-based respiratory parameters could be shown in most published reports. However, the reports with the highest improvement rates in PSG-based parameters performed titration of the neuro-stimulation parameters during the overnight in-lab post-operative PSG.1–6 Only few studies represent the real-world outcome after implantation of an inspiration coupled unilateral HGNS.7,8 Therapy adherence is reported to be more than 5 h per night on average.6,9–11 However, only one of these studies aimed to investigate the association between insomnia-related symptoms and therapy adherence.6 Insomnia may be associated with lower PAP therapy adherence.12 Comorbid insomnia and sleep apnea (COMISA) may affect between 30% and 50% of patients presenting with OSA-related complaints and is more difficult to treat than insomnia alone or OSA alone13 In this respect, it is necessary to specifically target distinct combinations of both insomnia (initial, middle, late) and OSA (mild, moderate, severe) phenotypes using both cognitive behavioural therapy for insomnia (CBTi) and PAP-therapy.14 Obstructive sleep apnea is associated with excessive daytime sleepiness (EDS). Although EDS in OSA may be captured using multimodal signal analysis of the specific electroencephalographic patterns of these patients,15 it is routinely assessed clinically by means of the patient-reported Epworth sleepiness scale.16 More specifically, in PAP-intolerant patients with OSA that have been eventually treated with HGNS, insomnia severity (as depicted by the insomnia severity index, ISI)17 correlated very strongly with EES both preoperatively and postoperatively.18 Therefore, there is evidence that in this specific subgroup of patients with OSA insomnia features may play a significant role in the mechanisms promoting EDS.
Non-adherence or intolerance to PAP therapy is a major indication for evaluating HGNS treatment. Therefore, patients undergoing HGNS therapy may suffer preoperatively more insomnia than patients tolerant to PAP-therapy, which may also potentially lead to lower HGNS therapy adherence.
One study that aimed to investigate the impact of insomnia on the HGNS therapy adherence6 showed that 62% of the patients included an insomnia severity-index (ISI) score of ≥15 (moderate/severe insomnia). However, in this study, no significant difference in HGNS therapy adherence between the subgroup of patients with an ISI score <15 points and ≥15 could be observed. Previously, it could be shown that insomnia was associated with a lower reduction in AHI in the short-term follow-up.18
Two further studies investigated the impact of insomnia of adherence to HGNS therapy. One study proved that in patients with COMISA, compared to patients with OSA, a reduced device usage (4.9 vs 5.8 h/night) and higher frequent pauses in therapy (1.4 vs 0.4 pauses/night).19 The other study showed no statistically significant difference concerning device usage in patients with insomnia.20
Additionally, to the best of our knowledge, there are no studies investigating the impact of insomnia, daytime sleepiness and age on the HGNS neurostimulation parameters.
The aim of this study was 1) to gather data on therapy adherence under HGNS therapy on our cohort of patients, 2) to investigate the association between age, patient-reported insomnia and daytime sleepiness and HGNS-therapy adherence and 3) to investigate the association between age, patient-reported insomnia and daytime sleepiness and neurostimulation parameters.
Methods
Data from a cohort of forty three consecutive patients, treated between January 1st 2020 and December 31st 2023, in whom the complete information on adherence (use) time was available, were evaluated retrospectively. All patients met the indication criteria for implantation of an inspiration-coupled unilateral HGNS system (Inspire Medical Systems Inc., Golden Valley, MN).21 More specifically, inclusion/indication criteria for HGNS implantation were an intolerance to PAP therapy, an apnea/hypopnea index (AHI) >15 respiratory events (ie, apneas and hypopneas) per hour sleep with less than 25% central apneas, as recorded on full-night diagnostic polysomnography (PSG), a body mass index (BMI) <35 kg/m2. Exclusion criteria for HGNS implantation were a complete concentric collapse at the velar level during drug-induced sleep endoscopy (DISE) a chronic neurodegenerative condition, pregnancy or planned pregnancy, presence of severe psychiatric disease and a recent (<6 months) myocardial infarction.
Before implantation, PSG was performed and scored in all patients according to the American Academy of Sleep Medicine (AASM, 2012) standard guidelines.22 Also, a drug-induced sleep endoscopy (DISE) using propofol was done. Eventually, 225 ± 191 days after implantation a PSG without any in-lab titration was performed in a board – accredited sleep lab. No titration PSG study was performed at all in this patient cohort. Furthermore, data on the adherence time and stimulation amplitude were assessed at this time. The adherence data is automatically read from the system as soon as the medical programming device (physician programmer) connects to the patient’s impulse generator via a wireless connection. Adherence is indicated by the system as usage time in hours per week. This is calculated from the time of connection between the physician programmer and the patient’s impulse generator. The data was collected in the morning after the PSG.
The following PSG-based metrics were evaluated: AHI, apnea index (AI), hypopnea index (HI), cumulative time of apnea and hypopnea during sleep, snoring index, oxygen desaturation index (ODI), mean oxygen desaturation, percentage of sleep time with blood oxygen desaturation lower than 90% (t90) and number of arousal events per hour (arousal index).
Insomnia-related symptoms were assessed pre- and post-operatively using the ISI score.23 The ISI is a validated questionnaire containing seven items covering different aspects of insomnia. Each item is scored with a range of 0 points (= no problems at all) to 4 points (= very severe problems with this issue). This results in a total score ranging between 0 and 28 points. Zero to 7 points is defined as no clinically significant insomnia, 8–14 points as sub-threshold clinical insomnia, 15–21 as moderately severe insomnia and 22–28 as severe clinical insomnia. Epworth Sleepiness Scale (ESS) was used pre- and post-operatively to detect daytime sleepiness.24 The ESS is a questionnaire containing 8 items on a 4-point Likert scale (0 = no sleepiness at all, 1, 2, 3 = very increased likelihood of falling asleep) resulting a total score between 0 and 24. Higher self-reported ESS score values represent more pronounced daytime sleepiness.
Statistical Analysis
SPSS (IBM, Armonk, NY, USA) software was used for statistical analysis. All parameters were presented as mean ± standard deviation. Within-group comparisons were done by using Wilcoxon’s signed rank test. Spearman’s correlation coefficients were calculated. Multivariate regression model was performed for therapy adherence as dependent variable and therapeutic amplitude as dependent variable including ESS, ISI, age, BMI and AHI as independent variables. Results with p<0.05 were regarded as statistically significant. In the study by Kaffenberger et al,19 a standard deviation of 2.8 h/night for the adherence to HGNS usage was found. Based on these findings, our present study had a power of 80% to detect a difference in adherence to the use of HGNS of 1.23 h/night with a two-sided significance level 5% by using a one-sample t-test.
Ethical Statement
In this study, only health data that is collected in the clinical routine was analyzed retrospectively. So-called “third parties” did not have access to the data and publication occurs exclusively in anonymized form. The Ethics Committee of the local Medical Association (Central Ethics Committee of the Medical Association of Rhineland-Palatinate) clearly states, that patient informed consent can be waived in this kind of studies and furthermore refrains from providing advice in such cases, citing the State Hospital Act (§36 and §37). All study procedures comply with the Declaration of Helsinki for studies in humans.
Results
The study cohort included data from 10 females and 33 males (23.3% and 76.7% of the cohort, respectively).
A significant reduction of AHI, apnea index, hypopnea index, cumulative time under apnea or hypopnea, snoring index, oxygen desaturation index, ISI-score and ESS-score has been observed in this patient cohort after HGNS therapy. A reduction in the arousal index and t90 (% time with peripheral blood oxygen saturation <90%) after HGNS therapy was observed, although it did not reach statistical significance at the 0.05-level. In parallel, a statistically non-significant at the 0.05-level increase in mean peripheral blood oxygen saturation has been found (Table 1). We also calculated the post hoc power for the AHI metric from our data. The post-hoc power for the AHI amounts to 99.5%.
 |
Table 1 Age, BMI (Body Mass Index), Stimulation Amplitude, ESS Score, ISI Score and PSG Related Pre- and Postoperative Values of HGNS Patients |
Pre- and postoperative PSG-related results are presented in Table 1.
Quite a high adherence time in a real-world setting with 48.72 ± 14.74 hours per week, corresponding to 6.96 hours of device usage per night has been found in this patient cohort.
Less sleepy patients of this cohort (ESS score ≤10; N=17) had a mean adherence time of 55.06 h/week (range: 31–70 h/week). Patients who reported on significant sleepiness (ESS > 10) showed a mean adherence time of 44.58 h/week (range: 10–62 h/week).
Significant correlations were observed between preoperative ESS score and adherence time (r = - 0.43; p<0.005) and between preoperative ISI score and preoperative ESS core (r=0.53; p<0.001) (Table 2). No significant correlations were observed between preoperative ISI, adherence time, stimulation amplitude and ∆ AHI, ∆ ODI, ∆ t90 (Table 2).
 |
Table 2 Correlation Between Adherence Time (h/Week); Stimulation Amplitude (V); Age (Years) and Preoperative Epworth Sleepiness Scale (ESS), Insomnia Severity Index (ISI), Numerical Difference in Apnea-Hypopnea Index (∆AHI), Numerical Difference in Oxygen Desaturation Index (∆ODI) and Numerical Difference in t90 Index (∆t90) |
The multivariate regression model revealed a significant regression coefficient for preoperative ESS and therapy adherence (r=−1.14; p=0.04) and for age and therapeutic amplitude (r=0.03; p=0.02) (** if p < 0.01)(Table 3, Figures 1 and 2).
 |
Table 3 Multivariate Regression Model With Therapy Adherence and Stimulation Amplitude as Dependent Variables and Pre-Operative ISI, ESS, BMI and AHI as Independent Variables |
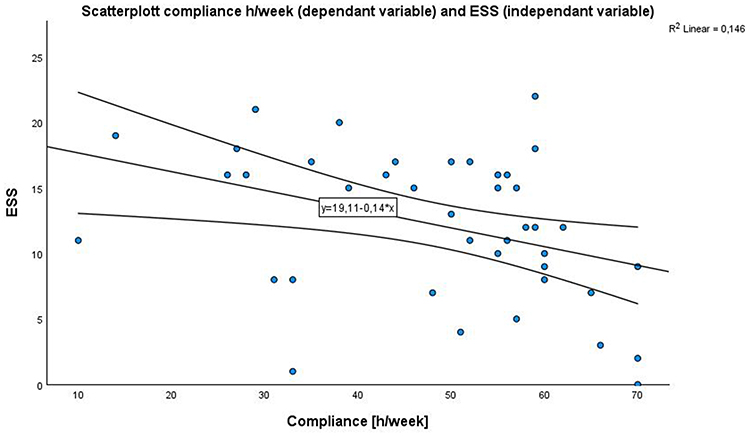 |
Figure 1 Scatterplot between adherence h/week (dependent variable) and ESS (independent variable). The respective regression line with confidence intervals is also depicted. |
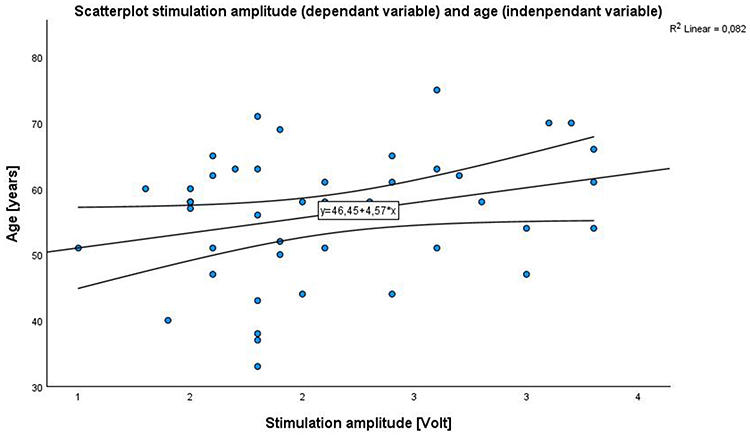 |
Figure 2 Scatterplot between stimulation amplitude (dependent variable) and age (independent variable). The respective regression line with confidence intervals is also depicted. |
Discussion
In this study, we provide evidence for a quite high adherence time in a real-world setting. A strong negative association between daytime sleepiness and adherence time could be shown. Also, a strong positive association between preoperative age and therapeutic amplitude levels could be shown.
With 6.96 hours per night, adherence in our cohort was much higher (>1 hour more per night) than previously reported.6,9–11 This increased adherence in our study representing real-world data without in-lab titration of stimulation parameter is surprising. One possible explanation is the close connection and engagement between the patients and our implantation centre. There is a regular phone or Email contact with the patients during the first four weeks after device activation and hence patients are advised on any uncertainties that arise with the neurostimulation at its early stages.
First-line therapy for OSA is a positive airway pressure (PAP) therapy. However, we know that adherence to PAP therapy is challenging. One review including 80 studies proved an overall night use of 4.7 hours with a non-adherence rate of 34.1% for PAP therapy.25 This means that HGNS therapy was used 48% more compared to the patients using PAP-therapy in the aforementioned review. It should be highlighted that only patients who (almost) do not use PAP therapy, which means whose adherence to PAP therapy was almost close to zero hours per night, are eligible for HGNS. This makes the high usage time of HGNS therapy within the same cohort even more remarkable. The higher adherence during HGNS therapy in our cohort may provide a valid explanation for the excellent improvement concerning patient-reported outcomes such as insomnia-related symptoms and daytime sleepiness after HGNS therapy. A continuously performed therapy may have a greater impact on patient-reported outcomes even if the improvement in respiratory PSG-based metrics is higher in PAP therapy compared to HGNS therapy. Previous studies concerning the outcome of PAP therapy showed an AHI reduction between 72% and 87%.26,27 Interestingly, the adherence time did not significantly correlate with ∆ AHI at the time of the performed PSG. However, little use of HGNS therapy over one week may therefore have no influence on AHI reduction if therapy is interrupted during therapy.
We observed a strong negative association between daytime sleepiness and therapy adherence. Despite a significant benefit in daytime sleepiness, usage of HGNS therapy is reduced in highly symptomatic (sleepy) patients. Based on the results of the present study, the indication for HGNS therapy in very sleepy patients not tolerating PAP therapy should be evaluated more carefully in the future, because their excessive sleepiness may negatively impact on therapeutic adherence to HGNS therapy.
It seems surprising that insomnia, including symptoms such as difficulty falling asleep and staying asleep, did not significantly correlate with the adherence time. The impact of insomnia on HGNS therapy outcomes, including objective PSG-based as well as subjective patient-reported outcomes, remains unclear. One study proved insomnia was associated with objective PSG-related outcomes.18 However, most of the published studies showed no significant difference in the PSG-related outcome of patients with comorbid insomnia and OSA (COMISA).28,29 Concerning patient-reported outcomes, one study showed insomnia was associated with worse daytime sleepiness and sleep-related quality of life.30 As previously stated, there are two studies investigating the impact of insomnia on adherence to HGNS therapy. One study showed a reduced device usage and more frequent pauses in therapy in patients with COMISA compared to patients with OSA without insomnia.19 The other study showed no statistically significant difference concerning device usage in patients with insomnia compared to those without insomnia.20
Age was positively associated with stimulation amplitudes. This is not surprising, since with increasing age the nerve excitability and hence the neural response may be reduced.31 Therefore, higher stimulation amplitude may be necessary and higher stimulation amplitude may be accepted. It is well known that stimulation parameters such as voltage amplitude,32 pulse width and frequency,33 electrode configuration affecting tongue motion patterns,34,35 and respiratory sensing quality36 influence HGNS therapy outcomes. However, no study has investigated the influence of insomnia-related symptoms on neurostimulation amplitudes.
No significant association was observed between insomnia-related symptoms and stimulation parameters. Therapy adherence to PAP therapy is largely reduced in patients with comorbid insomnia,12 and the effect of insomnia on HGNS therapy outcomes remains unclear so far.18,28,29 There is evidence that difficulty falling asleep is associated with poorer HGNS therapeutic outcomes.37 Additionally, there is evidence for a differential effect of PAP therapy and HGNS on sleepiness and/or insomnia, because a much higher improvement in daytime sleepiness and insomnia was observed after HGNS compared to PAP therapy, despite a significantly less AHI reduction after HGNS therapy.8 Therefore, we hypothesized that patients with insomnia may be affected significantly faster by increased therapy amplitudes. Our experience is that patients under HGNS therapy with concomitant insomnia often need to be monitored over a longer period of time in order to find the optimal therapeutic amplitude by adjusting the stimulation parameters (pulse width, frequency, electrode configuration). In addition, patients with concomitant insomnia must be very confident in the use of the therapy, as they must be able to switch the therapy on and off if they have difficulty falling asleep or sleeping through the night, or the stimulation must be tolerable even when they are awake, which can be difficult, particularly at the start of therapy.
However, our study clearly showed that there is no significant association between insomnia-related symptoms and stimulation amplitude. In this context, it is important to understand that the stimulation amplitude does not automatically refer to the exact energy received by the hypoglossal nerve. The stimulation amplitude is one among other parameters that influences the energy received by the hypoglossal nerve. Further parameters such as pulse width and frequency and electrode configuration affecting tongue motion patterns influence the stimulation amplitude and may influence the tolerance of HGNS therapy.33 Besides these configuration parameters, the electrode position may also affect the exact energy received by the hypoglossal nerve. In addition, individual factors such as the stiffness of the tissue, the position of the hyoid bone, but also the patient’s age and preferred sleeping position play a role in the experience of the stimulation and thus influence the outcome of the therapy.38 How all these factors affect the perception of the individual patient during sleep has been poorly investigated.
In future trials, the use of further insomnia-related questionnaires (eg SCI-Sleep Condition Indicator), that may capture other insomnia-related features than ISI does, could provide further evidence on this specific topic.39
Also, assessment of patient-reported excessive daytime sleepiness using other instruments than the ESS (eg use of the Stanford Sleepiness Scale – SSS) may also decipher further aspects on sleepiness-related issues in these patients.40
Our study has some important limitations. The study was conducted retrospectively. Only 40 of the 43 patients included filled in the ISI questionnaire and 41 of the 43 patients included filled in the ESS questionnaire. Data on adherence may not be easily obtained in the European “Inspire Setting”. There is no cloud or “Inspire Sleep Sync” available, like in the US. The only available data is the mean usage time in hours per week since the previous consultation in our department. It is therefore unclear whether a patient regularly uses the therapy for a similar number of hours per night on average or uses it more in some nights but not at all in other nights. In addition, there has been a large variability (225± 191 days) in the time point of PSG after implantation. This large variability may have added a certain degree of bias in the results. This issue should be considered in future studies, in order to reduce the respective bias.
For future studies, a larger HGNS patient cohort with comorbid clinically confirmed insomnia should be considered, to allow investigating the relationships between insomnia, adherence and treatment success in more detail.
Conclusion
We showed a high therapy adherence to HGNS therapy in a real-world setting. With 6.96 hours per night, the adherence in this cohort was much higher than previously reported. A strong negative correlation between daytime sleepiness and HGNS adherence time was found. Furthermore, preoperatively insomnia severity had a strong positive correlation with excessive daytime sleepiness. Insomnia-related symptoms showed no correlation with neurostimulation amplitude levels, although age did.
Disclosure
Haralampos Gouveris reports funding of his institution (University Medical Center Mainz) for research not related to this manuscript by Inspire Medical Systems, Inc. (Golden Valley, MN, USA). All other authors have no conflicts of interest to declare.
References
1. Heiser C, Maurer JT, Hofauer B, Sommer JU, Seitz A, Steffen A. Outcomes of upper airway stimulation for obstructive sleep apnea in a multicenter German postmarket study. Otolaryngol Head Neck Surg. 2017;156(2):378–384. doi:10.1177/0194599816683378
2. Steffen A, Sommer JU, Hofauer B, Maurer JT, Hasselbacher K, Heiser C. Outcome after one year of upper airway stimulation for obstructive sleep apnea in a multicenter German post-market study. Laryngoscope. 2018;128(2):509–515. doi:10.1002/lary.26688
3. Strollo PJ, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139–149. doi:10.1056/NEJMoa1308659
4. Huntley C, Kaffenberger T, Doghramji K, Soose R, Boon M. Upper airway stimulation for treatment of obstructive sleep apnea: an evaluation and comparison of outcomes at two academic centers. J Clin Sleep Med. 2017;13(9):1075–1079. doi:10.5664/jcsm.6726
5. Boon M, Huntley C, Steffen A, et al. Upper airway stimulation for obstructive sleep apnea: results from the ADHERE registry. Otolaryngol Head Neck Surg. 2018;159(2):379–385. doi:10.1177/0194599818764896
6. Dhanda Patil R, Ishman SL, Chang JL, Thaler E, Suurna MV. Impact of insomnia on hypoglossal nerve stimulation outcomes in the ADHERE registry. Laryngoscope. 2024;134(1):471–479. doi:10.1002/lary.30933
7. Pordzik J, Seifen C, Ludwig K, et al. Short-term outcome of unilateral inspiration-coupled hypoglossal nerve stimulation in patients with obstructive sleep apnea. Int J Environ Res Public Health. 2022;19(24):16443. doi:10.3390/ijerph192416443
8. Pordzik J, Ludwig K, Seifen C, et al. Real-world data on polysomnography- and patient-reported outcomes in hypoglossal nerve stimulation and auto-titrating positive airway pressure therapy for obstructive sleep apnea. Respir Med. 2024;232:107750. doi:10.1016/j.rmed.2024.107750
9. Hofauer B, Steffen A, Knopf A, Hasselbacher K, Heiser C. Patient experience with upper airway stimulation in the treatment of obstructive sleep apnea. Sleep Breathing. 2019;23(1):235–241. doi:10.1007/s11325-018-1689-4
10. Hasselbacher K, Hofauer B, Maurer JT, Heiser C, Steffen A, Sommer JU. Patient-reported outcome: results of the multicenter German post-market study. Eur Arch Otorhinolaryngol. 2018;275(7):1913–1919. doi:10.1007/s00405-018-5017-1
11. Heiser C, Steffen A, Strollo PJ, Giaie-Miniet C, Vanderveken OM, Hofauer B. Hypoglossal nerve stimulation versus positive airway pressure therapy for obstructive sleep apnea. Sleep Breathing. 2023;27(2):693–701. doi:10.1007/s11325-022-02663-6
12. Sweetman A, Lack L, Crawford M, Wallace DM. Comorbid insomnia and sleep apnea: assessment and management approaches. Sleep Med Clin. 2022;17(4):597–617. doi:10.1016/j.jsmc.2022.07.006
13. Sweetman A, Lack L, McEvoy RD, et al. Bi-directional relationships between co-morbid insomnia and sleep apnea (COMISA). Sleep Med Rev. 2021;60:101519. doi:10.1016/j.smrv.2021.101519
14. Bahr K, Camara RJA, Gouveris H, Tuin I. Current treatment of comorbid insomnia and obstructive sleep apnea with CBTI and PAP-therapy: a systematic review. Front Neurol. 2018;9:804. doi:10.3389/fneur.2018.00804
15. Gouveris H, Koirala N, Anwar AR, et al. Reduced cross-frequency coupling and daytime sleepiness in obstructive sleep apnea patients. Biology. 2022;11(5):700. doi:10.3390/biology11050700
16. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
17. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
18. Pordzik J, Ludwig K, Seifen C, et al. Insomnia in patients undergoing hypoglossal nerve stimulation therapy for obstructive sleep apnea. Biology. 2023;12(1):98. doi:10.3390/biology12010098
19. Kaffenberger TM, Chandna M, Kaki P, et al. Reduced usage of upper airway stimulation therapy in patients with comorbid insomnia and obstructive sleep apnea. J Clin Sleep Med. 2023;19(12):1997–2004. doi:10.5664/jcsm.10752
20. Jomha M, Dabboussi T, Parker NP, Manchanda S, Chernyak Y, Stahl SM. Prevalence of insomnia and restless legs syndrome in patients with upper airway stimulation therapy and effects on treatment outcomes. Sleep Med. 2022;98:121–126. doi:10.1016/j.sleep.2022.06.016
21. Steffen A, Heiser C, Galetke W, et al. Die Stimulation des Nervus hypoglossus in der Behandlung der obstruktiven Schlafapnoe–Aktualisiertes Positionspapier der Arbeitsgemeinschaft Schlafmedizin der DGHNO-KHC. Laryngo-Rhino-Otologie. 2021;100(01):15–20 German . doi:10.1055/a-1327-1343
22. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events: deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
23. Gerber M, Lang C, Lemola S, et al. Validation of the German version of the insomnia severity index in adolescents, young adults and adult workers: results from three cross-sectional studies. BMC Psychiatry. 2016;16:174. doi:10.1186/s12888-016-0876-8
24. Bloch KE, Schoch OD, Zhang JN, Russi EW. German version of the Epworth sleepiness scale. Respiration. 1999;66(5):440–447. doi:10.1159/000029408
25. Rotenberg BW, Murariu D, Pang KP. Trends in CPAP adherence over twenty years of data collection: a flattened curve. J Otolaryngol Head Neck Surg. 2016;45(1):43. doi:10.1186/s40463-016-0156-0
26. Senn O, Brack T, Matthews F, Russi EW, Bloch KE. Randomized short-term trial of two autoCPAP devices versus fixed continuous positive airway pressure for the treatment of sleep apnea. Am J Respir Crit Care Med. 2003;168(12):1506–1511. doi:10.1164/rccm.200304-542OC
27. Hussain SF, Love L, Burt H, Fleetham JA. A randomized trial of auto-titrating CPAP and fixed CPAP in the treatment of obstructive sleep apnea–hypopnea. Respir Med. 2004;98(4):330–333. doi:10.1016/j.rmed.2003.11.002
28. Dhanda Patil R, Ishman SL, Chang JL, Thaler E, Suurna MV. Impact of insomnia on hypoglossal nerve stimulation outcomes in the ADHERE registry. Laryngoscope. 2023;134:471–479.
29. Dhanda Patil R, Hong MP, Ishman SL. Hypoglossal nerve stimulation in veterans with comorbid insomnia and sleep apnea. Otolaryngol Head Neck Surg. 2021;164(6):1345–1353. doi:10.1177/0194599820982638
30. Steffen A, Baptista P, Ebner EM, Jeschke S, Konig IR, Bruchhage KL. Insomnia affects patient-reported outcome in sleep apnea treated with hypoglossal nerve stimulation. Laryngoscope Investig Otolaryngol. 2022;7(3):877–884. doi:10.1002/lio2.761
31. Zullo A, Fleckenstein J, Schleip R, Hoppe K, Wearing S, Klingler W. Structural and functional changes in the coupling of fascial tissue, skeletal muscle, and nerves during aging. Front Physiol. 2020;11:592. eCollection 2020. doi:10.3389/fphys.2020.00592
32. Safiruddin F, Vanderveken OM, De Vries N, et al. Effect of upper-airway stimulation for obstructive sleep apnoea on airway dimensions. Eur Respir J. 2015;45(1):129–138. doi:10.1183/09031936.00059414
33. Steffen A, Jeschke S, Soose RJ, Hasselbacher K, Konig IR. Impulse configuration in hypoglossal nerve stimulation in obstructive sleep apnea: the effect of modifying pulse width and frequency. Neuromodulation. 2022;25(8):1312–1316. doi:10.1111/ner.13490
34. Heiser C, Maurer J, Steffen A. Functional outcome of tongue motions with selective hypoglossal nerve stimulation in patients with obstructive sleep apnea. Sleep Breathing. 2016;20:553–560. doi:10.1007/s11325-015-1237-4
35. Steffen A, Kilic A, König IR, Suurna MV, Hofauer B, Heiser C. Tongue motion variability with changes of upper airway stimulation electrode configuration and effects on treatment outcomes. Laryngoscope. 2018;128(8):1970–1976. doi:10.1002/lary.27064
36. Steffen A, Sommer JU, Strohl K, et al. Changes in breath cycle sensing affect outcomes in upper airway stimulation in sleep apnea. Laryngoscope Investig Otolaryngol. 2020;5(2):326. doi:10.1002/lio2.334
37. Pordzik J, Petrowski K, Ludwig K, Seifen C, Matthias C, Gouveris H. Difficulty falling asleep is associated with poorer therapeutic outcomes in unilateral hypoglossal nerve stimulation. Nat Sci Sleep. 2024;16:813–821. doi:10.2147/NSS.S459690
38. Serghani MM, Heiser C, Schwartz AR, Amatoury J. Exploring hypoglossal nerve stimulation therapy for obstructive sleep apnea: a comprehensive review of clinical and physiological upper airway outcomes. Sleep Med Rev. 2024;76:101947. doi:10.1016/j.smrv.2024.101947
39. Espie CA, Kyle SD, Hames P, Gardani M, Fleming L, Cape J. The sleep condition indicator: a clinical screening tool to evaluate insomnia disorder. BMJ Open. 2014;4(3):e004183. doi:10.1136/bmjopen-2013-004183
40. Hoddes E, Zarcone V, Smythe H, Phillips R, Dement WC. Quantification of sleepiness: a new approach. Psychophysiology. 1973;10(4):431–436. doi:10.1111/j.1469-8986.1973.tb00801.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.