")
Back to Journals » Clinical Ophthalmology » Volume 18
Impact of TearCare on Reading Speed in Patients with Dry Eye Disease
Authors Feng Y , Venkateswaran N, Steele A, Rosenberg ED, Gupta PK
Received 15 July 2024
Accepted for publication 1 October 2024
Published 10 October 2024 Volume 2024:18 Pages 2873—2878
DOI https://doi.org/10.2147/OPTH.S469300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yilin Feng,1 Nandini Venkateswaran,1 Amanda Steele,2 Eric D Rosenberg,3 Preeya K Gupta2,4
1Department of Ophthalmology, Massachusetts Eye and Ear, Harvard Medical School, Boston, MA, USA; 2Triangle Eye Consultants, Raleigh, NC, USA; 3Department of Ophthalmology, New York Medical College, Valhalla, NY, USA; 4Department of Ophthalmology, Tulane University, New Orleans, LA, USA
Correspondence: Preeya K Gupta, Email [email protected]
Purpose: To evaluate the impact of TearCare (TC) treatment on clinical, quality of life, and functional visual outcome metrics in patients with dry eye disease (DED) and meibomian gland disease (MGD).
Methods: This is a prospective, single-center clinical trial. Adults with MGD and a DED diagnosis and tear break-up time (TBUT) < 10 seconds were included. All subjects had at least 20/40 vision and no surgery or new treatment for DED within 60 days prior to enrollment. All patients had one baseline visit prior to undergoing TC and one follow-up visit 1 month after TC. At each visit, the meibomian gland secretion score (MGSS), TBUT, and corneal fluorescein staining (KFL) were assessed. DED symptoms were evaluated using the Ocular Surface Disease Index (OSDI) questionnaire, Visual Function Questionnaire 25 (VFQ-25), and the Fatigue Severity Scale. Reading speed was determined through the International Reading Speed Texts (IReST), Minnesota Low Vision Reading Test (MNREAD), and Wilkins Rate of Reading Test (WRRT).
Results: Thirty-two subjects were included. The average age was 55.9 years. Sixteen (52%) participants had a clinically significant improvement in reading speed after treatment with TC, defined as > 10 words per minute increase in their IReST score. Improvement on the IReST and the MNREAD reached statistical significance (p = 0.012 and p = 0.028, respectively). OSDI scores significantly decreased and VFQ-25 scores significantly increased after TC treatment (p < 0.001). All of the clinical exam parameters showed statistically significant improvements after treatment (p < 0.001).
Conclusion: TC is an effective treatment both clinically and with respect to visual function. Patients who had TC exhibited improvements in quality of life and improved reading speed after a single treatment. This treatment should be frequently considered and utilized to reduce the disease burden of DED related to MGD.
Keywords: thermal pulsation, tearcare, meibomian gland dysfunction, dry eye disease, reading speed
Introduction
Dry eye disease (DED) is a chronic condition that causes significant reduction in quality of life.1 In the United States, it is estimated that up to 40 million people suffer from DED, leading to an economic burden of approximately $3.84 billion.2,3 DED can be classified into two major categories: aqueous-deficient and evaporative dry eye, with the latter accounting for up to 86% of patients with DED.4,5 Evaporative dry eye is caused by a disruption of the tear film lipid layer and is primarily driven by meibomian gland dysfunction (MGD).6 The mainstay of treatment is the application of heat to promote softening and secretion of meibum from the meibomian glands. The standard of care for MGD includes warm compresses, eyelid massage, and maintenance of proper eyelid hygiene. However, the effectiveness of self-administered home treatments has been shown to be low due to suboptimal temperature levels reached as well as poor compliance.7–10 As such, office-based treatments such as LipiFlow and Intense Pulsed Light therapy have been introduced as alternative options.
In 2021, TearCare (TC) received clearance from the United States Food and Drug Administration as an in-office treatment for MGD.11 The system employs wearable SmartLid devices that are placed onto the patient’s lids while preserving the patient’s natural blink.12 The session is activated by a SmartHub controller, which sets the temperature of the four SmartLids to a therapeutically optimal temperature of 45°C, above the 41°C threshold necessary to soften and melt meibum.7,12–14 Following the 15-minute heating session, manual gland expression is performed by the clinician using proprietary forceps.
Several clinical trials have studied the safety and efficacy of TearCare. In a multicenter, masked, randomized control trial, subjects who received a single TC treatment demonstrated significant improvements in their mean tear break-up time (TBUT) and meibomian gland secretion score (MGSS).12 The mean Eye Dryness Score (EDS), Symptom Assessment in Dry Eye (SANDE), and Ocular Surface Disease Index (OSDI) scores were also significantly reduced.12 In a clinical trial comparing TC and Lipiflow systems in reducing symptoms of DED, subjects with more severe disease (MGSS < 7) achieved statistically greater improvement with TC compared to LipiFlow in their total OSDI scores, quality of vision, and SANDE frequency scores.15 Another study comparing outcomes of DED treated with TC versus cyclosporine 0.05% showed that the TC group had greater improvement in TBUT and MGSS, supporting the use of TC as the preferred treatment for MGD.13
While clinical parameters and patient questionnaires are frequently utilized in DED research, measurement of reading speed can be a useful method to assess functional impairment from DED. Studies have shown that DED patients have slower reading speeds, which is correlated with the severity of disease.16,17 The International Reading Speed Texts (IReST) is a standardized assessment of reading speed in a natural context.18 Other assessments such as the Minnesota Low Vision Reading Test (MNREAD) and Wilkins Rate of Reading Test (WRRT) have also been employed in vision research.19,20 To date, there have been no studies that assess how interventional procedures for MGD, such as TC, impact functional metrics. In this prospective, single center clinical trial, we aim to evaluate the efficacy of TC in a population with DED from MGD using clinical, quality of life, and functional visual outcome metrics.
Materials and Methods
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Sterling Institutional Review Board (protocol #9478). Consent was obtained by the study participants prior to study commencement, and the participants were informed about the purpose of the study. This study was a prospective, single-center clinical trial. Any adult patient with a prior DED diagnosis and MGD with TBUT <10 seconds was eligible to be included in the study. All subjects had to have at least 20/40 or better vision in both eyes, no new treatment for DED or surgeries within 60 days prior to the initial study visit and have a high-school level education or higher.
All patients had two visits: one at baseline prior to TC and one 1 month after the TC procedure. At each visit, subjects underwent a clinical exam and reading speed and questionnaire testing. The clinical exam included slit-lamp exam, MGSS, TBUT, and corneal fluorescein staining (KFL) assessment. Patients were given 3 questionnaires to assess symptoms and visual function: OSDI, National Eye Institute Visual Function Questionnaire 25 (NEI VFQ-25), and the Fatigue Severity Scale. Patients were given 3 reading tests to assess reading speed and function: out-loud reading speed using the MNRead which was used to assess maximum reading speed, IReST (paragraph form of reading text), and the WRRT.
The TC device was used according to manufacturer’s approved instructions as described in the Instructions for Use (IFU). Patients had eyelid skin cleansed with a moist towelette, and SmartLids were placed above the lash line over the meibomian glands on all four eyelids. The 15-minute heating cycle was maintained per the IFU. Once completed, the SmartLids were removed, and manual expression using the Clearance Assistant Forceps was performed on all four eyelids.
A power calculation was performed prior to initiation of the study to determine that 32 patients would be an appropriate sample size, as was calculated using an alpha of 0.05 and power of 80%. This was calculated based on the IReST meaningful difference to be greater than 10 words per minute (wpm), as published in the literature.18 Data were analyzed using Microsoft Excel (Version 16.68) and GraphPad Prism for Mac (v.8, GraphPad Software). Differences between patients pre- and post-treatment were analyzed using appropriate statistical methods. A chi-squared test was used for analyses involving exclusively nominal variables (for example, gender and race). Analyses involving continuous variables utilized the paired t-test. A p-value less than or equal to 0.05 was considered statistically significant.
Results
A total of 32 subjects were included in this study, of whom 81.3% were female (Table 1). The average age in the cohort was 55.9 years with a range of 31 to 79 years. At baseline, subjects had severe MGD, with an average MGSS of 4.1 ± 2.5 (on a scale from 0 to 45 with <12 considered to be abnormal). Prior to treatment, subjects had diminished reading speed, averaging 163.6 ± 33.9 words/min on the IReST test. As a reference, normally sighted readers average approximately 184 ± 29 words/min.18
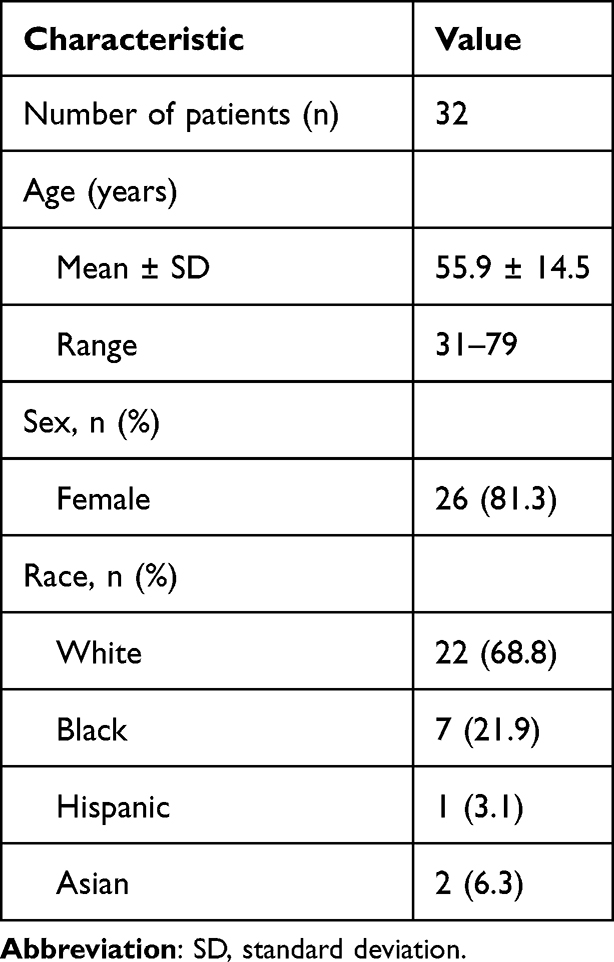 |
Table 1 Baseline Patient Demographics |
Sixteen (52%) participants had a clinically significant improvement in reading speed after treatment with TC, defined as >10 wpm increase in their IReST score. On average, there was improvement in all of the functional reading assessments after TC treatment when compared to baseline (Table 2). Specifically, improvement on the IReST and the MNREAD reached statistical significance after TC treatment (p = 0.012 and p = 0.028, respectively). Among the administered patient questionnaires, OSDI scores significantly decreased from 45.7 ± 24.9 to 33.4 ± 22.7 post-treatment (p < 0.001) and NEI VFQ-25 scores significantly increased from 73.8 ± 15.7 to 80.5 ± 13.2 (p < 0.001). Section B of the OSDI questionnaire contains questions related to visual function,15 and a statistically significant improvement was also seen when isolating OSDI scores to section B only after administration of TC (p = 0.009). Notably, all of the clinical exam parameters showed statistically significant improvement after treatment. The mean pre-treatment MGSS improved from 4.2 ± 2.5 to 6.1 ± 2.4 (p < 0.001), the mean pre-treatment TBUT improved from 5.2 ± 2.6 to 6.5 ± 2.6 seconds (p < 0.001), and the mean pre-treatment KFL scores decreased from 0.6 ± 0.2 to 0.3 ± 0.3 (p = <0.0001) when compared to post-treatment.
 |
Table 2 Pre-Treatment and Post-Treatment Results |
Further subgroup analysis showed that patients who experienced >10 wpm increase in their IReST score had a greater improvement in their KFL scores post-treatment (−0.5 ± 0.1 vs −0.3 ± 0.1, p = 0.049). Those same patients also had higher OSDI scores pre-treatment suggesting that they had more visual symptoms from their DED; however, this difference was not statistically significant (50.7 ± 5.9 vs 40.8 ± 6.5, p = 0.27). Patients who had an improvement of their TBUT by 2 or more seconds were more likely to have lower MGSS and TBUT pre-treatment, suggesting more significant disease at baseline (3.1 ± 0.5 vs 5.0 ± 0.7 p = 0.034; 4.6 ± 0.3 vs 5.8 ± 0.4, p = 0.047, respectively). There were no demographic differences between patients who experienced a >10 wpm increase in their IReST score and those who did not, or between patients who had an improvement in their TBUT by 2 or more seconds and those who did not.
Discussion
In our study, more than half of the subjects experienced a clinically meaningful improvement in reading speed with a single TC treatment. Statistically significant improvements in reading speeds were seen in two out of three reading tests, and significant improvements in both DED signs (TBUT, MGSS, and KFL) and symptoms (OSDI and NEI VFQ-25) were also observed post-treatment when compared to pre-treatment baseline. The improvement in OSDI scores following treatment was also statistically significant when the scores were isolated to section B only, which focuses on visual function-related questions. These results suggest that a single treatment of TC is effective in treating DED secondary to MGD and thus TC should be considered in patients with reduced visual function who experience difficulty reading and/or blurred vision from their DED.
Dry eye disease can significantly impact visual function and performance. Several published reports suggest that DED negatively impacts visual acuity, leading to a decrease in concentration, productivity, and ability to accomplish daily activities.21–23 One method of assessing visual function is through reading speed. Many reading tests have been developed for use in clinical studies. In our study, three reading tests were employed to assess visual function. The IReST test is a standardized non-stress-inducing reading test that has low within-subject variability.18 Patients are given whole paragraphs to read, rather than single sentences, as paragraphs more closely mimic the demands of everyday reading.18 The WWRT, on the other hand, uses a passage with no semantic content and is designed to stress the visual processing system.24 Both IReST and WWRT have been previously used in DED research.17,25 Unlike the IReST and WWRT, the MNREAD uses continuous text acuity charts and allows for assessment of the maximum reading speed. In our study, all of the subjects had improvement in their reading speed post-treatment. Research has suggested that a >10 wpm increase in the IReST score indicates a clinical significant improvement.18 Because the IReST test most closely mimics everyday reading, we conducted a sub-analysis of patients who had >10 wpm increase in their IReST score following treatment with TC. There were no demographic differences between subjects who experienced a >10 wpm increase in their IReST score post-treatment compared to those who did not. Subjects with a >10 wpm increase in their IReST score had greater improvements in their KFL scores post-treatment (−0.5 ± 0.1 vs −0.3 ± 0.1, p = 0.049). They also had higher OSDI scores pre-treatment (50.7 ± 5.9 vs 40.8 ± 6.5, p = 0.27), suggesting they were more symptomatic at baseline, though this difference did not reach statistical significance. The minimal clinically important difference (MCID) is used in clinical trials to evaluate for a meaningful difference following an intervention.26 It is defined as the smallest difference in score in the domain of interest which patients perceive as beneficial and which would mandate, in the absence of troublesome side effects and excessive cost, a change in the patient’s management. 27 A greater OSDI score change of 7.3 to 13.4 has been proposed to be the MCID for severe DED.26 In our cohort, 20 out of 32 (62.5%) patients had an OSDI score of 33 or greater (suggestive of severe disease). Among those 20 individuals, 16 (80%) met the MCID criteria for having a reduction in OSDI score between 7.3 and 13.4, suggesting that the administration of TC provides a meaningful improvement for the majority of patients with severe DED.
In the evaluation of MGD, TBUT is a common exam parameter used by clinicians. The presence of meibum is critical for the stability of the tear film, and in MGD, obstruction of the meibomian glands causes reduced secretion of meibum and thus rapid tear film evaporation. A TBUT of >10 seconds is considered to be normal, with 5 to 10 seconds considered to be marginal and < 5 seconds considered to be low.28 In our cohort, the average TBUT was 5.2 ± 1.6 seconds. We found that patients who had an improvement of their TBUT by 2 or more seconds after their TC treatment were likely to have lower MGSS and TBUT at baseline (3.1 ± 0.5 vs 5.0 ± 0.7, p = 0.034; 4.6 ± 0.3 vs 5.8 ± 0.4, p = 0.047, respectively), indicating more significant disease. There were no demographic differences between subjects who experienced a TBUT improvement of 2 or more seconds post-treatment and those who did not. Our results suggest that TC may provide additional benefits for patients with more severe disease and thus should be considered in patients with mild, moderate, and severe MGD, especially if they fail at-home therapies.
Our study has several limitations. First, the clinical parameters are graded by the clinician evaluating each subject, which can be subjective. As such, the use of objective parameters such as the measurements of reading speed was implemented to decrease the subjective nature of the study. Second, subjects were only followed for 1 month after their treatment. A longer follow-up period would help demonstrate the long-term benefits of TC and potentially identify patients who peak in their improvement beyond 1 month, as effects of TC have been shown to last up to 12 months post-treatment.29 Third, one factor that affects dry eye disease and reading is the blink rate, which was not assessed and could be included in future studies on this subject. Finally, a single-center study limits the generalizability of the results, and additional multi-center studies are needed to evaluate the long-term impacts of TC treatment.
Conclusion
This prospective study adds to the growing body of literature that supports the use of TC in treating patients with DED and MGD. In addition to improvements in clinical parameters and patients’ quality of life, our results show that a single treatment of TC also improves visual function. By improving the tear film function, TC likely allows for better optical quality resulting in improved reading ability. To our knowledge, this is the first study that assesses changes in reading speed following treatment with TC. Given the high prevalence of DED, new office-based therapies such as TC should be utilized to reduce the disease burden of DED and improve patients’ visual function and quality of life.
Acknowledgments
The abstract of this paper was presented at the American Society of Cataract and Refractive Surgery Conference in 2024 as a poster presentation with interim findings.
Funding
This study was supported by an educational grant from Sight Sciences.
Disclosure
PG and NV are consultants to Sight Sciences. The authors report no other conflicts of interest in this work.
References
1. McDonald M, Patel DA, Keith MS, et al. Economic and humanistic burden of dry eye disease in Europe, North America, and Asia: a systematic literature review. Ocul Surf. 2016;14(2):144–167. doi:10.1016/j.jtos.2015.11.002
2. Ding J, Sullivan DA. Aging and dry eye disease. Exp Gerontol. 2012;47(7):483–490. doi:10.1016/j.exger.2012.03.020
3. Yu J, Asche CV, Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea. 2011;30(4):379–387. doi:10.1097/ICO.0b013e3181f7f363
4. Rabensteiner DF, Aminfar H, Boldin I, et al. The prevalence of meibomian gland dysfunction, tear film and ocular surface parameters in an Austrian dry eye clinic population. Acta Ophthalmol (Copenh). 2018;96(6):e707–e711. doi:10.1111/aos.13732
5. Lemp MA, Crews LA, Bron AJ, et al. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012;31(5):472–478. doi:10.1097/ICO.0b013e318225415a
6. Findlay Q, Reid K. Dry eye disease: when to treat and when to refer. Aust Prescr. 2018;41(5):160–163. doi:10.18773/austprescr.2018.048
7. Blackie CA, Solomon JD, Greiner JV, et al. Inner eyelid surface temperature as a function of warm compress methodology. Optom Vis Sci off Publ Am Acad Optom. 2008;85(8):675–683. doi:10.1097/OPX.0b013e318181adef
8. Bitton E, Lacroix Z, Léger S. In-vivo heat retention comparison of eyelid warming masks. Contact Lens Anterior Eye J Br Contact Lens Assoc. 2016;39(4):311–315. doi:10.1016/j.clae.2016.04.002
9. Alghamdi YA, Camp A, Feuer W, et al. Compliance and subjective patient responses to eyelid hygiene. Eye Contact Lens. 2017;43(4):213–217. doi:10.1097/ICL.0000000000000258
10. Chuckpaiwong V, Nonpassopon M, Lekhanont K, et al. Compliance with lid hygiene in patients with meibomian gland dysfunction. Clin Ophthalmol Auckl NZ. 2022;16:1173–1182. doi:10.2147/OPTH.S360377
11. Tearcare. Sight sciences receives FDA 510(k) clearance of the tearcare system for treatment of meibomian gland dysfunction (MGD), the leading cause of dry eye disease. December 2021. Available from: https://tearcare.com/sight-sciences-receives-fda-510k-clearance-of-the-tearcare-system-for-treatment-of-meibomian-gland-dysfunction-mgd-the-leading-cause-of-dry-eye-disease/.
12. Gupta PK, Holland EJ, Hovanesian J, et al. TearCare for the treatment of meibomian gland dysfunction in adult patients with dry eye disease: a masked randomized controlled trial. Cornea. 2022;41(4):417–426. doi:10.1097/ICO.0000000000002837
13. Ayres BD, Bloomenstein MR, Loh J, et al. A randomized, controlled trial comparing tearcare® and cyclosporine ophthalmic emulsion for the treatment of dry eye disease (SAHARA). Clin Ophthalmol Auckl NZ. 2023;17:3925–3940. doi:10.2147/OPTH.S442971
14. Borchman D. The optimum temperature for the heat therapy for meibomian gland dysfunction. Ocul Surf. 2019;17(2):360–364. doi:10.1016/j.jtos.2019.02.005
15. Holland EJ, Loh J, Bloomenstein M, et al. A comparison of tearcare and lipiflow systems in reducing dry eye disease symptoms associated with meibomian gland disease. Clin Ophthalmol Auckl NZ. 2022;16:2861–2871. doi:10.2147/OPTH.S368319
16. Mathews PM, Ramulu PY, Swenor BS, et al. Functional impairment of reading in patients with dry eye. Br J Ophthalmol. 2017;101(4):481–486. doi:10.1136/bjophthalmol-2015-308237
17. Ridder WH, Zhang Y, Huang J-F. Evaluation of reading speed and contrast sensitivity in dry eye disease. Optom Vis Sci off Publ Am Acad Optom. 2013;90(1):37–44. doi:10.1097/OPX.0b013e3182780dbb
18. Trauzettel-Klosinski S, Dietz K. IReST Study Group, Standardized assessment of reading performance: the new international reading speed texts IReST. Invest Ophthalmol Vis Sci. 2012;53(9):5452–5461. doi:10.1167/iovs.11-8284
19. Altinbay D, Adibelli FM, Taskin I, et al. The evaluation of reading performance with Minnesota low vision reading charts in patients with age-related macular degeneration. Middle East Afr J Ophthalmol. 2016;23(4):302–306. doi:10.4103/0974-9233.194078
20. Xiong Y-Z, Calabrèse A, Cheong AMY, et al. Reading acuity as a predictor of low-vision reading performance. Invest Ophthalmol Vis Sci. 2018;59(12):4798–4803. doi:10.1167/iovs.18-24716
21. Szczotka-Flynn LB, Maguire MG, Ying G-S, et al. Impact of dry eye on visual acuity and contrast sensitivity: dry eye assessment and management study. Optom Vis Sci off Publ Am Acad Optom. 2019;96(6):387–396. doi:10.1097/OPX.0000000000001387
22. Yamada M, Mizuno Y, Shigeyasu C. Impact of dry eye on work productivity. Clin Outcomes Res CEOR. 2012;4:307–312. doi:10.2147/CEOR.S36352
23. Pflugfelder SC. Prevalence, burden, and pharmacoeconomics of dry eye disease. Am J Manag Care. 2008;14(3 Suppl):S102–106.
24. Wilkins AJ, Jeanes RJ, Pumfrey PD, et al. Rate of Reading Test: its reliability, and its validity in the assessment of the effects of coloured overlays. Ophthalmic Physiol Opt J Br Coll Ophthalmic Opt Optom. 1996;16(6):491–497. doi:10.1046/j.1475-1313.1996.96000282.x
25. Ousler GW, Rodriguez JD, Smith LM, et al. Optimizing reading tests for dry eye disease. Cornea. 2015;34(8):917–921. doi:10.1097/ICO.0000000000000490
26. Miller KL, Walt JG, Mink DR, et al. Minimal clinically important difference for the ocular surface disease index. Arch Ophthalmol Chic IL 1960. 2010;128:94–101. doi:10.1001/archophthalmol.2009.356
27. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10(4):407–415. doi:10.1016/0197-2456(89)90005-6
28. Vidas Pauk S, Petriček I, Jukić T, et al. Noninvasive tear film break-up time assessment using handheld lipid layer examination instrument. Acta Clin Croat. 2019;58(1):63–71. doi:10.20471/acc.2019.58.01.09
29. Chester T, Ferguson T, Chester E. Localized heat treatment for meibomian gland dysfunction: a single-center retrospective analysis of efficacy over time. Optom Vis Sci off Publ Am Acad Optom. 2023;100(9):625–630. doi:10.1097/OPX.0000000000002053
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.