")
Back to Journals » Patient Preference and Adherence » Volume 19
Improving Medication Adherence in Heart Failure Through Pharmacist-Led Patient Education: Protocol for a Mechanism-Based Study of Information, Motivation, and Behavioral Skills
Authors Chien TCR, Weng SE, Hsu WT
Received 11 March 2025
Accepted for publication 10 June 2025
Published 26 June 2025 Volume 2025:19 Pages 1855—1868
DOI https://doi.org/10.2147/PPA.S527419
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Tung-Chun Russell Chien,1,2 Shao-En Weng,3 Wan-Tseng Hsu1,2,4
1Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan; 2School of Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan; 3Department of Pharmacy, Taipei City Hospital Zhongxing Branch, Taipei, Taiwan; 4Department of Pharmacy, National Taiwan University Hospital, Taipei, Taiwan
Correspondence: Shao-En Weng, Department of Pharmacy, Taipei City Hospital Zhongxing Branch, 145 Zhengzhou Road, Datong Dist., Taipei City, 103212, Taiwan, Tel +886 2 2552-3234, Email [email protected] Wan-Tseng Hsu, School of Pharmacy, National Taiwan University, 33 Linsen S. Road, R201, Zhongzheng Dist, Taipei City, 100025, Taiwan, Tel +886 2 3366-8195, Fax +886 2 2391-9098, Email [email protected]
Background: Heart failure (HF) remains a major global health challenge. Guideline-directed medical therapy can effectively reduce mortality and hospitalizations; however, persistent medication nonadherence hinders its real-world impact. Although recent guidelines emphasize the pivotal role of pharmacists in supporting medication adherence, the mechanisms through which pharmacist-led patient education influences medication adherence remain underexplored. Identifying these mechanisms could inform the development of evidence-based strategies to optimize medication adherence and ultimately improve long-term outcomes in HF management.
Objective: This study aims to establish an Information–Motivation–Behavioral Skills (IMB) model to elucidate the mechanisms influencing medication adherence among patients with HF and to compare pre- and postintervention models for identifying significant pathways affected by pharmacist-led patient education.
Methods: In this longitudinal pretest–posttest study, all IMB constructs—information, personal motivation, social motivation, behavioral skills, and behavior—will be assessed using validated patient-reported outcome measures (PROMs) at baseline and three and six months postintervention; additionally, verbal inquiries will be conducted to evaluate the information construct and prescription refill data will be incorporated to supplement the behavior construct. Multigroup structural equation modeling will examine relationships among these constructs and their impact on medication adherence. Latent class growth modeling will also be employed to identify distinct adherence trajectory subgroups after six-month follow-up.
Expected Outcomes: The recruitment phase commenced in early May 2025. By evaluating structural changes in IMB pathways pre- and postintervention using PROMs, followed by identifying short-term and sustained responders, the study is expected to facilitate the precise targeting of pharmacist-led interventions to maximize clinical impact. This approach emphasizes the importance of tailoring healthcare delivery to individual medication adherence profiles. It aims to ensure that pharmacist-led patient education achieves its fullest potential in populations expected to benefit the most, particularly patients with HF—a perspective that, to our knowledge, has not been previously explored.
Keywords: information–motivation–behavioral skills model, heart failure, pharmacist-led patient education, structural equation modeling, medication adherence, latent class growth modeling
Introduction
Heart failure (HF) is a pervasive and quintessential clinical syndrome that disproportionately affects geriatric populations, contributing to poor health-related quality of life (HRQoL)1 and remaining a leading global health concern.2 In 2019, an estimated 56 million individuals worldwide were battling HF; its prevalence is projected to increase from 2.4% in 2012 to 3.0% by 2030.3 Significant progress has been made in improving outcomes, especially for patients with HF with reduced ejection fraction (HFrEF), a condition characterized by high hospitalization rates and mortality.4,5 Recent advances are attributed primarily to guideline-directed medical therapy (GDMT), which has been shown to reduce hospitalizations, improve survival rates, and enhance HRQoL.6–8 Given the promising benefits of GDMT, high utilization rates would be expected in real-world settings.
However, the persistent issue of medication nonadherence continues to limit the transformative potential of GDMT for patients with HF.9 This issue is particularly pronounced in geriatric populations, who experience the greatest HF burden, thereby undermining the benefits of GDMT and resulting in poor prognoses.10,11 Medication adherence, which mediates the association between HRQoL and survival,5 is challenged by the compounded effects of polypharmacy, adverse side effects, inherent aging-related frailties, and comorbidities.12,13 Current HF guidelines still mandate an essential compromise and advocate the use of multiple medications (often exceeding five) exclusively for HF management, implicitly framing polypharmacy as an unavoidable trade-off to achieve optimal patient outcomes.7 This paradox reinforces polypharmacy as both a sanctioned standard and a persistent barrier to medication adherence in the populations,14 which contributes to the deterioration of HRQoL.15 Consequently, adherence rates are only 40%–60%, reflecting the difficulty in achieving and sustaining optimal medication use.16 Clinical inertia among healthcare professionals and intolerance among patients with HF further complicate this landscape and hinder the full implementation of GDMT.17 Therefore, nonadherence continues to impede optimal HF outcomes, and the promise of GDMT can be realized only if this issue is effectively addressed.18
HF clinical practice guidelines (the 2022 American Heart Association, American College of Cardiology, Heart Failure Society of America [AHA/ACC/HFSA]) recognize that nonadherence jeopardizes the potential of GDMT and underutilization compromises its outcomes.19 However, patients with HF often face unique challenges, with worse outcomes among older patients compared with their younger counterparts.13,20,21 This scenario demands dedicated efforts to refine care strategies that specifically target patients with HF, many of whom face ongoing risks related to health disparities.20,21
The ACC/AHA/HFSA emphasizes a collaborative, team-based approach that has become prominent in HF management.7 Notably, pharmacists are indispensable in reinforcing medication adherence and facilitating the appropriate use of GDMT among patients with HF.7,22 For example, pharmacists optimize GDMT by offering evidence-based recommendations, deprescribing potentially inappropriate medications, monitoring drug–drug interactions, and performing drug use evaluations to prevent medication-related issues.23–25 Such pharmacist-led interventions have delivered wide-ranging favorable outcomes in both inpatient and outpatient settings,23–26 and these positive outcomes support the integration of pharmacists into multidisciplinary HF management teams,22,27 especially for improving medication adherence.28–32
Nevertheless, the benefits of pharmacist-led interventions could dissipate over time, particularly after active intervention ends.30 Thus, critical concerns arise about gaps in the sustainability and long-term effectiveness of such initiatives. Additionally, mechanisms influencing medication adherence (e.g., motivational factors, behavioral tendencies, and patient–pharmacist interactions) remain insufficiently understood. Intensive exploration of such mechanisms could inform the development of sustainable and effective pharmacist-led interventions that can continually improve medication adherence and HRQoL, eventually optimizing HF outcomes.
The Information–Motivation–Behavioral Skills (IMB) model, developed by Jeffrey D. Fisher and William A. Fisher in 1992, offers a promising theoretical framework for addressing the complexities of health behavior change.33 Originally designed to promote acquired immunodeficiency syndrome-preventive behaviors,34 the IMB model has since been applied to various health-related behaviors, including medication adherence.35–37 The model comprises four core components—information, personal motivation, social motivation, and behavioral skills—which interact to influence the enactment of health-related behaviors, conceptualized as the fifth construct (Figure 1).33
 |
Figure 1 Structure of the Information–Motivation–Behavioral Skills (IMB) model. The IMB model illustrates the relationships between information, motivation (personal and social), behavioral skills, and behavior. The model demonstrates how these components influence behavior, with behavioral skills mediating the effects of information and motivation on behavior. |
Specifically, information refers to reliable and accurate knowledge about health behaviors and their implications, facilitating behavioral changes; conversely, misinformation can hinder this process. In the context of medication adherence, information entails understanding the importance of adhering to prescribed regimens, recognizing potential side effects, and comprehending the consequences of nonadherence. Healthcare practitioners, particularly pharmacists, are crucial in delivering information through effective communication and education.38
Motivation encompasses both personal and social dimensions.39 Personal motivation reflects individual values, attitudes, and beliefs toward health behaviors, while social motivation stems from friends, peers, family, societal norms, and support systems.40 Notably, support received from family members, peers, and particularly pharmacists enhances medication adherence.38,41 The higher the satisfaction with pharmacist-provided services, the more likely are patients to adhere to their medication regimens.38 Thus, pharmacist-led patient education reinforces positive social motivation, further promoting medication adherence.
Behavioral skills refer to the capabilities and self-efficacy individuals need to consistently engage in health-promoting behaviors, such as organizing medications, setting reminders, and maintaining medication adherence routines. These skills are essential for empowering individuals to overcome practical barriers to medication adherence.
These four fundamental constructs—information, personal motivation, social motivation, and behavioral skills—interact dynamically through direct, indirect, and reciprocal pathways to influence medication adherence (the behavior construct) (Figure 1).33,38 A clear understanding of medication instructions (i.e., information) may independently encourage medication adherence, whereas motivation may drive efforts to acquire more health-related knowledge. Although knowledge alone may not guarantee medication adherence, it enables patients to interpret prescriptions and take appropriate actions, bridging the gap between intention and behavior. Therefore, behavioral skills are necessary to translate knowledge and intention into action, with enhanced motivation at both personal and social levels. While motivation for adherence and knowledge of medication usage and potential side effects mutually reinforce each other, patients develop greater self-efficacy, promoting medication adherence. These factors intertwine and highlight why targeted interventions—especially pharmacist-led ones—may improve long-term medication adherence, thus enhancing HRQoL and prognosis among patients with HF.
Taken together, the IMB model provides a valuable framework for understanding the multifaceted nature of medication adherence and insights into designing targeted interventions to achieve sustained, effective improvements in HF management. To the best of our knowledge, the IMB model has not yet been validated in patients with HF, nor has it been employed to specify how pharmacist-led patient education can enhance medication adherence in this population. Accordingly, this study aims to use the IMB model as a conceptual framework to examine the mechanisms through which pharmacist-led patient education influences medication adherence among patients with HF. A longitudinal pretest–posttest design will be employed to assess changes in medication adherence before and after the intervention. Patient-reported outcome measures (PROMs) will be integrated within the IMB framework, and structural equation modeling (SEM) along with latent class growth modeling (LCGM) will be applied to analyze the pathways affecting medication adherence and to identify distinct adherence trajectories.
Materials and Methods
Study Aims
This study’s aims are threefold. Primarily, it aims to apply the IMB model using PROMs to investigate the impact of pharmacist-led patient education on medication adherence among individuals with HF. It hypothesizes that patients who acquire accurate medication-related knowledge, develop personal motivation, receive supportive social motivation from pharmacists and other sources, and possess adequate behavioral skills regarding medication use will exhibit significantly high levels of medication adherence. Furthermore, the study also seeks to compare the IMB models pre- and postintervention to identify the pathways most influential in improving medication-taking behaviors. This comparison will inform refinements in existing pharmacist-led patient education programs. Multigroup SEM will be used to specify the pre- and postintervention models, testing whether specific relationships among IMB constructs are significantly strengthened or weakened following pharmacist-led patient education. This analysis will help identify the pathways that are the most responsive to intervention and inform targeted refinements in pharmacist counseling strategies. Finally, adherence trajectories will be classified using LCGM following pharmacist-led patient education in order to identify distinct patient subgroups based on their long-term adherence patterns. Subsequent multigroup SEM and comparisons of baseline characteristics will be conducted between subgroups to determine whether IMB pathways or demographic factors differ between responders, providing evidence to refine pharmacist-led interventions for sustained medication adherence.
Study Design
This prospective pre- and postintervention study will administer the same PROMs to eligible participants before and after pharmacist-led patient education. Baseline (preintervention) assessment will be performed immediately before the education session, and follow-up assessments will be administered approximately three and six months postintervention, aligning with routine HF follow-ups (i.e., 3-month intervals) in clinical practice.
Ethical Considerations
The study received approval from the Institutional Review Board and Ethics Committee of National Taiwan University Hospital (NTUH) (No. 202501197RINC). All eligible participants will be invited and fully informed of research objectives and procedures; voluntary informed consent will be obtained before study commencement. Participants will be assured of their entitlement to withdraw without negative repercussions at any time.
Study Setting
This study will be conducted in NTUH, a leading medical center in Taipei, Taiwan. Pharmacist-led sessions will be conducted in the HF education room near the pharmacist-led HF clinic, accessible by clinician referral.
Study Participants
Patients referred with HFrEF (defined as a left ventricular ejection fraction ≤ 40%)7 as well as those referred at the clinicians’ discretion, will be invited to participate via purposive sampling. Eligibility criteria include patients aged ≥ 20 years, referred by their clinicians, and willing to participate. Given the pragmatic nature of this pharmacist-led intervention, strict inclusion and exclusion criteria are intentionally not applied to better reflect real-world scenarios. Participants will be excluded only if they have previously received patient education at the pharmacist-led HF clinic in the NTUH, fail to complete baseline assessments, or are unwilling to participate. Consecutive eligible and willing participants will provide written informed consent before receiving pharmacist-led patient education. Recruitment will continue until the estimated sample size is reached.
Study Intervention
The Advanced Patient-centered Pharmacist-Led Education on Heart Failure (APPLE-HF) management program was developed to support patients with HF in the pharmacist-led HF clinic (Figure 2); this service at NTUH is accessible only upon clinician referral. In this program, well-trained pharmacists with clinical pharmacy experience will deliver patient education sessions on a rotating schedule. Before this, all pharmacists will receive a standardized compendium containing evidence-based training materials to ensure consistency in education delivery.
 |
Figure 2 Illustration of the Advanced Patient-centered Pharmacist-Led Education on the Heart Failure (APPLE-HF) management program. The program integrates pharmacist-led individualized counseling, which addresses barriers to medication adherence and suggests lifestyle and supportive measures. Patients are referred by clinicians and co-managed with assigned pharmacists. They receive tailored education informed by the latest HF guidelines. Key components of the APPLE-HF management program include (1) using predefined consolidated medication lists to collaboratively review prescriptions and advance adherence strategies; (2) addressing barriers to adherence through proactive discussions and interactive dashboards with patient-specific visualizations of risks and projected survival curves to identify misconceptions and enhance medication adherence; and (3) guiding lifestyle modifications, including dietary control, fluid management, and exercise. This team-based, patient-centered model aims to improve HF outcomes. Abbreviation: GDMT, guideline-directed medical therapy. |
Upon referral to the pharmacist-led HF clinic, patients will receive co-management by their primary clinicians and assigned consulting pharmacists, fostering a comprehensive, team-based model of care.7 Prior to the patient’s scheduled education visit, the clinical team will thoroughly review medical records, laboratory data, medication history (including data retrieved from the National Health Insurance [NHI] MediCloud System), and current prescriptions to document all current medications. Subsequently, a hard copy of the consolidated medication list will be provided during and after the education sessions for patients to monitor potential drug–drug or drug–food interactions and verify prescriptions following recognized HF guidelines.7,42 Any identified concerns—particularly related to GDMT and its up-titration to target doses, such as potentially inappropriate prescriptions, notable adverse effects or interactions, or suboptimal use—will be recorded in the electronic health records (EHR), prepared for subsequent in-depth discussion with the patient, and communicated to the attending clinicians.
Face-to-face sessions will generally occur on the same day following the clinician visit, in lieu of patient preference, or as scheduled separate visits, with each session lasting approximately 1 h. The customized APPLE-HF program, enhanced by the interactive visualization dashboards developed by our research team,43,44 is based on the most recent 2022 and 2024 AHA/ACC guidelines on HF management.7,42 It begins with an introductory discussion and adopts the following three core objectives to improve clinical outcomes (Figure 2):
- Individualized counseling: Pharmacists will adapt educational content to each patient’s clinical profiles and health literacy. Counseling will follow the ACE Medication Adherence framework, which includes clarifying each medication’s purpose (as detailed in the consolidated medication list), explaining common adverse effects and interactions, assessing medication adherence, and demonstrating self-monitoring techniques (e.g., blood pressure and body weight monitoring), with an emphasis on reinforcing the appropriate use of GDMT.
- Addressing barriers to adherence: Pharmacists will employ a think-aloud approach to uncover misconceptions about prescriptions, particularly GDMT, including concerns about side effects (e.g., hypotension), perceived benefits or risks, and doubts about efficacy. Through proactive discussions, incorporating nonverbal communication and empathetic responses, patients will be encouraged to articulate underlying factors affecting their medication adherence. This process will enable pharmacists to recommend practical, individualized reinforcement strategies. The interactive visualization dashboards will be pragmatically integrated into the intervention and leveraged at the pharmacist’s discretion to address patient-specific needs.43,44 The dashboards use patient-specific data to illustrate risk differences and projected survival curves based on selected patient-related variables and treatment options in real time. The dashboard-generated visualizations can facilitate a deeper understanding of different options and treatment plans, particularly among geriatric patients with HF, alleviating concerns that might otherwise impede medication adherence, and empowering patients with the motivation to change their behaviors.43,44
- Lifestyle and supportive measures: Pharmacists will provide individualized guidance on lifestyle modifications, such as recommendations on protein- and potassium-rich dietary control, fluid management, and exercise, among others. Emphasis will be placed on how these nonpharmacologic interventions can complement and enhance the effectiveness of pharmacotherapy.
Following regulatory guidelines in Taiwan, pharmacists do not have the authority to prescribe independently. Consequently, any pharmacist recommendations will be formally documented in the EHR. Such proposed modifications to the patient’s pharmacotherapeutic regimen or additional tests will be communicated to the attending clinicians. This interdisciplinary process will ensure the systematic integration of pharmacist-initiated suggestions into the APPLE-HF program.
Early introduction and stepwise up-titration of GDMT according to established HF treatment guidelines is essential.7 Pharmacists will employ an evidence-based, stepwise strategy to achieve recommended or maximally tolerated doses, balancing efficacy with safety.7,42 Given that complications such as hypotension, hyperkalemia, and renal dysfunction may arise during GDMT initiation or up-titration, careful monitoring will be implemented.12 The approach will focus on proactive strategies such as advising patients to tolerate mild hypotension when clinically appropriate, promoting professional guidance before self-discontinuing medication, and recognizing early warning signs.45
By systematically integrating medication counseling, comprehensive patient education, and cohesive collaboration with prescribing clinicians, the APPLE-HF program addresses patient concerns about therapy, improves GDMT, medication adherence, and long-term clinical outcomes, and enables patient engagement in treatment. This structured pharmacist-led intervention strategy fosters an environment in which the patient is engaged and knowledgeable about the treatment plan, thereby encouraging medication adherence.
Study Measures
Seven PROMs will be administered face-to-face to eligible patients before and three and six months after the intervention (i.e., all questions except sociodemographic items will have to be answered three times) to assess the IMB model’s five corresponding components. The first instrument is a sheet containing 13 sociodemographic questions (age, sex, education, employment status, marital status, living status, monthly income, number of medications taken, self-reported HF status, self-reported health status, exercise status, experience of using digital health tools, and attitude toward using digital health tools), followed by a PROM involving oral inquiries and six PROMs presented as a 48-item sheet, as outlined below.
Medication Understanding Questionnaire (MUQ)
The MUQ assesses knowledge of medication purpose, dosage, and frequency.46 Each current GDMT (and diuretics) in the consolidated medication list will be evaluated on a 3-point scale: 1 point for the indication, 0.5 points for the dosage strength, 0.5 points for the dosage unit, and 1 point for the frequency. Oral inquiries will be incorporated into the patient education process. All medication scores will be averaged to assess patients’ overall understanding of the medication regimen and to measure the information construct.
Patient-Perceived Medication Knowledge and Confidence in Medication Use (Okere–Renier Survey)
The Okere–Renier Survey assesses patients’ medication knowledge and confidence in medication use. It has demonstrated good reliability and an acceptable model fit through prior exploratory and confirmatory factor analyses.47 The original survey comprises ten items divided into three dimensions: six items measure medication knowledge (of which one was finally removed due to low inter-item correlation), three assess confidence, and one evaluates satisfaction. Each item is rated on a five-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating greater knowledge and confidence. Given that the information construct in the IMB model emphasizes patients’ medication knowledge over confidence, only the five items examining medication knowledge were retained from the original questionnaire to measure this construct.
Beliefs About Medicines Questionnaire–Specific (BMQ-Specific)
The BMQ-Specific assesses patients’ beliefs about their prescribed medications and evaluates their personal motivation through two subscales: Necessity and Concerns.48,49 Each subscale comprises four items. The Necessity subscale captures patients’ perceptions of medication importance, while the Concerns subscale reflects potential fears or anxieties regarding medication use. Items are rated on a five-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating stronger beliefs. A previous study reported the Cronbach’s alpha values of 0.77 for the Necessity subscale and 0.76 for the Concerns subscale, demonstrating good reliability.49
Patient Satisfaction with Pharmacist Services Questionnaire 2.0 (PSPSQ 2.0)
Sakharkar et al developed and validated the PSPSQ 2.0 to measure patient satisfaction with pharmacist-provided services.50 The questionnaire has been translated into and validated in multiple languages; it comprises 16 items divided into two domains: 10 items assess patient satisfaction with the quality of care (QOC) and six evaluate satisfaction with the patient–pharmacist relationship (PPR). Each item was rated on a four-point Likert scale, ranging from 1 (strongly disagree) to 4 (strongly agree), with higher scores indicating greater satisfaction with pharmacist-provided services. The Traditional Chinese version of the modified PSPSQ 2.0 (C-mPSPSQ 2.0), translated and validated by our research team, will be used to assess the social motivation construct.51 The C-mPSPSQ 2.0 comprises six items retained from the original PSPSQ 2.0, demonstrating acceptable model fit and strong validity, with a Cronbach’s alpha of 0.919 and McDonald’s ω of 0.922; it includes three items assessing the QOC domain and three evaluating the PPR domain.
Medication-Specific Social Support Questionnaire (MSSS)
The MSSS evaluates the frequency with which patients received support for their medication-related behaviors over the preceding 3 months,52 capturing their social motivation component. The questionnaire comprises eight items, each rated on a scale from 0 (never) to 4 (very often), demonstrating good reliability and Cronbach’s alpha values of 0.878–0.920.37,52 The final score averages all item scores, with higher average scores indicating greater social support for medication-related behaviors. Along with the C-mPSPSQ 2.0, the MSSS was employed to collectively measure the social motivation construct.
Self-Efficacy for Appropriate Medication Use Scale (SEAMS)
The SEAMS assesses patients’ self-efficacy in medication management, indicating their behavioral skills. It demonstrated excellent reliability, with Cronbach’s alpha values of 0.89–0.93.53,54 The scale measures patients’ confidence in maintaining proper medication adherence under various environmental challenges. Responses are scored on a three-point scale from 1 (not confident) to 3 (confident), with higher scores indicating greater self-efficacy and stronger behavioral capabilities regarding medication use.
Eight-Item Morisky Medication Adherence Scale (MMAS-8)
The MMAS-8 is widely applied to assess patients’ medication adherence and actual medication-taking behavior.55 It comprises seven yes/no items and one item rated on a five-point frequency scale, with higher overall scores indicating better adherence to prescribed medications.
In addition to the MMAS-8, the proportion of days covered (PDC) will be calculated to assess medication adherence (the behavior construct). The PDC is a commonly used and preferred indicator for measuring medication adherence,56 calculated as the ratio of the number of days in a specified period during which patients have access to their medication (based on prescription refills) to the total number of days in the specified period. A threshold of 80% indicates adequate medication adherence.57 The PDC will be calculated 3 and 6 months postintervention using data from the NHI MediCloud System.
Data Collection
After completing baseline assessments, participants will be invited for the intervention session. During the session, a hard copy of the individualized consolidated medication list prepared by the assigned pharmacist will be provided to facilitate in-depth patient–pharmacist interaction; this list will also help assess patients’ understanding of current medications through oral inquiries (the MUQ). Participants will complete the same assessments and PROMs at 3 and 6 months postintervention. Baseline characteristics will be collected from a questionnaire comprising 13 sociodemographic items and a consolidated medication list, as well as from the EHR at NTUH, which includes medical history and comorbidities. All collected data will be de-identified and stored on a secure, access-restricted server. Access will be limited to authorized study personnel, and regular backups will be conducted to maintain data integrity.
Conceptual Framework
This study adopts the IMB model as its theoretical framework, comprising four core constructs—information, personal motivation, social motivation, and behavioral skills—which collectively influence patients’ medication adherence behaviors. The information construct was assessed using the Okere–Renier Survey and oral MUQ inquiries to evaluate patients’ depth of understanding regarding medication knowledge. Motivation is divided into two components: personal and social motivation. Personal motivation is measured using the BMQ-Specific, which evaluates patients’ beliefs about the necessity of medications and their concerns about potential adverse effects. Social motivation is assessed using two instruments: (1) the C-mPSPSQ 2.0, which evaluates patients’ satisfaction with pharmacist-provided services and (2) the MSSS, which evaluates the level of social support available to patients. Behavioral skills are evaluated using the SEAMS, focusing on patients’ self-efficacy in managing their medications correctly. Finally, medication-taking behaviors are assessed using the MMAS-8, which reflects patients’ adherence to prescribed regimens, combined with the PDC. The IMB model’s conceptual framework, as applied in this study, is illustrated in Figure 3.
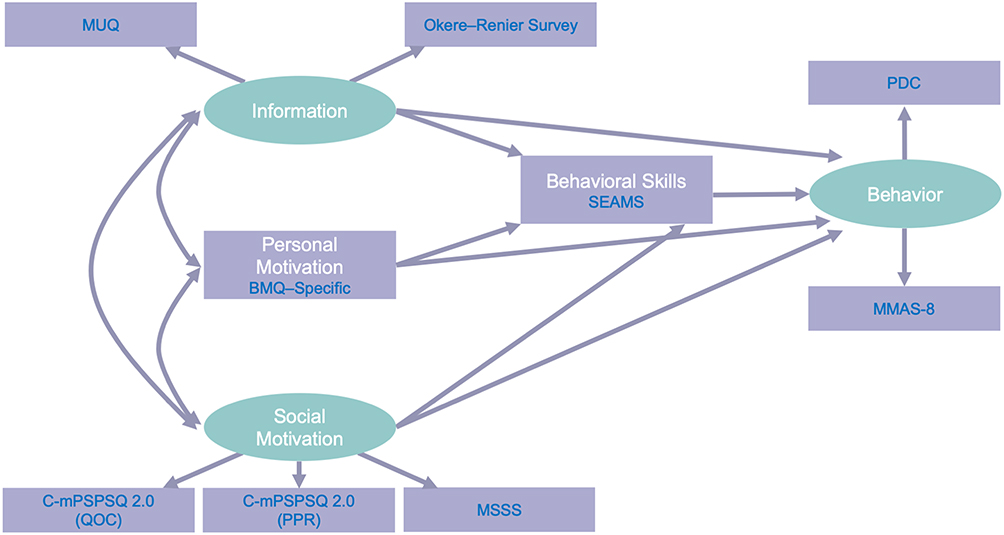 |
Figure 3 Proposed conceptual framework of the Information–Motivation–Behavioral Skills (IMB) model integrated with selected instruments. Ellipses represent latent variables conceptualized and measured through observed variables, while rectangles represent observed variables directly associated with a single instrument. The latent construct of information is measured using two tools: the Medication Understanding Questionnaire (MUQ) and the Okere–Renier Survey. Personal motivation and behavioral skills are represented as rectangles because each construct is measured using a single instrument—personal motivation via the Beliefs about Medicines Questionnaire–Specific (BMQ-Specific) and behavioral skills via the Self-Efficacy for Appropriate Medication Use Scale (SEAMS). Social motivation is measured using two instruments, the Traditional Chinese version of the modified Patient Satisfaction with Pharmacist Services 2.0 (C-mPSPSQ 2.0) (subscales for quality of care [QOC] and patient–pharmacist relationship [PPR]) and the Medication-Specific Social Support Questionnaire (MSSS). Finally, behavior is represented as an ellipse and assessed using the proportion of days covered (PDC) and the Eight-Item Morisky Medication Adherence Scale (MMAS-8). |
Sample Size
The required sample size was estimated based on the SEM framework, considering the model’s configuration. The model includes nine observed variables and 26 parameters for estimation, resulting in 19 degrees of freedom. Sample size determination was performed using root mean square error of approximation (RMSEA)-based calculations to achieve a statistical power of 0.80 and the significance level of α = 0.05 following the method proposed by MacCallum et al.58 RMSEA values were set to 0.05 for the null hypothesis (H0) and 0.10 for the alternative hypothesis (H1) to detect a meaningful difference in model fit. This analysis indicated the need for a minimum of 191 samples. A 10% adjustment was applied to account for potential attrition or incomplete responses,59 resulting in a final target sample size of 200 participants. This sample size meets the minimum requirement for modeling two trajectories (short-term and sustained responders) in LCGM.60
Statistical Analysis
Descriptive statistics will be conducted using Statistical Package for the Social Sciences version 30.0 and R version 4.3.2 to summarize baseline characteristics. Depending on data distribution, categorical variables will be presented as frequencies and percentages, while continuous variables will be presented as means and standard deviations or medians and interquartile ranges, as appropriate. Group comparisons will be performed for adherence trajectory subgroups identified through LCGM. Chi-square (χ2) tests will be employed for categorical variables, with Fisher’s exact test applied when expected cell counts are < 5. For continuous variables, independent t-tests or Mann–Whitney U-tests will be used, as appropriate. A two-sided p-value < 0.05 will be considered statistically significant.
SEM and LCGM will be conducted using Mplus 8.0 to analyze the IMB models, evaluate hypothesized structural relationships, assess overall model fit, and classify prespecified two-class adherence trajectories. To assess the robustness of this assumption, a sensitivity analysis will be conducted by fitting models with alternative class structures (e.g., one to four classes) and comparing their fit using the Akaike information criterion (AIC) and Bayesian information criterion (BIC). The results will be reported to inform future research involving larger sample sizes.
Two separate SEMs will be developed for pre- (Model 1) and post- (Model 2) intervention assessments to determine the structural relationships among latent variables. Following LCGM, additional SEMs will be conducted separately for short-term responders and sustained responders. Goodness-of-fit will be evaluated using multiple fit indices: the χ2 to degrees-of-freedom ratio (χ2/df), comparative fit index (CFI), Tucker–Lewis index (TLI), RMSEA with a 90% confidence interval, and standardized root mean square residual (SRMR).61 The maximum likelihood estimation method will be employed to estimate model parameters. Acceptable thresholds for model fit are defined as χ2/df < 5, CFI and TLI > 0.95, and RMSEA and SRMR < 0.08.62,63
After fitting each model, a multigroup SEM approach will be employed to compare structural changes between pre- and postintervention models and between short-term responders and sustained responders. Given the use of identical questionnaires, measurement invariance will be assumed. Path coefficients will first be constrained and then freely estimated to identify statistically significant differences. This approach enables an examination of how the intervention influences key pathways within the IMB model, particularly with regard to changes in path strength and direction. Additionally, path analysis will be conducted to assess direct, indirect, and total effects among latent variables. Missing data, if any, will be handled using the full information maximum likelihood approach, which is well-suited for SEM and LCGM analyses.
Dissemination
Once the study is completed, the results will be submitted for publication in an international peer-reviewed journal to dissemination the findings to the broader scientific community.
Study Status
As of May 19, 2025, the study protocol is at Version 1.1. Recruitment commenced in early May 2025 and is projected to conclude by September 2026.
Discussion
Nearly half of all patients with HF do not receive GDMT prescriptions or do not adhere to prescribed regimens,64,65 thus exacerbating their prognoses. Particularly in Taiwan, time-constrained clinical settings and the absence of robust support systems pose additional barriers.66 Pharmacists are therefore uniquely positioned to bridge this gap by providing essential education, supporting patients, and following up with them to improve medication adherence after clinician visits.7,22
Extensive evidence underscores that pharmacist-led interventions effectively enhance medication adherence for various diseases,67–69 including HF.22,27,32 However, the precise mechanisms underlying such improvements remain underexplored, limiting the ability to optimize current pharmacist-led models. Further investigation into these mechanisms and the optimization of pharmacist-led interventions is essential for refining current practices and enhancing the quality of pharmacist-provided care for patients with HF. Thus, our study aims to evaluate the impact and mechanisms of pharmacist-led patient education on medication adherence among patients with HF by employing the IMB model with PROMs in a longitudinal pretest–posttest framework. We seek to compare IMB model structures before and after the intervention to identify pathways with significant potential for enhancing medication adherence. A multigroup SEM approach will be employed to address this gap and enable a robust comparison of pre- and postintervention models, highlighting how pharmacist-led interventions affect medication adherence and provide insights into the pathways of influence. We hypothesize that patients with HF can significantly enhance medication adherence after pharmacist-led interventions. Additionally, this study incorporates LCGM to classify distinct adherence trajectory subgroups, identifying patients who may require more intensive interventions. Multigroup SEM and baseline characteristic analysis will be used to examine differences between short-term responders and sustained responders, determining key factors influencing long-term adherence to inform tailored strategies.
While the study is designed to be feasible and well-integrated into clinical practice, several anticipated challenges may arise. These have been proactively addressed through the proposed solutions. First, given the longitudinal nature of the study, which involves data collection across multiple time points, participant loss to follow-up represents a potential concern. Attrition could lead to a reduced sample size and diminished statistical power, thus affecting the stability and interpretability of the SEM and LCGM analyses. To mitigate this risk, an attrition buffer of at least 10% has been incorporated into the sample size estimation. Moreover, follow-up assessments will be scheduled to coincide with routine clinical visits to reduce participant burden. Reminder notifications will also be sent via a designated LINE communication group one week and one day before each scheduled follow-up; phone calls will be made if needed. As an incentive to improve retention, participants will receive a gift card valued at NT$100 upon completing each follow-up phase.
Another anticipated challenge involves the stability of the latent classes identified through LCGM, particularly in light of the projected sample size of approximately 200 participants. To address this, the study will prespecify a two-class solution based on theoretical assumptions, distinguishing short-term responders from sustained responders. Sensitivity analyses using AIC and BIC will be conducted to assess the robustness of the latent class solution. Any limitations regarding class stability due to sample size constraints will be transparently reported, and findings will be positioned as preliminary and exploratory, underscoring the need for future validation with larger cohorts.
Finally, recruiting a sufficient number of eligible participants solely through the pharmacist-led HF clinic alone may be difficult. To enhance recruitment, the study will also include patients enrolled in the NTUH Heart Failure Post-Acute Care (HF-PAC) program, which routinely refers patients to pharmacist-led education sessions. The HF-PAC program offers holistic, team-based care for hospitalized patients with HF in Taiwan,70 incorporating pharmacists to provide predischarge counseling, reinforce patients’ understanding of home-based care, strengthen self-care capabilities, and promote medication adherence. In addition, collaboration is ongoing with clinicians participating in NTUH’s pharmacist-led clinic referral program, which includes twelve cardiology outpatient clinics, therefore broadening the recruitment base. These proactive strategies are intended to ensure recruitment feasibility, uphold methodological rigor, and enhance the validity, robustness, and generalizability of the study’s findings through the inclusion of a more diverse participant population.
To our knowledge, no prior study has utilized the IMB model in conjunction with SEM and LCGM to evaluate pharmacist-led patient education among patients with HF, a predominantly geriatric population often challenged by polypharmacy and poor HRQoL. This research will serve as a foundation for advancing the APPLE-HF management program, expanding holistic care for patients with HF, and reshaping future adherence strategies to optimize pharmacist-led interventions.
Conclusion
This study will employ a longitudinal pretest–posttest design to evaluate the impact and underlying mechanisms of pharmacist-led patient education on medication adherence in individuals with HF. By integrating the IMB model with PROMs through SEM, the study will identify the pathways through which pharmacist-led interventions improve medication adherence. In addition, it seeks to refine pharmacist-led patient education by examining the interactions among information, motivation, behavioral skills, and adherence behavior. Tailored interventions will also be developed to support long-term medication adherence by classifying distinct adherence trajectories using LCGM. Consequently, this study is expected to empower pharmacists with evidence-based strategies to optimize their practice, enhance medication adherence among vulnerable patients with HF, enable more precise identification of individuals requiring targeted interventions, and reinforce pharmacists’ role as essential members of healthcare teams.
Abbreviations
ACC, American College of Cardiology; AHA, American Heart Association; AIC, Akaike information criterion; APPLE-HF, Advanced Patient-centered Pharmacist-Led Education on Heart Failure; BIC, Bayesian information criterion; BMQ-Specific, Beliefs About Medicines Questionnaire–Specific; C-mPSPSQ 2.0, Traditional Chinese version of the modified Patient Satisfaction with Pharmacist Services Questionnaire 2.0; CFI, comparative fit index; EHR, electronic health records; GDMT, guideline-directed medical therapy; HF, Heart failure; HF-PAC, Heart Failure Post-Acute Care; HFSA, Heart Failure Society of America; HFrEF, Heart failure with reduced ejection fraction; HRQoL, health-related quality of life; IMB, Information–Motivation–Behavioral Skills; LCGM, latent class growth modeling; MMAS-8, Eight-Item Morisky Medication Adherence Scale; MSSS, Medication-Specific Social Support Questionnaire; MUQ, Medication Understanding Questionnaire; NHI, National Health Insurance; NTUH, National Taiwan University Hospital; PDC, proportion of days covered; PPR, patient–pharmacist relationship; PROMs, patient-reported outcome measures; PSPSQ 2.0, Patient Satisfaction with Pharmacist Services Questionnaire 2.0; QOC, quality of care; RMSEA, root mean square error of approximation; SEAMS, Self-Efficacy for Appropriate Medication Use Scale; SEM, structural equation modeling; SRMR, standardized root mean square residual; TLI, Tucker–Lewis index.
Data Sharing Statement
Data supporting the findings of this study will be available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Research Ethics Committee of the National Taiwan University Hospital (No. 202501197RINC) granted approval for this study.
Consent for Publication
Patients will provide informed consent for their data to be published, and anonymity will be ensured by excluding any identifying information.
Acknowledgments
Shan-En Weng and Wan-Tseng Hsu are co-corresponding authors for this study.The authors would like to acknowledge in advance the invaluable contributions of all participants, as well as the anticipated support from the Department of Pharmacy and Department of Nursing at the National Taiwan University Hospital during the study.
Author Contributions
All authors made a significant contribution to the work reported, whether in study conception or design; took part in drafting, revising, or critically reviewing the article; approved the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is expected to be supported by National Taiwan University (Grant No. NTU-JP 113L7240) and Taipei City Hospital (Grant No. TPCH-114-20). The funding bodies will not have any role in the design of the study, data collection, analysis, interpretation of the results, or the preparation of this manuscript.
Disclosure
The authors report there are no competing interests to declare for this work.
References
1. Heo S, Moser DK, Lennie TA, Zambroski CH, Chung ML. A comparison of health-related quality of life between older adults with heart failure and healthy older adults. Heart Lung J Cardiopulm Acute Care. 2007;36(1):16–24. doi:10.1016/j.hrtlng.2006.06.003
2. Díez-Villanueva P, Alfonso F. Heart failure in the elderly. J Geriatr Cardiol. 2016;13(2):115–117. doi:10.11909/j.issn.1671-5411.2016.02.009
3. Martin SS, Aday AW, Almarzooq ZI, Anderson CA, Arora P, Avery CL. heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024;149(8):e347–913. doi:10.1161/CIR.0000000000001209
4. Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC, Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. 2023;118(17):3272–3287. doi:10.1093/cvr/cvac013
5. Wu J-R, Moser DK. Health-related quality of life is a mediator of the relationship between medication adherence and cardiac event-free survival in patients with heart failure. J Card Fail. 2021;27(8):848–856. doi:10.1016/j.cardfail.2021.03.004
6. Merlo M, Pivetta A, Pinamonti B, et al. Long‐term prognostic impact of therapeutic strategies in patients with idiopathic dilated cardiomyopathy: changing mortality over the last 30 years. Eur J Heart Fail. 2014;16(3):317–324. doi:10.1002/ejhf.16
7. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM. AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e895–e1032.
8. McMurray JJV, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004. doi:10.1056/NEJMoa1409077
9. van der Wal MHL, Jaarsma T. Adherence in heart failure in the elderly: problem and possible solutions. Int J Cardiol. 2008;125(2):203–208. doi:10.1016/j.ijcard.2007.10.011
10. Azad N, Lemay G. Management of chronic heart failure in the older population. J Geriatr Cardiol. 2014;11(4):329–337. doi:10.11909/j.issn.1671-5411.2014.04.008
11. Garred CH, Zahir D, Butt JH, et al. Adherence and discontinuation of optimal heart failure therapies according to age: a Danish nationwide study. J Am Heart Assoc. 2022;11(19):026187. doi:10.1161/JAHA.122.026187
12. Greene SJ, Tan X, Yeh YC, et al. Factors associated with non-use and sub-target dosing of medical therapy for heart failure with reduced ejection fraction. Heart Fail Rev. 2022;27(3):741–753. doi:10.1007/s10741-021-10077-x
13. Prokopidis K, Testa GD, Veronese N, et al. What is the association of polypharmacy with frailty in heart failure? A systematic review and meta-analysis. J Frailty Sarcopenia Falls. 2024;9(1):51–65. doi:10.22540/JFSF-09-051
14. Gorodeski EZ, Goyal P, Hummel SL, et al. Domain management approach to heart failure in the geriatric patient: present and future. J Am Coll Cardiol. 2018;71(17):1921–1936. doi:10.1016/j.jacc.2018.02.059
15. Wilder LV, Devleesschauwer B, Clays E, Pype P, Vandepitte S, De Smedt D. Polypharmacy and health-related quality of life/psychological distress among patients with chronic disease. Prev Chronic Dis. 2022;19:220062. doi:10.5888/pcd19.220062
16. Gathright EC, Dolansky MA, Gunstad J, et al. The impact of medication nonadherence on the relationship between mortality risk and depression in heart failure. Health Psychol. 2017;36(9):839–847. doi:10.1037/hea0000529
17. Verhestraeten C, Heggermont WA, Maris M. Clinical inertia in the treatment of heart failure: a major issue to tackle. Heart Fail Rev. 2021;26(6):1359–1370. doi:10.1007/s10741-020-09979-z
18. Ruppar TM, Cooper PS, Mehr DR, Delgado JM, Dunbar‐Jacob JM. Medication adherence interventions improve heart failure mortality and readmission rates: systematic review and meta‐analysis of controlled trials. J Am Heart Assoc. 2016;5(6):2606. doi:10.1161/JAHA.115.002606
19. Cleland J, Cohen-Solal A, Aguilar JC, et al. Management of heart failure in primary care (the IMPROVEMENT of Heart Failure Programme): an international survey. Lancet. 2002;360(9346):1631–1639. doi:10.1016/S0140-6736(02)11601-1
20. Komajda M, Hanon O, Hochadel M, et al. Contemporary management of octogenarians hospitalized for heart failure in Europe: euro Heart Failure Survey II. Eur Heart J. 2009;30(4):478–486. doi:10.1093/eurheartj/ehn539
21. Pulignano G, Del Sindaco D, Tavazzi L, et al. Clinical features and outcomes of elderly outpatients with heart failure followed up in hospital cardiology units: data from a large nationwide cardiology database (IN-CHF registry). Am Heart J. 2002;143(1):45–55. doi:10.1067/mhj.2002.119608
22. Koshman SL. Pharmacist Care of Patients With Heart Failure A Systematic Review of Randomized Trials. Arch Intern Med. 2008;168(7):687–694. doi:10.1001/archinte.168.7.687
23. Pearson GJ, Cooke C, Simmons WKT, Sketris I. Evaluation of the use of evidence-based angiotensin-converting enzyme inhibitor criteria for the treatment of congestive heart failure: opportunities for pharmacists to improve patient outcomes. J Clin Pharm Ther. 2001;26(5):351–361. doi:10.1046/j.1365-2710.2001.00364.x
24. Roblek T, Deticek A, Leskovar B, et al. Clinical-pharmacist intervention reduces clinically relevant drug-drug interactions in patients with heart failure: a randomized, double-blind, controlled trial. Int J Cardiol. 2016;203:647–652. doi:10.1016/j.ijcard.2015.10.206
25. Suzuki M, Matsue Y, Izumi S, et al. Pharmacist-led intervention in the multidisciplinary team approach optimizes heart failure medication. Heart Vessels. 2018;33(6):615–622. doi:10.1007/s00380-017-1099-8
26. Gattis WA, Hasselblad V, Whellan DJ, O’Connor CM. Reduction in heart failure events by the addition of a clinical pharmacist to the heart failure management team: results of the pharmacist in heart failure assessment recommendation and monitoring (PHARM) study. Arch Intern Med. 1999;159(16):1939–1945. doi:10.1001/archinte.159.16.1939
27. Schumacher PM, Becker N, Tsuyuki RT, et al. The evidence for pharmacist care in outpatients with heart failure: a systematic review and meta‐analysis. ESC Heart Fail. 2021;8(5):3566–3576. doi:10.1002/ehf2.13508
28. Davis EM, Packard KA, Jackevicius CA. The pharmacist role in predicting and improving medication adherence in heart failure patients. J Manag Care Pharm. 2014;20:741–755.
29. Martinez AS, Saef J, Paszczuk A, Bhatt-Chugani H. Implementation of a pharmacist-managed heart failure medication titration clinic. Am J Health Syst Pharm. 2013;70(12):1070–1076. doi:10.2146/ajhp120267
30. Murray MD, Young J, Hoke S, et al. Pharmacist Intervention to Improve Medication Adherence in Heart Failure. Ann Intern Med. 2007;146(10):714–725. doi:10.7326/0003-4819-146-10-200705150-00005
31. Nguyen HN, Nguyen CV, Nguyen DT, Le TD, Bui QTH. Impact of pharmacist-led interventions on heart failure medication adherence: a prospective cohort study. J Pharm Health Serv Res. 2023;14(2):205–211. doi:10.1093/jphsr/rmad008
32. Wang L, Zhao Y, Han L, et al. Pharmacist-led management model and medication adherence among patients with chronic heart failure. JAMA Netw Open. 2024;7(12):e2453976. doi:10.1001/jamanetworkopen.2024.53976
33. Fisher JD, Fisher WA. Changing AIDS-risk behavior. Psychol Bull. 1992;111(3):455–474. doi:10.1037/0033-2909.111.3.455
34. Fisher JD, Fisher WA, Misovich SJ, Kimble DL, Malloy TE. Changing AIDS risk behavior: effects of an intervention emphasizing AIDS risk reduction information, motivation, and behavioral skills in a college student population. Health Psychol. 1996;15(2):114–123. doi:10.1037/0278-6133.15.2.114
35. Chang SJ, Choi S, Kim S-A, Song M. Intervention strategies based on information-motivation-behavioral skills model for health behavior change: a systematic review. Asian Nurs Res. 2014;8(3):172–181. doi:10.1016/j.anr.2014.08.002
36. Rongkavilit C, Naar-King S, Kaljee LM, et al. Applying the information-motivation-behavioral skills model in medication adherence among Thai youth living with HIV: a qualitative study. AIDS Patient Care STDs. 2010;24(12):787–794. doi:10.1089/apc.2010.0069
37. Yang C, Lee DTF, Chair SY. Validation and adaption of an Information-Motivation-Behavioral Skills model of medication adherence in older patients with multimorbidity. Patient Educ Couns. 2023;113:107756. doi:10.1016/j.pec.2023.107756
38. Gu NY, Gai Y, Hay JW. The effect of patient satisfaction with pharmacist consultation on medication adherence: an instrumental variable approach. Pharm Pract. 2008;6:201–210.
39. Fisher JD, Fisher WA, Amico KR, Harman JJ. An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychol. 2006;25(4):462–473. doi:10.1037/0278-6133.25.4.462
40. Kim S-H, McDonald S, Kim S, Foster C, Fidler S. Importance of self-motivation and social support in medication adherence in HIV-infected adolescents in the United Kingdom and Ireland: a multicentre HYPNet study. AIDS Patient Care STDs. 2015;29(6):354–364. doi:10.1089/apc.2014.0335
41. Shahin W, Kennedy GA, Stupans I. The association between social support and medication adherence in patients with hypertension: a systematic review. Pharm Pract. 2021;19:2300.
42. Maddox TM, Januzzi JL, Allen LA, et al. ACC expert consensus decision pathway for treatment of heart failure with reduced ejection fraction. J Am Coll Cardiol. 2024;83(15):1444–1488. doi:10.1016/j.jacc.2023.12.024
43. Hsu W-T, Cheng -Y-Y, Yang T-Y, et al. The worsening renal perfusion index predicts the prognoses of heart failure patients treated with sacubitril/valsartan. Cardiorenal Med. 2023;13(1):310–323. doi:10.1159/000534095
44. Chien TCR, Chang Y-W, Weng S-E, Wu Y-J, Wang S-R, Hsu W-T. An interactive visualization dashboard for predicting the effect of sacubitril/valsartan initiation in patients with heart failure. Comput Biol Med. 2025;186:109667. doi:10.1016/j.compbiomed.2025.109667
45. Heidenreich P, Sandhu A. Advances in management of heart failure. BMJ. 2024;385:e077025. doi:10.1136/bmj-2023-077025
46. Marvanova M, Roumie CL, Eden SK, Cawthon C, Schnipper JL, Kripalani S. Health literacy and medication understanding among hospitalized adults. J Hosp Med. 2011;6(9):488–493. doi:10.1002/jhm.925
47. Okere AN, Renier CM, Morse J. Development and validation of a survey to assess patient-perceived medication knowledge and confidence in medication use. J Nurs Meas. 2014;22(1):120–134. doi:10.1891/1061-3749.22.1.120
48. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
49. Huang CL, Chiang C-H, Yang SC. eHealth literacy and beliefs about medicines among Taiwanese college students: cross-sectional study. JMIR Med Inform. 2021;9(11):e24144. doi:10.2196/24144
50. Sakharkar P, Bounthavong M, Hirsch JD, Morello CM, Chen TC, Law AV. Development and validation of PSPSQ. 2.0 measuring patient satisfaction with pharmacist services. Res Soc Adm Pharm. 2015;11(4):487–498. doi:10.1016/j.sapharm.2014.10.006
51. Chien TCR, Ko PH, Weng SE, et al. Patient satisfaction matters: translation, cross-cultural adaptation, and validation of the modified Patient Satisfaction with Pharmacist Services Questionnaire into Traditional Chinese (C-mPSPSQ 2.0) among patients with heart failure. Res Soc Adm Pharm. 2025;21(8):559–572. doi:10.1016/j.sapharm.2025.03.006
52. Lehavot K, Huh D, Walters KL, King KM, Andrasik MP, Simoni JM. Buffering effects of general and medication-specific social support on the association between substance use and HIV medication adherence. AIDS Patient Care STDs. 2011;25(3):181–189. doi:10.1089/apc.2010.0314
53. Chen P-T, Wang T-J. Translation and validation of the Taiwanese version of the self-efficacy for appropriate medication use scale. Open J Nurs. 2017;07(01):28–38. doi:10.4236/ojn.2017.71003
54. Risser J, Jacobson TA, Kripalani S. Development and psychometric evaluation of the self-efficacy for appropriate medication use scale (SEAMS) in low-literacy patients with chronic disease. J Nurs Meas. 2007;15(3):203–219. doi:10.1891/106137407783095757
55. Morisky DE, Ang A, Krousel‐Wood M, Ward HJ. Retracted: predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
56. Hess LM, Raebel MA, Conner DA, Malone DC. Measurement of adherence in pharmacy administrative databases: a proposal for standard definitions and preferred measures. Ann Pharmacother. 2006;40(7–8):1280–1288. doi:10.1345/aph.1H018
57. Baumgartner PC, Haynes RB, Hersberger KE, Arnet I. A systematic review of medication adherence thresholds dependent of clinical outcomes. Front Pharmacol. 2018;9:1290. doi:10.3389/fphar.2018.01290
58. MacCallum RC, Browne MW, Sugawara HM. Power analysis and determination of sample size for covariance structure modeling. Psychol Methods. 1996;1(2):130–149. doi:10.1037/1082-989X.1.2.130
59. Hoerger M. Participant dropout as a function of survey length in internet-mediated university studies: implications for study design and voluntary participation in psychological research. Cyberpsychology Behav Soc Netw. 2010;13(6):697–700. doi:10.1089/cyber.2009.0445
60. Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct Equ Model. 2007;14(4):535–569. doi:10.1080/10705510701575396
61. Hu L, Bentler PM. Fit indices in covariance structure modeling: sensitivity to underparameterized model misspecification. Psychol Methods. 1998;3(4):424–453. doi:10.1037/1082-989X.3.4.424
62. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model Multidiscip J. 1999;6(1):1–55. doi:10.1080/10705519909540118
63. McDonald RP, Ho M-HR. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002;7(1):64–82. doi:10.1037/1082-989X.7.1.64
64. Shahid I, Khan MS, Fonarow GC, Butler J, Greene SJ. Bridging gaps and optimizing implementation of guideline-directed medical therapy for heart failure. Prog Cardiovasc Dis. 2024;82:61–69. doi:10.1016/j.pcad.2024.01.008
65. Huang W, Ahmed MM, Morris EJ, et al. Trajectories of sacubitril/valsartan adherence among medicare beneficiaries with heart failure. JACC: Adv. 2024;3(7):100958. doi:10.1016/j.jacadv.2024.100958
66. Wu T-Y, Majeed A, Kuo KN. An overview of the healthcare system in Taiwan. Lond J Prim Care. 2010;3(2):115–119. doi:10.1080/17571472.2010.11493315
67. Marcum Z, Jiang S, Bacci J, Ruppar T. Pharmacist-led interventions to improve medication adherence in older adults: a meta-analysis. J Am Geriatr Soc. 2021;69(11):3301–3311. doi:10.1111/jgs.17373
68. Mes MA, Katzer CB, Chan AHY, Wileman V, Taylor SJC, Horne R. Pharmacists and medication adherence in asthma: a systematic review and meta-analysis. Eur Respir J. 2018;52(2):1800485. doi:10.1183/13993003.00485-2018
69. Presley B, Groot W, Pavlova M. Pharmacy-led interventions to improve medication adherence among adults with diabetes: a systematic review and meta-analysis. Res Soc Adm Pharm. 2019;15(9):1057–1067. doi:10.1016/j.sapharm.2018.09.021
70. Wang CH, Kao FY, Tsai SL, Lee CM. Policy-driven post-acute care program lowers mortality rate and medical expenditures after hospitalization for acute heart failure: A nationwide propensity score-matched study. J Am Med Dir Assoc. 2023;24(7):978–984.e4. doi: 10.1016/j.jamda.2023.03.031.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.