")
Back to Journals » Clinical Ophthalmology » Volume 19
Incidence and Factors Related to Double Anterior Chamber Complications After Deep Anterior Lamellar Keratoplasty
Authors Huang J, Asano K , Uchio E
Received 11 December 2024
Accepted for publication 9 March 2025
Published 20 March 2025 Volume 2025:19 Pages 985—991
DOI https://doi.org/10.2147/OPTH.S508993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr John Miller
Jane Huang, Kohei Asano, Eiichi Uchio
Department of Ophthalmology, Fukuoka University School of Medicine, Fukuoka, Japan
Correspondence: Eiichi Uchio, Department of Ophthalmology, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku, Fukuoka, 814-0180, Japan, Tel +81 92 801 1011, Fax +81 92 865 4445, Email [email protected]
Background: Deep anterior lamellar keratoplasty (DALK) has safety advantages over penetrating keratoplasty. However, one of the serious complications of DALK is Descemet membrane (DM) detachment, which can lead to double anterior chamber (DAC) and visual impairment. This study examines the incidence and factors related to the complication of DAC after DALK, including preexisting conditions such as atopic dermatitis (AD).
Methods: This is a retrospective evaluation of all patients who underwent DALK from January 2019 to April 2024 in the Department of Ophthalmology, Fukuoka University Hospital. Cases with DAC postoperatively were analyzed statistically. A total of 85 eyes in 73 patients were included. We excluded eyes with preexisting corneal perforations that required grafts that were less than 6mm in diameter. A binomial logistic predictive model was used to determine factors associated with postoperative DAC. Collated variables were age, AD, preexisting corneal diseases, donor button size, intraoperative DM perforation, and cornea supply source.
Results: Among 85 eyes that underwent DALK, 12 eyes (14.1%) developed postoperative DAC. Binomial regression analysis revealed preexisting corneal diseases (p=0.031) including preoperative DM perforation, infectious keratitis, keratoconus, corneal dystrophy, and corneal scar, intra-operative DM perforation (p=0.049), and AD (p=0.031) to be significant factors associated with DAC. This binomial regression model had 83.3% sensitivity and 78.0% specificity.
Conclusion: AD and preexisting corneal diseases were significant factors in DAC after DALK, and DALK during active infection predisposes to DAC, while intraoperative perforation was also significantly associated. Our study suggests that these factors could be of importance in considering the mechanism of pathogenesis of DM and DAC.
Keywords: deep anterior lamellar keratoplasty, double anterior chamber, Descemet membrane, atopic dermatitis, binomial regression model
Introduction
Deep anterior lamellar keratoplasty (DALK) is an advanced corneal surgical procedure using air-injection or other methods to separate the corneal stroma from the Descemet membrane (DM).1 Compared with penetrating keratoplasty (PK), DALK avoids complications associated with open-globe surgery, has a lower rate of graft rejection, and results in a better visual outcome.2 DALK is technically more challenging than PK, particularly in the step of exposing the DM. The stroma can be separated from the DM and endothelium through manual stromal dissection or injection of air, saline, or viscoelastic material just anterior to the DM. We used the Anwar big bubble air injection approach, which is currently the most widely used technique.3 The indication for DALK is conditions where the corneal stroma is affected, primarily by scarring, dystrophy or ectasia, but the DM and endothelium are normal. Since the host DM and endothelium are retained and the affected stroma and epithelium are replaced, DALK eliminates the risk of immune-mediated endothelial rejection and consequent graft failure.4 However, complications related to sutures, induced astigmatism, folds within DM, DM perforation, pseudo-anterior chamber formation, interface keratitis, and weak graft-host junction remain.5,6
Despite the safety benefits of DALK over PK, one of its serious complications is DM detachment, which can lead to double anterior chamber (DAC) and visual impairment.7 There are reports on the incidence, risk factors, and management of intraoperative DM perforations and early complications after DALK.8 A PubMed search of the English literature showed limited reports on the incidence and statistical analysis of factors associated with post-DALK DAC. Therefore, our study aimed to identify pre- and perioperative risk factors for DAC. This could provide valuable information for prognostication for post-DALK DAC eyes. Our study also suggests the importance of considering the mechanism of pathogenesis of DAC.
Materials and Methods
Patients
This study received approval from the Institutional Review Board of Fukuoka University School of Medicine (approval number: 11-9-07) and complied with the principles in the Declaration of Helsinki. Written informed consent was obtained from all subjects enrolled in this study prior to study commencement. We reviewed all consecutive eyes that underwent DALK from January 2019 to April 2024 at Fukuoka University Hospital. A total of 85 eyes in 73 patients were retrospectively evaluated for complications of DAC after DALK. The indications for DALK in our study were therapeutic DALK for infectious keratitis and optical DALK for: a) DM microperforation, b) keratoconus, c) corneal dystrophy, and d) corneal scar. Table 1 shows the demographic data and indications for DALK in our study. The clinical outcome predictors for statistical analysis were age, concomitant atopic dermatitis (AD), preexisting corneal diseases, donor button size, intra-operative DM perforation, and donor cornea supply.
 |
Table 1 Demographic Characteristics of Patients |
Surgical Techniques
All surgery was conducted by a single surgeon under general anesthesia. Patients with active infectious keratitis were treated with antimicrobial or antiviral agents until the infection became quiescent, provided that the endothelium remained intact. Preexisting macro- or micro-perforated eyes with DALK with donor corneal diameter less than 6 mm (tectonic patches) were excluded in our study. The recipient cornea was marked and partially cut using a hand-held trephine 0.5 mm larger than the pathological corneal lesion. A corneal incision was made at the edge of the trephination with a 15° blade followed by corneal stromal layer-by-layer dissection to approximately two-thirds of the outer cornea or to the pre-DM level using a dissector blade (golf knife). Following stromal dissection, a 27G blunt needle attached to an air-filled 5-mL cannula was placed as deep as possible between the pre-DM and DM layers to create a large bubble (BB) for the cleavage plane, according to the modified Anwar’s BB technique.3 If the BB failed, the remaining stromal tissue was then carefully excised by freehand manual dissection with either a crescent blade or a golf knife until complete removal of the pathological stroma was achieved, leaving approximately 150–200 µm of residual stroma. DALK procedure was continued in eyes with intra-operative corneal microperforation when the integrity of the anterior chamber was maintainable. Donor corneal tissue from the Japanese domestic eye bank, Eye Bank Association of America, or frozen corneal tissue was used. The donor corneal tissue was oversized by 0.50 mm and the donor graft was denuded of its Descemet’s endothelial layer using forceps and scissors, and then placed over the host cornea followed by 16 running bites of 10-0 nylon suture. Air was injected into the anterior chamber at the end of the procedure in those eyes with intra-operative DM perforations. All patients underwent either biomicroscopic slit lamp and/or anterior segment optical coherence tomography (AS-OCT, NIDEK) examinations for evaluation of DAC on day one and two post-DALK.
Statistics
All statistical evaluations were conducted using Excel Toukei-Kaiseki software (BellCurve, Tokyo, Japan). Univariate and multivariate analysis were conducted on the following explanatory variables: age, AD, preexisting corneal diseases, donor button size, intra-operative DM perforation, and donor cornea supply. Considering the clinical situation, these six explanatory variables had no dependency on each other. For univariate analysis, we performed chi-squared test and Mann–Whitney U-tests. Independent test for multiple comparisons was conducted for preexisting corneal disease categories: preoperative DM perforation, infectious keratitis, keratoconus, corneal dystrophy, and corneal scar, and donor cornea supply. We also conducted binomial logistic regression analysis to determine the most reliable clinical predictors of DAC outcome. Akaike’s information criterion (AIC) was employed to assess the reliability of the binomial logistic predictive model. The area under the curve (AUC) with receiver operating characteristic (ROC) was used to evaluate the predictability of the analysis. A p value of < 0.05 was considered statistically significant.
Results
Patient Characteristics
Baseline preoperative demographic characteristics of 85 eyes in 75 patients are shown in Table 1. There were 36 male eyes and 49 female eyes, and age ranged from 18 to 96 years (median = 61.0 years). Donor button size ranged from 6.75 mm to 9.50 mm (mean = 7.99 ± 0.59). Infectious keratitis treated with therapeutic DALK included fungal keratitis: 9 (10.6%), herpes keratitis: 4 (4.7%), bacterial keratitis: 3 (3.5%), and amoebic keratitis: 2 (2.4%), fungal keratitis being the most frequent preoperative keratitis in our study. Optical DALK cases included keratoconus: 18 (21.2%), corneal dystrophy: 18 (21.2%), microperforation that required a graft equal or more than 6 mm in diameter: 8 (9.4%), and corneal scar: 23 (27.1%).
Characteristics and comparisons of DALK are grouped and listed for all eyes, in those with and without DAC postoperatively in Table 2. Post-DALK DAC occurred in 12 eyes (14.1%). Types of BB in post-DALK cases were Type 1: 4 (33.3%), Type 2: 3 (25%), and Type 3: 5 (41.7%), and those in cases without DAC were Type 1: 22 (30.1%), Type 2: 20 (27.4%), and Type 3: 31 (42.5%). The median age of patients with DAC was 66.0 years, which was older than the median age of 61.0 years in the group without DAC. The average donor button size in the DAC group was 8.18 ± 0.55 mm compared to 7.95 ± 0.59 mm in the group without DAC. Despite these higher percentages, our binomial logistic analysis revealed that age and donor button size were not significant factors in DAC (Table 3).
 |
Table 2 Characteristics and Comparisons of Patients with and without DAC Post-DALK |
 |
Table 3 Binomial Logistic Regression of DAC |
Eyes with DAC included more therapeutic indications and fewer optical indications compared to eyes without DAC. In the group with DAC, concomitant AD (16.7%) and preexisting corneal diseases such as preoperative DM perforation (16.7%) and infectious keratitis (58.3%) were notably higher. The intra-operative complication of DM perforation also showed a higher percentage in the DAC group (33.3%). All cases of DAC in this present study resolved either after injection of air into the anterior chamber or spontaneously without further requirement for keratoplasty. Significant endothelial loss was not observed in either group, and no case with endothelial decompensation was observed.
Binomial Logistic Regression for DAC and Non-DAC Groups
Binomial logistic regression was used to identify independent clinical outcome predictors of post-DALK DAC. The full results of binomial logistic regression of factors associated with DAC are shown in Table 3. The regression revealed that preexisting corneal disease (p=0.031), intra-operative DM perforation (p=0.049), and concomitant AD (p=0.031) were significant factors associated with DAC, while donor cornea supply, donor button size and age were not significant in our study. This binomial logistic predictive model identified predictors of DAC with AIC of 61.3. The model demonstrated 83.3% sensitivity and 78.0% specificity, as indicated by the ROC curve, suggesting predictors of DAC (Figure 1). Furthermore, univariate analysis showed that the prevalence of DAC in cases with preexisting corneal diseases was significantly different, showing a tendency for intra-operative corneal perforation and infectious keratitis to be associated with DAC.
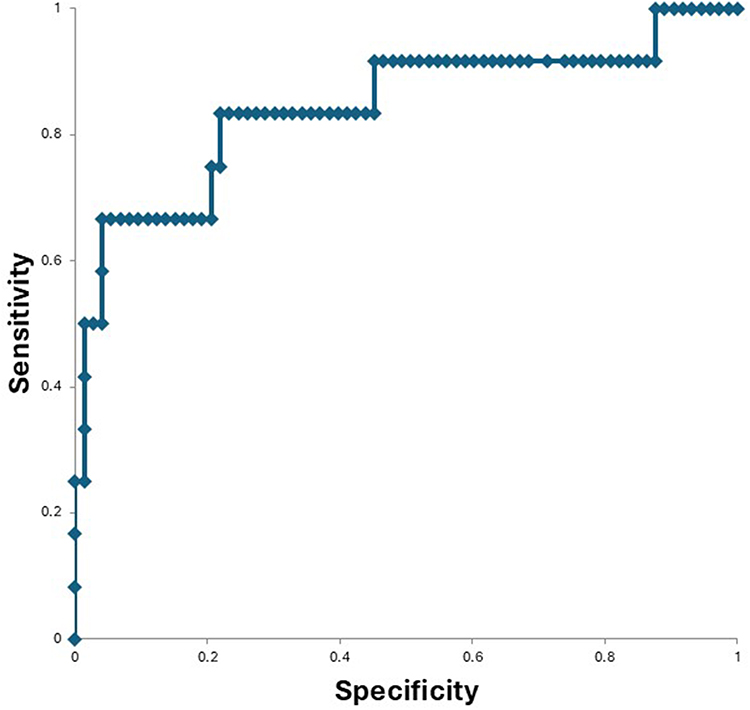 |
Figure 1 Performance of binomial logistic predictive model. ROC (receiver operating characteristic) curve of the predictive model is displayed. |
Discussion
Our results showed an incidence of DAC in 12 out of 85 eyes (14.1%), which is compatible with the reported incidence of about 10% after DALK.9 However, to our knowledge, no studies have addressed the clinical or pathological backgrounds contributing to post-DALK DAC. Our findings suggest that intra-operative DM perforation (p=0.049), preexisting corneal disease (p=0.031), and concomitant AD (p=0.031) are significantly associated with post-DALK DAC. We included age, donor button size, and donor cornea supply as demographics for our analysis for the following reasons: a) Age has been noted to influence the thickness of the zone between the last row of keratocytes and the anterior margin of the DM, potentially affecting the host-donor interface.4 b) Cornea supply might be a factor influencing the quality of the donor cornea due to possible tissue damage upon handling and shipping that could cause some degree of “elastin-fatigue”, resulting in fragile host-donor interface adherence. Ethnic factors might also have some influence on the surgical outcome.4 c) Donor button size could influence corneal misalignment or suture-related complications.9 However, our study showed that age, donor cornea supply, and donor button size were not significant factors associated with DAC (Table 3). It has been reported that survival analysis showed no significant difference in the cumulative risk of endothelial rejection between race-matched and race-mismatched recipients.10
Detachment of the endothelium-Descemet complex, leading to DAC, is a rare but serious complication of DALK, typically caused by the presence of macro- or micro-tears in the DM.8,11 Our study included 8 out of 85 eyes (9.1%) with preoperative perforated DM, which was manageable with the DALK procedure upon injection of air into the anterior chamber at the end of the procedure. Preoperative perforated DM was shown to be a clinical outcome predictor in our analysis. The overall significance of preexisting corneal disease was p = 0.031 (Table 3). Preoperative perforated DM showed a tendency to be associated with DAC according to our statistical analysis based on the observed distributions of preexisting corneal diseases.
On the other hand, our statistical analysis revealed that intra-operative DM perforation (p = 0.049) is a significant factor in DAC (Table 3). Six out of 85 eyes (7.1%) had intra-operative DM perforation and among these eyes, 4 out of 6 eyes (66.7%) resulted in DAC in our study (Table 2). Several studies have indicated that intra-operative DM perforation rates ranged from 4% to 39.2%, with a higher risk observed in cases with corneal scarring close to the DM.8,11 Our cases of intra-operative DM perforation occurred during repeated manual stromal excision and mostly in eyes with preexisting infectious keratitis (5/6 eyes). In eyes with DAC (n=12), infectious keratitis; microbial and herpetic keratitis, accounted for 7 out of 12 eyes (58.3%), indicating the underlying corneal pathological condition to be a risk for DAC. There are limited studies documenting the incidence and statistical analysis of DAC in similar cases to adequately assess the outcome. However, the incidence of DM perforation in infectious keratitis has been reported to be 41.7% in microbial keratitis and 54.3% in herpetic keratitis.8,12 The exact pathogenesis of corneal scarring and vascularization remain unclear. Similar to infections, the production of inflammatory cytokines and chemokines triggers coordinated phenotypic changes, extracellular matrix deposition and remodeling, ultimately leading to tissue repair as observed in corneal scarring.13 Possible explanations for the propensity for intra-operational DM perforation could be the difficulty of direct baring of the DM in infectious keratitis due to the pathological fragility of the DM or scarring around stromal keratocytes close to the DM.4 Prolonged microbial infection and possibly side effects of extensive medical treatment resulting in corneal cellular toxicity could add to the explanation for the fragility of the recipient cornea.13 The preDM layer is naturally quite elastic; however, when it becomes fibrosed, it loses its elasticity.4 As a result, incomplete Type 1 or Type 2 BB formation intraoperatively resulted in a mixed BB of Type 3 in these cases, which could have led to uneven distribution of air either between the posterior stroma and PDL (pre-Descemet layer)/DL (Dua’s layer) between PDL/DL and DM, causing difficulties in separating the layers uniformly.4 Often, these eyes demand highly skilled layer-by-layer manual dissection techniques which could otherwise increase the risk of intra-operative DM perforation.12 Postoperative DM detachment is known to occur up to three times more frequently in eyes complicated with intraoperative DM perforation compared to those without.8
In our study, concomitant AD was another significant factor in DAC (p=0.031) (Table 3). Two out of 12 eyes (16.7%) with DAC had AD (Table 2). Although the pathophysiologic connection is unclear, reports have shown systemic diseases such as ocular allergy, AD, connective tissue disorders, and Down syndrome to be related to the development of keratoconus and corneal ectasia.14 In patients with AD, the incidence of keratoconus ranged from 0.5% to 39%.15 Atopy is associated with pathology of the cornea because pruritis leads to eye rubbing, which causes mechanical “wear” of the cornea and progressive ectasia and keratoconus. Potential mechanisms include high corneal temperature, release of inflammatory mediators in the tear film, increased enzyme activity, elevated intraocular and hydrostatic tissue pressure, changes in keratocytes, decreased corneal strength, and loss of ground substance viscosity or its temporary displacement from the corneal apex.15 Our study included 18 eyes with keratoconus, with only one eye (8.33%) complicated with DAC compared to 17 eyes (15.1%) without DAC. Although the incidence of keratoconus with concomitant AD resulting in DAC was low in our study, this eye highlighted the significance of understanding the pathophysiology of keratoconus in AD patients. The aforementioned facts lead to our hypothesis on the pathophysiological characteristics of AD, which may have contributed to collagenous weakening of the cornea, pertaining to DM detachment and DAC in our cases.
A limitation of our study is the lack of preoperative measurement of endothelial cell density (ECD) because of advanced corneal scarring. Other limitations include lack of study of the clinical course of DAC, graft survival rates in those with and without DAC, and determining the rate of endothelial decompensation post-DAC. The strengths of our study lie in its inclusion of all consecutive cases undergoing DALK over a 5-year period by a single surgeon, as well as the relatively large number of DALK eyes from a single institution, which is notable compared to the available literature.
In conclusion, our binomial regression analysis showed intra-operative DM perforation, preexisting corneal disease, particularly preoperative DM perforation and infectious keratitis, and AD to be significant factors associated with post-DALK DAC. The binomial regression model based on dependent explanatory variables demonstrated high sensitivity and specificity. Recognition of these significant clinical factors associated with DAC prior to DALK in this observational case series could help improve our understanding of the clinical characteristics and behavior of various backgrounds, which could aid in early diagnosis and targeted interventions for high-risk populations as well as future prognostics in DALK treatment strategies.
Acknowledgments
This work was supported by a Grant-in-Aid for Encouragement of Scientists (24K12755) from the Ministry of Education, Science, Sports, and Culture of Japan. We thank Dr W. Gray for editing this manuscript.
Funding
The authors have no relevant financial or non-financial interests to disclose.
Disclosure
The authors declare that they have no conflict of interest related to this work.
References
1. Melles GR, Lander F, Rietveld FJ, et al. A new surgical technique for deep stromal, anterior lamellar keratoplasty. B J Ophthalmol. 1999;83:53–59.
2. MacIntyre R, Chow SP, Chan E, et al. Long-term outcomes of deep anterior lamellar keratoplasty versus penetrating keratoplasty in Australian keratoconus patients. Cornea. 2014;33:6–9. doi:10.1097/ICO.0b013e3182a9fbfd
3. Anwar M, Teichmann KD. Big-bubble technique to bare Descemet’s membrane in anterior lamellar keratoplasty. J Cataract Refract Surg. 2002;28(3):398–403. doi:10.1016/S0886-3350(01)01181-6
4. Dua HS, Sinha R, D’Souza S, et al. Descemet membrane detachment: a novel concept in diagnosis and classification. Am J Ophthalmol. 2020;218:84–98. doi:10.1016/j.ajo.2020.05.038
5. Zarei-Ghanavati S, Zarei-Ghanavati M, Sheibani S. Traumatic wound dehiscence after deep anterior lamellar keratoplasty: protective role of intact Descemet membrane after big-bubble technique. Cornea. 2010;29:220–221. doi:10.1097/ICO.0b013e3181a2a7cf
6. Karimian F, Feizi S. Deep anterior lamellar keratoplasty: indications, surgical techniques and complications. Middle East Afr J Ophthalmol. 2010;17(1):28–37. doi:10.4103/0974-9233.61214
7. Dua HS, Freitas R, Mohammed I, et al. The pre-Descemet’s layer (Dua’s layer, also known as the Dua-Fine layer and the pre-posterior limiting lamina layer): discovery, characterization, clinical and surgical applications, and the controversy. Prog Retin Eye Res. 2023;97:1–35. doi:10.1016/j.preteyeres.2022.101161
8. Huang OS, Htoon HM, Chan AM, et al. Incidence and outcomes of intraoperative Descemet membrane perforations during deep anterior lamellar keratoplasty. Am J Ophthalmol. 2019;199:9–18. doi:10.1016/j.ajo.2018.10.026
9. Romano D, Aiello F, Parekh M, et al. Incidence and management of early postoperative complications in lamellar corneal transplantation. Graefe’s Arch Clin Exp Ophthalmol. 2023;261:3097–3111. doi:10.1007/s00417-023-06073-6
10. Musch DC, Meyer RF, Sugar A, Soong HK. A study of race matching between donor and recipient in corneal transplantation. Am J Ophthalmol. 1988;105(6):646–650. doi:10.1016/0002-9394(88)90058-X
11. Passani A, Sframeli AT, Loiudice P, et al. Late spontaneous resolution of a double anterior chamber post deep anterior lamellar keratoplasty. Saudi J Ophthalmol. 2017;31:58–60. doi:10.1016/j.sjopt.2017.01.003
12. Nguyen HT, Pham ND, Mai TQ, et al. Tectonic deep anterior lamellar keratoplasty to treat corneal perforation and descemetocele from microbial keratitis. Clin Ophthalmol. 2021;15:3549–3555. doi:10.2147/OPTH.S324390
13. Tsatsos M, MacGregor C, Athanasiadis I, et al. Herpes simplex virus keratitis: an update of the pathogenesis and current treatment with oral and topical antiviral agents. Clin Exp Ophthalmol. 2016;44:824–837. doi:10.1111/ceo.12785
14. Woodward M, Blachley T, Stein J. The association between sociodemographic factors, common systemic diseases, and keratoconus: and analysis of a nationwide healthcare claims database. Ophthalmology. 2016;123(3):457–465. doi:10.1016/j.ophtha.2015.10.035
15. Pietruszynska M, Zawadzka-Krajewska A, Duda P, et al. Ophthalmic manifestations of atopic dermatitis. Adv Dermatol Allergol. 2020;37:174–179. doi:10.5114/ada.2018.79445
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.