")
Back to Journals » Journal of Inflammation Research » Volume 17
Increased Intestinal Inflammation and Permeability in Glaucoma
Authors Wang Z, Guo S, He C, Chen L, Wang J, Xiu W, Zhang G, Chen Y, Li A, Zhu X, Xiao X, Yu L , Lu F
Received 1 August 2024
Accepted for publication 24 September 2024
Published 30 September 2024 Volume 2024:17 Pages 6895—6904
DOI https://doi.org/10.2147/JIR.S480809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Zuo Wang,1,2,* Siqi Guo,3,* Chong He,2,4,* Lingling Chen,5 Jinxia Wang,2 Wenbo Xiu,2 Gao Zhang,2 Yang Chen,2 An Li,2 Xiong Zhu,6 Xiao Xiao,2 Ling Yu,3 Fang Lu2,4,7
1Department of Clinical Laboratory, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, Affiliated Cancer Hospital of University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 2Clinical Immunology Translational Medicine Key Laboratory of Sichuan Province, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 3Department of Ophthalmology, Daping Hospital, Army Medical Center, Army Medical University, Chongqing, People’s Republic of China; 4Medico-Engineering Cooperation on Applied Medicine Research Center, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 5Department of Immunology, West China School of Basic Medical Sciences & Forensic Medicine, Sichuan University, Chengdu, People’s Republic of China; 6Department of Prenatal Diagnosis, Chengdu Women’s and Children’s Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 7Health Management Center, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Yu; Fang Lu, Email [email protected]; [email protected]
Objective: Evidence suggests that dysbiosis of the gut microbiota plays a pivotal role in the development of glaucoma. This dysbiosis is commonly associated with chronic intestinal inflammation and increased intestinal permeability. However, the understanding of intestinal inflammation and permeability in glaucoma remains insufficient. This study aims to investigate the potential relationship between fecal inflammation and permeability markers and glaucoma.
Methods: We recruited 114 glaucoma patients and 75 healthy controls. Levels of fecal lactoferrin (Lf) and alpha-1 antitrypsin (AAT) were quantified using enzyme linked immunosorbent assay (ELISA) to compare both biomarkers between groups and across different severity grades of glaucoma. Logistic regression analysis was used to assess the association between these fecal biomarkers and glaucoma. The severity of glaucoma was assessed based on the mean deviation (MD) in the visual field.
Results: In this study, we observed elevated levels of fecal Lf and AAT in glaucoma patients. The proportion of glaucoma patients with abnormal fecal Lf levels (≥ 7.25 μg/g) was significantly higher than that of the controls (p = 0.012). A positive correlation was noted between fecal Lf and AAT (rho = 0.20, p = 0.006). After adjusting for age and sex, multivariable logistic regression analysis indicated that both fecal Lf (OR = 1.11, 95% CI: 1.01– 1.21, p = 0.026) and AAT (OR = 1.01, 95% CI: 1.01– 1.02, p < 0.001) positively correlated with glaucoma. These biomarkers might reflect glaucoma severity, with significant differences in fecal Lf levels observed between moderate and severe stages, but not in the early stage. Furthermore, increasing levels of fecal AAT correlated with greater severity of glaucomatous injury and a larger vertical cup-to-disc ratio (VCDR) (p < 0.05).
Conclusion: This study suggests an increase in intestinal inflammation and permeability in glaucoma, further indicating the importance of the ‘gut-retina axis’ in the pathogenesis of the disease and potentially offering new therapeutic avenues.
Keywords: fecal lactoferrin, fecal alpha-1 antitrypsin, glaucoma, intestinal inflammation, intestinal permeability, intestinal barrier
Introduction
Glaucoma, the second leading cause of blindness worldwide, currently affects approximately 80 million people globally.1 This complex neurodegenerative condition is primarily characterized by the degeneration of the optic nerve, reduction of retinal ganglion cells (RGCs), and visual field defects.1,2 Although elevated intraocular pressure (IOP) is traditionally viewed as a principal contributor to glaucomatous damage, some patients exhibit normal IOP levels.2 Recent studies have suggested that alterations of the gut environment may be implicated in glaucoma.3–5 Specifically, some research has demonstrated alterations in the gut microbiome of patients with this condition.3–5 Mouse model experiments show that germ-free mice are resistant to glaucomatous neural damage, underscoring the essential role of intestinal flora in the disease’s etiology.6 Additionally, our previous research indicates that gut-licensed β7+ CD4+ T cells and MAdCAM-1 contribute to RGC degeneration, highlighting the importance of the “gut-retina” axis in the development of glaucoma.7
Gut-microbiota dysbiosis is commonly associated with chronic intestinal inflammation and increased intestinal permeability.8,9 In previous studies, we have suggested a potential link between glaucoma and intestinal inflammation, as indicated by the inflammation marker fecal calprotectin.10 However, more evidence is required to substantiate these findings, and the identification of additional non-invasive fecal markers is necessary to confirm the presence of intestinal inflammation in glaucoma patients beyond this single marker.10 Additionally, inflammation is a primary cause of increased intestinal permeability and is considered pivotal in the pathophysiology of inflammatory bowel disease (IBD).11 The relationships may suggest a potential role for intestinal permeability in the pathogenesis of glaucoma.9 To date, as far as we know, no studies have directly investigated changes in intestinal permeability in patients with glaucoma.
Fecal lactoferrin (Lf), a non-invasive biomarker for detecting gut inflammation and predicting endoscopically active disease in the colon.12 Alpha-1 antitrypsin (AAT), a protease inhibitor, reflects loss of proteins to the intestinal lumen, serving as a biomarker for intestinal permeability.13 Fecal Lf and AAT are established markers widely used to assess intestinal inflammation and permeability in various diseases, such as inflammatory bowel disease (IBD) and Parkinson’s disease (PD).12–15 Moreover, our previous study demonstrated that plasma levels of Lf and AAT were elevated and correlated with the severity of glaucoma.16,17 However, since plasma is derived from peripheral blood circulation, it primarily reflects systemic inflammation and may not directly indicate local intestinal inflammation.18 In contrast, fecal samples, directly sourced from the gastrointestinal tract, offer a more accurate reflection of gastrointestinal conditions.19 In this study, we try to use fecal Lf and AAT to investigate changes of intestinal inflammation and permeability in patients with glaucoma.
Materials and Methods
Subjects
The study was conducted in adherence to the Declaration of Helsinki and received approval from the Institutional Review Board for Clinical Research of Sichuan Provincial People’s Hospital (No. 201968) and Daping Hospital (No. 202192). We enrolled 114 patients and 75 healthy controls from the two hospitals. All participants were informed about the study details and provided written informed consent. As previously reported,7 glaucoma was diagnosed by ophthalmologists based on comprehensive eye examinations, typically identifying characteristic optic nerve damage and associated visual field loss. Some glaucoma patients use between one and five different types of antiglaucoma eye drops, such as travoprost, carteolol, brimonidine, or brinzolamide. Inclusion criteria required participants to be free from antibiotics, probiotics, or prebiotics for the past three months and to have no history of acute or chronic gastrointestinal disorders (like irritable bowel syndrome, celiac disease, IBD), gastrointestinal surgery, malignant tumors, or other neurodegenerative diseases such as Parkinson’s disease.
Healthy controls exhibited no clinical signs of glaucoma or a family history of the disease. Exclusion criteria included a history of ocular surgery, ocular trauma, malignant tumors, recent surgery, gastrointestinal tract diseases (like irritable bowel syndrome, celiac disease, IBD), neurodegenerative diseases, and recent use of antibiotics, probiotics, or prebiotics. The inclusion and exclusion criteria for healthy controls were designed to ensure matching by gender and age.
Collection and Testing of Fecal Samples
Subjects were provided with sterile containers to collect fecal samples (5–10 g) at the hospital. The samples were immediately frozen at −80°C upon receipt at the laboratory. Fecal levels of Lf and AAT were quantified using an enzyme-linked immunosorbent assay (ELISA) with commercially available Lactoferrin ELISA kits (Catalogue No: EH0396, Fine Test, Wuhan, China), alpha-1 antitrypsin ELISA kits (Catalogue No: E-EL-H0965, Elabscience, Wuhan, China), following the manufacturer’s instructions.
Determination of Glaucoma Severity
Glaucoma severity was categorized based on the mean deviation (MD) values derived from visual field assessments. Specifically, an MD greater than −6 dB indicated early-stage glaucoma, an MD ranging from −12 dB to −6 dB was indicative of moderate-stage glaucoma, and an MD of −12 dB or lower signified severe-stage glaucoma.20,21
Statistical Analysis
Statistical analyses were conducted using R (version 4.1.3). The Kolmogorov–Smirnov test was utilized to assess normal distribution. For non-normally distributed data, non-parametric statistics (the Mann–Whitney U-test or Kruskal–Wallis test) were employed to compare differences in fecal markers between groups. Categorical data were analyzed using the chi-square test, and correlation analyses were performed using Spearman rank correlation. Logistic regression models conditioned on matched pairs were employed to estimate odds ratios and their 95% confidence intervals (CIs). Receiver operating characteristics (ROC) curve analysis and the area under the ROC curve (AUC) were utilized to assess discriminative ability. P-value < 0.05 was considered statistically significant.
Result
Characteristics of the Participants
The characteristics of this study participants are detailed in Table 1. This study included 114 patients with glaucoma and 75 healthy controls, matched for age and gender. The average age in the glaucoma group was 59.6 years, compared to 57.6 years in the control group (p = 0.24). In terms of gender distribution, 60 men (52.6%) were in the glaucoma group and 42 men (56.0%) in the control group (p = 0.76). We categorized patients with glaucoma into subgroups based on the severity of damage: Early (n = 16), Moderate (n = 12), Severe (n = 67).
 |
Table 1 Characteristics of Glaucoma Patients and Healthy Controls |
Elevation of Fecal Lactoferrin Levels as a Biomarker for Intestinal Inflammation in Glaucoma Patients
Fecal Lf levels were compared between glaucoma patients and a cohort of healthy controls, revealing a statistically significant elevation in fecal Lf levels among the glaucoma patients (Figure 1A). Among the glaucoma types, Primary Open-Angle Glaucoma (POAG) and Primary Angle-Closure Glaucoma (PACG) were the most prevalent. Analysis revealed significantly higher median fecal Lf levels in both the PACG and POAG groups compared to controls. However, no significant differences were observed in fecal Lf levels between the POAG and PACG groups (Figure 1B).
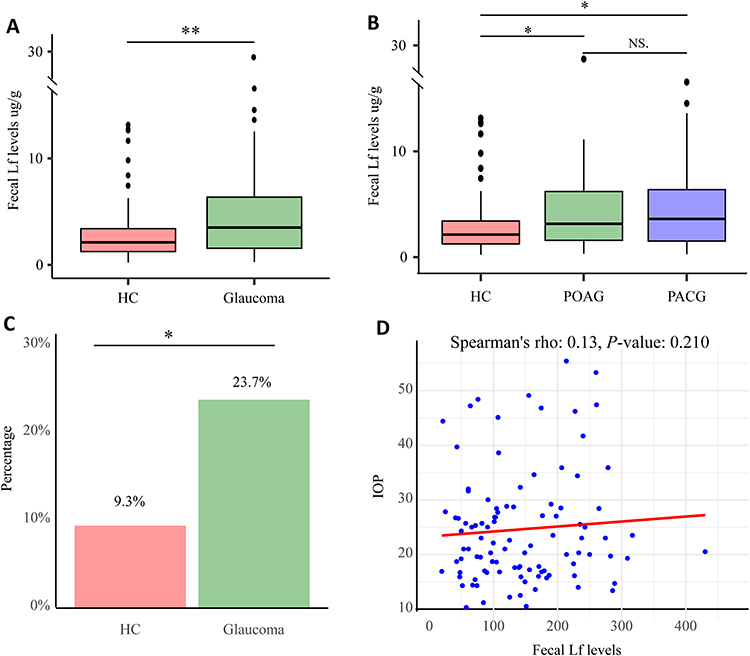 |
Figure 1 Fecal Lf levels in glaucoma patients. (A) Elevated fecal Lf in glaucoma patients. (B) Comparison of fecal Lf levels among healthy controls (HC), Primary Angle-Closure Glaucoma (PACG), and Primary Open-Angle Glaucoma (POAG) subgroups. (C) Comparison the abnormal levels percent of fecal Lf between HC and Glaucoma. (D) The relation between intraocular pressure (IOP) and Fecal Lf levels. Differences between groups were assessed using the Mann–Whitney U-test, and variations among the PACG, POAG, and healthy controls were analyzed using the Kruskal–Wallis test. Abnormal fecal Lf levels were analyzed using the Chi-square test. Additionally, Spearman correlation analysis was employed to assess the relationship between fecal Lf and IOP levels. NS (not significant) indicates no statistical significance; **p < 0.01; *p < 0.05. |
Considering that fecal Lf levels above 7.25 µg/g are highly specific indicators of intestinal inflammation,12,13 we categorized the glaucoma patients into two groups: those with levels ≥ 7.25 µg/g and those with levels < 7.25 µg/g. Elevated fecal Lf levels, exceeding the upper reference limit of 7.25 µg/g, were observed in 23.7% of the 114 glaucoma patients compared to 9.3% of the 75 controls (p = 0.012). The proportion of glaucoma patients with abnormal fecal Lf levels was significantly higher than that of the controls (Figure 1C). It was noted that fecal Lf levels were not influenced by intraocular pressure (IOP) (Figure 1D), age (p > 0.05), and gender (p > 0.05).
Elevation of Fecal Alpha-1 Antitrypsin Levels as a Biomarker for Intestinal Permeability in Glaucoma Patients
Fecal AAT levels were compared between glaucoma patients and healthy controls, demonstrating a statistically significant increase in fecal AAT levels among glaucoma patients (Figure 2A). Concurrent analysis revealed significantly higher median fecal AAT levels in both the PACG and POAG groups compared to controls. However, no significant differences in fecal AAT levels were found between the POAG and PACG groups (Figure 2B). It was observed that fecal AAT levels were not observed by IOP (Figure 2C), age (p > 0.05), and gender (p > 0.05).
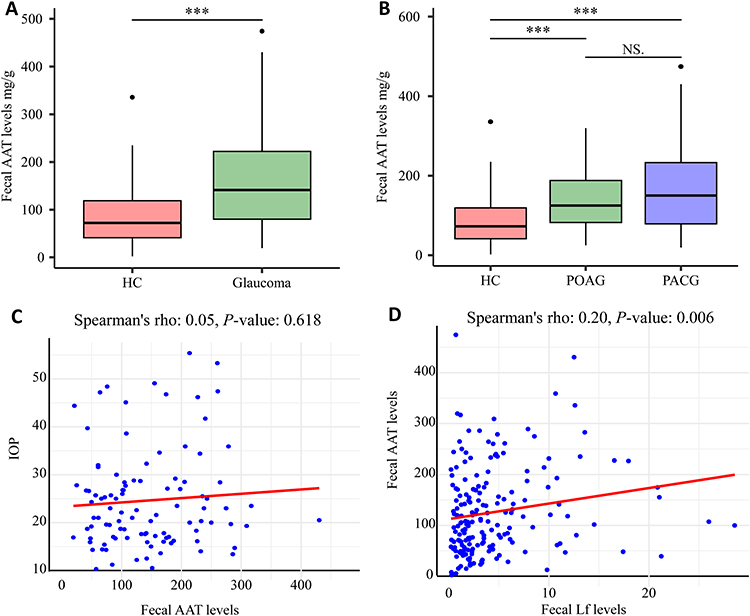 |
Figure 2 Fecal AAT levels in glaucoma patients. (A) Elevated fecal AAT in glaucoma patients. (B) Comparison of fecal Lf levels among HC, PACG, and POAG subgroups. (C) The relationship between fecal AAT levels and IOP. (D) The correlation between fecal Lf and AAT levels. Differences between groups were assessed using the Mann–Whitney U-test, and variations among the PACG, POAG, and healthy controls were analyzed using the Kruskal–Wallis test. Additionally, the relationship was examined using Spearman correlation analysis. NS (not significant) indicates no statistical significance; ***p < 0.001. |
Given the the potential link between intestinal inflammation and permeability, Spearman correlation analysis was employed to assess the relationship between fecal Lf and AAT levels. This analysis revealed a positive correlation between fecal Lf and AAT (rho = 0.20, p = 0.006) (Figure 2D).
Logistic Regression Analysis to Identify Intestinal Biomarkers Associated with Glaucoma
We employed univariate and multivariable logistic regression analyses to evaluate the associations between intestinal inflammation, permeability, and glaucoma. In the univariate analysis, fecal Lf was significantly associated with glaucoma (OR = 1.14, 95% CI: 1.04–1.24, p = 0.004), as was fecal AAT (OR = 1.01, 95% CI: 1.01–1.02, p < 0.001). To further investigate the impact of Lf and AAT on glaucoma, we conducted multivariate logistic regressions, adjusting for age and sex. Both Lf and AAT remained statistically significant predictors after adjusting for these confounders (Lf: OR = 1.11, 95% CI: 1.01–1.21, p = 0.026; AAT: OR = 1.01, 95% CI: 1.01–1.02, p < 0.001) (Table 2).
 |
Table 2 Logistic Regression Analysis of Glaucoma Influencing Factors |
Correlation Between Fecal Biomarkers and Disease Severity and Neural Damage in Glaucoma
We compared fecal Lf and AAT levels among patients with varying disease severities in glaucoma, categorized based on mean deviation (MD) into three subgroups: Early, Moderate, and Severe. Notably, significant differences in fecal Lf levels were observed in the Moderate and Severe stages, but not in the Early stages (Figure 3A). Additionally, patients with different levels of disease severity exhibited varying AAT levels compared to healthy controls, with more severe glaucoma associated with increased AAT levels (Figure 3C). Furthermore, clinical signs of glaucomatous damage are characterized by excavation of the optic nerve head, quantified by the Vertical Cup-to-Disc Ratio (VCDR).22 Patients were grouped based on their VCDR to assess the correlation between fecal Lf and AAT levels with optic nerve damage. The findings revealed that an increase in VCDR was associated with elevated levels of AAT. The group with a C/D ratio between 0.80 and 1.0 exhibited significantly higher AAT levels compared to the group with a C/D ratio of 0.6 or less (Figure 3D). However, Lf levels did not show a significant change (Figure 3B).
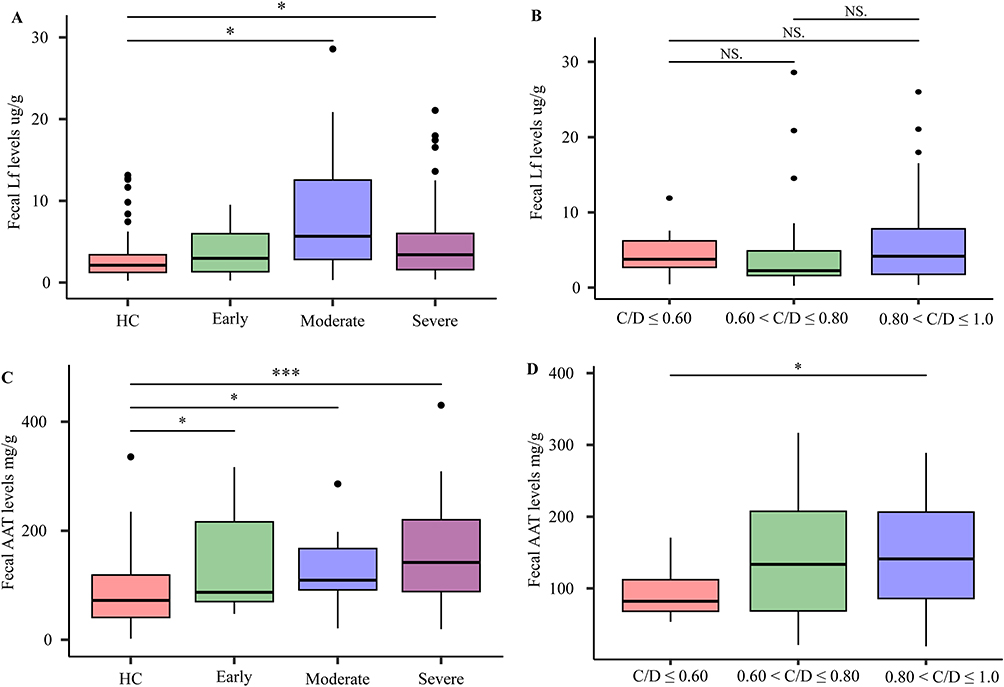 |
Figure 3 Correlations between fecal Lf and AAT levels, glaucoma Severity, and optic nerve damage. (A and C) Lf and AAT levels across different severities of glaucoma. (B and D) and Vertical Cup-to-Disc Ratio (C/D) variations. The differences across the parameters were evaluated using the unpaired Mann–Whitney U-test. Significance levels are indicated as *p < 0.05, ***p < 0.001. |
ROC Curve Analysis of the Discriminatory Ability of Fecal Lf and AAT in Assessing the Severity of Glaucoma
ROC curves were generated to evaluate the discriminative ability of fecal Lf and AAT in distinguishing healthy controls from glaucoma patients with varying severity. The AUC for Lf was 0.722 for differentiating healthy controls from patients with moderate glaucoma, and 0.624 for severe glaucoma (Figure 4A), with respective Youden indices of 0.436 and 0.278. For AAT, the AUCs were 0.686, 0.684, and 0.754 for identifying healthy controls from patients with early, moderate, and severe glaucoma (Figure 4B), respectively, with Youden indices of 0.371, 0.380, and 0.424.
 |
Figure 4 Receiver operating characteristic (ROC) curve analysis was evaluate the discriminative ability of fecal Lf (A) and AAT (B). |
Discussion
In this study, we investigated changes in intestinal inflammation and permeability using fecal biomarkers in patients with glaucoma. Building on our preliminary findings, we further confirmed the presence of intestinal inflammation in patients with glaucoma and the importance of the “gut-retinal” axis in the disease. Our findings revealed that: 1) A higher percentage of abnormalities, considered a highly specific indicator of intestinal inflammation, along with elevated fecal Lf levels, collectively suggest the presence of intestinal inflammation in glaucoma. 2) Increased levels of fecal AAT suggest enhanced intestinal permeability. 3) The positive correlation between fecal Lf and AAT suggests a link between intestinal inflammation and permeability. 4) After adjusting for age and sex, multivariable logistic regression analysis showed that both fecal Lf and AAT are positively correlated with glaucoma. 5) The levels of fecal Lf and AAT might reflect the severity of glaucoma. The AUC demonstrated the relatively good discriminative ability of fecal Lf and AAT in distinguishing glaucoma patients with varying degrees of severity.
Fecal Lf is indicative of intestinal leukocyte infiltration and correlates with the severity of endoscopic and histological inflammation.23 It is known that Lf increases the permeability of the bacterial cell membrane, leading to the release of lipopolysaccharides and other cellular contents from the outer membrane, potentially causing tissue inflammation.22,23 Notably, Lf demonstrates exceptional stability in fecal at room temperature for extended periods.24 Research has shown that among neutrophil-derived proteins in whole gut lavage fluid, Lf serves as a reliable indicator of disease activity in IBD due to its stability, thereby establishing it as a suitable marker for intestinal inflammation.18,24 Fecal Lf concentrations are elevated in IBD compared to irritable bowel syndrome (IBS) and healthy controls.13 Interestingly, increased fecal Lf levels are observed not only in patients with digestive diseases such as IBD but also in neurodegenerative diseases like Parkinson’s disease (PD).12,14 Considering the retina as an extension of the central nervous system (CNS), the characteristics of neurodegenerative processes and immune responses observed in PD are often analogous.25 Additionally, fecal calprotectin is a surrogate marker for endoscopic detection of gut inflammation and intestinal disease activity.10 It is elevated in glaucoma patients, and exhibits a significantly higher percentage of abnormal levels (≥ 250 µg/g), which are considered a highly specific indicator of intestinal inflammation compared to controls.10 Alterations in the gut microbiome of glaucoma patients, along with elevated fecal calprotectin levels, suggest intestinal inflammation.5,10 In this study, elevated fecal Lf levels in glaucoma patients, marked by highly specific abnormal percentages, further support the presence of intestinal inflammation in glaucoma.
AAT is a protease inhibitor synthesized by the liver, served as a reliable indicator of gut leakiness. Compromised intestinal integrity permits this inhibitor to seep into the intestinal lumen, where it resists degradation by digestive enzymes.13 AAT can be detected in fecal samples and remains stable at ambient temperature for extended periods.13,26 Fecal AAT levels are elevated not only in intestinal diseases such as IBD, but also in neurodegenerative diseases like PD.27 Intestinal inflammation often coincides with changes in intestinal permeability.8 Intestinal inflammation is an important cause of increased permeability.8 This heightened permeability allows undesirable large molecules and commensal bacteria to infiltrate the lamina propria, triggering further inflammation and creating a cycle where inflammation increases permeability, which in turn leads to more inflammation.8,28 Our finding of a positive correlation between fecal Lf and fecal AAT also revealed the relationship between these two markers in glaucoma. The increased intestinal permeability and its association with glaucoma severity suggested that AAT played a role in glaucoma development, further reinforcing the importance of the “gut-retina” axis.
Intestinal inflammation and permeability can be influenced by microbiota dysbiosis within the gut.10,22 Recent studies have demonstrated significant variations in the gut microbiome compositions between patients with PACG and healthy individuals, as well as between those with POAG and healthy individuals.29,30 Similarly, rat models have demonstrated significant alterations in gut microbiome compositions in glaucoma compared to controls.31 Dysbiosis of the gut microbiome is frequently linked with chronic intestinal inflammation and increased intestinal permeability.9,32 Our findings of increased intestinal inflammation and permeability are consistent with these observations. Thus, we speculated that increased intestinal inflammation and permeability in glaucoma may be induced by gut microbiome dysbiosis. But, the possible causal relationship between intestinal inflammation and permeability and gut microbiome dysbiosis still remains to be proven.
Although the exact mechanisms by which intestinal inflammation and permeability contribute to the development of glaucoma remain unclear, the intestinal mucosal immune response may play an important role.33 Some studies have indicated that patients with IBD, a chronic inflammatory condition of the gastrointestinal tract, exhibit extra-intestinal manifestations in the eyes.34,35 Our previous study found that mucosal addressin cell adhesion molecule 1 (MAdCAM-1) was upregulated in retinal microvessels, recruiting gut-homing CD4+ T cells, which co-localized with ganglion cells and led to retinal neuron degeneration in a dextran sulfate sodium-induced (DSS) colitis model.36 Additionally, we previously found an increased percentage of circulating CD4+ T cells expressing the gut-homing integrin β7 in patients with glaucoma.7 In an elevated intraocular pressure-triggered glaucoma mouse model, gut-homing β7+ CD4+ T cells gained the ability in the gut to induce retinal MAdCAM-1 expression and cross the blood-retina barrier, leading to retinal ganglion cell degeneration.7 Above all, increased intestinal inflammation and permeability may contribute to the development of glaucoma through the intestinal mucosal immune response, highlighting the pivotal role of the “gut-retina” axis in glaucoma progression.
Intestinal inflammation and permeability can serve as indicators of intestinal barrier integrity.22 Disruptions in gut microbiota composition or inflammatory changes in the mucosal tissue can compromise adherence and tight junctions, increasing permeability and leading to the breakdown of the intestinal barrier.33 This, in turn, results in the abnormal translocation of luminal contents into the mucosa.33,37 Current evidence suggests that various neurological, psychiatric, and neurodevelopmental CNS disorders are linked to functional and structural changes in the intestinal barrier.37 Mechanistically, an impaired gut barrier may allow bacteria and their products to translocate into the mucosa and bloodstream, potentially spreading to the brain.37,38 This translocation, along with haptoglobin release, could activate immune and inflammatory responses, thereby contributing to central neuroinflammation.37 Given the analogous characteristics of the neurodegenerative processes in glaucoma and CNS diseases,25 along with gut microbiome dysbiosis, increased intestinal inflammation, and permeability, we propose that disruption of the intestinal barrier may play a role in the development of glaucoma. Drugs that protect the intestinal barrier could potentially be repurposed as adjunct therapy for glaucoma.
This study has several limitations that warrant further investigation. Firstly, our conclusions require further validation through the recruitment of a larger cohort of glaucoma patients and the execution of a multi-center study. Secondly, while fecal Lf and AAT serve as robust non-invasive markers for assessing gut inflammation and permeability, additional studies employing endoscopic and histological evaluations are essential. Lastly, further mechanistic studies are necessary to determine whether changes in intestinal markers simply correlate with an increased risk of glaucoma or play a causal role, a question not addressed by the current study design.
In conclusion, our findings indicated increased intestinal inflammation and permeability in glaucoma, which were correlated with disease severity. These results highlight the significant role of intestinal permeability and inflammation in glaucoma pathogenesis, further emphasizing the importance of the “gut-retina” axis and potentially revealing new therapeutic targets.
Acknowledgments
This work is financially supported by grants from the National Natural Science Foundation of China (82370560 and 82450003) and the Si-chuan Science and Technology Program grants (2023YFS0022).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Jayaram H, Kolko M, Friedman DS, Gazzard G. Glaucoma: now and beyond. Lancet. 2023;6736(23):1–14. doi:10.1016/S0140-6736(23)01289-8
3. Vergroesen JE, Jarrar ZA, Weiss S, et al. Glaucoma patients have a lower abundance of butyrate-producing taxa in the gut. Invest Ophthalmol Visual Sci. 2024;65(2). doi:10.1167/iovs.65.2.7
4. Li C, Lu P. Association of gut microbiota with age-related macular degeneration and glaucoma: a bidirectional Mendelian randomization study. Nutrients. 2023;15(21):4646. doi:10.3390/nu15214646
5. Pezzino S, Sofia M, Greco LP, et al. Microbiome dysbiosis: a pathological mechanism at the intersection of obesity and glaucoma. Int J Mol Sci. 2023;24(2). doi:10.3390/ijms24021166
6. Chen H, Cho KS, Vu TK, et al. Commensal microflora-induced T cell responses mediate progressive neurodegeneration in glaucoma. Nat Commun. 2018;9(1). doi:10.1038/s41467-018-05681-9
7. He C, Xiu W, Chen Q, et al. Gut-licensed β7+ CD4+ T cells contribute to progressive retinal ganglion cell damage in glaucoma. Sci Trans Med. 2023;15(707):1–14. doi:10.1126/scitranslmed.adg1656
8. Mishra SP, Wang B, Jain S, et al. A mechanism by which gut microbiota elevates permeability and inflammation in obese/diabetic mice and human gut. Gut. 2023;72(10):1848–1865. doi:10.1136/gutjnl-2022-327365
9. Chang CCJ, Liu B, Liebmann JM, Cioffi GA, Winn BJ. Glaucoma and the Human Microbiome. J Glaucoma. 2024;33:529–538. doi:10.1097/ijg.0000000000002448
10. Wang Z, Yuan H, Zhu X, et al. Fecal calprotectin as an intestinal inflammation marker is elevated in glaucoma. Biomarkers Med. 2023;17(9):465–473. doi:10.2217/bmm-2023-0352
11. Martini E, Krug SM, Siegmund B, Neurath MF, Becker C. Mend your fences: the epithelial barrier and its relationship with mucosal immunity in inflammatory bowel disease. Cmgh. 2017;4(1):33–46. doi:10.1016/j.jcmgh.2017.03.007
12. Singh S, Ananthakrishnan AN, Nguyen NH, et al. AGA clinical practice guideline on the role of biomarkers for the management of ulcerative colitis. Gastroenterology. 2023;164(3):344–372. doi:10.1053/j.gastro.2022.12.007
13. Musci JOD, Cornish JS, Däbritz J. Utility of surrogate markers for the prediction of relapses in inflammatory bowel diseases. J Gastroenterol. 2016;51(6):531–547. doi:10.1007/s00535-016-1191-3
14. Rajkovaca Latic I, Popovic Z, Mijatovic K, et al. Association of intestinal inflammation and permeability markers with clinical manifestations of Parkinson’s disease. Parkinsonism Related Disord. 2024;123(December 2023):106948. doi:10.1016/j.parkreldis.2024.106948
15. Yang X, Ai P, He X, et al. Parkinson’s disease is associated with impaired gut–blood barrier for short-chain fatty acids. Mov Disord. 2022;37(8):1634–1643. doi:10.1002/mds.29063
16. Wang Z, Liu D, Yuan H, et al. Association of plasma lactoferrin levels with disease severity in glaucoma patients. Front Med. 2024;11:1–7. doi:10.3389/fmed.2024.1385358
17. Yuan H, Li A, Chen L, et al. Α-1 antitrypsin is promising for the identification of glaucoma severity and is associated with glaucomatous neural damage. Biomarkers Med. 2024:18. doi:10.1080/17520363.2024.2347190
18. Mosli MH, Zou G, Garg SK, et al. C-reactive protein, fecal calprotectin, and stool lactoferrin for detection of endoscopic activity in symptomatic inflammatory bowel disease patients: a systematic review and meta-analysis. Am J Gastroenterol. 2015;110(6):802–819. doi:10.1038/ajg.2015.120
19. Carrasco-Labra A, Lytvyn L, Falck-Ytter Y, Surawicz CM, Chey WD. AGA technical review on the evaluation of functional diarrhea and diarrhea-predominant irritable bowel syndrome in adults (IBS-D). Gastroenterology. 2019;157(3):859–880. doi:10.1053/j.gastro.2019.06.014
20. Yu L, Chen Y, Xu X, et al. Alterations in peripheral b cell subsets correlate with the disease severity of human glaucoma. J Inflamm Res. 2021;14(September):4827–4838. doi:10.2147/JIR.S329084
21. Chen CL, Bojikian KD, Wen JC, et al. Peripapillary retinal nerve fiber layer vascular microcirculation in eyes with glaucoma and single-hemifield visual field loss. JAMA Ophthalmol. 2017;135(5):461–468. doi:10.1001/jamaophthalmol.2017.0261
22. Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol. 2002;86(2):238–242. doi:10.1136/bjo.86.2.238
23. Yamamoto T, Shimoyama T, Bamba T, Matsumoto K. Consecutive monitoring of fecal calprotectin and lactoferrin for the early diagnosis and prediction of pouchitis after restorative proctocolectomy for ulcerative colitis. Am J Gastroenterol. 2015;110(6):881–887. doi:10.1038/ajg.2015.129
24. Gisbert JP, McNicholl AG, Gomollon F. Questions and answers on the role of fecal lactoferrin as a biological marker in inflammatory bowel disease. Inflammat Bowel Dis. 2009;15(11):1746–1754. doi:10.1002/ibd.20920
25. Ashok A, Singh N, Chaudhary S, et al. Retinal degeneration and Alzheimer’s disease: an evolving link. Int J Mol Sci. 2020;21(19):1–17. doi:10.3390/ijms21197290
26. Putra C, Bello D, Kelleher SL, Tucker KL, Mangano M. NanoImpact Stool titanium dioxide is positively associated with stool alpha-1 antitrypsin and calprotectin in young healthy adults. NanoImpact. 2024;
27. Dillmann U, Grundmann D, Schwiertz A, et al. Fecal markers of intestinal in fl ammation and intestinal permeability are elevated in Parkinson’ s disease. Parkinsonism Related Disord. 2018:8–11. doi:10.1016/j.parkreldis.2018.02.022
28. Camara-lemarroy CR, Metz L, Meddings JB, Sharkey KA, Wee Yong V. The intestinal barrier in multiple sclerosis: implications for pathophysiology and therapeutics The intestinal barrier. Brain. 2018;141:1900–1916. doi:10.1093/brain/awy131
29. Gong H, Zhang S, Li Q, et al. Gut microbiota compositional profile and serum metabolic phenotype in patients with primary open-angle glaucoma. Exp. Eye Res. 2020;191(September 2019):107921. doi:10.1016/j.exer.2020.107921
30. Gong H, Zeng R, Li Q, et al. The profile of gut microbiota and central carbon-related metabolites in primary angle-closure glaucoma patients. Intl Ophthalmol. 2022;42(6):1927–1938. doi:10.1007/s10792-021-02190-5
31. Zhang Y, Zhou X, Lu Y. Gut microbiota and derived metabolomic profiling in glaucoma with progressive neurodegeneration. Front Cell Infect Microbiol. 2022;12(August):1–12. doi:10.3389/fcimb.2022.968992
32. Chen J, Wright K, Davis JM, et al. An expansion of rare lineage intestinal microbes characterizes rheumatoid arthritis. Genome Med. 2016;8(1):1–14. doi:10.1186/s13073-016-0299-7
33. Matei DE, Menon M, Alber DG, et al. Intestinal barrier dysfunction plays an integral role in arthritis pathology and can be targeted to ameliorate disease. Med. 2021;2(7):864–883.e9. doi:10.1016/j.medj.2021.04.013
34. Falloon K, Cohen B, Ananthakrishnan AN, et al. HHS Public Access manifestations in inflammatory bowel disease. Gastroenterol Hepatol. 2023;55(9):1179–1191. doi:10.1111/apt.16853.A
35. Hedin CRH, Vavricka SR, Stagg AJ, Schoepfer A, Raine T. ECCO scientific workshop paper ECCO scientific workshop paper the pathogenesis of extraintestinal manifestations: implications for IBD research, diagnosis, and therapy. J Crohn’s Colitis. 2019;13:541–554. doi:10.1093/ecco-jcc/jjy191
36. Peng K, Xiao J, Wang J, et al. MAdCAM-1 mediates retinal neuron degeneration in experimental colitis through recruiting gut-homing CD4+ T cells. Mucosal Immunol. 2021;14(1):152–163. doi:10.1038/s41385-020-0282-x
37. Pellegrini C, Fornai M, D’Antongiovanni V, Antonioli L, Bernardini N, Derkinderen P. The intestinal barrier in disorders of the central nervous system. Lancet Gastroenterol Hepatol. 2023;8(1):66–80. doi:10.1016/S2468-1253(22)00241-2
38. Pellegrini C, Antonioli L, Calderone V, Colucci R, Fornai M, Blandizzi C. Microbiota-gut-brain axis in health and disease: is NLRP3 inflammasome at the crossroads of microbiota-gut-brain communications? Progres Neurobiol. 2020;191(March):101806. doi:10.1016/j.pneurobio.2020.101806
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.