")
Back to Journals » Journal of Inflammation Research » Volume 17
Inflammation-Associated Coagulation Reactions are Associated with the Prognosis in Critically Ill Very Old Patients (VOPs) with Infection
Authors Lian H, Cai H, Wang X , Zhang H, Gao Y, Zhang S, Zhang Y
Received 22 April 2024
Accepted for publication 12 November 2024
Published 21 November 2024 Volume 2024:17 Pages 9335—9346
DOI https://doi.org/10.2147/JIR.S474990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Hui Lian,1 Huacong Cai,2 Xiaoting Wang,3 Hongmin Zhang,3 Yuan Gao,4 Shuyang Zhang,5 Yan Zhang2
1Department of Health Care, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Hematology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3Department of Critical Care Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 4Department of Information Technology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 5Department of Cardiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, 100730, People’s Republic of China
Correspondence: Yan Zhang, Department of Hematology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China, Email [email protected]; Shuyang Zhang, Department of Cardiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, 100730, People’s Republic of China, Email [email protected]
Background: Dysregulated host response is an important cause of critical illness. Coagulation reaction is the most primitive response and can be used to assess patient status. Coagulation reactions may be amplified in very old patients (VOPs). This study aimed to demonstrate coagulation reactions in critically ill VOPs by linking cytokines, coagulation, and fibrinolytic processes.
Methods: We analyzed 33 critically ill VOPs admitted to our hospital, with an average age of 91.97. Laboratory test results were collected and double checked. In-hospital mortality, Intensive Care Unit (ICU) stay, and length of in-hospital stay (LOS)-associated variables were assessed using a generalized additive mix model. Smooth curves and interaction tests were used to quantify statistical interactions.
Results: The in-hospital mortality rate was 45.5% in this study. The D-dimer level was correlated with ICU stay [risk ratio (RR), 1.39; 95% confidential interval (CI), 1.16– 1.67] and LOS (RR, 1.75; 95% CI, 1.19– 2.57). Other function or quantity indices, such as platelet (PLT), prothrombin time (PT), activated partial prothrombin time (APTT), and thrombomodulin (TM), were all correlated with clinical outcomes. After the link between coagulation reaction and the outcomes was constructed, it was revealed that, compared to lower level of IL-6, under high level of IL-6, elevated TM was likely to be associated with tissue plasminogen activator inhibitor complex (t-PAIC) elevation, which probably promoted the production of D-dimer (RR, 3.216; 95% CI, 1.840– 4.592).
Conclusion: D-dimer levels are associated with outcomes in VOPs with critical illness. There is a certain link between inflammatory cytokines and the coagulation process. Under high IL-6 levels, the elevated TM may contribute to the increased t-PAIC, which contributes to the higher D-dimer level. Conversely, under low IL-6 levels, elevated TM levels are associated with reduced t-PAIC levels.
Keywords: blood coagulation, very old patients, VOPs, critical illness, in-hospital mortality
Introduction
With an in-depth understanding of the pathophysiology of patients, critical illnesses have been redefined.1 Dysregulated host defense or response is revealed to be an important cause of critical illnesses. According to the definition from Sepsis 3.0, the patients with sepsis develop critical illness because of a dysregulated host response,2 rather than direct invasion by infected pathogens, which confirms this viewpoint. Previous study has shown that the inflammatory response and activation of coagulation are two important responses in the host defense against infection.3 These two responses interact, which affects prognosis.4
Coagulation reaction refers to the process in which coagulation factors in the blood interact after blood vessel damage to form fibrin clots, which includes a series of complex biochemical processes such as the activation of coagulation factor, the production of thrombin and the conversion of fibrinogen to fibrin.5 The coagulation reaction is the most primitive response, which can be observed in ancient horseshoe crabs.6 The coagulation reactions can be divided into three main stages. The first stage is a cytokine reaction to injury in the tissues or endothelial cells. Many cells and molecules, including white blood cells, platelets (PLT), and various cytokines, are involved in this process. The second stage is the formation of a coagulation cascade in which both the intrinsic and extrinsic coagulation pathways are activated. The final stage is the fibrinolytic process. With the rapid development of medical laboratory technology, almost all coagulation processes can be detected, offering a good opportunity for medical staff to understand the different stages of host response. Unlike other host responses, coagulation reactions increase with age, which is confirmed by higher levels of biomarkers.7 The CHA2DS2-VASc score has been used to guide anticoagulation therapy in atrial fibrillation patients.8,9 In the score, patients older than 75 years will receive doubled points, which represents a higher risk for thrombosis. Another study concluded that aging plays an important role in ischemic stroke.10 However, these studies were conducted in patients with chronic diseases rather than those with acute illnesses. Recent studies have focused on consumptive coagulopathy in critically ill patients and found that prolonged prothrombin time (PT) may be associated with a dysregulated host response in patients with sepsis.11
At present, few studies have clearly linked cytokines, coagulation, and fibrinolytic processes to assess the coagulation response in critically ill patients. As critical illness progresses rapidly, especially in very old patients (VOPs, ≥ 80 years old),12 which might amplify the coagulation reaction, we conducted the present study. Our study aimed to demonstrate the coagulation reactions in critically ill VOPs and their effect on prognosis, and to preliminarily explore their relationship with the inflammatory response from a clinical point of view.
Methods
Patients Enrollment
This study complies with the Declaration of Helsinki. This prospective study began in September 2022. The periodic pandemic COVID-19 broke out in China between November 2022 and March 2023. During this period, many VOPs actively sought medical help, and as a result, hospitals received more VOPs than usual, providing relatively sufficient patients for study. Written informed consent was obtained from all the participants. The research protocol was approved by the Ethics Committee of the Peking Union Medical College Hospital (Ethical Approval Number: I-23YJ187). VOPs (≥ 80 years of age) with various underlying diseases admitted to our inpatient department due to recent infections were included between October 1st, 2022, and March 31st, 2023, from Peking Union Medical College Hospital. Patients with critical illness during hospitalization were included, regardless of whether they were admitted to the intensive care unit (ICU). Patients who refused to participate were excluded from the study. Ultimately, 33 VOPs were included in this study. Among them, 17 VOPs were admitted to hospital due to COVID-19.
Data Collection
Demographic, clinical, laboratory, medication, and outcome data were obtained from an electronic medical record system. The demographic data included age and sex. Clinical and medication data included clinical outcomes, comorbidities, length of hospital stay (LOS), and intensive care unit (ICU) days. The results of laboratory tests included routine blood tests (eg, PLT count), 12 items of cytokines [including interleukin (IL)-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12p70, IL-17, interferon (IFN)-α, IFN-γ, tumor necrosis factor (TNF)-α], coagulation function-related parameters [eg, fibrinogen (Fbg), activated partial thromboplastin time (APTT), PT, D-dimer], thrombosis-related parameters [including thrombomodulin (TM), thrombin antithrombin complex (TAT), α2-plasmininhibitor-plasmin complex (PIC), tissue plasminogen activator inhibitor complex (t-PAIC)], blood gas analyses, and other assessments (hepatorenal function, myocardial enzymes, and electrolytes). The levels of cytokines were detected with immunofluorescence method by a flow cytometer (FACScalibur, BD Biosciences, San Jose, CA, USA), with the corresponding kits (Saiji Biotech., Nanchang, China). Chemiluminescence method was applied to detect the levels of t-PAIC and PIC, with an automated immunoassay system (HISCL −2000i, SYSMEX, Takaoka, Japan). The data of other parameters were obtained from the routine tests in the hospital. All of the above parameters were measured at baseline, while the testing frequency was determined based on disease progression. Personal information was removed to protect privacy. The primary endpoint was in-hospital mortality, while the secondary endpoints included ICU stay and length of in-hospital stay (LOS).
Statistical Analysis
Categorical variables are presented as numbers (percentages). After the Kruskal–Wallis test, only age conformed to a normal distribution, which is presented as mean ±standard deviation (SD). The rest of the continuous data are presented as the minimum, 25th percentile, median (50th percentile), 75th percentile, and maximum. A generalized additive mix (GAM) model was used to conduct the univariate analysis, and smooth curves were used to quantify statistical interactions with GAM package in R software. Interaction tests were performed to test for statistical significance. A 2-tailed P<0.05 was considered to be statistically significant in all analyses. EmpowerStats (http://www.empowerstats.com) and R software, version 4.2.0 (http://www.R-project.org/) were used for all the statistical analyses.
Results
Baseline Characteristics of the Patients
The ages of the patients ranged from 80 to 103 years, with a mean age of 91.97. Among them, 30 were male, accounting for 90.9% of the study population. Most of them were hospitalized for more than six weeks, and the longest length of stay in this group was 91 days. 20 of them experienced ICU during hospitalization. The in-hospital mortality rate was 45.5% (Table 1).
 |
Table 1 Demographic Characteristics and Clinical Outcomes of the Study Population |
The Results of Laboratory Tests
The PLT was tested 206 times, 155 of which were below the normal lower limit, while almost none of them were higher than the upper normal limit. A total of 12 cytokines were tested 61 times. IL-1β, IL-2, and IFN-α levels were all within the normal range, whereas TNF-α levels were almost within the normal range in all patients. For IL-4, IL-5, IL-12p70, and IFN-γ, over 75% of the measurements were within normal ranges. Almost half of the measurements were abnormal for IL-10 and IL-17 levels. For IL-6, only 4 of the 61 measurements were within the normal range. This number was 7 for IL-8. These results suggested IL-6 and IL-8 were the main cytokines involved in the inflammatory response of VOPs. PT, Fbg, APTT, and D-dimer levels were measured 201 times. A prolonged PT and APTT were observed in 125 and 136 tests, respectively. For Fbg, 17 tests were below the normal lower limit and 65 were above the upper normal limit. For D-dimer, the results of 4 tests were normal, and the rest were abnormal. Thrombosis-related examination indicated that the results of 24 tests of TMs were normal, whereas 108, 93, and 119 tests were outside the normal ranges for TAT, PIC, and t-PAIC, respectively (Table 2).
 |
Table 2 Coagulation Related Serum Biomarkers of the Study Population |
The Relationship Between Laboratory Tests and Clinical Variables of the VOPs
The maximum parameters measured after admission were used to determine their relationship with the outcome variables. As shown (Table 3), prolonged PT and APTT were correlated with increased mortality, whereas PLT was a protective factor against mortality. VOPs with higher APTT and D-dimer, TAT, and PIC levels had longer ICU stays. PT, APTT, PIC, and D-dimer levels were risk factors for a longer LOS. Notably, a 1 mg/L increase in D-dimer level will extend the ICU stay by 39%, while the LOS will be extended by 75%. We focused on D-dimer as it has been examined as an outcome indicator. As shown (Figure 1), D-dimer levels changed in a curvilinear relationship over time in both survivors and non-survivors, with an upward trend in the non-survivor group. Spearman correlation analysis was used to preliminarily explore the correlation between inflammatory factors and coagulation reactions. As shown (Table 4), statistically significant differences were observed between multiple pairs of cytokines and serum coagulation biomarkers. A strong correlation, with a coefficient greater than 0.7, was observed between IL-2 and IL-4, IL-4 and IL-17, IL-4 and IFN-α, and IL-17 and IFN-α. Moderate correlation, with a coefficient between 0.5 and 0.7, was observed between IL-2 and IL-17, IL-2,andIL-1β, IL-2 and IFN-α, IL-2 and IL-5, IL-6 and APTT, IL-6 and IL-8, IL-6 and IL-10, IL-8 and PLT, IL-8 and TM, IL-8 and APTT, IL-8 and PT, IL-8 and TNF-α, IFN-α and IL-10, IFN-α and IL-17, IFN-α and TNF-α, TNF-α and IL-1β, TNF-α and IL-5, TNF-α and TM, IFN-α and IFN-γ, IL-1β and IL-12p70, IL-1β and IL-5, TAT and D-dimer, TM, and Fbg. Among these, TM and Fbg levels were negatively correlated.
 |
Table 3 Maximum Levels of Coagulation Related Factors and Correlation with Mortality, ICU Stay and LOS in Single-Factor Model |
 |
Table 4 Spearman Correlation Analyses Among Serum Biomarkers |
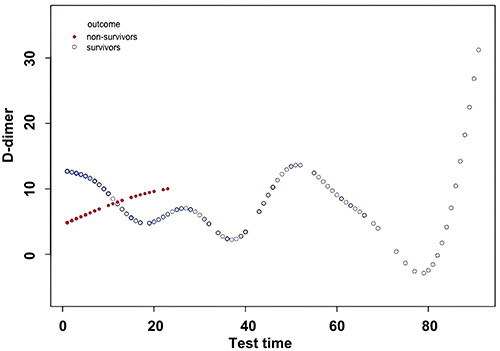 |
Figure 1 D-dimer trend in both survivors and non-survivors over time. The smooth curves were generated by generalized additive mix models. Abbreviation: Test Time, days after admission. |
Under Inflammation TM and t-PAIC May Contribute to Elevated D-Dimer
Furthermore, we conducted interaction tests for all the cytokines and coagulation factors. All repeated measurements of the data were used for the interaction evaluation. The interaction between inflammation status, coagulation process, and coagulation outcome indicators was statistically significant. Figure 2A–C shows the changing trend of statistically significant parameters (including TM, t-PAIC, and D-dimer) over time. Figure 3A and B presents the association between different parameters stratified by IL-6, and the results indicate that there are significant associations between TM and t-PAIC levels and between t-PAIC and D-dimer levels, with P-values of 0.0343 and 0.0011, respectively. Table 5 quantifies risk ratio (RR) in Figure 1, using a multi-factor model adjusted for age, sex, and test time. Although TM and t-PAIC do not directly affect the primary clinical outcomes, they can affect D-dimer levels during inflammation. The inflammation status was divided into two groups on average, based on IL-6 levels. Elevated TM was associated with t-PAIC elevation, which promoted D-dimer production in the presence of high IL-6 levels.
 |
Table 5 Risk Ratio for TM, t-PAIC and D-Dimer Stratified by IL-6 Status in the Single-Factor Model and P-value for Interaction. The Model Adjusts for Age, Gender and Test Time |
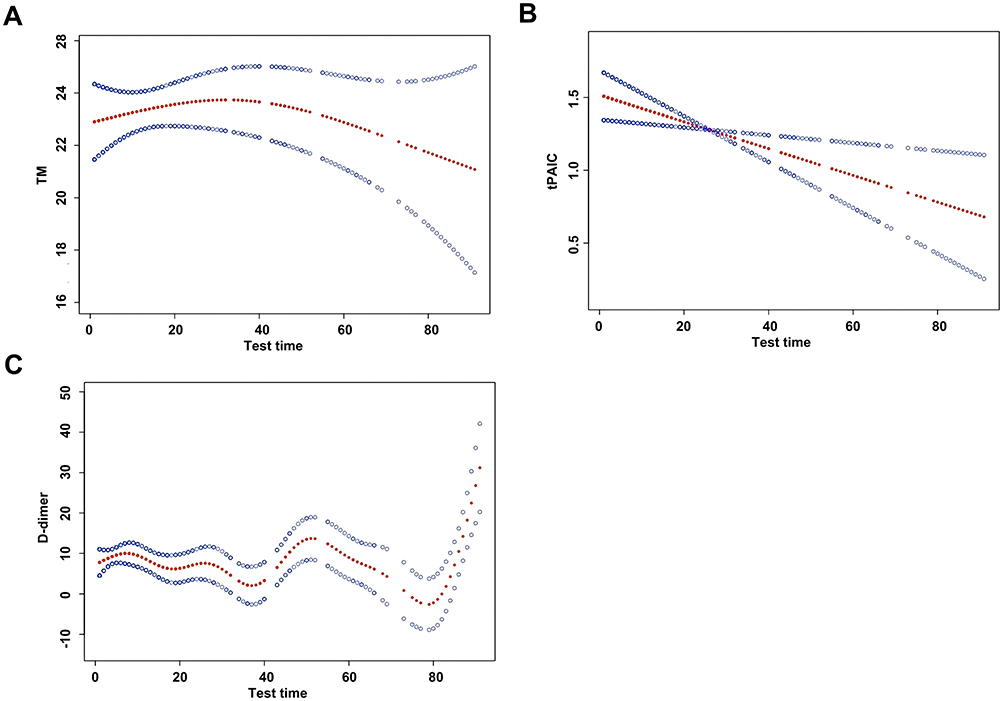 |
Figure 2 The smooth curves of three parameters over time. (A) The change trend of TM after the VOPs admitted to the hospital. TM showed a downward trend after the patients admitted to the hospital. (B) The change trend of t-PAIC after the VOPs admitted to the hospital. t-PAIC showed a downward trend after the patients admitted to the hospital. (C) The change trend of D-dimer after the VOPs admitted to the hospital. D-dimer showed an upward trend after the patients admitted to the hospital. The red solid dot represents the risk ratio value, and the blue control new store represents the 95% confidence intervals. Abbreviations: Test Time, days after admission; TM, thrombomodulin; t-PAIC, tissue plasminogen activator inhibitor complex. |
 |
Figure 3 The association among the parameters after the patients were stratified by IL-6 level (A) Smooth curves between TM and t-PAIC stratified by IL-6 status in single-factor model. In condition of high IL-6 level, TM level and t-PAIC level showed a positive correlation; while in the condition of low IL-6 level, TM level and t-PAIC level showed a negative correlation. (B) Smooth curves between t-PAIC and D-dimer stratified by IL-6 status in single-factor model. The model adjusts for age, gender and test time. In condition of high IL-6 level, D-dimer level and t-PAIC level showed a positive correlation; while in the condition of low IL-6 level, D-dimer level and t-PAIC level showed a negative correlation. Abbreviations: IL-6, interleukin 6; TM, thrombomodulin; t-PAIC, tissue plasminogen activator inhibitor complex. |
Discussion
This study was conducted in VOPs with critical illness, with an average age of 91.97 years old. The results showed that coagulation abnormalities affect the prognosis in this special population. Notably, only under high levels of IL-6, indicating excessive inflammation, elevated TM contributes to the increase in t-PAIC, which then contributes to a higher D-dimer level. Furthermore, a higher D-dimer level was associated with prolonged ICU stay and LOS.
Critical illness is a life-threatening organ dysfunction caused by dysregulated host responses to various factors, such as coronavirus disease 2019,13–15 severe acute pancreatitis,16 and traumatic brain injury.17,18 Coagulation reaction plays an important role in the host response.19 The coagulation reaction starts with injury or inflammation to the vascular wall or endothelial cells. With the development of detection technology, there are many function and quantity indices for every coagulation process. D-dimer is the product of fibrin degradation, which is the last process. Previously, we reported that elevated D-dimer levels were associated with disease severity in patients aged > 65 years in the ICU.20 This conclusion is confirmed again in this small cohort of VOPs: patients with higher D-dimer levels had longer ICU stays and LOS. Similar to a previous retrospective study,20 we did not find a significant correlation between D-dimer level and mortality. The upward trend in D-dimer levels in the non-survivor group indicated that the coagulation reaction was not well-controlled after admission. Good control of the coagulation reaction may affect the prognosis of VOPs. Another factor that might influence prognosis is willingness for treatment. As VOPs have more basic diseases and poor compensatory abilities, it is difficult to recover to a normal state after critical illness. To reduce pain, many families chose to withhold invasive resuscitative efforts at any time during hospitalization, such as tracheal intubation, blood purification treatment, and chest compression, which may have influenced the statistical results.
Some function or quantity indices, such as PLT, PT, APTT, PIC, and TAT, are associated with prognostic factors. Among these, PLT count appears to be a protective factor against mortality, ICU stay, and LOS. A U-shaped curve was found between the baseline PLT count and total mortality in the Women’s Health Initiative Study.20 A meta-analysis conducted among adults with COVID-19 admitted to the ICU showed that PLT counting is a protective factor against mortality.21 This is both reasonable and understandable. In critical illness, a high PLT count is rare because most patients have a low platelet count owing to coagulation reactions and platelet consumption. However, in patients with chronic diseases, PLT counts with a level higher than the upper limit can be seen in a small group of patients, which is a risk factor for mortality (eg, some patients with cancers).22 In our study, the highest PLT count was 354×109/L, which is slightly higher than the threshold value (350×109/L). PT and APTT are functional indicators in coagulation reaction assessment, whereas TAT and PIC are quantitative indicators for coagulation and fibrinolysis. They represented the severity of the coagulation reaction. We did not positively associate TM and t-PAIC with the endpoints. Previous studies have found the link between TM and increased mortality in children.23,24 A meta-analysis of 12 studies has yielded similar results in adults.25 However, in the present study, similar findings were not observed for the VOPs. This may be because TM has several physiological effects and has complex mechanisms of action. The targets of this action require further exploration in VOPs.
Although we measured 12 cytokines, we did not use them directly for prognostic research. Cytokines produced by various pathways initiate inflammatory and coagulation responses, which may influence the prognosis. Previous studies have suggested that reduced inflammation, but not telomere length, contributes to the successful aging of centenaries.26 However, other studies have suggested that older individuals tend to develop chronic inflammation.27 In fact, not cytokines, but their place of action, might determine whether they are dangerous or beneficial for physiological responses. In addition, high levels of anti-inflammatory molecules in long-living groups may promote prognosis. Thus, high systemic levels of unique cytokines would not confer outcomes in VOPs.28
Inflammation is associated with coagulation reactions in the VOPs. Spearman correlation analysis revealed several associations. Most of these associations were among the cytokines. Our findings suggest that IL-6 and IL-8 are involved in the activation of coagulation, with significant upregulation in some VOPs, which is supported by another study.29 However, the causal relationship between inflammation and thrombosis still remains unknown among VOPs. Increased levels of IL-6, IL-8, and TNF-α have been observed in patients with venous thrombosis.30 Activation of Xa factor can induce the expression of IL-6 and IL-8 in endothelial cells and monocytes.31 Some products of the clotting cascade may also affect cytokine production and release of cytokines.32 These findings may explain the up-regulation of cytokines in VOPs with infection. The concerted action of TNF-α and neutrophils promotes TM release from the endothelial cells.33 In our study, we observed a positive relationship between TNF-α and TM levels, which is reasonable.
To further explore the relationship between cytokines and the coagulation process, we performed interaction analysis. Fortunately, we identified an underlying mechanism linking TM and mortality in VOPs. In other words, under high IL-6 levels, TM may promote the formation of t-PAIC. Increased t-PAIC was correlated with D-dimer overproduction, which affected the outcomes. Under relatively low levels of IL-6, high levels of TM were correlated with low levels of t-PAIC. The possible mechanism is as follows: IL-6 is a pro-inflammatory factor; however, a lower level of IL-6 may be associated with anti-inflammatory status.34 TM can reduce the clotting activity of thrombin by binding to it and enhancing its activation of protein C, the main anticoagulant.35 The activation of the fibrinolytic system is weak due to reduced thrombosis. Therefore, t-PAIC levels were low. The higher the level of TMs in the blood, the lower is the need for t-PAICs. In contrast, a higher IL-6 level indicates more thrombosis, and TMs are related to the amount of thrombosis. More TMs indicate that more t-PAICs are required. Under the latter circumstances, more t-PAICs eventually lead to more D-dimers, which are a type of fibrin degradation product. At lower IL-6 levels, t-PAIC can promote fibrinolysis and inhibit fibrinolysis, which can be adjusted accordingly in the VOPs. Further studies are needed to confirm this hypothesis in the future.
Our study has some limitations. First, this was a single-center, prospective study. Limited by age and willingness to seek medical help, the sample size is relatively small. A severe imbalance was observed in the proportion of male-to-female patients. The current study is ongoing, and the sample size will gradually expand with the extension of the research time. However, trends in the main findings may not changed. Sex was not considered a relative risk in our study because coagulation reaction is a classic biological process. In future, we will further explore the relationship between chronic diseases and coagulation reactions. Secondly, it should be noted that, LOS is also a risk factor of thrombosis, and in the future work, with larger sample size, the causal relationships among inflammation, LOS and coagulation disorders should be clarified with more convincing data. Thirdly, the frequency of repeated measurements depends on the clinician. Therefore, the individual heterogeneity was relatively high. We will fix the frequency in the future if possible. Additionally, as mentioned above, mortality rate is affected by the wishes of the patient or family members in clinical activities, which improves the heterogeneity of individuals. Nevertheless, the trend of the results will not change, which still has a guiding significance for clinical research and further work. Last but not least, in the present work, COVID-19 was the main etiology for the enrolled patients (17/33). Even though COVID-19 leads to severe inflammation of the “cytokine storm”, which is a typical characteristic of severe infection,36 in the future work, it is worth investigating, for the VOPs with other types of infections (eg hospital acquired pneumonia), whether there exists an relationship between inflammation-associated coagulation reaction and the clinical outcome of the patients.
Conclusion
In VOPs with critical illnesses related to infection, coagulation abnormalities including PLT, PT, APTT, TAT, PIC, and D-dimer probably contribute to poor outcomes. A link exists between inflammatory cytokines and coagulation. Under high IL-6 levels, elevated TM may contribute to the increase in t-PAIC, which contributes to a higher D-dimer level. Conversely, under low IL-6 levels, elevated TM is linked to reduced t-PAIC, suggesting that actively controlling inflammation in clinical practice is of great significance in improving the prognosis of these patients. More studies should concentrate on inflammation-endothelial cell-fibrinolytic systems to decipher the regulatory mechanisms of inflammation, TM, t-PAIC, and D-dimer levels.
Data Sharing Statement
All clinical data that support this study are available from the corresponding authors upon reasonable request. All materials will be provided only after the request is submitted, formally reviewed, and approved by the Ethics Committee of the Peking Union Medical College Hospital. The details of methodology to detect the parameters used in the present work are also available from the corresponding authors upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Peking Union Medical College Hospital (Ethical Approval Number: I-23YJ187). Written informed consent was obtained from all the participants.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Hui Lian and Huacong Cai are co-first authors.
Funding
This study is supported by the National High Level Hospital Clinical Research Funding (2022-PUMCH-B-026).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Maslove DM, Tang B, Shankar-Hari M, et al. Redefining critical illness. Nat Med. 2022;28:1141–1148. doi:10.1038/s41591-022-01843-x
2. Liu S, Zhuge C, Zhang J, Cui N, Long Y. Simplified immune-dysregulation index: a novel marker predicts 28-day mortality of intensive care patients with sepsis. Shock. 2024;61(4):570–576. doi:10.1097/SHK.0000000000002316
3. Iba T, Levy JH. Inflammation and thrombosis: roles of neutrophils, platelets and endothelial cells and their interactions in thrombus formation during sepsis. J Thromb Haemost. 2018;16:231–241. doi:10.1111/jth.13911
4. Michels EHA, Butler JM, Reijnders TDY, et al. Association between age and the host response in critically ill patients with sepsis. Crit Care. 2022;26:385. doi:10.1186/s13054-022-04266-9
5. Hörber S, Prystupa K, Jacoby J, et al. Blood coagulation in Prediabetes clusters-impact on all-cause mortality in individuals undergoing coronary angiography. Cardiovasc Diabetol. 2024;23(1):306. doi:10.1186/s12933-024-02402-z
6. Kairies N, Beisel HG, Fuentes-Prior P, et al. The 2.0-A crystal structure of tachylectin 5A provides evidence for the common origin of the innate immunity and the blood coagulation systems. Proc Natl Acad Sci USA. 2001;98(24):13519–13524. doi:10.1073/pnas.201523798
7. Ochi A, Adachi T, Inokuchi K, et al. Effects of aging on the coagulation fibrinolytic system in outpatients of the cardiovascular department. Circ J. 2016;80:2133–2140. doi:10.1253/circj.CJ-16-0530
8. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines and the heart rhythm society in collaboration with the society of thoracic surgeons. Circulation. 2019;140:e125–e151. doi:10.1161/CIR.0000000000000665
9. Writing Group M, January CT, Wann LS, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a Report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines and the heart rhythm society. Heart Rhythm. 2019;16:e66–e93. doi:10.1016/j.hrthm.2019.01.024
10. Suzuki S, Yamashita T, Okumura K, et al. Incidence of ischemic stroke in Japanese patients with atrial fibrillation not receiving anticoagulation therapy--pooled analysis of the Shinken database, J-RHYTHM registry, and Fushimi AF registry. Circ J. 2015;79:432–438. doi:10.1253/circj.CJ-14-1131
11. van Vught LA, Uhel F, Ding C, et al. Consumptive coagulopathy is associated with a disturbed host response in patients with sepsis. J Thromb Haemost. 2021;19:1049–1063. doi:10.1111/jth.15246
12. Guidet B, Vallet H, Flaatten H, et al. The trajectory of very old critically ill patients. Intensive Care Med. 2024;50(2):181–194. doi:10.1007/s00134-023-07298-z
13. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:801–810. doi:10.1001/jama.2016.0287
14. Bermejo-Martin JF, Gonzalez-Rivera M, Almansa R, et al. Viral RNA load in plasma is associated with critical illness and a dysregulated host response in COVID-19. Crit Care. 2020;24:691. doi:10.1186/s13054-020-03398-0
15. Bhatraju PK, Morrell ED, Zelnick L, et al. Comparison of host endothelial, epithelial and inflammatory response in ICU patients with and without COVID-19: a prospective observational cohort study. Crit Care. 2021;25:148. doi:10.1186/s13054-021-03547-z
16. Shen Y, Cui N, Miao B, Zhao E. Immune dysregulation in patients with severe acute pancreatitis. Inflammation. 2011;34:36–42. doi:10.1007/s10753-010-9205-4
17. Liu W, Fan M, Lu W, Zhu W, Meng L, Lu S. Emerging roles of T helper cells in non-infectious neuroinflammation: savior or sinner. Front Immunol. 2022;13:872167. doi:10.3389/fimmu.2022.872167
18. Moro F, Pischiutta F, Portet A, et al. Ageing is associated with maladaptive immune response and worse outcome after traumatic brain injury. Brain Commun. 2022;4:fcac036. doi:10.1093/braincomms/fcac036
19. Huang W, Liu D, Zhang H, Ding X, Wang X. Critical care ultrasound study G. Focus on host/organ unregulated response: a common cause of critical illness. Chin Med J. 2023;136:108–110. doi:10.1097/CM9.0000000000002374
20. Lian H, Cai H, Zhang H, Ding X, Wang X, Zhang S. The prediction value of D-dimer on prognosis in intensive care unit among old patients (>/=65 years): a 9-year single-center retrospective study of 9261 cases. Oxid Med Cell Longev. 2022;2022:2238985. doi:10.1155/2022/2238985
21. Kabat GC, Kim MY, Verma AK, et al. Platelet count and total and cause-specific mortality in the women’s health initiative. Ann Epidemiol. 2017;27:274–280. doi:10.1016/j.annepidem.2017.02.001
22. Taylor EH, Marson EJ, Elhadi M, et al. Factors associated with mortality in patients with COVID-19 admitted to intensive care: a systematic review and meta-analysis. Anaesthesia. 2021;76:1224–1232. doi:10.1111/anae.15532
23. Sandfeld-Paulsen B, Aggerholm-Pedersen N, Winther-Larsen A. Pretreatment platelet count is a prognostic marker in lung cancer: a Danish registry-based cohort study. Clin Lung Cancer. 2023;24(2):175–183. doi:10.1016/j.cllc.2022.12.012
24. Monteiro ACC, Flori H, Dahmer MK, et al. Thrombomodulin is associated with increased mortality and organ failure in mechanically ventilated children with acute respiratory failure: biomarker analysis from a multicenter randomized controlled trial. Crit Care. 2021;25:271. doi:10.1186/s13054-021-03626-1
25. Lin JJ, Hsiao HJ, Chan OW, Wang Y, Hsia SH, Chiu CH. Increased serum thrombomodulin level is associated with disease severity and mortality in pediatric sepsis. PLoS One. 2017; 12:e0182324.
26. Liu Z, Li Y, Zhao Q, Kang Y. Association and predictive value of soluble thrombomodulin with mortality in patients with acute respiratory distress syndrome: systematic review and meta-analysis. Ann Transl Med. 2023;11:181. doi:10.21037/atm-23-432
27. Arai Y, Martin-Ruiz CM, Takayama M, et al. Inflammation, but not telomere length, predicts successful ageing at extreme old age: a longitudinal study of semi-supercentenarians. EBioMedicine. 2015;2:1549–1558. doi:10.1016/j.ebiom.2015.07.029
28. Gao D, Ni X, Fang S, et al. Exploration for the reference interval of C-reactive protein in the Chinese longevity people over 90 years of age. Diabetes Metab Syndr. 2023;17(8):102817. doi:10.1016/j.dsx.2023.102817
29. Salvioli S, Monti D, Lanzarini C, et al. Immune system, cell senescence, aging and longevity--inflamm-aging reappraised. Curr Pharm Des. 2013;19:1675–1679.
30. Montes-Worboys A, Rodriguez-Portal JA, Arellano-Orden E, Digon-Pereiras J, Rodriguez-Panadero F. Interleukin-8 activates coagulation and correlates with survival after talc pleurodesis. Eur Respir J. 2010;35:160–166. doi:10.1183/09031936.00146808
31. Reitsma PH, Rosendaal FR. Activation of innate immunity in patients with venous thrombosis: the Leiden Thrombophilia Study. J Thromb Haemost. 2004;2:619–622. doi:10.1111/j.1538-7836.2004.00689.x
32. Busch G, Seitz I, Steppich B, et al. Coagulation factor Xa stimulates interleukin-8 release in endothelial cells and mononuclear leukocytes: implications in acute myocardial infarction. Arterioscler Thromb Vasc Biol. 2005;25:461–466. doi:10.1161/01.ATV.0000151279.35780.2d
33. Levi M, van der Poll T. Inflammation and coagulation. Crit Care Med. 2010;38:S26–34. doi:10.1097/CCM.0b013e3181c98d21
34. Boehme MW, Deng Y, Raeth U, et al. Release of thrombomodulin from endothelial cells by concerted action of TNF-alpha and neutrophils: in vivo and in vitro studies. Immunology. 1996;87:134–140.
35. Forcina L, Franceschi C, Musaro A. The hormetic and hermetic role of IL-6. Ageing Res Rev. 2022;80:101697. doi:10.1016/j.arr.2022.101697
36. Wang KC, Li YH, Shi GY, et al. Membrane-bound thrombomodulin regulates macrophage inflammation in abdominal aortic aneurysm. Arterioscler Thromb Vasc Biol. 2015;35:2412–2422. doi:10.1161/ATVBAHA.115.305529
37. Manzoor A, Umme-e-Aiman, Maryam M. Understanding COVID-19: an overview of the virus, variants, vaccines, and treatment strategies. Diagnostics Ther. 2024;3(1):9–19. doi:10.55976/dt.3202412169-19
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.