")
Back to Journals » Journal of Inflammation Research » Volume 17
Inflammatory and Immune Mechanisms in COPD: Current Status and Therapeutic Prospects
Authors Qi Y, Yan Y , Tang D , Han J, Zhu X , Cui M, Wu H, Tao Y, Fan F
Received 16 May 2024
Accepted for publication 12 September 2024
Published 20 September 2024 Volume 2024:17 Pages 6603—6618
DOI https://doi.org/10.2147/JIR.S478568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Yanan Qi,1,2 Yuanyuan Yan,1,2 Dawei Tang,1,2 Jingjing Han,1,2 Xinyi Zhu,1,2 Mengting Cui,1,2 Hongyan Wu,3 Yu Tao,1,2 Fangtian Fan1,2
1School of Pharmacy, Bengbu Medical University, Bengbu, People’s Republic of China; 2Anhui Engineering Technology Research Center of Biochemical Pharmaceutical, Bengbu, People’s Republic of China; 3Institute of Biomedical Technology, Jiangsu Vocational College of Medicine, Yancheng, Jiangsu, 224005, People’s Republic of China
Correspondence: Yu Tao; Fangtian Fan, Anhui Engineering Technology Research Center of Biochemical Pharmaceutical Bengbu Medical College, 2600 Donghai Avenue, Bengbu, Anhui, 233003, People’s Republic of China, Tel +86-15852921284 ; +86-16655258065, Email [email protected]; [email protected]
Background: Chronic obstructive pulmonary disease (COPD) currently ranks among the top three causes of mortality worldwide, presenting as a prevalent and complex respiratory ailment. Ongoing research has underscored the pivotal role of immune function in the onset and progression of COPD. The immune response in COPD patients exhibits abnormalities, characterized by diminished anti-infection capacity due to immune senescence, heightened activation of neutrophils and macrophages, T cell infiltration, and aberrant B cell activity, collectively contributing to airway inflammation and lung injury in COPD.
Objective: This review aimed to explore the pivotal role of the immune system in COPD and its therapeutic potential.
Methods: We conducted a review of immunity and COPD published within the past decade in the Web of Science and PubMed databases, sorting through and summarizing relevant literature.
Results: This article examines the pivotal roles of the immune system in COPD. Understanding the specific functions and interactions of these immune cells could facilitate the development of novel therapeutic strategies and interventions aimed at controlling inflammation, enhancing immune function, and mitigating the impact of respiratory infections in COPD patients.
Keywords: COPD, immune system, inflammation, immune regulation
Introduction
Chronic Obstructive Pulmonary Disease (COPD) represents a diverse lung condition marked by persistent respiratory manifestations stemming from both airway and alveolar irregularities that result in sustained airflow limitation.1 This prevalent global ailment disproportionately affects developing nations.2,3 While early indications may be subtle, disease progression intensifies symptoms notably during physical exertion leading to substantial impairment in patient’s quality of life.4 Primary risk factors encompass tobacco smoke exposure (both active and passive smoking), environmental pollution (indoor and outdoor pollutants) as well as occupational hazards like dust or chemicals5,6 (Figure 1). Prolonged tobacco use stands out as the foremost contributor to COPD with approximately 80–90% cases linked to smoking.7,8 Typical signs comprise coughing fits accompanied by sputum production alongside dyspnea culminating in profound deterioration in overall well-being.9
 |
Figure 1 COPD related risk factors. The risk factors include cigarette, bacteria, particulate matter and viruses. |
The immune system serves as a vital biological defense mechanism that safeguards the human body against various pathogenic microorganisms.10 However, in patients with COPD, abnormal activation of immune cells and the release of immune mediators can exacerbate lung inflammation.11 Upon respiratory tract infection, the immune system promptly mobilizes to combat the invading pathogens.12 Innate immunity effectively eliminates infections by engulfing viruses, bacteria, and other microorganisms while enhancing inflammatory responses to aid in their clearance;13–15 adaptive immunity identifies, localizes, and eradicates specific pathogenic agents.16,17 Prolonged exposure to harmful gases and particulate matter in COPD patients results in increased airway wall thickness, lung function impairment, and alterations in immune function.18,19 Immune cells, particularly neutrophils and macrophages, often exist in a hyperactivated state producing elevated levels of inflammatory mediators which perpetuate an expanded inflammatory response.20,21 Additionally, intricate interactions occur between immune cells and oxidative damage: oxidative stress can activate immune cells leading to the release of inflammatory mediators;22,23 conversely, immune cells can generate oxygen free radicals and other oxidative substances contributing to further damage to lung tissue structure and function.24–26
Therefore, it is crucial to understand the role of the immune system in COPD prevention and treatment. This article begins by examining the significant role of the immune system in COPD progression. It then explored the relationship between COPD and immunity, offering new insights into potential directions for managing COPD.
Immunosenescence in COPD
COPD is a chronic inflammatory disease, with environmental factors, such as smoking and air pollution, being the leading causes of chronic inflammation.27–29 Chronic inflammation can damage the airway mucosal cells, increase mucus secretion, and impair respiratory function.30–32 In response to this damage, the immune system initiates a series of responses to defend against aggressive factors.10,12 Innate and adaptive immune responses build the body’s immune defense system, protecting it from infection and disease.16 However, immune aging exacerbates disease progression in patients with COPD.11 During aging, the immune system may experience imbalanced regulation, leading to overactivation or suppression of the inflammatory response.33,34 This imbalance can result in an attack on the lung tissue and exacerbate inflammation.35 Overall, the immune response in COPD is a complex process that involves interactions between multiple immune cells and inflammatory mediators (Figure 2).
 |
Figure 2 Immune response in COPD. Innate and adaptive immune responses build the body’s immune defense system. Immunosenescence exacerbates disease progression in patients with COPD. |
Inflammatory Response in the Lungs
When tobacco smoke, indoor and outdoor pollutants, dust, chemicals, etc., infiltrate the lungs or cause damage from various other irritants, the immune system triggers a cascade of inflammatory responses to counteract aggressive factors.36 For instance, IL-33, IL-25, and TSLP are released in response to stimuli-induced epithelial cell damage.37,38 ILC2s are innate immune cells that become activated and secrete proinflammatory type 2 cytokines such as IL-5 and IL-13 to recruit eosinophils and promote mucus production.39,40 Meanwhile, T helper cells—adaptive immune cells—are activated by dendritic cells in an antigen-dependent manner. Inflammation is a crucial immune response to harmful substances and pathogens and plays a significant role in the immune response to COPD.41 When pathogens or irritants enter the lungs and cause damage, the immune system initiates a series of inflammatory responses to defend against these aggressive factors.42 For example, when lung tissue is irritated or infected, immune cells release various inflammatory mediators, these mediators guide the migration of other immune cells to the site of inflammation, regulate the inflammatory response, and increase vascular permeability and mucus secretion.43 Increased vascular permeability allows plasma, platelets, and other immune cells to enter the site of inflammation, providing sufficient resources and immune cells to fight infection and repair damaged lung tissues.44 Alveolar macrophages are an essential type of immune cell in the lungs that specialize in clearing pathogens and damaging substances.45,46 They engulf and remove harmful substances during infection or injury, thereby releasing inflammatory mediators to activate other immune cells. The inflammatory response also plays a key role in triggering the repair and regeneration of the lung tissue.47–49 After resolving inflammation, immune cells release various growth factors and cytokines to promote the regeneration and repair of lung cells, which helps restore function and structure within damaged lung tissue (Figure 3).
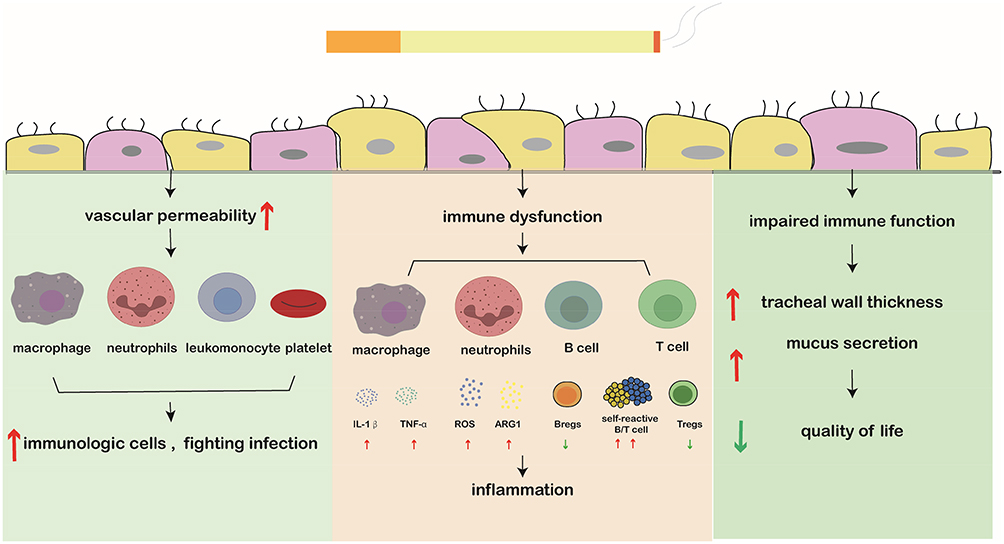 |
Figure 3 The autoimmune mechanism of COPD. Cigarette smoke induces lung damage, leading to increased vascular permeability. This allows the infiltration of macrophages, neutrophils, lymphocytes, and platelets into the inflammatory site, triggering a series of defense measures by the immune system. However, immune dysregulation has been observed in COPD patients, including the release of IL-1β and increased TNF-a from macrophages, as well as ROS and increased ARG1 from neutrophils. Additionally, there is an increase in autoreactive T and B cells and a decrease in immunosuppressive regulatory T and B cells which exacerbate inflammation. Due to impaired immune function, patients with COPD experience airway wall thickening and more frequent mucus secretion that significantly impacts their quality of life. |
In summary, the complex process of the inflammatory response in the lungs fights infections associated with respiratory system injuries through coordinated actions, including the release of inflammatory mediators, dilation and leakage from blood vessels, and promotion of tissue repair for effective defense mechanisms within the lungs.
Role of Innate Immunity and Adaptive Immune Responses
Upon exposure to external stimuli such as air pollution, harmful chemicals or infectious bacteria, COPD patients mount both innate and adaptive immune responses.50,51 The term “innate” refers to this type of immunity’s universal presence within the body along with its immediate action.52 Macrophages, natural killer cells, and phagocytes constitute key components of this defense mechanism against unfamiliar pathogens.53 When confronted with external threats, intrinsic immunity rapidly identifies and eliminates pathogens while also initiating an inflammatory reaction that aids in tissue repair.54,55 However, in individuals with COPD, this intrinsic immunity’s inflammatory response tends to be excessively activated. Exposure to hazardous substances triggers activation of macrophages, dendritic cells, and neutrophils within lung tissues, resulting in sustained inflammation, damage to airways.56,57 Oxidative stress induced by smoking or air pollutants leads to heightened production of free radicals.58 These free radicals not only directly harm lung tissue but also activate intrinsic immune cells, further exacerbating inflammatory responses.59
The adaptive immune system is distinguished by its high specificity, memory function, and is mediated by T cells, B cells, and other lymphocytes.60 Upon initial exposure to a specific pathogen, the adaptive immune system generates corresponding antibodies, T-cells for combating said pathogen.61,62 Moreover, it possesses memory capabilities, enabling faster, stronger responses upon subsequent encounters with identical pathogens. This attribute empowers our bodies’ ability fight infections form immune memory.63 In individuals suffering from COPD CD8+ T cells CD4+ T cell accumulate within lung tissues contributing towards airway inflammation. CD8+ T cells cause direct damage to tissue through attacks on lung epithelial cells with CD4+ T cell regulating inflammation via cytokine release.64,65 B cell produced antibodies may be linked to airway inflammation among those afflicted with COPD. Although the main etiology of COPD is long term harmful exposure, abnormal antibody production may also aggravate inflammatory responses in some patients.66
In summary, innate and adaptive immune responses collaborate to establish the body’s immune defense system, safeguarding it from infection and disease. Their unique strengths and characteristics complement each other, harmoniously upholding the immune balance and homeostasis of the body. In academic research, a comprehensive understanding of the mechanisms of action of innate and adaptive immunity is crucial for disease prevention, control, and immune regulation.55,59,64
Immune Aging in COPD Patients
Immunosenescence refers to age-related dysfunction of the immune system, which leads to decreased ability to combat infection and inflammation.63,67 This process is particularly significant in patients with COPD, as studies have shown that the production and function of immune cells may be abnormally regulated, resulting in an overreaction to inflammation that exacerbates respiratory inflammation and airway obstruction.36,66 With age, the function of immune cells, such as macrophages, T cells, and B cells, gradually declines in patients with COPD.68 The activity and sensitivity of these immune cells decrease, resulting in a reduced ability to fight infections and clear pathogens, making patients more susceptible to diseases and inflammatory responses.69 Immune aging also affects the memory function of immune cells in patients with COPD. Memory T and B cells of the adaptive immune system may be affected, thereby reducing the ability to recognize and respond to repeated infections.70 This makes patients more susceptible to repeated infections by the same pathogen or exacerbates their condition. Furthermore, immune aging can lead to chronic inflammation in patients with COPD, a prominent feature that contributes to disease progression.71 The slow inflammatory state induced by immune aging may exacerbate respiratory inflammation, oxidative stress, and airway remodeling. Given these implications for patient health outcomes, immunological intervention strategies targeting immune aging within this population have become increasingly important.72,73 According to the characteristics associated with immune aging, some intervention measures can be taken, including improving activity levels among key immune cell types, promoting balance within regulatory mechanisms, strengthening vaccination protocols, and enhancing overall immunity through improved memory functions, all aimed at reducing inflammatory responses while controlling disease progression.74,75
Role of Immune Cells and Mediators in COPD
In COPD, various immune cells and mediators are involved in the inflammatory responses and immune regulation.76 The first were macrophages and neutrophils, which are among of the earliest immune cells involved in the inflammatory response.77 Macrophages are among the initial immune cells that respond to inflammation. In COPD, irritants, such as smoking and air pollution, induce lung inflammation, activating macrophages to release inflammatory mediators, such as IL-1β and TNF-α, which subsequently trigger an inflammatory response.78,79 Inflammatory mediators, such as elastase, released by neutrophils can lead to airway tissue destruction; the resulting reactive oxygen species (ROS) can further exacerbate oxidative stress and promote airway inflammation and damage.80 Second, T lymphocytes play a crucial role in the immune response in COPD patients.81 T cells consist of CD4+ helper T cells and CD8+ cytotoxic T cells, which regulate the inflammatory response and maintain immune balance by secreting cytokines and activating other immune cells.80,82,83 Additionally, B lymphocytes contribute to COPD by producing antibodies that neutralize pathogens and antigens while participating in the fight against inflammation.84 In addition to these immune cells and these inflammatory mediators, chemokines, leukocyte adhesion molecules, and humoral factors regulate and participate in inflammatory responses.85 In conclusion, complex interactions exist between immune cells and mediators in COPD pathogenesis, which regulate the inflammatory response and maintain the immune balance, thereby influencing disease development and progression86 (Figure 4).
 |
Figure 4 Role of immune cells and mediators in COPD. (A) Neutrophils and macrophages play crucial roles in immune responses. (B) TNF-αand IL-1 increase vascular permeability. IL-8 cooperatively increases vascular permeability and recruit neutrophils. (C) Neutrophils and macrophages phagocytose pathogens. Damaged tissue is removed by proteolytic enzymatic digestion. (D) Mechanisms of T cell and B cell. |
Neutrophils and Macrophages
Neutrophils and macrophages play an important role in the development and inflammatory process of COPD.87,88 Neutrophils release a large number of proinflammatory cytokines, such as interleukin-8 (IL-8) and TNF-α, which can recruit more inflammatory cells to the airway and further aggravate inflammation.89 They secrete enzymes, such as elastase, collagenase and acid phosphatase, which can disrupt airway structure and function, leading to airway remodeling and tissue damage.90,91 Neutrophils produce large amounts of reactive oxygen species, which can oxidize cells and tissues, leading to oxidative stress and inflammation.92 ROS production is not only directly toxic to airway epithelial cells, but also aggravates airway inflammation.93,94 Elastase and other proteases released by neutrophils break down components of the extracellular matrix (ECM), leading to destruction of airway walls and airway remodeling.95,96 This tissue destruction is one of the important features of COPD.95,97 Macrophages are normally responsible for engulfing and removing harmful substances from the body, such as bacteria, viruses, and inhaled particles.98 In COPD patients, macrophages release large amounts of proinflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), interleukin-6 (IL-6), and interleukin-8 (IL-8) in the airways of COPD patients due to long-term exposure to tobacco smoke and other harmful substances.99 These factors are able to enhance the inflammatory response and recruit other inflammatory cells such as neutrophils to the airway, thereby exacerbating inflammation and tissue damage.100 Chemokines released by macrophages, such as CCL2 and CXCL8, promote the migration and accumulation of inflammatory cells, which lead to persistent inflammation and injury of the airways.101 One of the major roles of macrophages in COPD is to maintain the chronic inflammatory state of the airways.102 They maintain an inflammatory environment within the airways through the continuous release of inflammatory mediators and cytokines. It is more inclined to secrete proinflammatory cytokines and enzymes, which further aggravates airway inflammation and tissue damage. Macrophages secrete a variety of enzymes, such as elastase and metalloproteinase, which can decompose important components of the extracellular matrix (ECM), such as elastin and collagen.103,104 This destructive effect leads to airway wall damage and remodeling, which further aggravates the condition of COPD.105 Macrophages in COPD not only participate in the inflammatory response by secreting proinflammatory cytokines, but also may regulate the immune response by secreting anti-inflammatory factors such as IL-10 and transforming growth factor-beta (TGF-β).106 However, this regulation may be out of balance in COPD, leading to persistent inflammatory responses.107
Although neutrophils and macrophages play an essential role in COPD development, an overactivated and dysregulated immune response can also cause inflammation and tissue damage. Therefore, it is essential to balance and control the activity of neutrophils and macrophages for treating COPD.108
T Cells and B Cells
T lymphocytes and B lymphocytes provide specific immune protection by recognizing and eliminating pathogens and other harmful substances.109,110 These two types of adaptive immune cells are crucial for the immune response in COPD.111 T cells, an essential part of the adaptive immune system, can be divided into CD4+ helper T cells and CD8+ helper T cells. They are involved in immune regulation and the regulation of inflammation in COPD.112 The CD4+ helper T cells can differentiate into different subpopulations, such as Th1, Th2, Th17, and regulatory T cells (Treg cells).113 In COPD, there is an increase in the activity of Th1 and Th17 cells, leading to the production of cytokines, such as interferon-gamma (IFN-γ), from Th1 cells that stimulate inflammatory responses and cell damage.114 Additionally, IL-17 produced by Th17 cells can lead to inflammation by stimulating the production of GM-CSF and CAM-1. Furthermore, Th2 cells contribute to excessive pathological remodeling of the respiratory tract, leading to airway obstruction, whereas the weakened function of Treg cells results in reduced immune tolerance and immune dysregulation.115 B cells are another important component of the adaptive immune system that produces antibodies and participates in antibody-mediated immune responses. When activated, B cells differentiate into plasma cells that produce large quantities of clear pathogens.116 In COPD, B cell activity increases, resulting in increased antibody production. Although antibodies play a role in pathogen clearance, it is essential to note that overactivated B cells may overproduce antibodies, leading to an autoimmune response.84 B cells can also release cytokines and inflammatory mediators, further promoting the development of an inflammatory response.117 In a chronic inflammatory state, such as COPD, the activity of B cells may increase, further stimulating the inflammatory response and oxidative stress.118
In COPD treatment, immunomodulatory strategies focusing on regulating the activity of T and B cells are anticipated to alleviate the inflammatory response and oxidative stress in COPD, thereby reducing symptoms and delaying disease progression.119 Immunosuppressants, including those that inhibit T cell activity, can help reduce inflammatory lesions caused by immune response overactivation.120 Regulating the Th1/Th2/Th17/Treg balance is expected to decrease inflammation in COPD.121 Antibody drugs may also selectively interfere with B cell activity, reducing antibody production and the release of inflammatory mediators.122 Collectively, T and B cells play important roles in the pathogenesis and inflammatory processes of COPD.123 Therefore, immune regulation and antioxidant therapy may be crucial in COPD treatment.124 Balancing the immune response, inhibiting the overactivation of inflammation, and alleviating oxidative stress are expected to improve symptoms and quality of life in patients with COPD while delaying disease progression.125,126 This approach provides new ideas for personalized treatment in this field.127
The Treatment Strategy for COPD
While current treatments for COPD effectively manage symptoms and slow disease progression, they possess inherent limitations.128 In contrast, emerging immunotherapy presents distinct advantages by targeting specific inflammatory mediators or cells with precision to mitigate airway inflammation more effectively than conventional medications like bronchodilators or inhaled glucocorticoids which only alleviate symptoms without reversing or curing COPD entirely.129,130 Furthermore, the variable efficacy of these medications among individuals underscores their limited impact on certain patients due to inadequate consideration of individual immune status and pathological features during treatment selection.131,132 Immunotherapy holds promise in regulating immunity with greater specificity, potentially reducing both frequency and severity of acute exacerbations while enhancing overall quality of life through improved immune function in managing infections and injuries133 (Figure 5).
 |
Figure 5 The treatment strategy for COPD. (A)The normal lung, trachea, and alveoli were compared with those of COPD patients. On the left are the lung, trachea, and alveoli of the COPD patient, while the normal tissues are shown on the right. (B) Therapeutic interventions that reduce COPD mortality. |
Current Treatment Options for COPD
According to the 2024 guidelines from the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD), the management of chronic obstructive pulmonary disease (COPD) focuses on personalized treatment, symptom control, enhanced quality of life, and reduced acute exacerbations.134 Smoking cessation stands as the foremost measure in COPD treatment.135 Irrespective of the patient’s disease stage, smoking cessation is imperative for enhancing lung function, alleviating symptoms, and slowing disease progression.136 Pulmonary rehabilitation encompasses tailored exercise training, education, and nutritional guidance to enhance exercise capacity, symptom management, and quality of life.137 Long-term oxygen therapy enhances both quality of life and survival in patients with persistent hypoxemia.138,139 Pharmacotherapy is individualized based on symptom severity and risk of acute exacerbation140 (Table 1). While long-term use of inhaled glucocorticoids can mitigate inflammation, it may also lead to side effects such as oral candidiasis, osteoporosis, and diabetes.141 Prolonged use of certain medications may result in systemic side effects that could impact a patient’s long-term health.142 Despite medical therapy reducing exacerbation frequency overall; some patients with severe disease still experience frequent exacerbations leading to a significant decline in their quality of life.143,144 Patients with COPD often have comorbidities (cardiovascular disease or diabetes) that may not be adequately managed by current treatment options.145
 |
Table 1 Commonly Used Maintenance Medications in COPD |
Role of Immune Regulation in COPD Treatment
Immune regulation is crucial in treating COPD and can affect disease development and progression by controlling inflammatory responses, cellular immunity, and oxidative stress.146 The chronic inflammatory response in COPD is central to its development. The over-activated inflammatory response destroys lung tissue, increases mucus secretion, worsens patient symptoms, and decreases lung function. Immune regulation can reduce the degree of inflammatory response by inhibiting the release of inflammatory mediators and regulating the activity of inflammatory cells, thereby improving lung symptoms and patients’ quality of life.68 T cells play a significant role in the immunopathological processes of COPD. Immune regulation can influence T-cell differentiation and function, increase Tregs, inhibit the activity of inflammatory T cells (Th1 and Th17 cells), balance cellular immune processes, and reduce the intensity of the inflammatory response.103 Oxidative stress also plays a critical role in COPD pathogenesis and development by causing damage to the lung tissue through oxygen free radicals, which accelerate the decline in lung function.147 Oxidative stress is a pivotal factor in COPD pathogenesis by inducing oxidative damage to lung tissue through oxygen free radicals which accelerates pulmonary function decline.108 Immunoregulation has potential for mitigating oxidative stress progression while safeguarding against free radical-induced injury via antioxidant supplementation like vitamin C and vitamin E.26 Tailoring immunomodulatory interventions based on individual immune status and disease characteristics is crucial for optimizing therapeutic outcomes in COPD management.70 Immune monitoring and assessment enable selection of tailored immunomodulatory therapies that enhance efficacy while minimizing adverse effects.46 Overall, immunomodulation significantly impacts COPD treatment by modulating inflammatory response, cellular immunity and oxidative stress thereby reducing disease burden while enhancing pulmonary function and quality-of-life whilst lowering acute exacerbation risks.148,149
Summary and Discussion
COPD is a complex disease involving airway inflammation, airflow limitation and immune dysfunction.150 Although current treatment methods include bronchodilators and anti-inflammatory drugs, there are still many patients who do not achieve satisfactory results. Therefore, immunotherapy for COPD patients has gradually attracted wide attention.7,151 The application of immunotherapy in COPD has some potential advantages, which are different from traditional treatment methods and can provide new treatment options in specific clinical scenarios.152 First of all, understanding the specific functions of immune cells and their roles in the inflammatory process can provide a basis for the selection of appropriate immunotherapy strategies. For example, inhibition of proinflammatory cytokines such as TNF-α and IL-6 may help to alleviate the inflammatory response of COPD.153 The development of biological agents targeting specific immune cells or signaling pathways may become an important direction for the treatment of COPD in the future. Secondly, the immune status of COPD patients varies significantly, so individualized immunotherapy is particularly important. By assessing the patient’s immune function, inflammatory markers, and disease severity, more precise treatment can be developed to improve the efficacy and reduce side effects. Immunotherapy can target specific biomarkers or signaling pathways that play a key role in inflammation and disease progression in COPD.154 By precisely targeting these pathways, immunotherapy can reduce side effects and improve therapeutic efficacy. Finally, some immunotherapies, such as monoclonal antibody injections, can be administered in a clinic or home setting, which improves patient adherence to treatment. Traditional treatment of COPD often relies on inhalers, which may cause pharyngitis, oral microbial changes and other related side effects. Immunotherapy can reduce the dependence on these agents and the associated side effects.
The utilization of immunotherapy in the management of COPD holds significant promise, yet it also confronts numerous challenges.51 Firstly, the chronic inflammation associated with COPD is not solely driven by immune cells but is also influenced by environmental factors (such as smoking and air pollution) and genetic factors.18 Consequently, a singular immunotherapy approach may prove insufficient in addressing all inflammatory mechanisms. Secondly, the long-term efficacy and safety of immunotherapy necessitate validation through extensive clinical trials.155 The majority of current studies have focused on short-term effects, leaving the long-term effects ambiguous.156 Different types of immunotherapy may yield varying effects within distinct patient populations.51 The accurate assessment and optimization of these diverse therapeutic effects remain an ongoing challenge.157 Lastly, newer immunotherapies often entail higher costs, posing a financial burden for certain patient groups. Addressing this issue requires finding ways to reduce treatment costs while ensuring efficacy.158
In conclusion, the immune system plays a crucial role in the pathogenesis of COPD, and immunotherapy holds significant promise for its treatment. While current research is still exploratory, a comprehensive understanding of immune system function, personalized treatment strategies, and targeted immune pathway investigations are anticipated to offer new therapeutic prospects for COPD patients. Future research and clinical practice should prioritize addressing these challenges and integrating immunomodulation with drug therapy to enhance efficacy and improve patient quality of life. Advancements in this area will contribute to enhancing the quality of life for COPD patients and reducing disease burden.
Data Sharing Statement
We confirm that the data supporting the findings of this study are available within the publicly available data, ensuring transparency and accessibility for further analysis and verification by interested parties.
The data that support the findings of this study are available at the following URL:
https://www.ncbi.nlm.nih.gov/search/all/?term=COPD
https://webofscience.clarivate.cn/wos/woscc/basic-search
Example from:
https://pubmed.ncbi.nlm.nih.gov/36794439/
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant/Award Numbers: 81973658, 82274339, 82104487); Bengbu Medical College Major Science and Technology Project Incubation Program (Grant/Award Numbers: 2020byfy001); Jiangsu Province Engineering Research Center for Cardiovascular and Cerebrovascular Disease and Cancer Prevention and Control (2022); University Natural Science Research Project of Anhui Province (Grant/Award Numbers: 2023AH051972); Jiangsu Higher Education Institution Innovative Research Team For Science and Technology (2023). Excellent scientific research and innovation team project of Anhui Province (Grant/Award Numbers: 2022AH010084).
Disclosure
The authors declare no conflict of interest. The funders had no role in the design of the study, collection, analyses, or interpretation of data, writing of the manuscript, or in the decision to publish the manuscript.
References
1. Global Strategy for the Diagnosis. Global strategy for the diagnosis, management, and prevention of COPD 2024 Report; 2024.
2. Janjua S, Fortescue R, Poole P. Phosphodiesterase-4 inhibitors for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2020;5(5):CD002309. doi:10.1002/14651858.CD002309.pub6
3. Barnes PJ, Burney PG, Silverman EK, et al. Chronic obstructive pulmonary disease. Nat Rev Dis Primers. 2015;1:15076. doi:10.1038/nrdp.2015.76
4. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/S0140-6736(17)31222-9
5. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
6. Venkatesan P. GOLD COPD report: 2024 update. Lancet Respir Med. 2024;12(1):15–16. doi:10.1016/S2213-2600(23)00461-7
7. Fabbri LM, Celli BR, Agustí A, et al. COPD and multimorbidity: recognising and addressing a syndemic occurrence. Lancet Respir Med. 2023;11(11):1020–1034. doi:10.1016/S2213-2600(23)00261-8
8. Lareau SC, Fahy B, Meek P, Wang A. Chronic obstructive pulmonary disease (COPD). Am J Respir Crit Care Med. 2019;199(1):P1–1P2. doi:10.1164/rccm.1991P1
9. Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
10. Brodin P, Davis MM. Human immune system variation. Nat Rev Immunol. 2017;17(1):21–29. doi:10.1038/nri.2016.125
11. Bhat TA, Panzica L, Kalathil SG, Thanavala Y. Immune dysfunction in patients with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2015;12(Suppl Supplement 2):S169–75. doi:10.1513/AnnalsATS.201503-126AW
12. Netea MG, Domínguez-Andrés J, Barreiro LB, et al. Defining trained immunity and its role in health and disease. Nat Rev Immunol. 2020;20(6):375–388. doi:10.1038/s41577-020-0285-6
13. Mettelman RC, Allen EK, Thomas PG. Mucosal immune responses to infection and vaccination in the respiratory tract. Immunity. 2022;55(5):749–780. doi:10.1016/j.immuni.2022.04.013
14. Zhang Q, Cao X. Epigenetic remodeling in innate immunity and inflammation. Annu Rev Immunol. 2021;39:279–311. doi:10.1146/annurev-immunol-093019-123619
15. Ravesloot-Chávez MM, Van Dis E, Stanley SA. The innate immune response to mycobacterium tuberculosis infection. Annu Rev Immunol. 2021;39:611–637. doi:10.1146/annurev-immunol-093019-010426
16. Netea MG, Schlitzer A, Placek K, Joosten L, Schultze JL. Innate and adaptive immune memory: an evolutionary continuum in the host’s response to pathogens. Cell Host Microbe. 2019;25(1):13–26. doi:10.1016/j.chom.2018.12.006
17. Molofsky AB, Locksley RM. The ins and outs of innate and adaptive type 2 immunity. Immunity. 2023;56(4):704–722. doi:10.1016/j.immuni.2023.03.014
18. Cho SJ, Stout-Delgado HW. Aging and lung disease. Annu Rev Physiol. 2020;82:433–459. doi:10.1146/annurev-physiol-021119-034610
19. Bhatt SP, Nakhmani A, Fortis S, et al. FEV(1)/FVC severity stages for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2023;208(6):676–684. doi:10.1164/rccm.202303-0450OC
20. Rabe KF, Rennard S, Martinez FJ, et al. Targeting type 2 inflammation and epithelial alarmins in chronic obstructive pulmonary disease: a biologics outlook. Am J Respir Crit Care Med. 2023;208(4):395–405. doi:10.1164/rccm.202303-0455CI
21. Christenson SA, van den Berge M, Faiz A, et al. An airway epithelial IL-17A response signature identifies a steroid-unresponsive COPD patient subgroup. J Clin Invest. 2019;129(1):169–181. doi:10.1172/JCI121087
22. Zhang Z, Zhao L, Zhou X, Meng X, Zhou X. Role of inflammation, immunity, and oxidative stress in hypertension: new insights and potential therapeutic targets. Front Immunol. 2022;13:1098725. doi:10.3389/fimmu.2022.1098725
23. Menzel M, Ramu S, Calvén J, et al. Oxidative stress attenuates TLR3 responsiveness and impairs anti-viral mechanisms in bronchial epithelial cells from COPD and asthma patients. Front Immunol. 2019;10:2765. doi:10.3389/fimmu.2019.02765
24. Wang L, Cai Y, Garssen J, Henricks P, Folkerts G, Braber S. The bidirectional gut-lung axis in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2023;207(9):1145–1160. doi:10.1164/rccm.202206-1066TR
25. Lewis BW, Ford ML, Rogers LK, Britt RD. Oxidative stress promotes corticosteroid insensitivity in asthma and COPD. Antioxidants. 2021;10(9):1335. doi:10.3390/antiox10091335
26. Cazzola M, Page CP, Wedzicha JA, Celli BR, Anzueto A, Matera MG. Use of thiols and implications for the use of inhaled corticosteroids in the presence of oxidative stress in COPD. Respir Res. 2023;24(1):194. doi:10.1186/s12931-023-02500-8
27. MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirology. 2021;26(6):532–551. doi:10.1111/resp.14041
28. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global burden of disease study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
29. Yang IA, Jenkins CR, Salvi SS. Chronic obstructive pulmonary disease in never-smokers: risk factors, pathogenesis, and implications for prevention and treatment. Lancet Respir Med. 2022;10(5):497–511. doi:10.1016/S2213-2600(21)00506-3
30. Singanayagam A, Footitt J, Marczynski M, et al. Airway mucins promote immunopathology in virus-exacerbated chronic obstructive pulmonary disease. J Clin Invest. 2022;132(8):e120901. doi:10.1172/JCI120901
31. Wiegman CH, Li F, Ryffel B, Togbe D, Chung KF. Oxidative stress in ozone-induced chronic lung inflammation and emphysema: a facet of chronic obstructive pulmonary disease. Front Immunol. 2020;11:1957. doi:10.3389/fimmu.2020.01957
32. Sevilla-Montero J, Labrousse-Arias D, Fernández-Pérez C, et al. Cigarette smoke directly promotes pulmonary arterial remodeling and Kv7.4 channel dysfunction. Am J Respir Crit Care Med. 2021;203(10):1290–1305. doi:10.1164/rccm.201911-2238OC
33. Yousefzadeh MJ, Flores RR, Zhu Y, et al. An aged immune system drives senescence and ageing of solid organs. Nature. 2021;594(7861):100–105. doi:10.1038/s41586-021-03547-7
34. Snijckers R, Foks AC. Adaptive immunity and atherosclerosis: aging at its crossroads. Front Immunol. 2024;15:1350471. doi:10.3389/fimmu.2024.1350471
35. Li J, Zhao L, Zhang Y, et al. Imbalanced immune responses involving inflammatory molecules and immune-related pathways in the lung of acute and subchronic arsenic-exposed mice. Environ Res. 2017;159:381–393. doi:10.1016/j.envres.2017.08.036
36. Schneider JL, Rowe JH, Garcia-de-Alba C, Kim CF, Sharpe AH, Haigis MC. The aging lung: physiology, disease, and immunity. Cell. 2021;184(8):1990–2019. doi:10.1016/j.cell.2021.03.005
37. Yan J, Horng T. Lipid metabolism in regulation of macrophage functions. Trends Cell Biol. 2020;30(12):979–989. doi:10.1016/j.tcb.2020.09.006
38. Solis AG, Bielecki P, Steach HR, et al. Mechanosensation of cyclical force by PIEZO1 is essential for innate immunity. Nature. 2019;573:7772):69–74. doi:10.1038/s41586-019-1485-8
39. Noval Rivas M, Wakita D, Franklin MK, et al. Intestinal Permeability and IgA provoke immune vasculitis linked to cardiovascular inflammation. Immunity. 2019;51(3):508–21.e6. doi:10.1016/j.immuni.2019.05.021
40. Hoang ON, Ermund A, Jaramillo AM, et al. Mucins MUC5AC and MUC5B are variably packaged in the same and in separate secretory granules. Am J Respir Crit Care Med. 2022;206(9):1081–1095. doi:10.1164/rccm.202202-0309OC
41. Borek I, Birnhuber A, Voelkel NF, Marsh LM, Kwapiszewska G. The vascular perspective on acute and chronic lung disease. J Clin Invest. 2023;133(16):e170502. doi:10.1172/JCI170502
42. Aegerter H, Lambrecht BN, Jakubzick CV. Biology of lung macrophages in health and disease. Immunity. 2022;55(9):1564–1580. doi:10.1016/j.immuni.2022.08.010
43. Joshi N, Walter JM, Misharin AV. Alveolar Macrophages. Cell Immunol. 2018;330:86–90. doi:10.1016/j.cellimm.2018.01.005
44. Dikiy S, Rudensky AY. Principles of regulatory T cell function. Immunity. 2023;56(2):240–255. doi:10.1016/j.immuni.2023.01.004
45. Eming SA, Wynn TA, Martin P. Inflammation and metabolism in tissue repair and regeneration. Science. 2017;356(6342):1026–1030. doi:10.1126/science.aam7928
46. Wang Y, Wang L, Ma S, Cheng L, Yu G. Repair and regeneration of the alveolar epithelium in lung injury. FASEB J. 2024;38(8):e23612. doi:10.1096/fj.202400088R
47. Mikami Y, Grubb BR, Rogers TD, et al. Chronic airway epithelial hypoxia exacerbates injury in muco-obstructive lung disease through mucus hyperconcentration. Sci Transl Med. 2023;15(699):eabo7728. doi:10.1126/scitranslmed.abo7728
48. Hill DB, Button B, Rubinstein M, Boucher RC. Physiology and pathophysiology of human airway mucus. Physiol Rev. 2022;102(4):1757–1836. doi:10.1152/physrev.00004.2021
49. Quinton LJ, Walkey AJ, Mizgerd JP. Integrative physiology of pneumonia. Physiol Rev. 2018;98(3):1417–1464. doi:10.1152/physrev.00032.2017
50. Feredj E, Wiedemann A, Krief C, et al. Immune response to pertussis vaccine in COPD patients. Sci Rep. 2023;13(1):11654. doi:10.1038/s41598-023-38355-8
51. Kapellos TS, Conlon TM, Yildirim AÖ, Lehmann M. The impact of the immune system on lung injury and regeneration in COPD. Eur Respir J. 2023;62(4):2300589. doi:10.1183/13993003.00589-2023
52. Alisjahbana A, Mohammad I, Gao Y, Evren E, Ringqvist E, Willinger T. Human macrophages and innate lymphoid cells: tissue-resident innate immunity in humanized mice. Biochem Pharmacol. 2020;174:113672. doi:10.1016/j.bcp.2019.113672
53. Xue D, Lu S, Zhang H, et al. Induced pluripotent stem cell-derived engineered T cells, natural killer cells, macrophages, and dendritic cells in immunotherapy. Trends Biotechnol. 2023;41(7):907–922. doi:10.1016/j.tibtech.2023.02.003
54. Cortesi F, Delfanti G, Casorati G, Dellabona P. The pathophysiological relevance of the inkt cell/mononuclear phagocyte crosstalk in tissues. Front Immunol. 2018;9:2375. doi:10.3389/fimmu.2018.02375
55. Meyer M, Schwärzler J, Jukic A, Tilg H. Innate Immunity and MASLD. Biomolecules. 2024;14(4):476. doi:10.3390/biom14040476
56. DeMaio A, Mehrotra S, Sambamurti K, Husain S. The role of the adaptive immune system and T cell dysfunction in neurodegenerative diseases. J Neuroinflammation. 2022;19(1):251. doi:10.1186/s12974-022-02605-9
57. Zhang E, Ma Z, Lu M. Contribution of T- and B-cell intrinsic toll-like receptors to the adaptive immune response in viral infectious diseases. Cell Mol Life Sci. 2022;79(11):547. doi:10.1007/s00018-022-04582-x
58. Sadeghi M, Divangahi M. Discovering adaptive features of innate immune memory. Immunol Rev. 2024. doi:10.1111/imr.13328
59. Deets KA, Vance RE. Inflammasomes and adaptive immune responses. Nat Immunol. 2021;22(4):412–422. doi:10.1038/s41590-021-00869-6
60. Yan L, Wu X, Wu P, et al. Increased expression of Clec9A on cDC1s associated with cytotoxic CD8(+) T cell response in COPD. Clin Immunol. 2022;242:109082. doi:10.1016/j.clim.2022.109082
61. Eyraud E, Maurat E, Sac-Epée JM, et al. Short-range interactions between fibrocytes and CD8(+) T cells in COPD bronchial inflammatory response. Elife. 2023;12:RP85875. doi:10.7554/eLife.85875
62. Hou J, Wang X, Su C, et al. Reduced frequencies of Foxp3(+)GARP(+) regulatory T cells in COPD patients are associated with multi-organ loss of tissue phenotype. Respir Res. 2022;23(1):176. doi:10.1186/s12931-022-02099-2
63. Liu Z, Liang Q, Ren Y, et al. Immunosenescence: molecular mechanisms and diseases. Signal Transduct Target Ther. 2023;8(1):200. doi:10.1038/s41392-023-01451-2
64. Yaugel-Novoa M, Bourlet T, Paul S. Role of the humoral immune response during COVID-19: guilty or not guilty. Mucosal Immunol. 2022;15(6):1170–1180. doi:10.1038/s41385-022-00569-w
65. Shirai T, Nakai A, Ando E, et al. Celastrol suppresses humoral immune responses and autoimmunity by targeting the COMMD3/8 complex. Sci Immunol. 2023;8(81):eadc9324. doi:10.1126/sciimmunol.adc9324
66. Barnes PJ. Pulmonary Diseases and Ageing. Subcell Biochem. 2019;91:45–74. doi:10.1007/978-981-13-3681-2_3
67. Wang Y, Dong C, Han Y, Gu Z, Sun C. Immunosenescence, aging and successful aging. Front Immunol. 2022;13:942796. doi:10.3389/fimmu.2022.942796
68. Barnes PJ, Baker J, Donnelly LE. Cellular senescence as a mechanism and target in chronic lung diseases. Am J Respir Crit Care Med. 2019;200(5):556–564. doi:10.1164/rccm.201810-1975TR
69. Wan R, Srikaram P, Xie S, et al. PPARγ attenuates cellular senescence of alveolar macrophages in asthma-COPD overlap. Respir Res. 2024;25(1):174. doi:10.1186/s12931-024-02790-6
70. Dowery R, Benhamou D, Benchetrit E, et al. Peripheral B cells repress B-cell regeneration in aging through a TNF-α/IGFBP-1/IGF-1 immune-endocrine axis. Blood. 2021;138(19):1817–1829. doi:10.1182/blood.2021012428
71. Zhong S, Yang L, Liu N, et al. Identification and validation of aging-related genes in COPD based on bioinformatics analysis. Aging. 2022;14(10):4336–4356. doi:10.18632/aging.204064
72. Borgoni S, Kudryashova KS, Burka K, De Magalhães JP. Targeting immune dysfunction in aging. Ageing Res Rev. 2021;70:101410. doi:10.1016/j.arr.2021.101410
73. Jia M, Agudelo Garcia PA, Ovando-Ricardez JA, et al. Transcriptional changes of the aging lung. Aging Cell. 2023;22(10):e13969. doi:10.1111/acel.13969
74. Cevirgel A, Shetty SA, Vos M, et al. Identification of aging-associated immunotypes and immune stability as indicators of post-vaccination immune activation. Aging Cell. 2022;21(10):e13703. doi:10.1111/acel.13703
75. Bloom DE, Pecetta S, Scorza FB, et al. Vaccination for healthy aging. Sci Transl Med. 2024;16(745):eadm9183. doi:10.1126/scitranslmed.adm9183
76. Wang D, Chen B, Bai S, Zhao L. Screening and identification of tissue-infiltrating immune cells and genes for patients with emphysema phenotype of COPD. Front Immunol. 2022;13:967357. doi:10.3389/fimmu.2022.967357
77. Fan P, Zhang Y, Ding S, Du Z, Zhou C, Du X. Integrating RNA-seq and scRNA-seq to explore the mechanism of macrophage ferroptosis associated with COPD. Front Pharmacol. 2023;14:1139137. doi:10.3389/fphar.2023.1139137
78. Ciminieri C, Woest ME, Reynaert NL, et al. IL-1β induces a proinflammatory fibroblast microenvironment that impairs lung progenitors’ function. Am J Respir Cell Mol Biol. 2023;68(4):444–455. doi:10.1165/rcmb.2022-0209OC
79. Shyam Prasad Shetty B, Chaya SK, Kumar VS, et al. Inflammatory biomarkers interleukin 1 beta (IL-1β) and tumour necrosis factor alpha (TNF-α) are differentially elevated in tobacco smoke associated COPD and biomass smoke associated COPD. Toxics. 2021;9(4):72. doi:10.3390/toxics9040072
80. Villaseñor-Altamirano AB, Jain D, Jeong Y, et al. Activation of CD8(+) T cells in chronic obstructive pulmonary disease lung. Am J Respir Crit Care Med. 2023;208(11):1177–1195. doi:10.1164/rccm.202305-0924OC
81. Thomas R, Qiao S, Yang X. Th17/treg imbalance: implications in lung inflammatory diseases. Int J Mol Sci. 2023;24(5):4865. doi:10.3390/ijms24054865
82. Gémes N, Balog JÁ, Neuperger P, et al. Single-cell immunophenotyping revealed the association of CD4+ central and CD4+ effector memory T cells linking exacerbating chronic obstructive pulmonary disease and NSCLC. Front Immunol. 2023;14:1297577. doi:10.3389/fimmu.2023.1297577
83. Peng T. Bad neighbors or bad neighborhoods: pathogenic residency of T cells in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2023;208(11):1148–1150. doi:10.1164/rccm.202310-1760ED
84. Rojas-Quintero J, Ochsner SA, New F, et al. Spatial transcriptomics resolve an emphysema-specific lymphoid follicle b cell signature in COPD. Am J Respir Crit Care Med. 2023. doi:10.1164/rccm.202303-0507OC
85. Harel M, Fauteux-Daniel S, Girard-Guyonvarc’h C, Gabay C. Balance between Interleukin-18 and Interleukin-18 binding protein in auto-inflammatory diseases. Cytokine. 2022;150:155781. doi:10.1016/j.cyto.2021.155781
86. Kaplanski G. Interleukin-18: biological properties and role in disease pathogenesis. Immunol Rev. 2018;281(1):138–153. doi:10.1111/imr.12616
87. Lan CC, Su WL, Yang MC, Chen SY, Wu YK. Predictive role of neutrophil-percentage-to-albumin, neutrophil-to-lymphocyte and eosinophil-to-lymphocyte ratios for mortality in patients with COPD: evidence from NHANES 2011–2018. Respirology. 2023;28(12):1136–1146. doi:10.1111/resp.14589
88. Lokwani R, Wark PA, Baines KJ, Fricker M, Barker D, Simpson JL. Blood neutrophils in COPD but not asthma exhibit a primed phenotype with downregulated CD62L expression. Int J Chron Obstruct Pulmon Dis. 2019;14:2517–2525. doi:10.2147/COPD.S222486
89. Pournaras N, Andersson A, Kovach MA, et al. Glucose homeostasis in relation to neutrophil mobilization in smokers with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1179–1194. doi:10.2147/COPD.S353753
90. Stockfelt M, Christenson K, Andersson A, et al. Increased CD11b and Decreased CD62L in blood and airway neutrophils from long-term smokers with and without COPD. J Innate Immun. 2020;12(6):480–489. doi:10.1159/000509715
91. Barnes PJ. Inflammatory endotypes in COPD. Allergy. 2019;74(7):1249–1256. doi:10.1111/all.13760
92. Yao W, Han X, Guan Y, et al. Neutrophil elastase inhibitors suppress oxidative stress in lung during liver transplantation. Oxid Med Cell Longev. 2019;2019:7323986. doi:10.1155/2019/7323986
93. McDowell S, Luo R, Arabzadeh A, et al. Neutrophil oxidative stress mediates obesity-associated vascular dysfunction and metastatic transmigration. Nat Cancer. 2021;2(5):545–562. doi:10.1038/s43018-021-00194-9
94. Johnson J, Jaggers RM, Gopalkrishna S, et al. Oxidative stress in neutrophils: implications for diabetic cardiovascular complications. Antioxid Redox Signal. 2022;36(10–12):652–666. doi:10.1089/ars.2021.0116
95. Ryan EM, Sadiku P, Coelho P, et al. NRF2 activation reprograms defects in oxidative metabolism to restore macrophage function in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2023;207(8):998–1011. doi:10.1164/rccm.202203-0482OC
96. Öz HH, Cheng EC, Di Pietro C, et al. Recruited monocytes/macrophages drive pulmonary neutrophilic inflammation and irreversible lung tissue remodeling in cystic fibrosis. Cell Rep. 2022;41(11):111797. doi:10.1016/j.celrep.2022.111797
97. Genschmer KR, Russell DW, Lal C, et al. Activated PMN exosomes: pathogenic entities causing matrix destruction and disease in the lung. Cell. 2019;176(1–2):113–26.e15. doi:10.1016/j.cell.2018.12.002
98. Corleis B, Tzouanas CN, Wadsworth MH, et al. Tobacco smoke exposure recruits inflammatory airspace monocytes that establish permissive lung niches for Mycobacterium tuberculosis. Sci Transl Med. 2023;15(725):eadg3451. doi:10.1126/scitranslmed.adg3451
99. Lea S, Gaskell R, Hall S, Maschera B, Hessel E, Singh D. Assessment of bacterial exposure on phagocytic capability and surface marker expression of sputum macrophages and neutrophils in COPD patients. Clin Exp Immunol. 2021;206(1):99–109. doi:10.1111/cei.13638
100. Alfahad AJ, Alzaydi MM, Aldossary AM, et al. Current views in chronic obstructive pulmonary disease pathogenesis and management. Saudi Pharm J. 2021;29(12):1361–1373. doi:10.1016/j.jsps.2021.10.008
101. Li Y, Yang Y, Guo T, et al. Heme oxygenase-1 determines the cell fate of ferroptotic death of alveolar macrophages in COPD. Front Immunol. 2023;14:1162087. doi:10.3389/fimmu.2023.1162087
102. Fan W, Xu Z, Zhang J, et al. Naringenin regulates cigarette smoke extract-induced extracellular vesicles from alveolar macrophage to attenuate the mouse lung epithelial ferroptosis through activating EV miR-23a-3p/ACSL4 axis. Phytomedicine. 2024;124:155256. doi:10.1016/j.phymed.2023.155256
103. Dong C. Cytokine regulation and function in T cells. Annu Rev Immunol. 2021;39(1):51–76. doi:10.1146/annurev-immunol-061020-053702
104. Cancro MP. Age-Associated B Cells. Annu Rev Immunol. 2020;38(1):315–340. doi:10.1146/annurev-immunol-092419-031130
105. Cribbs SK, Crothers K, Morris A. Pathogenesis of HIV-related lung disease: immunity, infection, and inflammation. Physiol Rev. 2020;100(2):603–632. doi:10.1152/physrev.00039.2018
106. Chapman NM, Boothby MR, Chi H. Metabolic coordination of T cell quiescence and activation. Nat Rev Immunol. 2020;20(1):55–70. doi:10.1038/s41577-019-0203-y
107. Künzli M, Masopust D. CD4+ T cell memory. Nat Immunol. 2023;24(6):903–914. doi:10.1038/s41590-023-01510-4
108. Mark NM, Kargl J, Busch SE, et al. Chronic obstructive pulmonary disease alters immune cell composition and immune checkpoint inhibitor efficacy in non–small cell lung cancer. Am J Respir Crit Care Med. 2018;197(3):325–336. doi:10.1164/rccm.201704-0795OC
109. Fabre T, Barron A, Christensen SM, et al. Identification of a broadly fibrogenic macrophage subset induced by type 3 inflammation. Sci Immunol. 2023;8(82):eadd8945. doi:10.1126/sciimmunol.add8945
110. Dougan M, Dranoff G, Dougan SK. GM-CSF, IL-3, and IL-5 family of cytokines: regulators of inflammation. Immunity. 2019;50(4):796–811. doi:10.1016/j.immuni.2019.03.022
111. Laumont CM, Banville AC, Gilardi M, Hollern DP, Nelson BH. Tumour-infiltrating B cells: immunological mechanisms, clinical impact and therapeutic opportunities. Nat Rev Cancer. 2022;22(7):414–430. doi:10.1038/s41568-022-00466-1
112. Ladjemi MZ, Martin C, Lecocq M, et al. Increased iga expression in lung lymphoid follicles in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2019;199(5):592–602. doi:10.1164/rccm.201802-0352OC
113. Bod L, Kye YC, Shi J, et al. B-cell-specific checkpoint molecules that regulate anti-tumour immunity. Nature. 2023:619(7969):348–56. doi:10.1038/s41586-023-06231-0
114. McInnes IB, Schett G. Pathogenetic insights from the treatment of rheumatoid arthritis. Lancet. 2017;389(10086):2328–2337. doi:10.1016/S0140-6736(17)31472-1
115. Sakaguchi S, Mikami N, Wing JB, Tanaka A, Ichiyama K, Ohkura N. Regulatory T Cells and Human Disease. Annu Rev Immunol. 2020;38:541–566. doi:10.1146/annurev-immunol-042718-041717
116. Duffney PF, Falsetta ML, Rackow AR, Thatcher TH, Phipps RP, Sime PJ. Key roles for lipid mediators in the adaptive immune response. J Clin Invest. 2018;128(7):2724–2731. doi:10.1172/JCI97951
117. Chen Y, Li Z, Ji G, Wang S, Mo C, Ding BS. Lung regeneration: diverse cell types and the therapeutic potential. MedComm. 2024;5(2):e494. doi:10.1002/mco2.494
118. Tang J, Ramis-Cabrer D, Curull V, et al. Immune cell subtypes and cytokines in lung tumor microenvironment: influence of COPD. Cancers. 2020;12(5):1217. doi:10.3390/cancers12051217
119. Kapellos TS, Baßler K, Fujii W, et al. Systemic alterations in neutrophils and their precursors in early-stage chronic obstructive pulmonary disease. Cell Rep. 2023;42(6):112525. doi:10.1016/j.celrep.2023.112525
120. Kong Q, Wang B, Zhong Y, et al. Modified Bushen Yiqi Formula mitigates pulmonary inflammation and airway remodeling by inhibiting neutrophils chemotaxis and IL17 signaling pathway in rats with COPD. J Ethnopharmacol. 2024;321:117497. doi:10.1016/j.jep.2023.117497
121. Mateu-Jimenez M, Curull V, Pijuan L, et al. Systemic and Tumor Th1 and Th2 inflammatory profile and macrophages in lung cancer: influence of underlying chronic respiratory disease. J Thorac Oncol. 2017;12(2):235–248. doi:10.1016/j.jtho.2016.09.137
122. Asplund Högelin K, Isac B, Khademi M, Al Nimer F. B cell activating factor levels are linked to distinct B cell markers in multiple sclerosis and following B cell depletion and repopulation. Clin Immunol. 2024;258:109870. doi:10.1016/j.clim.2023.109870
123. Pisetsky DS. Pathogenesis of autoimmune disease. Nat Rev Nephrol. 2023;19(8):509–524. doi:10.1038/s41581-023-00720-1
124. Ohashi A, Murayama MA, Miyabe Y, Yudoh K, Miyabe C. Streptococcal infection and autoimmune diseases. Front Immunol. 2024;15:1361123. doi:10.3389/fimmu.2024.1361123
125. Kume H, Yamada R, Sato Y, Togawa R. Airway smooth muscle regulated by oxidative stress in COPD. Antioxidants. 2023;12(1):142. doi:10.3390/antiox12010142
126. Nucera F, Mumby S, Paudel KR, et al. Role of oxidative stress in the pathogenesis of COPD. Minerva Med. 2022;113(3):370–404. doi:10.23736/S0026-4806.22.07972-1
127. Barnes PJ. Oxidative stress-based therapeutics in COPD. Redox Biol. 2020;33:101544. doi:10.1016/j.redox.2020.101544
128. Mittelbrunn M, Kroemer G. Hallmarks of T cell aging. Nat Immunol. 2021;22(6):687–698. doi:10.1038/s41590-021-00927-z
129. Conlon TM, John-Schuster G, Heide D, et al. Inhibition of LTβR signalling activates WNT-induced regeneration in lung. Nature. 2020;588(7836):151–156. doi:10.1038/s41586-020-2882-8
130. Bu T, Wang LF, Yin YQ. How do innate immune cells contribute to airway remodeling in COPD progression. Int J Chron Obstruct Pulmon Dis. 2020;15:107–116. doi:10.2147/COPD.S235054
131. Chua C, Jiang AY, Eufrásio-da-Silva T, et al. Emerging immunomodulatory strategies for cell therapeutics. Trends Biotechnol. 2023;41(3):358–373. doi:10.1016/j.tibtech.2022.11.008
132. Tan Y, Qiao Y, Chen Z, et al. FGF2, an immunomodulatory factor in asthma and chronic obstructive pulmonary disease (COPD). Front Cell Dev Biol. 2020;8:223. doi:10.3389/fcell.2020.00223
133. Wu Y, Yang Z, Cheng K, Bi H, Chen J. Small molecule-based immunomodulators for cancer therapy. Acta Pharm Sin B. 2022;12(12):4287–4308. doi:10.1016/j.apsb.2022.11.007
134. Ramalingam V. NLRP3 inhibitors: unleashing their therapeutic potential against inflammatory diseases. Biochem Pharmacol. 2023;218:115915. doi:10.1016/j.bcp.2023.115915
135. Mosmann TR, McMichael AJ, LeVert A, McCauley JW, Almond JW. Opportunities and challenges for T cell-based influenza vaccines. Nat Rev Immunol. 2024. doi:10.1038/s41577-024-01030-8
136. Zhang PD, Zhang XR, Zhang A, et al. Associations of genetic risk and smoking with incident COPD. Eur Respir J. 2022;59(2):2101320. doi:10.1183/13993003.01320-2021
137. McRobbie H, Kwan B. Tobacco use disorder and the lungs. Addiction. 2021;116(9):2559–2571. doi:10.1111/add.15309
138. Brauwers B, Machado F, Beijers R, Spruit MA, Franssen F. Combined exercise training and nutritional interventions or pharmacological treatments to improve exercise capacity and body composition in chronic obstructive pulmonary disease: a narrative review. Nutrients. 2023;15(24):5136. doi:10.3390/nu15245136
139. Koreny M, Arbillaga-Etxarri A, Bosch de Basea M, et al. Urban environment and physical activity and capacity in patients with chronic obstructive pulmonary disease. Environ Res. 2022;214(Pt 2):113956. doi:10.1016/j.envres.2022.113956
140. Tan W, Shen HM, Wong W. Dysregulated autophagy in COPD: a pathogenic process to be deciphered. Pharmacol Res. 2019;144:1–7. doi:10.1016/j.phrs.2019.04.005
141. Bridgewood C, Newton D, Bragazzi N, Wittmann M, McGonagle D. Unexpected connections of the IL-23/IL-17 and IL-4/IL-13 cytokine axes in inflammatory arthritis and enthesitis. Semin Immunol. 2021;58:101520. doi:10.1016/j.smim.2021.101520
142. Zhao X, Zhang Q, Zheng R. The interplay between oxidative stress and autophagy in chronic obstructive pulmonary disease. Front Physiol. 2022;13:1004275. doi:10.3389/fphys.2022.1004275
143. Santos de Lima K, Schuch FB, Camponogara Righi N, et al. Effects of the combination of vitamins C and E supplementation on oxidative stress, inflammation, muscle soreness, and muscle strength following acute physical exercise: meta-analyses of randomized controlled trials. Crit Rev Food Sci Nutr. 2023;63(25):7584–7597. doi:10.1080/10408398.2022.2048290
144. de Oliveira D, Rosa FT, Simões-Ambrósio L, Jordao AA, Deminice R. Antioxidant vitamin supplementation prevents oxidative stress but does not enhance performance in young football athletes. Nutrition. 2019;63–64:29–35. doi:10.1016/j.nut.2019.01.007
145. Mousset A, Lecorgne E, Bourget I, et al. Neutrophil extracellular traps formed during chemotherapy confer treatment resistance via TGF-β activation. Cancer Cell. 2023;41(4):757–75.e10. doi:10.1016/j.ccell.2023.03.008
146. Belizaire R, Wong WJ, Robinette ML, Ebert BL. Clonal haematopoiesis and dysregulation of the immune system. Nat Rev Immunol. 2023;23(9):595–610. doi:10.1038/s41577-023-00843-3
147. Wiel C, Le Gal K, Ibrahim MX, et al. BACH1 stabilization by antioxidants stimulates lung cancer metastasis. Cell. 2019;178(2):330–45.e22. doi:10.1016/j.cell.2019.06.005
148. Forman HJ, Zhang H. Targeting oxidative stress in disease: promise and limitations of antioxidant therapy. Nat Rev Drug Discov. 2021;20(9):689–709. doi:10.1038/s41573-021-00233-1
149. Kontoghiorghes GJ, Kontoghiorghe CN. Prospects for the introduction of targeted antioxidant drugs for the prevention and treatment of diseases related to free radical pathology. Expert Opin Investig Drugs. 2019;28(7):593–603. doi:10.1080/13543784.2019.1631284
150. Kaur M, Chandel J, Malik J, Naura AS. Particulate matter in COPD pathogenesis: an overview. Inflamm Res. 2022;71(7–8):797–815. doi:10.1007/s00011-022-01594-y
151. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
152. Sin DD, Doiron D, Agusti A, et al. Air pollution and COPD: GOLD 2023 committee report. Eur Respir J. 2023;61(5):2202469. doi:10.1183/13993003.02469-2022
153. Tran HM, Chen TT, Lu YH, et al. Climate-mediated air pollution associated with COPD severity. Sci Total Environ. 2022;843:156969. doi:10.1016/j.scitotenv.2022.156969
154. Ryu MH, Murphy S, Hinkley M, Carlsten C. COPD exposed to air pollution: a path to understand and protect a susceptible population. Chest. 2024;165(4):836–846. doi:10.1016/j.chest.2023.11.012
155. Tilg H, Adolph TE, Trauner M. Gut-liver axis: pathophysiological concepts and clinical implications. Cell Metab. 2022;34(11):1700–1718. doi:10.1016/j.cmet.2022.09.017
156. Torres A, Cilloniz C, Niederman MS, et al. Pneumonia. Nat Rev Dis Primers. 2021;7(1):25. doi:10.1038/s41572-021-00259-0
157. Cazzola M, Hanania NA, Page CP, Matera MG. Novel anti-inflammatory approaches to COPD. Int J Chron Obstruct Pulmon Dis. 2023;18:1333–1352. doi:10.2147/COPD.S419056
158. Matera MG, Calzetta L, Annibale R, Russo F, Cazzola M. Classes of drugs that target the cellular components of inflammation under clinical development for COPD. Expert Rev Clin Pharmacol. 2021;14(8):1015–1027. doi:10.1080/17512433.2021.1925537
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.