")
Back to Journals » Journal of Inflammation Research » Volume 17
Inflammatory Myofibroblastic Tumor of the Orbit: A Case Series and Literature Review
Authors Guo S, Wang S, Chen C, He X, Yang B, Huang Z, Ma J, Shi J, Jiang L, Chen FK
Received 18 August 2024
Accepted for publication 21 November 2024
Published 14 December 2024 Volume 2024:17 Pages 11029—11039
DOI https://doi.org/10.2147/JIR.S485499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Sitong Guo,1,2 Songze Wang,2,3 Chunli Chen,2 Xiaojin He,4 Bentao Yang,5 Zhiqin Huang,2 Jianmin Ma,2 Jitong Shi,2 Libin Jiang,2 Fred Kuanfu Chen6– 8
1Department of Ophthalmology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China; 2Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University; Beijing Ophthalmology and Visual Sciences Key Laboratory, Beijing, 100730, People’s Republic of China; 3Beijing FengTai You’anmen Hospital, Beijing, People’s Republic of China; 4Department of Pathology, Beijing Tongren Hospital, Capital Medical University, Beijing, 100730, People’s Republic of China; 5Department of Radiology, Beijing Tongren Hospital, Capital Medical University, Beijing, 100730, People’s Republic of China; 6Centre for Ophthalmology and Visual Science, The University of Western Australia, Perth, WA, Australia; 7Ophthalmology, Department of Surgery, University of Melbourne, Melbourne, VIC, Australia; 8Department of Ophthalmology, Royal Perth Hospital, Perth, WA, Australia
Correspondence: Libin Jiang, Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University; Beijing Ophthalmology and Visual Sciences Key Laboratory, Beijing, 100730, People’s Republic of China, Email [email protected]
Purpose: Orbital inflammatory myofibroblastic tumors (IMTs) are a rare tumor with intermediate biological potential. We analyzed a series of orbital IMTs to determine their unique features.
Methods: Records from patients with pathologically confirmed IMT at Beijing Tongren Hospital, Capital Medical University, between January 2004 and August 2022, were reviewed for their ocular presentation and treatment outcomes.
Results: Thirteen cases of primary orbital IMT with positive anaplastic lymphoma kinase on fluorescent in situ hybridization were included. These consists of five men and eight women with an age of onset ranged from 2 to 54 years. Nearly half of the primary orbital IMTs displayed local invasion into the maxillary sinus, ethmoid sinus, and pterygopalatine fossa. On magnetic resonance imaging, orbital IMT usually appeared as an ill-defined, oval, irregular, or diffuse mass with heterogeneous signals. Nearly half (46.2%) of these lesions caused bone destruction, and 31% developed recurrence, which was more likely to occur in lesions involving multiple tissues (50%). All cases of recurrence occurred within five months after the first surgery. No patient developed distant metastases.
Conclusion: Orbital IMT is rare and prone to local invasion and recurrence. The histology and behavior of orbital IMT requires further investigation.
Keywords: inflammatory myofibroblastic tumor, orbit, MRI, pathologic, prognosis
Introduction
Inflammatory myofibroblastic tumor (IMT) is a rare neoplasm that was formerly incorrectly categorized as a subtype of “inflammatory pseudotumors”. IMT is now considered a true neoplasm due to a tendency for local recurrence and distant metastasis,1 and it has been re-classified by the World Health Organization as a myofibroblastic tumor with intermediate biological potential (rarely metastasizing).1–4 Although the lungs are the most common site of primary IMT, it can occur in any anatomical location. Extrapulmonary IMT most commonly occurs in the abdominal cavity, retroperitoneum, and mediastinum and less frequently in the head and neck region, including the orbit.5–13 In most extraorbital cases, surgical resection is the best approach for IMT treatment, generally resulting in a better prognosis. If the tumor is unresectable, steroids or chemotherapy regimens may be considered. To date, 42 cases of orbital IMT have been published.2,9–25 Here, we report the observations of our orbital IMT cases and summarize the clinical and imaging features in combination with previously reported cases.
Methods
We systematically collected clinical data and follow-up information on Chinese patients with orbital IMT treated at the Beijing Tongren Hospital, Capital Medical University between January 2004 and August 2022. Thirteen patients with ocular symptoms as their first clinical manifestation and histopathologically confirmed IMT underwent surgery at our institution. The inclusion criteria were as follows: (1) IMT cases fulfilling the morphological criteria defined in the World Health Organization classification;1 (2) positive for anaplastic lymphoma kinase (ALK) on fluorescent in situ hybridization; (3) ocular symptoms as the presenting feature; (4) neoplasms with orbital involvement confirmed by imaging or surgical record; and (5) complete clinicopathological data. Clinical data included age, sex, main symptoms and signs, imaging findings, treatment information, pathological findings, and prognosis. The study protocol was approved by the Ethics Committee of Beijing Tongren Hospital, affiliated with the Capital Medical University, and adhered to the tenets of the Declaration of Helsinki (TRECKY2020-045). All study participants or a parent of participants aged under 18 years provided informed consent.
A literature search from 1950 to the present was performed using PubMed/MEDLINE and the Cochrane database, using the key terms “inflammatory myofibroblastic tumor”, “ocular”, and “orbital”. Only articles or abstracts written in English were included.
Statistical analyses were performed using IBM SPSS v. 23.0 (Armonk, NY, USA). Comparisons between groups were performed using the Mann–Whitney U-test. P-values < 0.05 were considered statistically significant.
Results
Clinical Features
Epidemiological information and clinical features of the 13 patients are summarized in Table 1. There were five men and eight women. The age of onset ranged from 2 to 54 years, with a mean (± standard deviation, SD) age of 29.0 ± 15.7 years (median, 29 years; interquartile range, 17–41.5 years); three patients were aged 10 years or less. Tumors in 10 patients were located in the right orbit and three in the left orbit.
Symptoms developed between 20 days and 12 months prior to the initial examination, with a mean (± SD) age of 3.7 ± 3.3 months (median, 3 months; interquartile range, 1–5 months). The duration of symptoms was longer than 1 month in 11 patients. Six patients presented with proptosis, three had ocular pain, three had diplopia or ocular movement disorder, and three had decreased visual acuity. Eyelid or conjunctival masses were observed in four patients.
 |
Table 1 Clinical Features |
From our observation, we propose a classification system by dividing IMTs into those that are confined to the orbit as intraorbital IMT (IIMT), and those orbital lesions that have extended to adjacent tissues as intraorbital-extraorbital IMT (I-EIMT). There were seven cases of IIMT (Cases 1–7) and six cases of I-EIMT (Cases 8–13) (Table 2). There was no significant difference in the age of onset (t = 1.032, P = 0.324) or treatment duration (t = 1.564, P = 0.146) between the IIMT and I-EIMT groups.
 |
Table 2 Differences Between IIMT and I-EIMT |
Imaging Features
Twelve patients underwent orbital magnetic resonance imaging (MRI), and eight underwent computed tomography (CT). Orbital IMT usually appeared as an oval, irregular, or diffuse mass with ill-defined boundaries. They were relatively heterogeneous on MRI, showed low to high signal intensity (SI) on T2-weighted imaging (WI) compared to the gray matter, and low to equal SI on T1WI, most of which exhibited marked heterogeneous enhancement with gadolinium. On CT, the lesions showed soft tissue with equal density to the extraocular muscles, without calcification. One mass caused compression of the medial orbital wall as seen on MRI, and six lesions caused bone destruction, visible on CT. By using the coronal plane slicing through the globe’s equator, the orbit is divided into anterior and posterior parts. Four lesions were located in the anterior part of the orbit, such as lesions in the lacrimal gland, the surface of the globe, and subcutaneous tissue (Figure 1). Eight lesions were located in the posterior part of the orbit; in the intraconal and extraconal spaces. One lesion was located in both anterior and posterior orbit. When some lesions spread outside the orbit, they passed through the inferior orbital fissure and superior orbital fissure, to invade the cavernous sinus, sphenoid sinus, maxillary sinus, infratemporal fossa, and pterygopalatine fossa. Some lesions in the orbit and paranasal sinuses in the same patient presented with different signal intensities on MRI. Detailed imaging features are presented in Table 3.
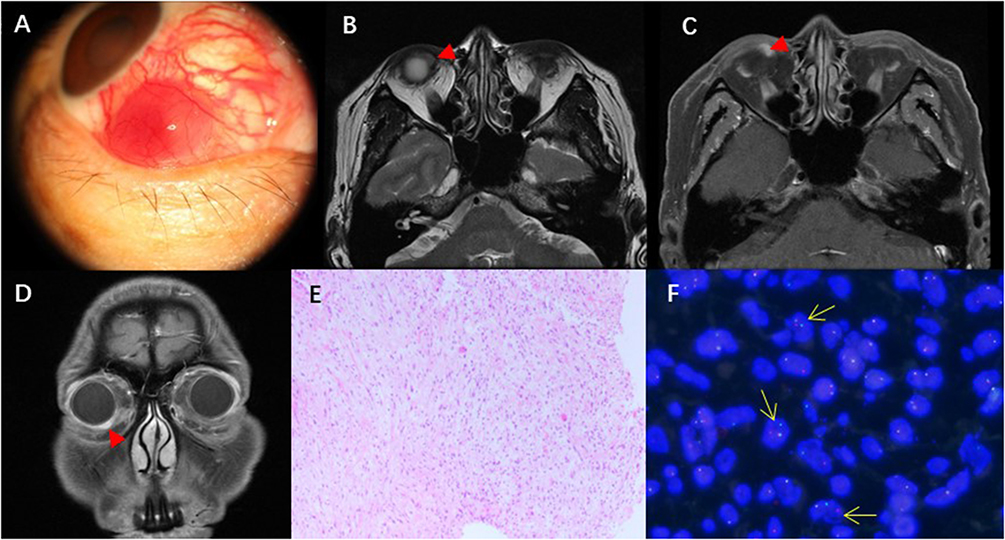 |
Figure 1 Case 7. Clinical photograph of right orbital mass (A), T2WI (B), and enhanced T1WI with fat-suppression (C and D) show an ill-defined mass wrapping around the globe in the right orbit (triangle). Myofibroblastomatous hyperplasia can be seen at low magnification. Tumor cells with atypia and cytoplasmic staining consistent with differentiation of muscle fibers (Original magnification X100. Hematoxylin and Eosin) (E). Anaplastic lymphoma kinase (ALK) gene rearrangement was detected by ALK break-apart fluorescence in situ hybridization. Separation of proximal (green) and distal (red) probes indicates ALK rearrangement (yellow arrows) (F). |
 |
Table 3 Imaging Features |
Treatment and Prognosis
All 13 patients underwent primary local resection and received post-operative systemic steroid. The surgical approaches included lateral orbitotomy, anterior orbitotomy, nasal endoscopic excision and coronal approach excision. Four patients relapsed after surgery, and all recurrences occurred within 1–4 months. In the IIMT group, only one patient relapsed 4 months after the operation, and in the I-EIMT group, three of six patients relapsed, with an average recurrence time of 2 months. The mean (± SD) age of patients with recurrence was 18.5 ± 10.8 years, compared to 33.7 ± 15.7 years in those without recurrence (t = 1.551, P = 0.152). One patient underwent radiotherapy and exenteration after the second recurrence, and no recurrence was observed 6 years after surgery (Case 9). Another patient underwent local resection and was alive with recurrent tumors (Case 2). One patient did not undergo surgery as the symptoms were tolerable (Case 11). One patient died 2 years later due to multiple organ dysfunction syndrome (MODS) after several cycles of chemotherapy (cyclophosphamide 1.0 g on days 1 and 8; epirubicin 100 mg on days 2 and 9; dexamethasone 5 mg on days 1, 2, 8, and 9; and dexamethasone 2 mg on days 3 and 10) (Case 13).
Pathological Features
Grossly, the lesions were usually ill-circumscribed, tough, or brittle masses with a gray-white or gray-red cut surface, and some adhered to adjacent tissues. Tumors ranged from 0.87 cm to 4.1 cm in the greatest dimension. Microscopic lesions showed proliferation of fibroblasts and myofibroblasts accompanied by mixed inflammatory cell infiltration, including plasma cells, lymphocytes, and a small number of neutrophils. The spindle cells were mild in shape, with pale eosinophilic cytoplasm and central vesicular oval nuclei with small nucleoli. Necrotic tissue and a few atypical cells were observed in some recurrent cases, suggesting a malignancy. Immunohistochemical staining for the lesions was positive for ALK, vimentin, and smooth muscle actin. Fluorescent in situ hybridization showed that all cases were positive for ALK.
Discussion
IMT was first observed in the lung and described by Brunn in 193926 and was termed as “inflammatory pseudotumor” by Umiker and Iverson in 1954,27 due to its clinical and radiological similarities to malignant tumors. In 1991, Meis and Enzinger28 first reported neoplastic features in some cases, including cytogenetic abnormalities and aggressive clinical behaviors such as local invasion, recurrence, and distant metastasis. These lesions comprised of fibroblast and myofibroblast proliferation; thus, they were termed “inflammatory fibrosarcoma.” To date, several synonyms have been used in the literature for this disease, such as plasma cell granuloma, xanthoma, fibroxanthoma, plasmacytoma, myxoid hamartoma, solitary mast cell granuloma, histiocytoma, pseudoneoplastic pneumonia, and inflammatory muscle cell proliferation.29–32 The pathogenesis of IMT remains controversial and its behavior, whether benign or locally aggressive, is unpredictable.33 To date, 18 reports with 42 cases of orbital IMT can be retrieved from PubMed (Table 4), including one case series of 25 orbital IMTs25 and 17 case reports.2,7,9–24 In addition to the cases of orbital IMT in the present study, there are 55 cases of primary orbital IMT. However, there may be additional cases of orbital IMT that were published using other labels and which therefore may not have been retrieved during the literature search.
 |
Table 4 Reported Cases of Orbital IMT |
Extrapulmonary IMTs may present at any age but occur more commonly in children and adolescents,18,34,35 with an equal incidence in men and women.8,36 The onset age of orbital IMT ranged from 5 months to 76 years in previous studies, and 26.2% of the cases were younger than 18 years. In contrast, a younger age of onset is more common in isolated case reports, accounting for about 64.7% of cases. Strianese et al25 reported a slightly higher prevalence in the 60–69-year age group. However, in our series, all patients developed the disease before reaching 60 years of age, and there was no clear trend based on age groups. Although there were slightly more female than male patients in this study, there was no obvious trend in the literature.
All orbital IMT appeared to be unilateral, whereas Case 10 had a history of inflammatory pseudotumor in the right eye, which was pathologically diagnosed at another hospital. IMT in the orbit may present with unilateral proptosis, eyelid swelling, and disturbance of ocular motility or diplopia. In some instances, the presence of these tumors in the orbit may lead to serious visual morbidity. The most frequent symptoms were proptosis, pain, and ocular movement disorders. In published cases, primary orbital IMT masses were located in the anterior part of the orbit in 15 patients, in the posterior part in 27 patients, diffuse in 11 patients, and intraocular in one patient. The location of one tumor was unknown. In this study, nearly half of the primary orbital IMTs showed localized invasion, often involving the maxillary sinus, ethmoid sinus, or pterygopalatine fossa. This may have occurred prior to initial surgery. However, there was no local invasion in the study by Strianese,25 and the local invasion rate of primary orbital IMT in separate case reports was 20%.10,11,14
The imaging presentations of IMT are nonspecific and may imitate a variety of orbital lesions such as lymphoma, sarcoma, and fungal disease. On MRI, orbital IMTs may be hypointense to isointense relative to the gray matter on T1WI, hypointense to hyperintense on T2WI, and homogeneous or heterogeneous after gadolinium enhancement. The composition of inflammatory cells and fibrous tissue may influence the signal intensities on MRI sequences. Low and equal signal intensities on both T1WI and T2WI may reflect the fibrotic nature, collagen components, or dense tumor cells; in contrast, high signal intensity on T2WI may reflect more vascular mucus components of these lesions. In this study, lesions of IIMT on T2WI showed high signal intensity, but lesions of I-EIMT showed mixed signal intensity from low to high. In addition, some lesions in different positions in the same patient, orbital, and paranasal sinuses also showed different signal intensities on T1WI and T2WI (Cases 8). Furthermore, 46.2% of primary orbital IMTs in this study invaded the bony orbital walls. However, these results are quite different from those of a previous study that reported no bony erosion, removal, or sclerosis.25 In separate case reports, bone invasion was observed in five of 13 patients with primary orbital IMT who underwent MRI or CT examinations.8,10,12,14,15 Sepahdari et al37 found that malignant lesions had a lower apparent diffusion coefficient (ADC) than benign lesions and that lymphoma had a lower ADC than IMT, which may be helpful in differential diagnosis. Calcifications were seen in 10–25% of orbital IMTs38 and the majority of pulmonary IMTs.39 However, no calcification was found on our cases of orbital IMT.
IMT is a true neoplasm and is characterized by cellular spindle cell proliferation in myxoid or collagenous stroma with inflammatory infiltration. Mild nuclear atypia, including scattered ganglion-like cells, and low mitotic rate without atypical forms can be observed on pathological examination.8 In the orbit, IMT often needs to be distinguished from inflammatory pseudotumor. They both belong to the group of inflammatory spindle cell lesions. Inflammatory pseudotumor is a more inflammatory reactive lesion with no heterotypic cells and pathological nuclear fission images, whereas it sometimes appears to be IMT. Therefore, morphology cannot fully and sufficiently distinguish IMT from inflammatory pseudotumor; accordingly, additional molecular tests, such as ALK, should be conducted.8 ALK gene rearrangements account for 50‒70% of IMT cases, followed by ROS1 or NTRK3 rearrangements, which account for 5–10% of cases, respectively.40 Other fusion genes identified in molecular genetics, such as RET, PDGFRβ, and IGF1R with their partner genes also exist.5,41,42 Further fluorescent in situ hybridization or next-generation sequencing testing is recommended for eligible patients with controversial diagnosis or patients clinically considered for targeted therapy.
Currently, the accepted treatment of choice for these lesions is complete surgical excision, although spontaneous regression of IMT in the orbit 14 years after partial excision has been documented.16 The use of CT and MRI plays a crucial role in defining the extent of the tumor and deciding the subsequent surgical options. Lateral orbitotomy and anterior orbitotomy are usually performed for lesions confined to the orbit. For lesions located in the superior quadrant of the orbit or involving the intracranial region, a coronal approach can be chosen. Nasal endoscopic surgery is a good choice for lesions involving the paranasal sinus. Previous reports have shown that complete surgical excision is indicated to avoid relapse.43,44 However, this is difficult when the tumor grows in the orbit. For lesions not amenable to complete excision, conservative oral corticosteroid and immunosuppressive therapy may alleviate or control the symptoms, depending on the activity of the inflammatory process. Crizotinib is an ATP-competitive inhibitor of the ALK tyrosine kinase receptor. Three patients with ALK-positive orbital IMT were treated with crizotinib after incomplete excision. A reduction in the size of the lesion was observed on repeat MRI.17–19 Other ALK tyrosine kinase inhibitors have also been shown to be effective in sporadic cases and may represent the direction of future research in the treatment of orbital IMT.45
Relapse occurred in 24% of patients with orbital IMT in Strianese’s study and in all of these were older than 40 years.25 However, in this study, 30.8% of patients with orbital IMT developed recurrence, which had no significant age predisposition and was more likely to occur in patients with diffuse lesions involving multiple sites. All recurrences in this study occurred within four months after excision. Some patients who underwent local excision combined with radiotherapy after recurrence developed recurrence again, and the disease was controlled after exenteration. However, the role of radiation and chemotherapy in IMTs remains unclear. Complete surgical excision was not possible due to the intimate relationship between the tumor and the optic nerve in Cases 2 and 11. However, after 4–12 years of follow-up, the tumor showed static behavior. No case of orbital IMT with distant metastasis has been reported, and only one patient in our study died of MODS after chemotherapy.
Several limitations are present in the study, including its retrospective design, small number of patients and the inclusion of only ALK-positive cases in this case series.
Conclusion
Orbital IMT is rare and lacks specific clinical manifestations. It has a tendency for local recurrence and bone destruction. Only 55 cases, including those in the present study, have been reported. Based on our observation of 13 cases of orbital lMT and a literature review, we report that local invasion and bone erosion by orbital IMT are features that can be seen on magnetic resonance imaging or computed tomography and that resection is the preferred treatment. Although the recurrence rate is high, distant metastasis is rare, and the prognosis is relatively good. Further investigation of the histology and clinical behavior of IMT are required.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
Funding
Capital Health Research and Development of Special Fund (No: 2020-2-1082) and Natural Science Foundation of Beijing Municipality (No: 7222028).
Disclosure
The authors have no conflict of interest.
References
1. Coffin CM, Fletcher JA. Inflammatory myofibroblastic tumor. In: Fletcher CDM, Unni KK, Mertens F, editors. World Health Organization Classification of Tumors Pathology and Genetics of Tumors of Soft Tissue and Bone. Lyon: IARC Press; 2002:91–93.
2. Sa HS, Ji JY, Suh YL, Kim YD. Inflammatory myofibroblastic tumor of the orbit presenting as a subconjunctival mass. Ophthalmic Plast Reconstr Surg. 2005;21(3):211–215. doi:10.1097/01.IOP.0000161713.41406.D0
3. Janik JS, Janik JP, Lovell MA, Hendrickson RJ, Bensard DD, Greffe BS. Recurrent inflammatory pseudotumors in children. J Pediatr Surg. 2003;38(10):1491–1495. doi:10.1016/S0022-3468(03)00501-3
4. Cerfolio RJ, Allen MS, Nascimento AG, et al. Inflammatory pseudotumors of the lung. Ann Thorac Surg. 1999;67(4):933–936. doi:10.1016/S0003-4975(99)00155-1
5. Coffin CM, Watterson J, Priest JR, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor). A clinicopathologic and immunohistochemical study of 84 cases. Am J Surg Pathol. 1995;19(8):859–872. doi:10.1097/00000478-199508000-00001
6. Kazantseva IA, Gurevich LE, Stepanova EV. [Extrapulmonary inflammatory myofibroblastic tumor]. Arkh Patol. 2001;63(6):35–39. Russian.
7. Ahmad SM, Tsirbas A, Kazim M. Inflammatory myofibroblastic tumour of the orbit in a 7-year-old child. Clin Exp Ophthalmol. 2007;35(2):160–162. doi:10.1111/j.1442-9071.2006.01435.x
8. Gleason BC, Hornick JL. Inflammatory myofibroblastic tumours: where are we now? J Clin Pathol. 2008;61(4):428–437. doi:10.1136/jcp.2007.049387
9. Polito E, Pichierri P, Loffredo A, Moramarco A, Occhini R. Inflammatory myofibroblastic tumor of the orbit. Ophthalmologica. 2007;221(5):353–355. doi:10.1159/000104767
10. Dutta V, Manoj MG, Malik A, Kumar P. ALK negative inflammatory myofibroblastic tumor of the orbit: a masquerading entity. Indian J Ophthalmol. 2014;62(5):627–629. doi:10.4103/0301-4738.133522
11. Lauwers N, De Groot V, Kenis C, Dhubhghaill SN, Claes J, De Keizer RJ. Atypical sino-orbital inflammatory myofibroblastic tumor with bone and cerebral invasion extending to the orbit. Eur J Ophthalmol. 2014;24(4):608–610. doi:10.5301/ejo.5000401
12. Tawfik HA, Raslan AO. Infantile inflammatory myofibroblastic tumor of the orbit with apical bone involvement. Ophthalmic Plast Reconstr Surg. 2013;29(2):e44–46. doi:10.1097/IOP.0b013e3182696922
13. Cramer SK, Skalet A, Mansoor A, Wilson DJ, Ng JD. Inflammatory myofibroblastic tumor of the orbit: a case report. Ophthalmic Plast Reconstr Surg. 2015;31(1):e22–23. doi:10.1097/IOP.0000000000000058
14. McKinney AM, Short J, Lucato L, SantaCruz K, McKinney Z, Kim Y. Inflammatory myofibroblastic tumor of the orbit with associated enhancement of the meninges and multiple cranial nerves. Am J Neuroradiol. 2006;27(10):2217–2220.
15. Callaway NF, Fisher O, Dubovy S, Bhatia R, Wester ST. Inflammatory myofibroblastic tumour presenting as a medial eyelid mass in a child. Can J Ophthalmol. 2018;53(6):e241–e244. doi:10.1016/j.jcjo.2018.01.018
16. Habib L, Son JH, Petris C, Kazim M. Spontaneous regression of inflammatory myofibroblastic tumor of the orbit: a case report and review of literature. Orbit. 2017;36(3):178–182. doi:10.1080/01676830.2017.1279645
17. Gupta RR, Trinh M, Mechel E, et al. Inflammatory myofibroblastic tumor of the orbit in a 5-month-old infant. J Pediatr Ophthalmol Strabismus. 2022;59(2):e25–e28. doi:10.3928/01913913-20220124-04
18. Dermarkarian CR, Patel KR, Fuller MY, Bernini JC, Chevez-Barrios P, Allen RC. Inflammatory myofibroblastic tumor of the orbit in an 8-month old. Ophthalmic Plast Reconstr Surg. 2020;36(3):e65–e68. doi:10.1097/IOP.0000000000001575
19. Kiratli H, Uzun S, Varan A, Akyuz C, Orhan D. Management of anaplastic lymphoma kinase positive orbito-conjunctival inflammatory myofibroblastic tumor with crizotinib. J AAPOS. 2016;20(3):260–263. doi:10.1016/j.jaapos.2016.01.009
20. O’Malley DP, Poulos C, Czader M, Sanger WG, Orazi A. Intraocular inflammatory myofibroblastic tumor with ALK overexpression. Arch Pathol Lab Med. 2004;128:e5–e7. doi:10.5858/2004-128-e5-IIMTWA
21. Mudhar HS, Nuruddin M. ALK-1 positive orbital inflammatory myofibroblastic tumour (IMT) associated with prominent numbers of IgG4 plasma cells - A case report. Orbit. 2013;32:321–323. doi:10.3109/01676830.2013.805789
22. Shah S, Badhu BP, Lavaju P, Pradhan A. Ocular inflammatory myofibroblastic tumor in the left eye with phthisis right eye: a rare occurrence in a child. Case Rep Ophthalmol Med. 2015;2015:281528. doi:10.1155/2015/281528
23. Lahlou G, Classe M, Wassef M, et al. Sinonasal inflammatory myofibroblastic tumor with anaplastic lymphoma kinase 1 rearrangement: case study and literature review. Head Neck Pathol. 2017;11:131–138. doi:10.1007/s12105-016-0744-3
24. Chow SP, Nastri A, Hardy T. Infratemporal inflammatory myofibroblastic tumour with orbital extension. Clin Exp Ophthalmol. 2010;38:727–730. doi:10.1111/j.1442-9071.2010.02329.x
25. Strianese D, Tranfa F, Finelli M, Iuliano A, Staibano S, Mariniello G. Inflammatory myofibroblastic tumor of the orbit: a clinico-pathological study of 25 cases. Saudi J Ophthalmol. 2018;32(1):33–39. doi:10.1016/j.sjopt.2018.04.001
26. Brunn H, Francisco S. Two interesting benign lung tumors of contradictory histopathology: remarks on the necessity for maintaining the chest tumour registry. J Thorac Cardiovasc. 1939;9:119–131.
27. Umiker WO, Iverson L. Postinflammatory tumors of the lung; report of four cases simulating xanthoma, fibroma, or plasma cell tumor. J Thorac Surg. 1954;28(1):55–63. doi:10.1016/S0096-5588(20)30758-3
28. Meis JM, Enzinger FM. Inflammatory fibrosarcoma of the mesentery and retroperitoneum. A tumor closely simulating inflammatory pseudotumor. Am J Surg Pathol. 1991;15(12):1146–1156. doi:10.1097/00000478-199112000-00005
29. Patnana M, Sevrukov AB, Elsayes KM, Viswanathan C, Lubner M, Menias CO. Inflammatory pseudotumor: the great mimicker. AJR Am J Roentgenol. 2012;198(3):W217–227. doi:10.2214/AJR.11.7288
30. Narla LD, Newman B, Spottswood SS, Narla S, Kolli R. Inflammatory pseudotumor. Radiographics. 2003;23(3):719–729. doi:10.1148/rg.233025073
31. Park SB, Cho KS, Kim JK, et al. Inflammatory pseudotumor (myoblastic tumor) of the genitourinary tract. AJR Am J Roentgenol. 2008;191(4):1255–1262. doi:10.2214/AJR.07.3663
32. Kirkpatrick Jr JA, Harris GB, Kushner DC. Thoracic complications of plasma cell granuloma of the lung. Ann Radiol. 1984;27(2–3):145–149.
33. Neuhauser TS, Derringer GA, Thompson LD, et al. Splenic inflammatory myofibroblastic tumor (inflammatory pseudotumor): a clinicopathologic and immunophenotypic study of 12 cases. Arch Pathol Lab Med. 2001;125(3):379–385. doi:10.5858/2001-125-0379-SIMTIP
34. Cook JR, Dehner LP, Collins MH, et al. Anaplastic lymphoma kinase (ALK) expression in the inflammatory myofibroblastic tumor: a comparative immunohistochemical study. Am J Surg Pathol. 2001;25(11):1364–1371. doi:10.1097/00000478-200111000-00003
35. Myint MA, Medeiros LJ, Sulaiman RA, Aswad BI, Glantz L. Inflammatory pseudotumor of the ileum. A report of a multifocal, transmural lesion with regional lymph node involvement. Arch Pathol Lab Med. 1994;118(11):1138–1142.
36. Coffin CM, Dehner LP, Meis-Kindblom JM. Inflammatory myofibroblastic tumor, inflammatory fibrosarcoma, and related lesions: an historical review with differential diagnostic considerations. Semin Diagn Pathol. 1998;15(2):102–110.
37. Sepahdari AR, Aakalu VK, Setabutr P, Shiehmorteza M, Naheedy JH, Mafee MF. Indeterminate orbital masses: restricted diffusion at MR imaging with echo-planar diffusion-weighted imaging predicts malignancy. Radiology. 2010;256(2):554–564. doi:10.1148/radiol.10091956
38. Van Dorpe J, Ectors N, Geboes K, D’Hoore A, Sciot R. Is calcifying fibrous pseudotumor a late sclerosing stage of inflammatory myofibroblastic tumor? Am J Surg Pathol. 1999;23(3):329–335. doi:10.1097/00000478-199903000-00013
39. Oguz B, Ozcan HN, Omay B, Ozgen B, Haliloglu M. Imaging of childhood inflammatory myofibroblastic tumor. Pediatr Radiol. 2015;45(11):1672–1681. doi:10.1007/s00247-015-3377-x
40. WHO Classification of Tumours Editorial Board. WHO Classification of Tumours. Soft Tissue and Bone Tumours.
41. Mariño‐Enríquez A, Wang WL, Roy A, et al. Epithelioid inflammatory myofibroblastic sarcoma: an aggressive intra‐abdominal variant of inflammatory myofibroblastic tumor with nuclear membrane or perinuclear ALK. Am J Surg Pathol. 2011;35(1):
42. Busca A, Parra‐Herran C. Myxoid mesenchymal tumors of the uterus: an update on classification, definitions, and differential diagnosis. Adv Anat Pathol. 2017;24(6):
43. Athanassiadi K, Laenger F, Dickgreber N, Haverich A. Multiple inflammatory myofibroblastic tumors involving lung and mediastinum: a rare clinical entity. Thorac Cardiovasc Surg. 2009;57(6):343–346. doi:10.1055/s-0029-1185574
44. Lee HJ, Kim JS, Choi YS, et al. Treatment of inflammatory myofibroblastic tumor of the chest: the extent of resection. Ann Thorac Surg. 2007;84(1):221–224. doi:10.1016/j.athoracsur.2007.03.037
45. Wang QA, Chen HW, Wu RC, et al. Update of diagnosis and targeted therapy for ALK(+) inflammation myofibroblastic tumor. Curr Treat Options Oncol. 2023;24(12):1683–1702. doi:10.1007/s11864-023-01144-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.