")
Back to Journals » Clinical Ophthalmology » Volume 19
Influential Factors and Outcome of High-Risk Keratoplasty in a Tertiary Referral Corneal Center: A Retrospective Study
Authors Aschauer J, Klimek M , Donner R, Steiner I, Lammer J, Schmidinger G
Received 7 November 2024
Accepted for publication 21 January 2025
Published 21 February 2025 Volume 2025:19 Pages 653—662
DOI https://doi.org/10.2147/OPTH.S502563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Julia Aschauer,1 Michal Klimek,1 Ruth Donner,1 Irene Steiner,2 Jan Lammer,1 Gerald Schmidinger1
1Department of Ophthalmology and Optometry, Medical University of Vienna, Vienna, Austria; 2Center for Medical Data Science, Institute of Medical Statistics, Medical University of Vienna, Vienna, Austria
Correspondence: Julia Aschauer, Department of Ophthalmology and Optometry Medical University of Vienna, Spitalgasse 23, Vienna, 1090, Austria, Tel +4314040079310, Fax +4314040079320, Email [email protected]
Purpose: Corneal allograft survival is dramatically decreased in high-risk (HR) host beds. The purpose of this study was to investigate the outcome of HR keratoplasty (KP) in a single-center tertiary referral clinic and to determine risk factors for graft failure.
Methods: This retrospective study included adults referred for HR penetrating KP between 2014 and 2022. HR criteria were history of re-KP, stromal neovascularization in ≥ 2 quadrants, and signs of significant inflammation/manifest perforation at the time of surgery. The primary endpoint was graft failure within the first postoperative year. Donor endothelial cell count, donor age, stromal neovascularization, and manifest perforation/acute inflammation at surgery were independent variables in the univariate/multivariable logistic regression.
Results: Graft survival 1 year after surgery was 56.2% (CI: 45.7, 66.4), 68.3% (CI: 59.3, 76.4), and 70.2% (CI: 56.6, 81.6) after the first, second, and third KP, respectively. The presence of perforation/acute inflammation at baseline was found to be an independent factor statistically significantly associated with graft failure. Graft failure occurred in 190 (51%) of 375 KPs in 257 patients during overall observation. The median time (95% CI) from KP until graft failure was 559 (392, 994) days for the 1st KP, 1052 (833, 1375) days for the 2nd KP and 1089 (689, inf) for the 3rd KP. The most frequent cause was immune rejection (n=55, 29%), whereas in a majority (n=66, 35%) the reason remained undefined. The median time (95% CI) until neovascularization (re-) formation after KP was 739 days (550, inf) and 1566 (1055, inf) days for the 1st and the 2nd KP.
Conclusion: Acute inflammation/perforation at the time of surgery were the major risk factors for graft failure in HR KP. Reduced survival rates for HR KPs were confirmed in this study, which highlights the need for further developments in the treatment of these patients.
Keywords: cornea, graft failure, inflammation, keratoplasty, perforation
Introduction
The immune privilege of the cornea1,2 is at least partly based on the concept of the healthy human cornea being completely avascular and alymphatic due to the delicate balance between pro- and anti-angiogenic factors in the cornea and the adjacent aqueous humor, also known as “lymphangiogenic” privilege.3,4 This immunological environment builds the foundation of the high success rates associated with keratoplasty (KP), with a reported 1-year and 5-year survival rate of about 90%, and a 15-year survival rate of about 55% in non-inflamed and avascular host beds.5,6 However, survival of the allograft dramatically decreases in inflamed, vascularized host beds, so-called high risk (HR) KPs that show a 5-year survival ranging only between 25% and 65%.7–12
The Collaborative Corneal Transplantation Study (CCTS) provided us with important insights in regards to the definition of these high-risk host characteristics.13,14
In a low-risk eye, vascular sprouting from limbal arcades post-transplantation is rapidly inhibited to restore the angiogenic privilege state of the cornea. However, in the high-risk cornea, blood and lymphatic vessels are not inhibited and thus invade the donor corneal bed driving potential immune rejection.15,16
Therefore, the principal risk factor for corneal allograft rejection has been defined as host bed vascularity. The risk of allograft rejection thereby seems to correlate directly with the extent and depth of vessels invading the cornea. The CCTS defines a high-risk cornea as one with at least two quadrants of deep stromal neovascularization (NV) prior to surgery.14 Survival of transplants after penetrating keratoplasty (PKP) was reported as high as 83% after 4 years in the absence of NV, whereas it was 73%, 66%, 63%, and 50% for 1-, 2-, 3- and 4- quadrant NV, respectively.17 Once allograft rejection occurs, the difficulty of reversal may also depend on the degree of corneal NV.18
A further independent variable associated with corneal allograft failure is acute inflammation, and imminent or even manifest corneal perforation at the time of surgery.19
Outcome statistics have also provided evidence for a higher risk of graft loss regardless of the primary corneal disease in the event of re-transplantation following failure of one or more corneal allografts.20
This summarized evidence stems from studies and data registries that include data from a variety of surgical centers with diverse pre- and post-operative care settings, surgical techniques, and treatment regimes. Even further, a comparison of the precise influence of these three apparently most crucial high-risk characteristics on graft survival is still missing to this date.
The purpose of this study was to investigate the outcome of high-risk corneal transplantation due to at least one of three major high-risk characteristics (stromal neovascularization ≥ two quadrants, inflammation/perforation, re-transplantation) in a single-center tertiary referral clinic, and to determine the individual effect of these high-risk factors on time to graft failure and survival.
Methods
This retrospective study was conducted at the Department of Ophthalmology and Optometry at the Medical University of Vienna. All study investigations complied with the tenets of the Declaration of Helsinki. The study was approved by the Ethics Committee of the Medical University of Vienna (EK1295/2022).
We included data from adult patients who were referred to the tertiary clinic for corneal diseases for HR penetrating keratoplasty (KP) between March 2014 and September 2022. High-risk criteria were defined as 1. history of prior KP, 2. stromal neovascularization in at least 2 corneal quadrants, and/or 3. signs of significant inflammation or manifest perforation at the time of surgery based on the criteria suggested by the the Collaborative Corneal Transplantation Studies Research Group. Inflammation (defined as conjunctival/limbal injection with or without chemosis, ocular pain, discharge, eyelid swelling) and perforation (with signs of inflammation as defined before, either of infectious or non-infectious nature) were diagnosed at the slit-lamp. Data were obtained from electronic clinical reports. Exclusion criteria were incomplete medical records of the surgery itself or incomplete follow-up information. Routine follow-up visits after keratoplasty were scheduled 1 day, 1 week, 1 month, 3 months, 6 months, and 1 year after surgery. After this time point, intervals between follow-up visits were left to the discretion of the surgeon.
Post-operative standard medical schedule included a topical corticosteroid formulation (either prednisolone acetate or dexamethasone-21-dihydrogen phosphate) with gradual tapering of the frequency from hourly (first week), over 5 times daily (first month), to a reduced frequency of one drop less every month until month 6, with a maintenance dose of one drop every day from month 6 to month 12. The steroid treatment was complemented by a fluorchinolone antibiotic in topical formulation for the first month, as well as artificial tears. Selected patients undergoing repeated keratoplasty were treated systemic mycophenolate mofetil (CellCept, 500mg) at a dose of 1000 mg twice daily for at least 1 year after KP, or reduced to 500mg twice daily in the event of poor tolerability, with strictly ongoing monthly laboratory examinations. If systemic immunosuppression was not suitable due to any reason, tacrolimus eye drops (0.01%) were prescribed three times daily for topical administration in the affected eye. These supplementations to standard post-operative therapy were chosen based on the individual case.
In the event of significant pre-operative stromal neovascularization, accelerated peripheral crosslinking (CXL) (5.4 J/cm2 total energy dose) or fine-needle diathermy was applied in some cases as an angioregressive therapy for pre-operative conditioning of the transplant. These two options were combined with topical bevacizumab three times daily in some of the cases. Topical bevacizumab was also prescribed after surgery to prevent the de-novo sprouting or re-vascularization of the transplant.
Suture removal was performed 12 months after surgery (first row of interrupted sutures) and 13 months after surgery (second row of interrupted sutures), respectively. Maintenance and dose of steroid therapy were left to the discretion of the surgeon.
Statistical Analysis
Only one eye of a patient was selected for the analyses of this study. The right or left eye was randomly chosen in those patients with both eyes eligible (n=8). For quantitative variables, the median as well as the first (Q1) and third quartile (Q3) were calculated. Qualitative variables are reported as absolute frequencies and percentages.
The primary endpoint was defined as graft failure without recovery within the first postoperative year. Corneal graft failure was defined as the irreversible loss of refractive quality of the allograft with loss of transparency. The endpoint was chosen to be dichotomous, since the exact time of graft failure cannot be determined in the majority of cases. Hence, graft failure was either diagnosed in the event of an acute presentation of the patient due to symptoms (redness, pain, etc.) or at a routine follow-up visit (see above). Since we may have included several measurements for an individual patient in the data set (due to multiple KPs during follow-up), analyses were conducted for the 1st, 2nd and 3rd KP separately. Further KPs were not considered in the analyses due to low sample size.
The independent variables in regard to the primary outcome were baseline endothelial cell count (ECC) of the donor (metric), donor age (metric), presence of ≥2 quadrants with stromal neovascularization at baseline (bNV) of the host at the time of surgery (dichotomous), and presence of manifest perforation or significant inflammation (P/I) of the host at the time of surgery (dichotomous). For the 1st KP, the independent variables “bNV” and “P/I” were combined to one categorical variable with three levels (“bNV only”, “P/I only” “P/I plus bNV”), since patients with neither bNV nor P/I nor re-OP are excluded from the study according to the inclusion/exclusion criteria. For the 2nd and 3rd KP, only the main effects of bNV and P/I but not the interaction between these two variables were analyzed due to the low number of patients with bNV plus P/I (2nd KP: n = 5, 3rd KP: n = 1).
For each independent variable, a univariate logistic regression model was calculated next to multivariable logistic regression models. Patients without event (ie, graft failure) and an observation period less than one year were excluded from the logistic regression models.
Graphical visualization of the time until graft failure was done by Kaplan–Meier curves for the 1st, 2nd and 3rd KP separately, whereby the complete observation period as well as only the first year after KP was considered. Patients without event (ie, graft failure) were censored at the day of the last observation.
Kaplan–Meier curves were additionally used to illustrate the time from KP until “first neovascularization (re-) formation after KP” (defined as appearance of stromal NV on the graft/beyond the graft-host junction after KP identified in slit-lamp examination) stratified by 1st, 2nd and 3rd KP. P-values <0.05 were considered statistically significant. Due to the exploratory character of the study, no multiplicity correction was applied. The interpretation of the p-values is descriptive. Statistical analyses were conducted with R 4.3.1.
Results
This retrospective study includes data of a total of 375 hR KPs performed in 257 patients between March 2014 and September 2022.
The median age of the recipient patient at surgery was 58 years (Q1-Q3: 46–70). The median age of the donor at the time of death was 61 years (Q1-Q3: 53–68), with a median ECC of the transplant of 2512 cells/mm2 (Q1-Q3: 2381–2650 cells/mm2). One-hundred thirty-two (35%) patients were phakic at the time of surgery, whereas 156 (42%) were pseudophakic and 87 (23%) were aphakic.
Table 1 shows the cause for the included KPs to be classified as HR KP, which shows that the majority (n=260) of KPs were HR cases due to the re-transplantation. This number includes patients with or without further presence of inflammation, significant neovascularization or perforation at the time of surgery.
 |
Table 1 Cause for High-Risk Classification, 371 Surgeries (254 Patients, 254 Eyes – 4 Surgeries With More Than 2 Previous KPs but Unknown Number of Total Previous KPs Not Shown in the Table) |
Among the total of 257 eyes of 257 patients with 375 KPs, 185 (49%) experienced treatment-relevant intraocular pressure deterioration after surgery.
Concerning the main outcome measure of this study, Figure 1 shows Kaplan–Meier curves for the first, second, and third keratoplasty performed in these HR transplant eyes, which plot the time until graft failure outcome.
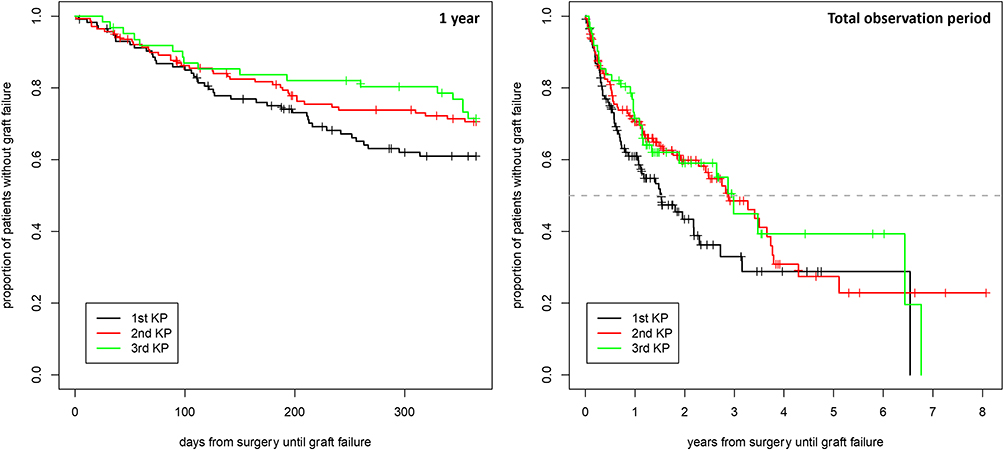 |
Figure 1 Time to graft failure. The left panel shows Kaplan–Meier curves for the time to event in days for the first year of observation, the right panel presents the total observation period. The colored curves represent data for the first, second and third keratoplasty separately. KP: keratoplasty. A grey dashed line was drawn at y = 0.5 (ie, 50% failures). |
Table 2 shows the estimates for the proportion of patients with graft survival 1 year after the first, second, and third KP, respectively. Kaplan–Meier estimates refer to the curves in the figures outlined below.
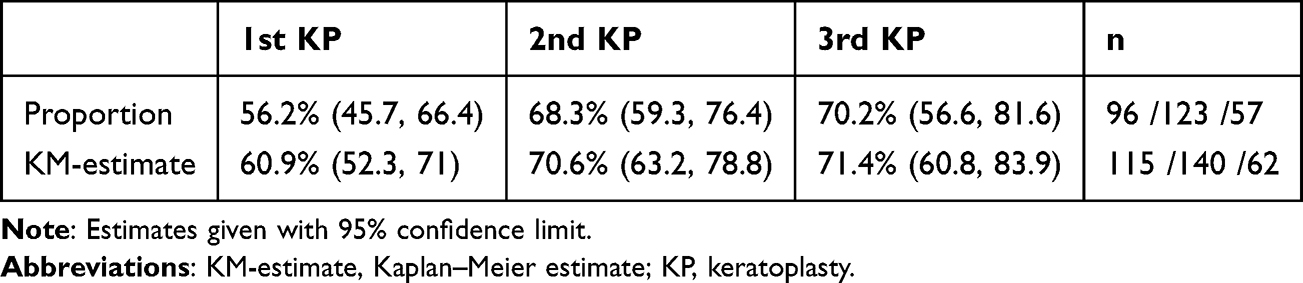 |
Table 2 Graft Survival 1 year After Surgery |
Of the 202 transplants with graft failure or immune rejection episodes, 10 eyes (5%) did not receive ultimate re-KP, 128 eyes (63%) underwent one, 41 eyes (20%) two, 7 eyes (3%) three and 16 eyes (8%) even four re-KPs during the observation period, respectively.
Graft failure occurred in 190 (51%) of the 375 surgeries during a total follow-up period of up to 97 months. One-hundred eighty-five (49%) did not experience graft failure, among which, 12 transplants underwent immune rejection episodes that experienced recovery of these episodes. Causes for graft failure were immune rejection (n=55, 29%), corneal melt (n=37, 19%), infection (n=32, 17%) and unknown cause including clouding/scarring of the transplant (n=66, 35%).
The median time (95% CI) from KP until diagnosis of graft failure was 559 (392, 994) days for the 1st KP, 1052 (833, 1375) days for the 2nd KP and 1089 (689, inf) for the 3rd KP.
One-hundred and nineteen eyes developed stromal NV after KP (32%), whereas in 38 (32%) of these eyes only one quadrant, in 28 (24%) eyes two quadrants, in 4 (3%) eyes three quadrants, and in 49 (41%) eyes all four quadrants were affected, respectively. The median time (95% CI) until first stromal NV (re-)formation after KP was 739 days (550, inf) and 1566 days (1055, inf) for the 1st and the 2nd KP. For the third KP, the median time was not reached.
Table 3 shows an overview of treatments that were used in addition to the standard treatment protocol described in the methods section.
 |
Table 3 Additional Therapy in High-Risk Keratoplasty, 375 Surgeries (257 Patients, 257 Eyes) |
Outcome Considering the First Keratoplasty During the Study Period
The univariate logistic regression models revealed a statistically significant effect of “the cause of high-risk transplantation” on outcome if considering only the first KP in each patient (global test: p = 0.010). The odds for graft failure was significantly higher for patients with P/I only compared to patients with bNV only (OR [95% CI]: 4.2 [1.6; 11.3], p=0.0041) and also higher for patients with P/I plus bNV compared to bNV only (OR [95% CI]: 4.3 [1.2; 15.4], p = 0.023), whereas patients with P/I only did not significantly differ from those with P/I plus bNV (OR [95% CI]: 0.97 [0.31; 3.07], p = 0.96).
Baseline ECC (OR (95% CI): 1.00 (0.99; 1.00), p = 0.09) and donor age (OR (95% CI): 1.01 (0.98; 1.04), p = 0.53) did not prove statistically significant in the univariate logistic regression models.
In the multivariable logistic regression model, only “the cause of high-risk transplantation” remained statistically significant in regards to KP outcome and graft failure (global test: p = 0.012).
Outcome Considering the Second Keratoplasty During the Study Period
In regards to those patients who underwent a second KP during the study period, the univariate logistic regression models revealed a statistically significant effect of baseline P/I, ECC, and donor age. With increased ECC, the odds for an event decreased (OR (95% CI): 0.998 (0.996; 1), p = 0.015), whereas with higher donor age the odds for an event increased (OR (95% CI): 1.04 (1.00; 1.07), p = 0.049). The odds for graft failure were higher for patients with P/I at baseline compared with those patients without P/I at baseline (OR (95% CI): 6.16 (2.24; 16.97), p = 0.0004). Baseline NV did not prove statistically significant in the univariate logistic regression models for the second performed KP (OR (95% CI): 0.67 (0.28; 1.61), p = 0.37).
The multivariable logistic regression model only showed baseline P/I to be statistically significant affecting the outcome of the second KP (OR (95% CI): 5.00 (1.72; 14.51), p = 0.003).
Outcome Considering the Third Keratoplasty During the Study Period
No statistically significant effects of the independent baseline variables on outcome of the third KP could be observed, whereby it has to be noted that the sample size was small (ECC, donor age: n = 51, thereof 13 events, P/I, bNVs: n = 57, thereof 17 events).
The Kaplan–Meier curves in Figure 2 show the influence of baseline NV and baseline P/I on the outcome of the second, and third KP, respectively, in regards to the first year of follow-up, as well as the comparison between patients with baseline NV versus patients with P/I versus patients with baseline NV plus P/I for the first KP. The respective Kaplan–Meier curves are presented in regards to total observation period in Figure 3.
 |
Figure 2 Influence of baseline neovascularization and/or perforation/inflammation status on graft failure in the first year of observation. The y-axes represent the proportion of eyes without event (= graft failure). The x-axes represent the time to event after surgery in days. Left panel: For the first keratoplasty, Kaplan–Meier curves are stratified by subgroup (bNV only, P/I only, bNV + P/I). Kaplan–Meier curves are shown for the second (panels in the middle column) and third (panels in the right column) keratoplasty separately, depending on baseline neovascularization status (top row: 0= no baseline neovascularization; 1= baseline neovascularization) and baseline perforation or inflammation status (bottom row). bNV: neovascularization at baseline; P/I: perforation/inflammation at baseline). |
 |
Figure 3 Influence of baseline neovascularization and/or perforation/inflammation status on graft failure in the total observation period. The y-axes represent the proportion of eyes without event (= graft failure). The x-axes represent the time to event after surgery in years. Left panel: For the first keratoplasty, Kaplan–Meier curves are stratified by subgroup (bNV only, P/I only, bNV + P/I). Kaplan–Meier curves are shown for the second (panels in the middle column) and third (panels in the right column) keratoplasty separately, depending on baseline neovascularization status (top row: 0= no baseline neovascularization; 1= baseline neovascularization) and baseline perforation or inflammation status (bottom row). bNV: neovascularization at baseline; P/I: perforation/inflammation at baseline). |
Discussion
Corneal graft failure is defined as the irreversible loss of refractive quality with loss of transparency and persistent, increased corneal thickness of the allograft, which can be immune or non-immune mediated.21 The threat to experience graft failure is increased in high-risk host corneas.
In this single-center tertiary referral series including data of 375 hR KPs performed in 257 patients between March 2014 and September 2022, graft failure occurred in 190 (51%) of 375 KPs. Among these, the most frequently identified cause for failure was immune rejection (n=55, 29%), whereas in a majority of cases (n=66, 35%) the reason for failure remained undefined. This finding is in line with literature reports, which outline immune rejection as the leading cause of graft decompensation, accounting for over half of these cases,21 with a reported incidence that varies in different studies between 2.3% and 68%.21,22 Literature shows that at least one episode of immune rejection is experienced by about 30% of all corneal transplants, whereas one-third of these eventually lead to ultimate failure.23,24 We here report that only 12 transplants (3%) of high-risk eyes undergoing immune rejection episodes showed full recovery after these episodes.
Immune rejection of corneal transplants is initiated by sensitization of the host to donor antigens and subsequent activation of dendritic cells (antigen presenting cells), which in turn induce proliferation of T-cells in the draining lymph nodes. The efferent phase, which is driven by the transport of immune effector cells to the graft site via blood vessels, is responsible for the T-cell dependent release of cytokines, which ultimately results in graft rejection.22,25 It was shown that HR recipients with previous graft rejection experience accelerated rejection after re-transplantation due to memory T-cells.26 This means that in such HR eyes, two types of adaptive immune responses are present, namely, the activation of allospecific T-cells, as well as the re-activation of memory T-cells.27 In this study, the majority (n=260) of KPs were classified as HR for being a re-transplantation.
Figure 1 illustrates that the outcome seems to be better for the 2nd and 3rd KP compared to the 1st KP. For the 1st KP, median time until graft failure was observed at 559 [392; 994] days, ie, in the second year after KP, whereas for patients with 2nd and 3rd KP median time was 1052 [833; 1375] days and 1089 [689; inf) days, respectively, ie, 50% failures were reached at the end of the third year after KP. The most likely explanation for this observation is that subsequent transplantations (2nd, 3rd, etc) were less likely performed in inflamed (perforated) eyes, which is illustrated in Table 1(62% P/I or bNV + P/I for 1st KP versus 17% for 2nd and 3rd KP).
In this study, the baseline presence of manifest perforation or acute inflammation (P/I) at the time of surgery was the only independent factor that remained statistically significant in regards to KP outcome (graft failure) in the multivariable logistic regression model (also see Figures 2 and 3). This supports the hypothesis that baseline P/I may be of greater impact on short-term graft survival compared with baseline NV, ECC, or donor age. However, this effect could only be observed for the 1st and 2nd KP performed in this patient population. After the 3rd KP, none of these independent variables showed significant effects on outcome in the multivariable logistic regression model, which may partly be explained by the low number of observations (n=57) being one limitation of this study.
Furthermore, Figures 2 and 3 depict a pattern of Kaplan–Meier curves, which suggests a better outcome for patients with bNV only compared to those with P/I only and those with P/I and NV at baseline for the 1st KP in the first postoperative year, as well as the total observation period. Considering the 2nd KP, the Kaplan–Meier curves of patients with or without bNV approach each other, and for the 3rd KP the curves depict better outcome in those without bNV (see Figures 2 and 3, top rows).
For the 2nd or 3rd KP, if considering baseline P/I status, patients without baseline P/I, irrespective of the observation period (first year of observation versus total study period) experienced better outcome compared with those with baseline P/I (see Figures 2 and 3, bottom rows).
One-hundred and nineteen eyes developed stromal NV after KP (32%), with a median time (95% CI) until NV (re-) formation of 739 days (550, inf) and 1566 days (1055, inf) for the 1st and the 2nd KP, respectively.
We observed that the most frequent anti-angiogenic therapy applied in this series was peripheral CXL and/or topical anti-VEGF medication (bevacizumab). These are two of a variety of strategies, which have been proposed for safe, pre-operative “(lymph)-angioregression” previously proposed including topical, stromal or subconjunctival anti-VEGF agents, with or without additional mechanical occlusive procedures such as fine-needle diathermy,28–30 argon laser- or cryo- coagulation or the recently introduced peripheral CXL technique, which might show an additional regressive effect on lymphatic vessels.31,32
Keratoplasty belongs to the most successful forms of transplantation with good functional recovery. However, we still face a lack of consensus on the optimal approach for rejection prevention and treatment, particularly in HR recipients. In this group of patients, topical corticosteroids are usually continued at a low dose for indefinite time spans to mitigate the risk of immune rejection. The evidence for the beneficial use of systemic immunosuppression is limited, although it seems justified, as experimental studies have shown that alloantigen sensitization occurs in the regional lymph nodes, rather than in the eye.33 Next to tacrolimus and mycophenolate mofetil, the evidence is mostly confined to cyclosporine, with though inconsistent results.34,35 With their use, survival rates of HR corneal grafts have been reported to range between 65% and 83% with good tolerance in most patients.36–40 However, the definition of a HR transplant differed between studies, as did the immunosuppression protocols and the duration of treatment. Furthermore, it is important to note that systemic immunosuppression sets the affected patient at risk for significant side effects (ie, infections) that have to be considered and discussed.
Although the evidence for topical compared with systemic immunosuppressants for rejection prevention is limited, some surgeons prefer topical administration of tacrolimus or cyclosporine. Compared with cyclosporine, tacrolimus provides the advantage of being more hydrophilic, ensuring higher trans-corneal diffusion, with satisfying results for safety and efficiency in the prevention of graft rejection.39–41
This study is limited by its retrospective nature and the limited follow-up period for part of the surgeries. However, we present outcome data of a large cohort of HR transplants of a single cornea tertiary referral center, with strict inclusion criteria for HR recipients, being re-transplantation, significant stromal neovascularization, and/or perforation/acute inflammation, whilst setting the focus on exploring the influence of these variables on outcome.
Conclusion
In conclusion, we provide evidence for acute inflammation or manifest perforation at the time of surgery being the most important influencing variables on transplant survival in HR keratoplasty, with 1-year survival rates being in line with previous reports. Understanding the underlying pathology and approaching a personalized pre- and post-operative treatment schedule next to optimal donor quality, meticulous tissue handling, and adequate post-operative care are crucial factors leading to better visual and functional outcome in this high-risk population.
Data Sharing Statement
The datasets generated during and analyzed during the current study are available from the corresponding author upon reasonable request. Patient consent was waived due to the retrospective nature of the study. All patients were consecutively numbered and pseudonymized for the analysis. Only authorized personnel has access to the data, which are stored on a restricted-access computer at the Department of Ophthalmology and Optometry, AKH Vienna.
Acknowledgments
This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-3854590/v1
Funding
This work was supported by the No funding/support to declare.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Billingham RE, Boswell T. Studies on the problem of corneal homografts. Proc R Soc Lond B Biol Sci. 1953;141(904):392–406. doi:10.1098/rspb.1953.0049
2. Medawar PB. Immunity to homologous grafted skin; the fate of skin homografts transplanted to the brain, to subcutaneous tissue, and to the anterior chamber of the eye. Br J Exp Pathol. 1948;29(1):58–69.
3. Bock F, Onderka J, Braun G, et al. Identification of novel endogenous anti(lymph)angiogenic factors in the aqueous humor. Invest Ophthalmol Vis Sci. 2016;57(15):6554–6560. doi:10.1167/iovs.15-18526
4. Abdelfattah NS, Amgad M, Zayed AA, Hussein H, Abd El-Baky N. Molecular underpinnings of corneal angiogenesis: advances over the past decade. Int J Ophthalmol. 2016;9(5):768–779. doi:10.18240/ijo.2016.05.24
5. Faraj LA, Hashmani K, Khatib T, Al-Aqaba M, Dua HS. The changing face of corneal graft rejection. Br J Ophthalmol. 2012;96(8):1049–1050. doi:10.1136/bjophthalmol-2012-301828
6. Niederkorn JY. High-risk corneal allografts and why they lose their immune privilege. Curr Opin Allergy Clin Immunol. 2010;10(5):493–497. doi:10.1097/ACI.0b013e32833dfa11
7. Urbańska K, Woźniak M, Więsyk P, et al. Management and Treatment Outcomes of High-Risk Corneal Transplantations. J Clin Med. 2022;11(19):5511. doi:10.3390/jcm11195511
8. Jabbehdari S, Rafii AB, Yazdanpanah G, Hamrah P, Holland EJ, Djalilian AR. Update on the management of high-risk penetrating keratoplasty. Curr Ophthalmol Rep. 2017;5(1):38–48. doi:10.1007/s40135-017-0119-2
9. Di Zazzo A, Kheirkhah A, Abud TB, Goyal S, Dana R. Management of high-risk corneal transplantation. Surv Ophthalmol. 2017;62(6):816–827. doi:10.1016/j.survophthal.2016.12.010
10. Guilbert E, Bullet J, Sandali O, Basli E, Laroche L, Borderie VM. Long-term rejection incidence and reversibility after penetrating and lamellar keratoplasty. Am J Ophthalmol. 2013;155(3):560–569.e2. doi:10.1016/j.ajo.2012.09.027
11. Ziaei M, Manzouri B. Topical cyclosporine in corneal transplantation. Cornea. 2015;34(1):110–115. doi:10.1097/ICO.0000000000000291
12. Kharod-Dholakia B, Randleman JB, Bromley JG, Stulting RD. Prevention and treatment of corneal graft rejection: current practice patterns of the Cornea Society (2011). Cornea. 2015;34(6):609–614. doi:10.1097/ICO.0000000000000403
13. Garg P, Krishna PV, Stratis AK, Gopinathan U. The value of corneal transplantation in reducing blindness. Eye. 2005;19(10):1106–1114. doi:10.1038/sj.eye.6701968
14. The Collaborative Corneal Transplantation Studies Research Group. The collaborative corneal transplantation studies (CCTS). Effectiveness of histocompatibility matching in high-risk corneal transplantation. Arch Ophthalmol. 1992;110(10):1392–1403. doi:10.1001/archopht.1992.01080220054021
15. Chauhan SK, Dohlman TH, Dana R. Corneal lymphatics: role in ocular inflammation as inducer and responder of adaptive immunity. J Clin Cell Immunol. 2014;5. doi:10.4172/2155-9899.1000256
16. Cursiefen C, Cao J, Chen L, et al. Inhibition of hemangiogenesis and lymphangiogenesis after normal-risk corneal transplantation by neutralizing VEGF promotes graft survival. Invest Ophthalmol Vis Sci. 2004;45(8):2666–2673. doi:10.1167/iovs.03-1380
17. Catry L, Van den Oord J, Foets B, Missotten L. Morphologic and immunophenotypic heterogeneity of corneal dendritic cells. Graefes Arch Clin Exp Ophthalmol. 1991;229(2):182–185. doi:10.1007/BF00170554
18. Dua HS, Azuara-Blanco A. Corneal allograft rejection: risk factors, diagnosis, prevention, and treatment. Indian J Ophthalmol. 1999;47(1):3–9.
19. Coster DJ, Williams KA. The impact of corneal allograft rejection on the long-term outcome of corneal transplantation. Am J Ophthalmol. 2005;140(6):1112–1122. doi:10.1016/j.ajo.2005.07.024
20. Armitage WJ, Goodchild C, Griffin MD, et al. High-risk corneal transplantation: recent developments and future possibilities. Transplantation. 2019;103(12):2468–2478. doi:10.1097/TP.0000000000002938
21. Qazi Y, Hamrah P. Corneal allograft rejection: immunopathogenesis to therapeutics. J Clin Cell Immunol. 2013;2013(Suppl 9). doi:10.4172/2155-9899.S9-006
22. Lam H, Dana MR. Corneal graft rejection. Int Ophthalmol Clin. 2009;49(1):31–41. doi:10.1097/IIO.0b013e3181924e23
23. Panda A, Vanathi M, Kumar A, Dash Y, Priya S. Corneal graft rejection. Surv Ophthalmol. 2007;52(4):375–396. doi:10.1016/j.survophthal.2007.04.008
24. Dana MR, Qian Y, Hamrah P. Twenty-five-year panorama of corneal immunology: emerging concepts in the immunopathogenesis of microbial keratitis, peripheral ulcerative keratitis, and corneal transplant rejection. Cornea. 2000;19(5):625–643. doi:10.1097/00003226-200009000-00008
25. Amouzegar A, Chauhan SK, Dana R. Alloimmunity and tolerance in corneal transplantation. J Immunol. 2016;196(10):3983–3991. doi:10.4049/jimmunol.1600251
26. Vitova A, Kuffová L, Klaska IP, Holan V, Cornall RJ, Forrester JV. The high-risk corneal regraft model: a justification for tissue matching in humans. Transpl Int. 2013;26(4):453–461. doi:10.1111/tri.12055
27. Yu T, Rajendran V, Griffith M, Forrester JV, Kuffová L. High-risk corneal allografts: a therapeutic challenge. World J Transplant. 2016;6(1):10–27. doi:10.5500/wjt.v6.i1.10
28. Pillai CT, Dua HS, Hossain P. Fine needle diathermy occlusion of corneal vessels. Invest Ophthalmol Vis Sci. 2000;41(8):2148–2153.
29. Le VN, Schneider AC, Scholz R, Bock F, Cursiefen C. Fine needle-diathermy regresses pathological corneal (Lymph)angiogenesis and promotes high-risk corneal transplant survival. Sci Rep. 2018;8(1):5707. doi:10.1038/s41598-018-24037-3
30. Hos D, Le VN, Hellmich M, et al. Risk of corneal graft rejection after high-risk keratoplasty following fine-needle vessel coagulation of corneal neovascularization combined with bevacizumab: a pilot study. Transplant Direct. 2019;5(5):e452. doi:10.1097/TXD.0000000000000894
31. Hou Y, Le VN, Tóth G, et al. UV light crosslinking regresses mature corneal blood and lymphatic vessels and promotes subsequent high-risk corneal transplant survival. Am J Transplant. 2018;18(12):2873–2884. doi:10.1111/ajt.14874
32. Schaub F, Hou Y, Zhang W, Bock F, Hos D, Cursiefen C. Corneal crosslinking to regress pathologic corneal neovascularization before high-risk keratoplasty. Cornea. 2021;40(2):147–155. doi:10.1097/ICO.0000000000002406
33. Yamagami S, Dana MR. The critical role of lymph nodes in corneal alloimmunization and graft rejection. Invest Ophthalmol Vis Sci. 2001;42(6):1293–1298.
34. Rumelt S, Bersudsky V, Blum-Hareuveni T, Rehany U. Systemic cyclosporin A in high failure risk, repeated corneal transplantation. Br J Ophthalmol. 2002;86(9):988–992. doi:10.1136/bjo.86.9.988
35. Inoue K, Kimura C, Amano S, et al. Long-term outcome of systemic cyclosporine treatment following penetrating keratoplasty. Jpn J Ophthalmol. 2001;45(4):378–382. doi:10.1016/s0021-5155(01)00339-2
36. Birnbaum F, Mayweg S, Reis A, et al. Mycophenolate mofetil (MMF) following penetrating high-risk keratoplasty: long-term results of a prospective, randomised, multicentre study. Eye. 2009;23(11):2063–2070. doi:10.1038/eye.2008.402
37. Reinhard T, Reis A, Böhringer D, et al. Systemic mycophenolate mofetil in comparison with systemic cyclosporin A in high-risk keratoplasty patients: 3 years’ results of a randomized prospective clinical trial. Graefes Arch Clin Exp Ophthalmol. 2001;239(5):367–372. doi:10.1007/s004170100285
38. Sloper CM, Powell RJ, Dua HS. Tacrolimus (FK506) in the management of high-risk corneal and limbal grafts. Ophthalmology. 2001;108(10):1838–1844. doi:10.1016/s0161-6420(01)00759-x
39. Joseph A, Raj D, Shanmuganathan V, Powell RJ, Dua HS. Tacrolimus immunosuppression in high-risk corneal grafts. Br J Ophthalmol. 2007;91(1):51–55. doi:10.1136/bjo.2006.097428
40. Chatel MA, Larkin DF. Sirolimus and mycophenolate as combination prophylaxis in corneal transplant recipients at high rejection risk. Am J Ophthalmol. 2010;150(2):179–184. doi:10.1016/j.ajo.2010.03.010
41. Van Eyk AD, Van Der Bijl P, Meyer D. In vitro diffusion of the immunosuppressant tacrolimus through human and rabbit corneas. J Ocul Pharmacol Ther. 2007;23(2):146–151. doi:10.1089/jop.2006.0105
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.