")
Back to Journals » Patient Preference and Adherence » Volume 18
Influential Factors for Self-Management Among Patients with Diabetic Retinopathy: A Structural Equation Model Analysis
Received 27 December 2023
Accepted for publication 25 July 2024
Published 2 August 2024 Volume 2024:18 Pages 1619—1628
DOI https://doi.org/10.2147/PPA.S456947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Rina Sa,1 Jingjing Zhang,1 Haiyang Xu2
1Department of Ophthalmology, The First Hospital of Jilin University, Changchun, People’s Republic of China; 2Department of Anesthesia, The First Hospital of Jilin University, Changchun, People’s Republic of China
Correspondence: Haiyang Xu, Department of Anesthesia, The First Hospital of Jilin University, 1 Xinmin Dajie, Chaoyang District, Changchun City, Jilin Province, People’s Republic of China, Tel +8615804303312, Fax +0431-81875567, Email [email protected]
Purpose: To investigate the influencing factors of self-management of diabetic retinopathy (DR) by constructing a structural equation model (SEM) to analyze the relationships among self-management behavior, perceived social support, and trait coping style as well as to determine the influencing path in order to provide a theoretical reference for exploring a multipath health management model that can be used to improve the quality of life of DR patients.
Patients and Methods: A total of 388 patients with DR were enrolled in this cross-sectional study conducted from January 2020 to January 2023. All subjects completed a general questionnaire and were assessed by the Self-management Scale for Patients with Diabetic Retinopathy, the Perceived Social Support Scale, and the Trait Coping Style Scale. Structural equation modeling was employed to examine the relationship between self-management and its influencing factors. The bootstrap method was used to examine the path relationships among self-management, perceived social support, and trait coping styles in DR patients.
Results: A total of 346 valid questionnaires were collected in this study, with a response rate of 89% (346/388). The average score of self-management of DR patients was 69.50± 18.32, and it was significantly positively correlated with perceived social support and positive coping (r=0.624, r=0.578, both P< 0.01). The total effect of perceived social support on DR self-management was 1.439, with a direct effect of 1.056 and an indirect effect of 0.384. Positive coping played a mediating role in perceived social support and self-management.
Conclusion: The self-management of DR was at an intermediate level. Perceived social support and trait coping styles were important influencing factors for self-management behavior in DR patients. Therefore, improving perceived social support and trait coping styles can promote the self-management behavior of DR patients, reduce their psychological burden, and improve their compliance and quality of life.
Keywords: diabetic retinopathy, self-management, social support, coping style, structural equation model
Introduction
Diabetic retinopathy (DR) is one of the most common microvascular complications in diabetic patients due to poor blood glucose control, and the prevalence of DR is about 27% worldwide. DR is a chronic, progressive, and painless disease that can cause irreversible vision damage and blindness.1 It is estimated that the number of patients suffering from DR worldwide will increase to 130 million by 2030, and 160 million by 2045,2 leading to an increased economic burden and an impaired quality of life. Existing evidence shows that DR is preventable and controllable; therefore, early prevention and scientific management are of great significance in the management of DR.
Engel proposed that traditional biomedical models did not leave space for social, psychological, and behavioral factors associated with diseases in the late 1980s.3 Patient empowerment has achieved a shift from traditional biomedical models to patient-centered approaches. Self-management refers to the ability of individuals, together with their families, communities, and healthcare professionals, to manage the symptoms, treatment, and lifestyle changes of diseases as well as control the psychological, socio-cultural, and spiritual consequences arising from their physical condition.4 It emphasizes identifying and discovering problems from the patient’s perspective as a revolution in nursing concepts and methods enhancing their initiative. Effective self-management includes the ability to monitor one’s own condition and maintain the cognitive, behavioral, and emotional responses necessary for a satisfactory quality of life.
A recent study has shown that early standardized treatment and effective self-management can reduce the blindness rate of proliferative DR patients from 50% to less than 5%, which can maximize their prognosis and avoid visual impairment caused by DR.5 However, another study has indicated that nearly 80% of diabetic patients have poor awareness of DR and its prevention and treatment.6 The lack of knowledge about related diseases and inadequate self-management lead to poor blood glucose control, further accelerating microvascular disease and increasing the readmission of patients. Therefore, it is urgent to improve the self-management of patients with DR.
Patients with DR can be affected by various symptoms, decreased vision, impaired self-care ability, and lower social participation in daily life. Support from family and society is crucial for diabetic patients. Social support is an important aspect of psychological regulation in DR patients, alleviating their depression and anxiety. In addition, poor social support can result in an increase in the depression level of DR patients, which aggravates disease progression, leading to poor blood glucose control and poor compliance to diabetes treatment.7,8 Previous studies also have demonstrated that family and friends can have a positive impact on patients’ psychology and behavior, improve their confidence, and regulate their behavior.9 Therefore, family, social, and peer support are crucial for the management of DR in affected patients.
The complex factors of psychology, emotions, and social relationships, combined with various pressures and burdens, make DR patients prone to anxiety and depression, often causing them to be unable to respond to diseases. A longitudinal study has shown that avoidance coping strategies (such as passive coping) can cause patients to lose vision over time as well as affect their quality of life and clinical outcomes related to vision.10 Avoidance-oriented coping efforts may have less of an impact on emotions in the short term, but they can reduce the patient’s sense of happiness in the long run. DR patients with poor problem-solving abilities may also have a higher risk of depression due to their seeing loss of vision as a burden on others and feeling ashamed or embarrassed about it, thus putting them at risk of facing mental health problems.11 Therefore, patient self-management helps maintain and prevent disease progression, and it requires lifelong persistence.
Self-management is a complex behavioral process related to many factors, including patient characteristics, religious beliefs,12 social support,13 and so on. Current research uses various research methods, including qualitative research,7,9 quantitative research,14,15 and mixed qualitative and quantitative research.16 In terms of DR, previous studies have investigated the relationships among diabetes knowledge, social support, health beliefs, treatment compliance, and self-management behavior in patients with DR.17 Yang et al used the self-care scale for type 2 diabetes developed by Toobert et al18 while it did not consider the difference between self-care and self-management, the former is more concentrated on disease control and ignores the psychological aspects. This study aimed to provide an approach and feasible basis for further exploring the different influencing factors of self-management in patients with DR.
Towards this aim, a quantitative study on the Self-management Scale for Diabetic Retinopathy, the Perceived Social Support Scale, and the Trait Coping Style Scale in DR patients was conducted, exploring the impact of DR patients’ perceived social support and trait coping style on self-management of DR while the patients were under medical care. We also performed path analysis by constructing a structural equation model to explore a multi-path dynamic health self-management mode. A structural equation model is a complex composite statistical hypothesis that consists of a measurement model and a structural model. It is used for considering factor analysis and the linear regression model simultaneously when examining complex associations.
The findings of this study will help to implement targeted mental health interventions and continuous care in clinical practice. By preventing the occurrence of DR and reducing the clinical complications and harm caused by DR, the treatment adherence and the quality of life of DR patients will be improved.
Materials and Methods
Study Population
Convenience sampling was used to enroll in patients with DR admitted to the Ophthalmology Department of a top-three hospital in Jilin Province as the study subjects from January 2020 to January 2023. The inclusion criteria were as follows: (1) patients diagnosed with DR; (2) clear awareness and ability to independently complete the questionnaire; and (3) volunteer to participate in this study and sign informed consent. The exclusion criteria were as follows: (1) patients with retinopathy caused by other diseases; (2) patients with basic diseases, such as hypertension and autoimmune diseases, other than diabetes; (3) patients who did not voluntarily participate in this study. This study was conducted in accordance with the Declaration of Helsinki, and it has been reviewed and approved by the hospital ethics committee (No. 23K279-001). All subjects gave written informed consent for inclusion before they participated.
Data Collection
All subjects completed four questionnaires to collect information about their general situation and self-management behavior via a popular online professional survey platform “Wenjuanxing” (www.wjx.cn). The four questionnaires were as follows: (1) General questionnaire, including sex, age, education level, DR staging, etc. (2) Self-Management Scale for Diabetic Retinopathy, developed by Liu Qiao and Zheng Lina;19 the Cronbach’s scale α value was 0.952, with a test-retest reliability of 0.991 and a split-half reliability of 0.883. This study selected three dimensions and 25 items of blood glucose management (6 items), disease management (13 items), and emotional management (6 items) for the research. (3) Perceived Social Support Scale, written by Zimet et al20 and revised by Jiang Qianjin,21 including three dimensions and 12 items of family support (4 items), friend support (4 items), and other support (4 items); the Cronbach’s α values of the total scale and the three subscales were 0.90, 0.87, 0.82, and 0.90, respectively. (4) Trait Coping Style Scale, developed and revised by Jiang Qianjin et al22 including two dimensions and 20 items of positive coping (10 items) and negative coping (10 items); the Cronbach’s α values were 0.69 and 0.70, respectively. The reliability and validity of all three scales are good and have been verified in other studies.
Statistical Analyses
SPSS23.0 software was used to analyze the data. Descriptive statistical analysis was used to present the characteristics of the study subjects. For continuous data, variables were described as the means and standard deviations (SDs), and the differences between groups were compared using the independent sample t-test. For categorical data, variables were described as counts and percentages, and the differences between groups were compared using the Chi-squared (χ2) test. Correlation analysis (Pearson correlation) was performed to detect the relationships among self-management, perceived social support, and trait coping styles. A structural equation model was constructed by AMOS 24.0 software to analyze the influencing factors of self-management in DR patients, and path analysis was performed. The maximum likelihood method was used for testing the parameter estimation in the conceptual model. The model fit was assessed based on the following model-fit indices: χ2, goodness-of-fit index (GFI), adjusted goodness-of-fit-index (AGFI), incremental fit index (IFI), comparative fit index (CFI), Tucker-Lewis index (TLI), normed fit index (NFI), and root mean square error of approximation (RMSEA). All P<0.05 (two-sided), indicating that the difference was statistically significant.
Results
Demographic Information of the Study Subjects
A total of 346 valid questionnaires were collected, with a response rate of 89% (346/388). The general demographic information of the DR patients is shown in Table 1. All subjects, including 229 females and 117 males, underwent surgery for DR. Most subjects had a high-school education or below and rural cooperative medical insurance. In terms of DR, the majority of the subjects suffered from moderate DR and underwent one surgery for DR.
 |
Table 1 Demographic Information of the Study Subjects |
The total self-management score was 69.50±18.32, with a blood glucose management score of 17.72±4.85, a disease management score of 35.36±10.09, and an emotional management score of 16.42±4.40. The total score of perceived social support was 64.92±13.57, with a family support score of 21.77±4.84, a friend support score of 21.67±4.81, and other support score of 21.48±4.67. The positive coping style score in the DR patients was 36.29±6.27, while the negative coping style score was 30.58±7.01 (Table 2).
 |
Table 2 The Scores of Three Scales in Diabetic Retinopathy Patients |
Correlation Among Self-Management, Perceived Social Support, and Trait Coping Styles in DR Patients
Linear regression was used to detect the relationships among self-management, perceived social support, and trait coping styles. The self-management of DR was significantly positively correlated with the perceived social support (r=0.624, P<0.01) as well as positive coping (r=0.578, P<0.01), while it was not related to negative coping (r=−0.104, P>0.05). Moreover, the perceived social support in DR patients was positively associated with positive coping (r=0.547, P<0.01) (Table 3).
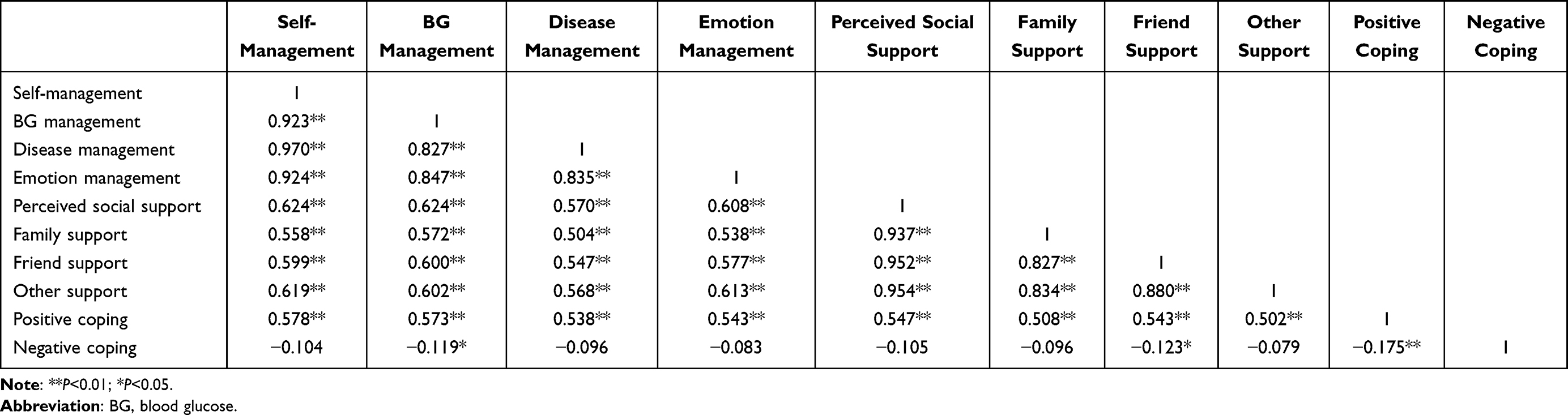 |
Table 3 Correlation Among Self-Management, Perceived Social Support, and Coping Style |
Construction of a Structural Equation Model and Path Analysis of Factors Influencing Self-Management in DR Patients
Correlation analysis suggested that perceived social support and positive coping in DR patients may be influencing factors of self-management. To explore and analyze the relationships and mechanisms among perceived social support, trait coping styles, and self-management behavior, we used a structural equation model and fitted it using the maximum likelihood method to construct a relationship model among the three aspects. Based on theoretical assumptions, the conceptual model was constructed with perceived social support as the independent variable, self-management behavior as the dependent variable, and positive coping as the mediating variable. All paths are shown in Figure 1.
 |
Figure 1 Significant pathways of the final model with standardized parameter estimates. |
The goodness-of-fit index of the model was relatively ideal, and the fitting effect was good. The CMIN/DF GFI was 0.982, the NFI was 0.990, the IFI was 0.996, the CFI was 0.996, the RMSEA was 0.048, and the other fitness index evaluation indicators also met the recommended reference, as shown in Table 4.
 |
Table 4 Goodness-of-Fit and Fitness Test Results of the Model |
The three paths (perceived social support to positive coping, positive coping to self-management, and perceived social support to self-management) were all significant (P<0.01). The patients’ perceived social support and positive coping had a direct positive impact on their self-management behavior (β=0.499 and 0.324, both P<0.01). Additionally, perceived social support had a direct and positive influence on positive coping (β=0.560, P<0.01). Standardized direct, indirect, and mediating effects are summarized in Table 5.
 |
Table 5 Results of the Path Relation Test of the Structural Equation Model |
The Bootstrap Method to Explore the Mediating Effect of Positive Coping on Perceived Social Support and Self-Management
Our study also used the bootstrap method to test the mediating effect of positive coping on perceived social support and self-management. The raw data were randomly sampled 2000 times at a 95% confidence interval. The results are shown in Table 6. The total effect of perceived social support on self-management was 1.439, with a direct effect of 1.056 and an indirect effect of 0.384. The bias correction intervals for positive coping with mediating and direct effects were 0.252–0.552 and 0.815–1.308, respectively; as the values are all greater than zero, the mediating and direct effects are valid. Positive coping played a significant mediating role in the model, with mediating effects and direct effects accounting for 27% and 73%, respectively. Therefore, positive coping was a mediating variable for perceived social support and self-management, and it showed a partially mediating relationship.
 |
Table 6 Bootstrap Mediation Effect Test for Positive Coping |
Discussion
The results of this study demonstrated that the total score of self-management in DR patients was 69.50±18.32, which is a middle level (range: 0–100). The highest score in each dimension was disease management, followed by blood glucose management, and the lowest was emotion management. These findings show that DR patients can use hypoglycemic drugs and control their blood glucose levels according to their doctors’ instructions, reasonably consume three meals per day, and comply with the dietary principles of diabetes. In addition, DR patients can effectively regulate negative emotions, confide in family and friends, view diseases more optimistically, and strive to treat existing diseases with a calm heart. However, it is necessary to establish health care goals based on each individual’s situation, strengthen disease management by providing regular eye examinations, and follow up in a timely manner according to medical advice.
Considering the fact that the majority of the subjects had an education level of high school or below and had new rural cooperative medical insurance, it was rare that the subjects were still able to accept and cooperate with clinical practice. However, the expensive medical cost inevitably brought both psychological and economic burden to the subjects, especially for farmers without a stable income, resulting in a lower level of self-management. Previous studies also have found that diabetic patients with a lower educational level and living in remote areas tend to neglect the complications of diabetes, especially microvascular complications, and suffer from more severe disease.23,24 Therefore, medical staff should pay more attention to patients with a low educational level as well as those with a low family income through targeted health promotion and education to enhance their self-management awareness. Moreover, they should regularly conduct fundus examinations and screening for DR as well as take effective measures to prevent blindness.
This study also showed that the self-management of DR was significantly positively correlated with perceived social support and positive coping, while there was no relationship between self-management and negative coping. Meanwhile, perceived social support had a direct predictive effect on self-management. The latest research by Li Yang et al also has indicated that social support from family, friends, and colleagues plays an important role in the treatment and self-management of DR. Moreover, previous studies have revealed that better social support is associated with better mental health and better health outcomes,25,26 illustrating that better social support also predicts more positive emotions and health outcomes. In addition, these findings can explain why better social support is, to some extent, associated with better compliance of patients. The DR patients experienced support from family, friends, and society, helping them to face the disease with a more positive attitude and better control of negative emotions. At the same time, support from family and society as well as peer education can help those who lack awareness and respect of DR screening to realize the importance of DR screening, leading them to more reasonably manage their own risks of developing a more severe situation such as blindness.27 When patients with DR face multiple physical and mental pressures, their perceived social support can help them better cope with difficulties, overcome psychological and practical obstacles, and voluntarily participate in treatment.
Compared to the available social support, the perceived social support by the patients was determined to be more important. The DR patients with social support also had better medical compliance and more actively cooperated with medical staff for treatment and disease management. Recent meta-analysis results demonstrate that the prevalence of depression among patients with ophthalmic diseases ranges from 5.4% to 57.0% (average: 25%).28 In addition, DR patients were eight times more likely to suffer from depression than those without DR.29 Poor compliance might result in feelings of helplessness in self-management, depression, and worse clinical outcomes. Mendenhall et al further showed that social factors play a more crucial role in depression than psychological factors with regard to diabetic patients.30 Bradley et al even found that DR patients with anxiety and depression avoided healthcare, including DR screening.31 Therefore, the better the social support from different aspects, the more confidence patients can have in their treatment to improve their self-management awareness and make more efforts to self-manage their condition. Thus, medical staff should pay attention to the impact of social support on DR patients and improve patient compliance by enhancing their social support and actively cooperate with disease treatment, thereby helping the patients form good self-management behavior.
The self-management of DR by the patients reflected not only their ability to control the disease but also their effective response to negative emotions generated by social culture and mental psychology. Several studies have shown that emotion is also related to the self-management of diabetes and plays a mediating role between coping styles and self-management. Improving emotion focusing on coping can also ameliorate management in diabetic patients.32 When patients with DR develop subhyaloid hemorrhage, they might experience sudden blurring of vision, shadows, and other subjective feelings, making them feel frightened and anxious. Especially in the preoperative stage, complex emotional reactions such as fear, worry, regret, and self-blame as well as inadequate coping abilities exacerbate the patient’s pain and affect their confidence in postoperative self-management and care.9 Patients urgently hope to receive support from family, friends, and medical staff to help them overcome these difficulties. Therefore, medical staff should communicate in a timely manner, conduct supportive educational activities, provide knowledge and skill guidance, and help patients develop personal goals and positive plans in order to alleviate negative emotions, make their own decisions, improve their ability to cope with emotions and life pressures, and actively explore self-management methods that are suitable for themselves.
This study is the first cross-sectional study in this field to investigate and analyze the relationships among perceived social support, trait coping styles, and self-management behavior in DR patients. We also tried to use structural equation models to analyze the impact paths among various factors. Nevertheless, there are some limitations of this study that must be addressed. Due to the convenience sampling method adopted in this study and the single-center design, selection bias might have occurred and the results may not apply to the general population. Additionally, patient self-management is a dynamic process requiring continuous evaluation and modification. Different stages of chronic diseases also have various effects on the psychology of patients. Therefore, future research should provide a more detailed analysis of patients’ self-management at different stages during disease development and determine its relationship with various influencing factors according to different stages of DR in order to provide more targeted healthcare services.
Conclusion
This study provided evidence for valid relationships among perceived social support, trait coping styles, and self-management behavior in DR patients, thus providing a reliable basis for the construction of self-management nursing intervention. Structural equation model path analysis showed that perceived social support and positive coping styles were important predictive factors for the self-management of DR. In addition, this study revealed a correlation mechanism between the predictive factors and influencing factors of self-management in DR patients, providing a theoretical basis for improving self-management of DR and a specific framework for developing intervention measures in complex clinical settings.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
This study has been reviewed and approved by the Ethics Committee of the First Hospital of Jilin University (Ethics Archive Number: 23K279-001) and was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We would like to thank all of the involved physicians, nurses, technicians, and workers from the communities for dedicating their time and skill to complete this study. We would also like to thank all participants for their dedication in data collection and laboratory measurements.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was used in this study.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Cheloni R, Gandolfi SA, Signorelli C, Odone A. Global prevalence of diabetic retinopathy: protocol for a systematic review and meta-analysis. BMJ Open. 2019;9(3):e022188. doi:10.1136/bmjopen-2018-022188
2. Teo ZL, Tham YC, Yu M, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580–1591. doi:10.1016/j.ophtha.2021.04.027
3. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. doi:10.1126/science.847460
4. Schulman-Green D, Jaser S, Martin F, et al. Processes of self-management in chronic illness. J Nurs Scholarsh. 2012;44(2):136–144. doi:10.1111/j.1547-5069.2012.01444.x
5. Shi J, Zhang C, Zhao Q, Zhang X, Guo L, Jia T. Experience of patients with diabetic retinopathy: a qualitative study. J Adv Nurs. 2023;79(5):1789–1798. doi:10.1111/jan.15457
6. Qi JY, Zhai G, Wang Y, et al. Assessment of knowledge, attitude, and practice regarding diabetic retinopathy in an urban population in Northeast China. Front Public Health. 2022;10:808988. doi:10.3389/fpubh.2022.808988
7. Xu L, Chen S, Xu K, et al. Prevalence and associated factors of depression and anxiety among Chinese diabetic retinopathy patients: a cross-sectional study. PLoS One. 2022;17(4):e0267848. doi:10.1371/journal.pone.0267848
8. Duan F, Liu Y, Chen X, et al. Influencing factors on compliance of timely visits among patients with proliferative diabetic retinopathy in southern China: a qualitative study. BMJ Open. 2017;7(3):e013578. doi:10.1136/bmjopen-2016-013578
9. Zhang M, Zhang C, Chen C, et al. The experience of diabetic retinopathy patients during hospital-to-home full-cycle care: a qualitative study. BMC Nurs. 2023;22(1):58. doi:10.1186/s12912-023-01206-y
10. Sturrock BA, Xie J, Holloway EE, et al. The influence of coping on vision-related quality of life in patients with low vision: a prospective longitudinal study. Invest Ophthalmol Vis Sci. 2015;56(4):2416–2422. doi:10.1167/iovs.14-16223
11. Sturrock BA, Rees G, Lamoureux EL, Wong TY, Holloway E, Fenwick EK. Individuals’ perspectives on coping with vision loss from diabetic retinopathy. Optom Vis Sci. 2018;95(4):362–372. doi:10.1097/OPX.0000000000001209
12. Duke N. Type 2 diabetes self-management: spirituality, coping and responsibility. J Res Nurs. 2021;26(8):743–760. doi:10.1177/17449871211026958
13. Kaya UP, Caydam OD. Association between social support and diabetes burden among elderly patients with diabetes: a cross-sectional study from Turkey. Saudi J Med Sci. 2019;7(2):86–92. doi:10.4103/sjmms.sjmms_44_18
14. Shen A, Wu P, Lu Q, et al. Predicting lymphedema self-management behaviours in breast cancer patients: a structural equation model with the integrated theory of health behaviour change. J Adv Nurs. 2023;79(12):4778–4790. doi:10.1111/jan.15759
15. Kong LN, Zhu WF, Li L, Lei QS, Wang T, Li YL. Self-management behaviors in adults with chronic hepatitis B: a structural equation model. Int J Nurs Stud. 2021;116:103382. doi:10.1016/j.ijnurstu.2019.06.013
16. Gulbahar Eren M, Celik S, Can Ozturk F, Celik M, Yon B. Spiritual well-being, diabetes burden, self-management, and glycemic control among patients with type 2 diabetes in turkey: a descriptive and correlational study. J Relig Health. 2023;62(6):4363–4381. doi:10.1007/s10943-023-01783-x
17. Yang L, Wu Q, Hao Y, et al. Self-management behavior among patients with diabetic retinopathy in the community: a structural equation model. Qual Life Res. 2017;26(2):359–366. doi:10.1007/s11136-016-1396-1
18. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23(7):943–950. doi:10.2337/diacare.23.7.943
19. Liu Q, Zheng L. Development, reliability and validity of self-management scale for patients with diabetic retinopathy. Chin J Mod Nurs. 2022;28(26):3595–3599.
20. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
21. Huang L, Jiang Q, Ren W. The correlation between coping styles, social support, and psychosomatic symptoms in cancer patients. Chin Mental Health J. 1996;10(4):160–161.
22. Vitaliano PP, Maiuro RD, Russo J, Katon W, DeWolfe D, Hall G. Coping profiles associated with psychiatric, physical health, work, and family problems. Health Psychol. 1990;9(3):348–376. doi:10.1037/0278-6133.9.3.348
23. Li C, Zhu B, Zhang J, et al. Epidemiology, health policy and public health implications of visual impairment and age-related eye diseases in mainland China. Front Public Health. 2022;10:966006. doi:10.3389/fpubh.2022.966006
24. Khair Z, Rahman MM, Kazawa K, et al. Health education improves referral compliance of persons with probable Diabetic Retinopathy: a randomized controlled trial. PLoS One. 2020;15(11):e0242047. doi:10.1371/journal.pone.0242047
25. Wu SF, Young LS, Yeh FC, Jian YM, Cheng KC, Lee MC. Correlations among social support, depression, and anxiety in patients with type-2 diabetes. J Nurs Res. 2013;21(2):129–138. doi:10.1097/jnr.0b013e3182921fe1
26. Polikandrioti M, Vasilopoulos G, Gerogianni G, et al. Depression in diabetic foot ulcer: associated factors and the impact of perceived social support and anxiety on depression. Int Wound J. 2020;17(4):900–909. doi:10.1111/iwj.13348
27. Hipwell AE, Sturt J, Lindenmeyer A, et al. Attitudes, access and anguish: a qualitative interview study of staff and patients’ experiences of diabetic retinopathy screening. BMJ Open. 2014;4(12):e005498. doi:10.1136/bmjopen-2014-005498
28. Zheng Y, Wu X, Lin X, Lin H. The prevalence of depression and depressive symptoms among eye disease patients: a systematic review and meta-analysis. Sci Rep. 2017;7(1):46453. doi:10.1038/srep46453
29. Mussa MR, Iseselo MK, Tarimo EAM. Depression and its associated factors among patients with diabetes: a cross-sectional survey at mnazi mmoja referral hospital in Zanzibar, Tanzania. PLoS One. 2023;18(4):e0284566. doi:10.1371/journal.pone.0284566
30. Mendenhall E, Norris SA, Shidhaye R, Prabhakaran D. Depression and type 2 diabetes in low- and middle-income countries: a systematic review. Diabet Res Clin Pract. 2014;103(2):276–285. doi:10.1016/j.diabres.2014.01.001
31. Bradley ER, Delaffon V. Diabetic retinopathy screening in persons with mental illness: a literature review. BMJ Open Ophthalmol. 2020;5(1):e000437. doi:10.1136/bmjophth-2020-000437
32. Miles SR, Khambaty T, Petersen NJ, Naik AD, Cully JA. The role of affect and coping in diabetes self-management in rural adults with uncontrolled diabetes and depressive symptoms. J Clin Psychol Med Settings. 2018;25(1):55–65. doi:10.1007/s10880-017-9527-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.