")
Back to Journals » Orthopedic Research and Reviews » Volume 16
Injection of Amniotic Membrane and Umbilical Cord Particulate for Muscle and Ligament Tears in Collegiate Football Athletes: A Single-Center, Retrospective Study
Authors Krystofiak J
Received 4 July 2024
Accepted for publication 25 November 2024
Published 28 November 2024 Volume 2024:16 Pages 295—301
DOI https://doi.org/10.2147/ORR.S485520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Jason Krystofiak1,2
1Matthew J. Morahan III Health Assessment Center for Athletes, Livingston, NJ, 07039, USA; 2Orthopedics and Sports Medicine, Livingston, NJ, 07039, USA
Correspondence: Jason Krystofiak, RWJBarnabas Health, Orthopedics and Sports Medicine, 200 S. Orange Avenue, Suite 123, Livingston, NJ, 07039, USA, Email [email protected]
Background: Football is a leading cause of sports-related injuries, accounting for more than half of time-loss injuries in men’s collegiate sports. Amniotic membrane and umbilical cord (AM/UC) powder injection is a novel treatment that may aid in functional recovery and return to play in collegiate athletes due to its anti-inflammatory, anti-scarring, and pro-regenerative properties.
Methods: A single-center, retrospective chart review was performed on consecutive college football players who sustained acute muscle or ligament tear and were subsequently treated with 50 or 100 mg injection of AM/UC powder (Clarix Flo, BioTissue, Miami, FL). Data collection included patient demographics, diagnosis, grade and extent of injury, position of the player, time to return to play (in days), and complications.
Results: Ten athletes with tears of the medial collateral ligament (n=3), hamstring (n=6), and abdomen (n=1) were included for analysis. The majority (n=6) of tears were partial (grade 2), with partial to full tears (grade 2± 3) noted in 2 patients, and a complete tear (grade 3) noted in 2 patients. Athletes returned to play 29.6 ± 15.2 days post-injury, with 80% of athletes returning to play within 4 weeks. No complications or re-injuries occurred during the follow-up period of 6 months.
Conclusion: Injection of AM/UC powder is a safe treatment that enables quick return to play in this cohort of football players suffering from muscle or tendon tears. Prospective, randomized studies are warranted to verify whether injection of AM/UC can hasten return to play compared to the current standard treatment.
Level of Evidence: IV.
Keywords: amniotic membrane, hamstring, injection, MCL, return to play, umbilical cord
Introduction
Football is a leading cause of sports-related injuries and accounts for more than half of time-loss injuries in men’s collegiate sports.1 Musculotendinous and ligament injuries are the most common, with muscle sprains and tears accounting for one-third of all injuries resulting in loss of playing time.2,3 Despite the high prevalence of injury and risk of recurrent injury, there is ongoing debate as to which therapeutic interventions are most effective in treating muscle, ligament, and tendon injuries in athletes. While corticosteroid and isolated local anesthetic injections have been used in the treatment of muscle or musculotendinous strains in NFL athletes,4 use of these treatments is generally contraindicated for tendon pathologies and higher-grade muscle or ligament tears due to the risk of tendon or ligament rupture.5,6 Furthermore, complications such as degeneration and muscle contracture have been reported following intra-muscular corticosteroid injection,7 which may deter their use for higher-grade muscle tears. While platelet rich plasma (PRP) injections have been increasingly used for musculoskeletal injuries, there is insufficient evidence supporting its effectiveness and ability to reduce time to return to play.8–10 In fact, a recent randomized, double-blind, controlled trial reported no benefit of PRP injections in acute hamstring injuries on the time to return to play and the re-injury rate within 2 months after return to play.11 Furthermore, fibrosis and failed anatomic reattachment have been observed following PRP injections upon MRI examination,12,13 suggesting the need for novel treatments that aid in regenerative healing by minimizing both inflammation and scarring.
Placenta-derived products, including cryopreserved amniotic membrane (AM) and umbilical cord (UC), have been increasingly used in orthopedics and sports medicine over the last decade due to their anti-inflammatory, anti-scarring, and pro-regenerative properties.14–17 These properties are particularly important for musculoskeletal diseases as scar tissue has been observed as high as 35.7% at six weeks after initial muscle injury which limits normal functional recovery.18 Published real-world evidence from a number of clinical studies supports the use of AM/UC powder for the repair, reconstruction, replacement, or supplementation of a variety of musculoskeletal disorders manifesting pain19 including plantar fasciitis,20 knee and wrist osteoarthritis,21–23 discogenic pain,24 rotator cuff tears,16 and lower extremity neuropathy.25 In those studies the patients generally had degenerative musculoskeletal disorders and there has yet to be data related to accelerating the functional recovery in high-level athletes. Given its widespread clinical benefit in orthopedics, we evaluated injection of AM/UC powder in aiding functional recovery of college football players with musculoskeletal injuries, ultimately enabling athletes to return to play.
Methods
This is a retrospective, single-center chart review of consecutive athletes who sustained traumatic injury of the medial collateral ligament (MCL), hamstring, or oblique and were subsequently treated with injection of AM/UC powder (Clarix® Flo; BioTissue, Inc, Miami, FL). The study was conducted at a single center (Orthopedics and Sports Medicine, Livingston, NJ) in accordance with the tenets of the Declaration of Helsinki and was exempt under 45 CFR §46.101(b)(4) by the Sterling Institutional Review Board.
Patients were included in the study if they were 18 years or older, actively played Division 1 college football, sustained traumatic injury, were subsequently treated with AM/UC injection, and had 6 months of follow-up. Players with a history of recurrent injury or previous injury within the last year were excluded from the study. Data collection was limited to information existing in the electronic medical records between January 2022 and May 2023 and included patient demographics (age, gender), diagnosis, muscle or ligaments involved, grade and extent of injury, position of the player, time to return to play (in days), and complications. For tear severity classification, a modification of Peetrons classification26 was used with the following grading system: grade 0 negative MRI without any visible pathology, grade 1 edema but no architectural distortion, grade 2 architectural disruption indicating partial tear and grade 3 total muscle or tendon rupture. All data were recorded in such a manner that subjects could not be identified directly or through identifiers that were linked to their records. Diagnosis was made on the basis of history, clinical examination, ultrasound examination, and magnetic resonance imaging (MRI).
All patients were initially treated with athletic training directed treatment modalities, physical therapy specific to their injury by a certified physical therapist, activity modification, and nonsteroidal anti-inflammatory medications (Indomethacin 75mg ER) for 7 days. Patients also received adjunctive injection of either 50 or 100 mg AM/UC powder within 5 days of injury. The AM/UC powder (Clarix® Flo; BioTissue, Inc, Miami, FL) is a commercially available, sterile, micronized human amniotic membrane product derived from placenta and umbilical cord that is aseptically processed, devascularized, cell devitalized, lyophilized and terminally sterilized by γ-irradiation. Before use, 50 or 100 mg AM/UC powder was reconstituted in 2cc of 1% lidocaine without epinephrine, yielding a final concentration of 25 mg/mL or 50 mg/mL. Using ultrasound-guidance, the reconstituted AM/UC solution was then injected directly at, above, and below the injury site using a 22- or 25-gauge needle. After each injection, all patients followed the same rehabilitation protocol and sport return progression.
Primary outcome measure was the time to return to play in days, which was calculated as the time from injury to the time to return to full physical activity. Secondary outcome measures included time to limited return to play (days), the proportion of athletes returning to play within four weeks of injury, rate of reinjury within six months, and complications.
Continuous outcomes were reported as mean ± standard deviation (range), and categorical data are reported as frequency and percentage. All statistical analyses were carried out using SPSS Software version 20.0 (IBM; Armonk, NY, USA). Correlations between variables were assessed using Spearman rank correlation coefficient (ρ). A p-value less than 0.05 was considered statistically significant.
Results
A total of 10 consecutive patients met the eligibility criteria and were included for analysis (Table 1). Injuries included tear of the MCL (n=3), hamstring (n=6), and oblique/abdomen (n=1). The majority (60%) of injuries were partial tears (grade 2), with partial to full tears (grade 2±3) noted in 2 patients (20%), and a complete tear (grade 3) noted in 2 patients (20%). The average age at the time of treatment was 19.8 ± 1.0 years (range: 18–21), and the average body mass index (BMI) was 28.5 ± 5.7 kg/m2 (range: 22–37). The patients played football in the following positions: wide receiver (n=3), offensive line (n=3), linebacker (n=1), running back (n=1), defensive line (n=1), and defensive back (n=1). Five athletes (50%) received 50 mg injection of AM/UC, whereas the other half received 100 mg injection.
 |
Table 1 Injury Characteristics and Treatment Outcomes by Case |
The injection was performed uneventfully in all cases. After injection, the patients returned to limited play by 19 ± 5.7 days (range: 10–29) post-injury. Athletes had full return to play at an average of 29.6 ± 15.2 days (range: 16–69) post-injury, with 80% of athletes (n=8) returning to play within 4 weeks. Athletes with partial tears returned to play at an average of 24 ± 4 days post-injury, whereas those with partial to full thickness tears returned to play at 33 ± 5 days. Two players with complete tears returned to play at 43 ± 37 days. Injury grade, BMI and AM/UC dose were not significantly correlated with time to return to play (p=0.44, p=0.22 and p=0.18, respectively). Time to return to play by AM/UC dose and injury grade are shown in Figure 1.
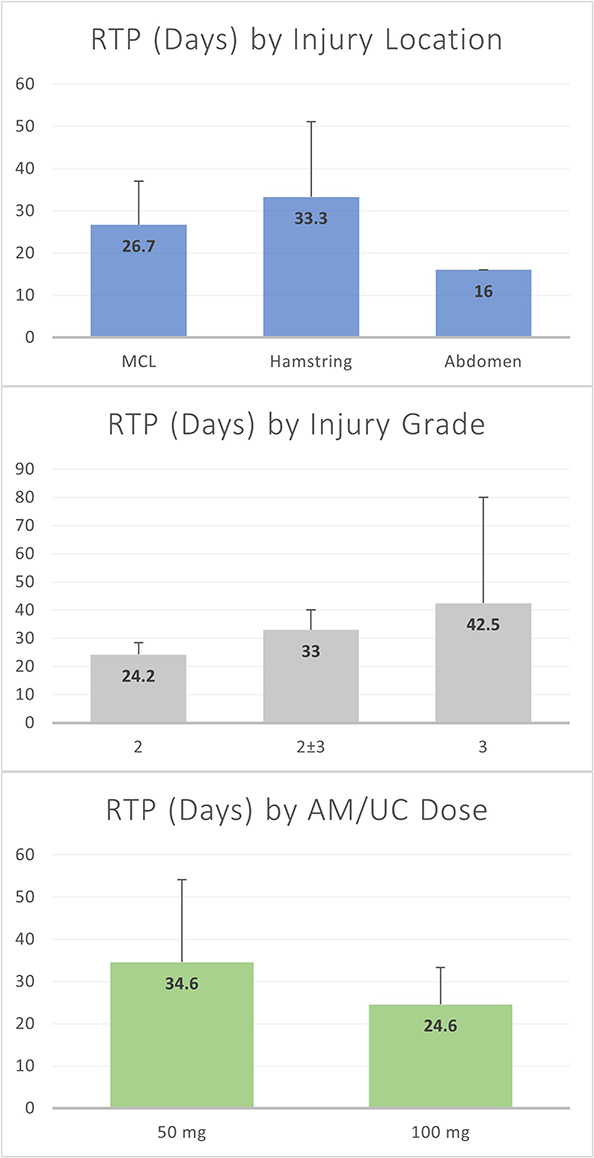 |
Figure 1 Time to Return to Play (RTP) by Injury Location, Injury Grade, and AM/UC Treatment Dose. |
When assessing return to play by injury location (Figure 1), athletes with MCL tears had limited return to play 21 ± 7 days post-injury and full return to play at 26.7 ± 10.3 days post-injury. Similarly, those with hamstring tears returned to limited play by 20 ± 1 days, with full return to play at 33.3 ± 17.8 days post-injury. One athlete with external oblique, internal oblique, and transverse abdominis avulsions from the iliac crest had limited return on day 10, with full return by day 16.
During the average follow-up period of 6 months, no patients experienced reinjury following return to play. Furthermore, no patients reported complications nor did any adverse events occur.
Discussion
It remains a clinical challenge to treat musculotendinous and ligament injuries in athletes, as treatment should aim to hasten return to play while enabling complete healing and functional recovery to reduce the risk of reinjury. Muscle injuries in particular account for one-third of all injuries resulting in loss of playing time, with the hamstring being the most commonly injured muscle in major sports.2,3 While rehabilitation programs serve as the foundation of treating acute hamstring injuries, adjunctive treatment methods, such as corticosteroid and PRP injections, have gained increasing interest to expedite recovery and return to play. Nevertheless, the use of corticosteroid injections remains controversial, and many studies have found no significant benefit of PRP injections in treating acute hamstring strains.27–31 The average return to play following corticosteroid injection is 28 days,4 while the average return to play following PRP injection ranges from 20–42 days.27–31 This is also in alignment with protocols that discuss return to play following PRP injection, which suggest that most patients can be allowed to return to play as early as 4–6 weeks, typically pending completion and progression through a physical therapy and home exercise program.19 Although the return to play was similar in the present study (27.7 days), it’s important to note that athletes sustained higher grade injuries (grade II and III) in this study, which have been associated with significantly longer recovery times.32
Following injury of the hamstring, MCL sprains and tears are the most common severe injury in professional football.33 MCL injuries are generally treated non-operatively with emphasis on early rehabilitation, knee bracing and range of motion exercises, while more severe injuries may require surgical intervention with ligament repair or reconstruction.34 While corticosteroid injections have been used for hamstring injuries, its use for MCL tears is generally contraindicated due to theoretical risk of ligamentous rupture.5,6 Furthermore, there is a lack of evidence supporting the efficacy of PRP injections in treating MCL injuries. Previous studies have shown that treatment with rehabilitation and bracing for grades II and III injuries resulted in a median time playing loss of 29–42 days following injury,35,36 with no observed difference in lay-off times in players treated with PRP injections versus rehabilitation and bracing alone.36 Herein, we found that the mean playing time loss was only 26.7 days for players treated with AM/UC injection for grade 2–3 MCL tears.
Avulsions of the internal/external oblique or the transversus abdominis from the iliac crest are more rare injuries, which have been previously treated with conservative measures including rehabilitation,37 PRP injections,12 and injection of steroid and local anesthetic.38 Athletes have been shown to return to play within 4–6 weeks using these conservative treatments, which is relatively longer compared to other sports injuries.12,37,38 In the present study, an athlete with external oblique, internal oblique, and transverse abdominis avulsions from the iliac crest had full return to play by day 16 following AM/UC injection.
The relatively quick return to play without reinjury following treatment with AM/UC injection is likely attributed to the inherent immunomodulatory properties of birth tissue.39 More specifically, it may be due to the preservation of a key extracellular matrix component, heavy chain-hyaluronan/pentraxin 3 (HC-HA/PTX3), that is found within the AM/UC tissue.40 HC-HA/PTX3 exerts broad anti-inflammatory actions extending from both innate to adaptive immune responses.14 More specifically, HC-HA/PTX3 has been shown to induce apoptosis of pro-inflammatory macrophages and neutrophils, promote polarization of pro-inflammatory M1 macrophages to the M2 phenotype, and suppress CD4+ T cell activation.14 In addition to its anti-inflammatory effects, HC-HA/PTX3 exerts direct anti-scarring effects that minimize fibrosis and support regenerative healing.14
There are several limitations of this retrospective study, with the biggest being the small sample size and lack of a control group. As a result, it is possible the athletes would have healed without injection therapy, but the adjunctive injection of AM/UC appears to have improved the time to return to play and functional outcomes given standard time course returns as reported in the literature. Furthermore, the grade of injury, the location of injury, and AM/UC dose was variable from patient to patient; thus, a more defined cohort that reduces such variability would strengthen the results and conclusions. Although treatment with AM/UC resulted in quick return to play, larger, prospective, comparative studies are required to confirm whether AM/UC can hasten return to play compared to standard treatment alone.
Conclusion
Injection of AM/UC powder is safe, and was shown to enable full return to play at an average of 29.6 ± 15.2 days (range: 16–69) post-injury in football players with muscle or tendon tears. Prospective, randomized, blinded studies are warranted to verify whether injection of AM/UC can hasten return to play compared to standard treatment alone.
Data Sharing Statement
All datasets on which the results and conclusions of the article rely are presented in Table 1.
Funding
No funding to report.
Disclosure
The author is a speaker for BioTissue. There is no other financial or proprietary interest in the subject matter of this article.
References
1. Powell JW, Dompier TP. Analysis of injury rates and treatment patterns for time-loss and non-time-loss injuries among collegiate student-athletes. J Athletic Training. 2004;39(1):56–70.
2. Shankar PR, Fields SK, Collins CL, Dick RW, Comstock RD. Epidemiology of high school and collegiate football injuries in the United States, 2005-2006. Am J Sports Med. 2007;35(8):1295–1303. doi:10.1177/0363546507299745
3. Feeley BT, Kennelly S, Barnes RP, et al. Epidemiology of national football league training camp injuries from 1998 to 2007. Am J Sports Med. 2008;36(8):1597–1603. doi:10.1177/0363546508316021
4. Drakos M, Birmingham P, Delos D, et al. Corticosteroid and anesthetic injections for muscle strains and ligament sprains in the NFL. HSS J. 2014;10(2):136–142. doi:10.1007/s11420-014-9395-7
5. Sellman JR. Plantar fascia rupture associated with corticosteroid injection. Foot Ankle Int. 1994;15(7):376–381. doi:10.1177/107110079401500706
6. Halpern AA, Horowitz BG, Nagel DA. Tendon ruptures associated with corticosteroid therapy. West J Emerg Med. 1977;127(5):378.
7. Matev I. Isolated contracture of the long head of biceps femoris muscle. Int Orthopaedics. 1991;15(2):167–168. doi:10.1007/BF00179719
8. Moraes VY, Lenza M, Tamaoki MJ, Faloppa F, Belloti JC, Platelet-rich therapies for musculoskeletal soft tissue injuries. Cochrane Database Syst Rev. 2013;12:Cd010071. doi:10.1002/14651858.CD010071.pub2
9. Sheth U, Simunovic N, Klein G, et al. Efficacy of autologous platelet-rich plasma use for orthopaedic indications: a meta-analysis. JBJS. 2012;94(4):298–307. doi:10.2106/JBJS.K.00154
10. Seow D, Shimozono Y, Tengku Yusof TNB, Yasui Y, Massey A, Kennedy JG. Platelet-rich plasma injection for the treatment of hamstring injuries: a systematic review and meta-analysis with best-worst case analysis. Am J Sports Med. 2021;49(2):529–537. doi:10.1177/0363546520916729
11. Reurink G, Goudswaard GJ, Moen MH, et al. Rationale, secondary outcome scores and 1-year follow-up of a randomised trial of platelet-rich plasma injections in acute hamstring muscle injury: the Dutch hamstring injection therapy study. Br J Sports Med. 2015;49(18):1206–1212. doi:10.1136/bjsports-2014-094250
12. Gultekin S, Cross T. The Franklin-Naismith Lesion: a severe variant of hip pointer. Orthopaedic J Sports Med. 2019;7(1):2325967118820507. doi:10.1177/2325967118820507
13. Connell DA, Jhamb A, James T. Side strain: a tear of internal oblique musculature. AJR. 2003;181(6):1511–1517. doi:10.2214/ajr.181.6.1811511
14. Tseng SC. HC-HA/PTX3 purified from amniotic membrane as novel regenerative matrix: insight into relationship between inflammation and regeneration. Invest Ophthalmol Visual Sci. 2016;57(5):ORSFh1–8. doi:10.1167/iovs.15-17637
15. Tseng SC, Espana EM, Kawakita T, et al. How does amniotic membrane work? Ocular Surf. 2004;2(3):177–187. doi:10.1016/S1542-0124(12)70059-9
16. Ackley JF, Kolosky M, Gurin D, Hampton R, Masin R, Krahe D. Cryopreserved amniotic membrane and umbilical cord particulate matrix for partial rotator cuff tears: a case series. Medicine. 2019;98(30):e16569. doi:10.1097/MD.0000000000016569
17. Duru N, Williams GK, Jones D A comparative, controlled, retrospective study of patient reported outcomes after meniscectomy with adjunctive use of platelet-rich plasma or amniotic membrane/Umbilical cord particulate.
18. Connell DA, Schneider-Kolsky ME, Hoving JL, et al. Longitudinal study comparing sonographic and MRI assessments of acute and healing hamstring injuries. AJR. 2004;183(4):975–984. doi:10.2214/ajr.183.4.1830975
19. D’Souza RS, Her YF, Hussain N, et al. Evidence-based clinical practice guidelines on regenerative medicine treatment for chronic pain: a consensus report from a multispecialty working group. J Pain Res. 2024;17:2951–3001. doi:10.2147/JPR.S480559
20. Hanselman AE, Tidwell JE, Santrock RD. Cryopreserved human amniotic membrane injection for plantar fasciitis: a randomized, controlled, double-blind pilot study. Foot Ankle Int. 2015;36(2):151–158. doi:10.1177/1071100714552824
21. Castellanos R. Amniotic membrane and umbilical cord particulate for pain associated with knee osteoarthritis: preliminary results of a single-center, prospective, pilot study. Pain Physician. 2018;21:E289–E305.
22. Kim SR. Successful treatment of scapholunate advanced collapse: a case report. Clin Case Reports. 2019;7(6):1230–1232. doi:10.1002/ccr3.2201
23. Mead OG, Mead LP. Intra-articular injection of amniotic membrane and umbilical cord particulate for the management of moderate to severe knee osteoarthritis. Orthop Res Rev. 2020;12:161–170. doi:10.2147/ORR.S272980
24. Buck D. Amniotic umbilical cord particulate for discogenic pain. J Am Osteopath Assoc. 2019;119(12):814–819. doi:10.7556/jaoa.2019.138
25. Buksh AB. Ultrasound-guided injections of amniotic membrane/umbilical cord particulate for painful neuropathy of the lower extremity. Cogent Med. 2020;7(1):1724067. doi:10.1080/2331205X.2020.1724067
26. Peetrons P. Ultrasound of muscles. Eur Radiol. 2002;12(1):35–43. doi:10.1007/s00330-001-1164-6
27. Reurink G, Goudswaard GJ, Moen MH, et al. Platelet-rich plasma injections in acute muscle injury. New Engl J Med. 2014;370(26):2546–2547. doi:10.1056/NEJMc1402340
28. Hamilton B, Tol JL, Almusa E, et al. Platelet-rich plasma does not enhance return to play in hamstring injuries: a randomised controlled trial. Br J Sports Med. 2015;49(14):943–950. doi:10.1136/bjsports-2015-094603
29. Rettig AC, Meyer S, Bhadra AK. Platelet-rich plasma in addition to rehabilitation for acute hamstring injuries in NFL players: clinical effects and time to return to play. Orthopaedic J Sports Med. 2013;1(1):2325967113494354. doi:10.1177/2325967113494354
30. Bradley JP, Lawyer TJ, Ruef S, Towers JD, Arner JW. Platelet-rich plasma shortens return to play in national football league players with acute hamstring injuries. Orthopaedic J Sports Med. 2020;8(4):2325967120911731. doi:10.1177/2325967120911731
31. Hamid MS A, Mohamed Ali MR, Yusof A, George J, Lee LPC. Platelet-rich plasma injections for the treatment of hamstring injuries: a randomized controlled trial. Am J Sports Med. 2014;42(10):2410–2418. doi:10.1177/0363546514541540
32. Ekstrand J, Healy JC, Waldén M, Lee JC, English B, Hägglund M. Hamstring muscle injuries in professional football: the correlation of MRI findings with return to play. Br J Sports Med. 2012;46(2):112–117. doi:10.1136/bjsports-2011-090155
33. Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553–558. doi:10.1136/bjsm.2009.060582
34. Miyamoto RG, Bosco JA, Sherman OH. Treatment of medial collateral ligament injuries. J Am Acad Orthopaedic Surg. 2009;17(3):152–161. doi:10.5435/00124635-200903000-00004
35. Roach CJ, Haley CA, Cameron KL, Pallis M, Svoboda SJ, Owens BD. The epidemiology of medial collateral ligament sprains in young athletes. Am J Sports Med. 2014;42(5):1103–1109. doi:10.1177/0363546514524524
36. Lundblad M, Hägglund M, Thomeé C, et al. Medial collateral ligament injuries of the knee in male professional football players: a prospective three-season study of 130 cases from the UEFA elite club injury study. Knee Surg Sports Traumatol Arthroscopy. 2019;27(11):3692–3698. doi:10.1007/s00167-019-05491-6
37. Murphy M, Stockden M, Breidahl B. Acute tearing of the oblique abdominal wall insertion onto the iliac crest in an Australian football player: a case report. Int J Sports Physical Ther. 2016;11(7):1125–1134.
38. Stevens KJ, Crain JM, Akizuki KH, Beaulieu CF. Imaging and ultrasound-guided steroid injection of internal oblique muscle strains in baseball pitchers. Am J Sports Med. 2010;38(3):581–585. doi:10.1177/0363546509350105
39. Kubrova E, D’Souza RS, Hunt CL, Wang Q, van Wijnen AJ, Qu W. Injectable biologics: what is the evidence? Am J Phys Med Rehabilitation. 2020;99(10):950–960. doi:10.1097/PHM.0000000000001407
40. Cooke M, Tan EK, Mandrycky C, He H, O’Connell J, Tseng SC. Comparison of cryopreserved amniotic membrane and umbilical cord tissue with dehydrated amniotic membrane/chorion tissue. J Wound Care. 2014;23(10):465–476. doi:10.12968/jowc.2014.23.10.465
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Outcomes of Amniotic Membrane/Umbilical Cord Particulate in Spinal Disorders: A Retrospective Study
Ross A, Gambrill V, Main C
Journal of Pain Research 2022, 15:3971-3979
Published Date: 16 December 2022