")
Back to Journals » Local and Regional Anesthesia » Volume 18
Innovative “Three-in-One” Method for Intervention of Lower Limb Neuropathic Pain: Retrospective Case Series Study
Authors Lai J , Lai Y, Wu Y, Xiang Y, Zhang F
Received 11 December 2024
Accepted for publication 25 March 2025
Published 2 April 2025 Volume 2025:18 Pages 9—15
DOI https://doi.org/10.2147/LRA.S511488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Stefan Wirz
Jinyu Lai,1 Yan Lai,2 Yijun Wu,3 Yong Xiang,1 Fengqin Zhang1
1Department of Pain, Taihe Hospital, Hubei University of Medicine, Hubei, People’s Republic of China; 2Department of Ultrasound, Baihe County People’s Hospital, Shanxi, People’s Republic of China; 3Department of Radiology, Taihe Hospital, Hubei University of Medicine, Hubei, People’s Republic of China
Correspondence: Yong Xiang, Department of Pain, Taihe Hospital, Hubei University of Medicine, Hubei, 442000, People’s Republic of China, Tel +86 719 13972451941, Email [email protected] Yijun Wu, Department of Radiology, Taihe Hospital, Hubei University of Medicine, Hubei, 442000, People’s Republic of China, Tel +86 719 13677198927, Email [email protected]
Purpose: Minimally invasive intervention therapy anterior cutaneous branch of the femoral nerve for refractory neuropathic pain in the inner thigh area typically requires punctures at multiple sites to target the three nerves of the obturator nerve cutaneous branch, anterior cutaneous branch of the femoral nerve, and infrapatellar branch of the saphenous nerve. Clinical practice has demonstrated that the innovative “three-in-one” technique allows for simultaneous targeting of the three cutaneous nerves from a single entry point, effectively treating inner thigh pain. Moreover, this approach can also be used for local anaesthesia in shallow surgical procedures in the inner thigh area. We hope to promote this puncture technique among pain physicians.
Patients and Methods: Clinical data of 8 patients with localized pain in the inner thigh from the Pain Department of Taihe Hospital, Shiyan City, Hubei Medical College, from April 2023 to September 2024 were collected. All the patients experienced pain in the cutaneous branch of the obturator nerve, the anterior branch of medial femoral cutaneous nerve, and the infrapatellar branch of the saphenous nerve. The “three-in-one” approach was used for nerve block and radiofrequency puncture.
Results: After the “three-in-one” approach, the 8 patients showed varying degrees of improvement in their Numeric Rating Scale (NRS) scores. The patients were satisfied with the treatment method and efficacy, and no complications, such as nerve damage, occurred during the operation.
Conclusion: The “three-in-one” approach is a potentially effective method for treating pain in the inner lower limb area, significantly reducing the damage caused by multiple puncture and providing ideas for more minimally invasive treatment of other areas; this approach meets expectations for more minimally invasive treatment.
Plain Language Summary: With the continuous development of society and the increasing demand of patients for more comfortable treatment experience, minimally invasive puncture technology has become a direction pursued by more and more pain specialists. Our proposed “three-in-one” puncture technique is suitable for patients with lower limb medial pain. There is only one puncture point on the skin, and by adjusting the puncture direction, the surgeon can simultaneously block three nerves (the cutaneous branch of the obturator nerve, the anterior branch of medial femoral cutaneous nerve, and the infrapatellar branch of the saphenous nerve). This technology can also be used for pain treatment or auxiliary anesthesia in the inner thigh area. We also hope that our innovation can promote the development of more minimally invasive puncture technologies.
Keywords: neuropathic pain, minimally invasive surgery, puncture technique, nerve block
Introduction
Neuropathic pain (NP) refers to pain caused by primary damage to or dysfunction of the nervous system; NP is a common symptom of many sensory neurological diseases, including diabetes neuropathy, drug-induced neuropathy, and traumatic nerve injury, and it seriously affects the quality of life of patients and presents major challenges to public health worldwide.1,2 NP is the main type of chronic pain, defined by the International Association for Study of Pain (IASP) as “pain caused by disorders or diseases of the somatosensory nervous system”.3 According to epidemiological research, this particular type of pain affects 3% to 17% of the population worldwide, and the incidence rate is increasing annually. NP significantly impacts patients’ quality of life and imposes a substantial economic burden. According to body part that is initially affected, this unique kind of pain can be divided into central and peripheral NP, and it can be induced by diabetes, herpes zoster, trauma, and cancer. It clinically manifests as spontaneous pain (burning, tingling and numbness-like pain), which can be accompanied by induced pain, especially in response to gentle touch or cold, and the pain is usually persistent and recurrent.
Currently, the specific mechanism underlying NP is not clear. NP can be induced by various diseases and is also related to adverse reactions to cancer chemotherapy drugs. The main methods for the clinical treatment of NP include oral medication therapy and minimally invasive intervention therapy. NP drug therapy includes opioid drugs, local anaesthetics, antidepressants, and anticonvulsants. The long-term use of large amounts of medication can lead to numerous side effects, unsatisfactory pain control, and increased difficulty in treatment.4,5 Minimally invasive intervention techniques, such as interfascial plane (IFP) blocks and myofascial release, are currently popular research topics with significant therapeutic effects. Ma. et al introduced a novel ultrasound-guided “three-in-one” approach plus IFP blocks for the treatment of cervicogenic headache, which allows for the modulation of C2 dorsal root ganglion, third occipital nerve, and C3 medial branch with one-point puncture. This method significantly improves treatment effectiveness while minimizing the patient’s discomfort caused by repeated punctures.6 We are considering whether it is also possible to treat lower limb neuralgia by planning the puncture path and blocking multiple nerves simultaneously in one puncture.
Minimally invasive intervention therapy for refractory neuropathic pain in the inner thigh area generally requires intervention in the L3 or L4 dorsal root ganglion, combined with local cutaneous nerve (obturator nerve cutaneous branch, anterior cutaneous branch of the femoral nerve, and infrapatellar branch of the hidden nerve) radiofrequency, IFP hydrodissection and release, and myofascial trigger point (MTrP) inactivation. Local hydrodissection and MTrP inactivation often require punctures at multiple sites, which undoubtedly increases the risk of iatrogenic injury and infection while reducing patient comfort during diagnosis and treatment. Compared with the traditional method of three independent punctures to block these three nerves, the innovative “three-in-one” puncture method adopted by these 8 patients with lower limb neuralgia significantly improved their satisfaction with minimally invasive treatment. We found that the “three-in-one” approach can simultaneously target these three cutaneous nerve branches from a single needle entry point, achieving satisfactory results. This approach can be used to relieve pain in the inner thigh area and can also be used for local anaesthesia during surgical procedures of the inner thigh area. We hope to promote this innovative puncture technique among pain physicians.
Materials and Methods
The ethical review of this retrospective study has been exempted by the Ethics Committee of Taihe Hospital, Shiyan city, affiliated with Hubei Medical University (Ethics batch number 2024KS104). From April 2023 to September 2024, 8 patients were selected, they are not satisfied with the effectiveness of simple dorsal root ganglion intervention therapy.But our innovative “three-in-one” method has achieved good results in relieving local pain on the inner thigh of these patients. All the patients experienced pain in the skin branch of the obturator nerve, the anterior branch of medial femoral cutaneous nerve, and the infrapatellar branch of the saphenous nerve. The causes of the chronic pain included herpes zoster and diabetes peripheral neuropathy. The symptoms, signs, and imaging examination results were consistent, and there was no clear surgical indication. All the patients underwent corresponding dorsal root ganglion radiofrequency before undergoing “three-in-one” approach block and radiofrequency.
This study was approved by the Institutional Review Board (IRB) of the Ethics Committee of Taihe Hospital, Shiyan city, affiliated with Hubei Medical University and the study was conducted in accordance with the Helsinki Declaration. Written informed consent was obtained from all patients included in this study.
Inclusion Criteria
- Typical NB in the inner thigh area;
- No obvious mental or psychological illness;
- Ability to cooperate fully and complete follow-up.
Exclusion Criteria
- Mental illness, psychological disorders, and inability to express one’s feelings clearly;
- Severe cardiopulmonary dysfunction and tumour;
- Local infections;
- Lower limb thrombosis;
- Rejection of minimally invasive intervention therapy.
Procedure
Ultrasound scanning of the lower limbs was performed from the middle section of the adductor tube downwards to the opening of the adductor tube, and the probe was approximately 4 fingers away from the upper edge of the patella. The inferior patellar branch of the hidden nerve is shallow in the groove of the sartorius muscle (SM) and the vastus medialis muscle (VM).7 Moving the probe inwards clearly displayed the SM, and the anterior cutaneous branch of the medial thigh nerve runs on the plane of the SM.8,9 Continuing to move the probe inwards, the cutaneous branch of the obturator nerve was observed to located in Fat-filled flat tunnel (FFFT) between the gracilis muscle(GM) and the SM.10 A colour Doppler ultrasound diagnostic device (Mindray Resona R90), an 8–12 MHz high-frequency linear array probe, and a radio frequency ablation therapy device (Cosman RFG-4, Cosman, USA) were used. Notably, before performing the “three-in-one” approach puncture, the puncture path and needle entry point need to be planned. By adjusting the probe position and needle angle, one needle entry point can be used to simultaneously target these three cutaneous nerves.
Intervention method: The patient was placed in a supine position, with the hip joint rotated externally. Preoperative planning of the puncture path, design of the puncture needle entry point, and routine disinfection and drape were performed (Figure 1). Local anaesthetics (2% lidocaine hydrochloride 2.5 mL+0.9% sodium chloride injection 2.5 mL), 0.9% sodium chloride injection (10 mL each, Xuzhou Ryan Pharmaceutical Co., Ltd)., and 2 mL of lidocaine hydrochloride (10 mL each, produced by Guangzhou Baiyun Mountain Mingxing Pharmaceutical Co., Ltd) Were only used for subcutaneous infiltration anaesthesia. A radiofrequency puncture needle (10 cm, bare end 5 mm) was used to first reach the infrapatellar branch of the saphenous nerve in the intermuscular groove between the SM and the VM. A sensory test was performed to induce a corresponding tingling, swelling, and pain sensation near the knee joint within 0.6 mV. High-voltage long-term pulsed radiofrequency was used at this location. After the radiofrequency procedure was complete, 5 mL solution (mixture of 0.5% lidocaine + 1mg/mL betamethasone + 0.9% normal saline) was slowly instilled through the needle. The infrapatellar branch of the hidden nerve was released, and withdrawal was repeated before administration to confirm that there was no blood. Second, the probe was moved inwards, and the SM was clearly displayed. The anterior branch of medial femoral cutaneous nerve is located on the surface myofascial plane of the SM. The needle was withdrawn subcutaneously, and the puncture needle was adjusted to perform radiofrequency on the surface of the SM for the medial femoral nerve cutaneous branch. After radiofrequency, 8 mL of anti-inflammatory and analgesic medication was injected into the muscle plane to fully release the anterior cutaneous branch of the medial femoral cutaneous nerve. Finally, the probe was moved inwards to identify the cutaneous branch of the obturator nerve in the FFFT channel between the GM and the SM. The needle was retracted subcutaneously, the direction of the puncture needle was adjusted, sensory stimulation was used to locate the cutaneous branch of the obturator nerve, and pulsed radiofrequency was performed with the same method (Figure 2). After the treatment was complete, the puncture site was covered with a dressing, and ice was applied to the puncture site to accelerate the closure of the needle eye. The operation is as follows. First, the superficial inferior patellar branch of the saphenous nerve in the intermuscular groove between the SM and the VM is identified. The inferior patellar branch of the saphenous nerve is placed directly below the probe and punctured at an angle of 80 degrees. The medication is expanded in the intermuscular groove. It is important to pay attention to the descending artery of the knee in the intermuscular groove and withdraw the administration channel to prevent medication from entering the bloodstream. Second, the probe is moved inwards to clearly display the cutaneous branches of the medial femoral nerve on the surface of the SM, the needle is withdrawn to the subcutaneous area, the puncture angle is adjusted to 60 degrees, the surface of the SM is punctured, and the drug solution is injected between the muscle planes. Finally, the probe continues to be moved inwards, the puncture needle is pushed subcutaneously, and a 30-degree angle is achieved to inject the medication into the FFFT tube.
 |
Figure 1 The patient is in a supine position with the probe located approximately 3 fingers away from the upper edge of the patella. The “☆” is the entry point of the puncture needle. |
 |
Figure 2 Schematic diagram of cutaneous nerve location and puncture angle. The surgeon first inserts a needle at an angle of 80°-90° into the VM and the infrapatellar branch of the hidden nerve in the SM groove, and then, the surgeon performs radiofrequency modulation and hydrodissection, as shown in (C). Then, the needle is withdrawn subcutaneously and inserted at a 60° angle to puncture the anterior branch of medial femoral cutaneous nerve on the surface of the SM. Radiofrequency modulation and hydrodissection are performed, as shown in (B). Finally, the needle is withdrawn subcutaneously again and punctured at a 30° angle into the closed foramen nerve cutaneous branch in the FFFT channel between the GM and the SM. Radiofrequency modulation and hydrodissection are performed, as shown in (A). The asterisk indicates the specific location of the corresponding nerve. The red arrow indicates the puncture angle and direction. Abbreviations: SM, sartorius muscle; VM, vastus medialis muscle; GM, gracilis muscle; FFFT, Fat-filled flat tunnel. |
Efficacy was assessed by evaluating changes in the numerical rating scale (NRS) score before and after surgery. The pain level was represented by numbers 0–10 instead of words, with 0 indicating no pain, 1–3 indicating mild pain (pain not affecting sleep), 4–6 indicating moderate pain, 7–9 indicating severe pain (inability to fall asleep or woke up during sleep), and 10 indicating severe pain. The follow-up time was at 2 days, 1 week, and 4 weeks after surgery.
Results
From April 2023 to September 2024, there were a total of 8 patients with pain in the inner thigh area, all of whom were included in this study. The basic information of the patients is shown in Table 1. All the patients underwent radiofrequency treatment through the “three-in-one” approach, and local nerve release was performed using hydrodissection after radiofrequency.
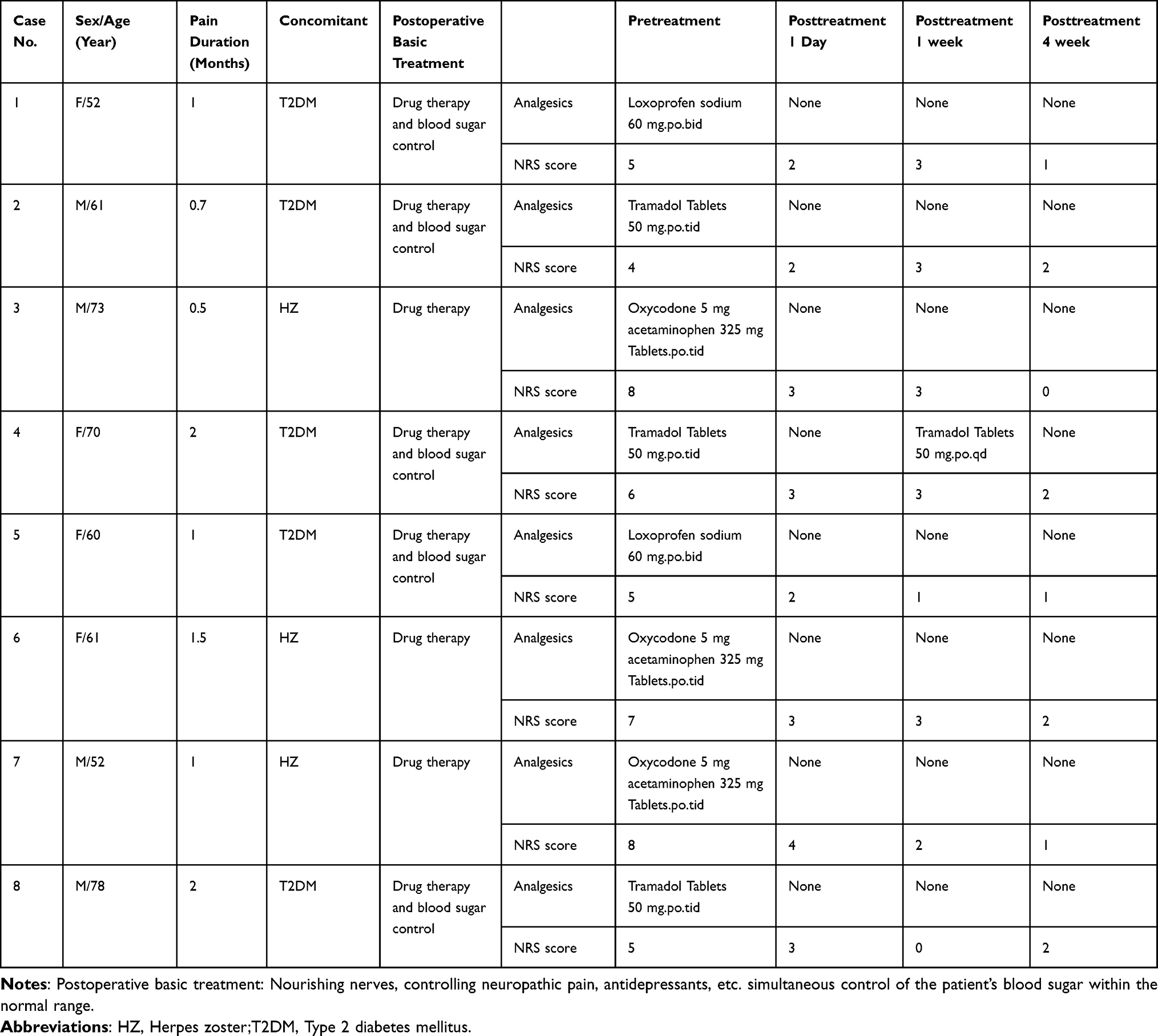 |
Table 1 Patient Basic Information and Clinical Parameters |
All patients were subjected to sensory electrical stimulation to produce corresponding nerve innervation zone soreness, numbness, swelling, and pain reactions within 0.8 mV. All patients experienced significant pain relief on the second postoperative day. The patients’ outpatient follow-up or telephone follow-up at 1 and 4 weeks after surgery revealed varying degrees of improvement in the patient rating scale (NRS) score, which are also shown in Table 1. The median (range) VAS pain score decreased from 5.5 (4–8) at baseline to 2 (2–4) after one day topical treatment. No nerve damage, haematoma, respiratory distress, bradycardia, or other serious complications occurred during the operation.
Discussion
With the rapid development of the social economy and people’s pursuit of higher-quality medical services, minimally invasive intervention therapy with less damage and better efficacy is increasingly favoured by patients. Pain management uses advanced guidance equipment such as ultrasound to intervene in diseased tissues, achieving immediate clinical treatment effects while also allowing treatment via minimally invasive approaches, benefiting an increasing number of patients.
Neuropathic pain associated with herpes zoster and diabetes is very common. When a nerve root has inflammation or demyelinating lesions, compression and adhesion problems often accompany the peripheral nerve. We usually target treatment to the nerve root and then supplement the local fascia and cutaneous branch nerve. This combination of the two techniques can achieve good clinical results. For lower limb medial pain, most pain experts choose to use adductor canal block or femoral nerve block, but now interventions involving the dorsal root ganglion have been added,11,12 but rarely choose more precise blockade of the distal cutaneous nerves such as the obturator nerve, medial femoral cutaneous nerve, and inferior patellar branch of the saphenous nerve. The infrapatellar branch of the saphenous nerve is a purely sensory nerve that innervates the medial side of the knee joint. Gong et al described a method that, under ultrasound guidance, can block it from the superficial site at the junction of the SM and VM. The anterior branch of the medial femoral cutaneous nerve runs along the SM and innervates the medial patellar area and the skin of the inner thigh.13 Gong WY et al innovatively described blocking the anterior branch of the medial femoral cutaneous nerve at the junction of SM and VM, while blocking the medial knee nerve along the posterior margin of the VM. This combination approach can better control acute and chronic pain in the medial patellar area.14 Staples B et al described a method for searching for the cutaneous branches of the obturator nerve when dissecting a corpse, the ultrasound probe locates the flat tunnel between the GM and the SM to block the cutaneous branch of the obturator nerve.10 Usually, if we want to block these three cutaneous nerves more accurately, we requires punctures at multiple sites, and patients must endure the pain caused by multiple punctures. Sometimes, the pain caused by skin punctures can exceed that caused the disease itself, which clearly violates our minimally invasive concept. The “three-in-one” method allows simultaneous intervention in three cutaneous nerves through a single puncture, minimizing damage from repeated punctures.
The “three-in-one” approach described in this study can simultaneously target these three cutaneous nerves with a single puncture without the need to change the puncture site. We adjusted the puncture angle only subcutaneously, reducing iatrogenic damage caused by multiple punctures and minimizing the risk of local infections. In this study, none of the patients experienced any complications, and their pain was relieved to varying degrees, confirming the practicality of the above method.
Conclusions
This preliminary study suggests that the “three-in-one” approach is a potentially effective method for treating pain in the inner lower limb area, significantly reducing the damage caused by multiple puncture and providing ideas for more minimally invasive treatment in other regions, this approach meets expectations for more minimally invasive treatment. In the future, more patients will use this innovative puncture method to test its advantages. This study is a retrospective study with a small sample size, with a relatively single evaluation index, and without a control group. In the future, more in-depth research will be conducted that includes larger sample sizes, additional postoperative observation indicators, and a control group.
Data Sharing Statement
We agree to share all the data related to this article. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study is a retrospective clinical analysis and has been approved by the Ethics Committee of Taihe Hospital, Hubei University of Medicine (number: 2024KS104).
Author Contributions
All the authors made a significant contribution to the reported work, whether in the conception, study design, execution, data acquisition, data analysis and interpretation, or all these areas; participated in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed about the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was funded by the Guiding Research Project of Shiyan Science and Technology Bureau (24Y073).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Finnerup NB, Kuner R, Jensen TS. Neuropathic pain: from mechanisms to treatment. Physiol Rev. 2021;101(1):259–301. doi:10.1152/physrev.00045.2019
2. Bannister K, Sachau J, Baron R, et al. Neuropathic pain: mechanism-based therapeutics. Annu Rev Pharmacol Toxicol. 2020;60(1):257–274. doi:10.1146/annurev-pharmtox-010818-021524
3. Scholz J, Finnerup NB, Attal N, et al. The IASP classification of chronic pain for ICD-11: chronic neuropathic pain. Pain. 2019;160(1):53–59. doi:10.1097/j.pain.0000000000001365
4. Meaadi J, Obara I, Eldabe S, Nazar H . The safety and efficacy of gabapentinoids in the management of neuropathic pain: a systematic review with meta-analysis of randomised controlled trials. Int J Clin Pharm. 2023;45(3):556–565 doi:10.1007/s11096-022-01528-y
5. Weiyi Z, Yong L, Xinye S. Targeted gene therapy for neuropathic pain based on viral vectors. Chin J Pain Med. 2024;30(10):764–768.
6. Ma D, Maimaitimin A, Wang Y. A novel ultrasound-guided “three in one” approach plus interfascial plane blocks for the treatment of cervicogenic headache. Local Reg Anesth. 2024;17:1–8. doi:10.2147/LRA.S446667
7. Abd-Elsayed A, Henjum LJ, Shiferaw BT, et al. Infrapatellar branch of the saphenous nerve: therapeutic approaches to chronic knee pain. Curr Pain Headache Rep. 2024;28(4):279–294. doi:10.1007/s11916-024-01217-7
8. Yang C, Yimin C, Qinglin K. Clinical application of the retrograde flap of the medial femoral cutaneous nerve nutrition vessel vein fascia. Chin J Microsurg. 2007;30(4):296–297.
9. BjøRn S, Nielsen TD, Jensen AE, et al. The anterior branch of the medial femoral cutaneous nerve innervates the anterior knee: a randomized volunteer trial. Minerva Anestesiol. 2023;89(7–8):643–652. doi:10.23736/S0375-9393.22.16910-5
10. Staples B, Ennedy E, Kim T, et al. Cutaneous branch of the obturator nerve extending to the medial ankle and foot: a report of two cadaveric cases. J Foot Ankle Surg. 2019;58(6):1267–1272. doi:10.1053/j.jfas.2019.03.007
11. Hasabo EA, Assar A, Mahmoud MM, et al. Adductor canal block versus femoral nerve block for pain control after total knee arthroplasty: a systematic review and Meta-analysis. Medicine. 2022;101(34):e30110 doi:10.1097/MD.0000000000030110
12. Park S, Park JH, Jang JN, et al. Pulsed radiofrequency of lumbar dorsal root ganglion for lumbar radicular pain: a systematic review and meta-analysis. Pain Pract. 2024;24(5):772–785. doi:10.1111/papr.13351
13. Gong W, Wang A, Fan K. A simple and novel ultrasound-guided approach for infrapatellar branch of the saphenous nerve block. J Clin Anesth. 2019;57:22–23. doi:10.1016/j.jclinane.2019.02.027
14. Gong WY, Li CG, Fan K. A novel ultrasound-guided anterior branch of medial femoral cutaneous nerve block. Minerva Anestesiol. 2021;87(12):1387–1388. doi:10.23736/S0375-9393.21.15868-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.