")
Back to Journals » Clinical Ophthalmology » Volume 19
Intermediate Vision Following Monofocal IOL Implantation
Authors Agarwal S , Thornell E, Frye SN
Received 14 October 2024
Accepted for publication 24 January 2025
Published 19 February 2025 Volume 2025:19 Pages 617—627
DOI https://doi.org/10.2147/OPTH.S499745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Smita Agarwal,1,2 Erin Thornell,1 Sara Nadege Frye3
1Wollongong Eye Specialists, Wollongong, NSW, Australia; 2Graduate School of Medicine, University of Wollongong, Wollongong, NSW, Australia; 3Clinical Development & Medical Affairs, Alcon, Fort Worth, TX, USA
Correspondence: Smita Agarwal, Wollongong Eye Specialists, Level 2, 2 Victoria St, Wollongong, NSW, Australia, Tel +61 2 42630500, Email [email protected]
Purpose: While providing exceptional distance visual outcomes, intermediate vision achieved with monofocal IOLs has not been thoroughly investigated.
Patients and Methods: A total of 63 eyes from 52 patients (average age 73.48± 6.8 years, 56% female) were included for analysis following implantation of the Clareon and Clareon Toric monofocal intraocular IOL with AutonoMe (CNA0T0 or CNA0T2-T6) for the treatment of cataract or refractive error. Visual and refractive outcomes including uncorrected distance, intermediate and near visual acuity, distance-corrected intermediate and near visual acuity, manifest refraction and defocus were first assessed at 4– 6 weeks and then again at 12 weeks following surgery. Patient satisfaction was assessed using a modification of the IOLSAT questionnaire and subjective visual quality was assessed using a modified version of the QUVID questionnaire.
Results: Average postoperative spherical equivalent (SE) was − 0.17± 0.40 D, with 82% and 96% of eyes achieving within ± 0.5 D and ± 1.0 D of the refractive SE target, respectively. Average monocular uncorrected distance visual acuity (UDVA) and uncorrected intermediate visual acuity (UIVA) were 0.03± 0.10 and 0.35± 0.13 LogMAR. Postoperative UIVA improved with more myopic SE (P < 0.0001) and spherical refractive error (P < 0.0001). Bilaterally implanted patients had higher spectacle independence for intermediate tasks compared to unilateral patients (51.1% versus 31.2% respectively).
Conclusion: The Clareon monofocal IOL provided excellent distance vision with a majority of patients achieving spectacle independence for intermediate tasks. While the IOL likely contributed to these visual outcomes, surgeons can also adjust refractive targets to help achieve better intermediate vision postoperatively.
Keywords: Clareon, monofocal IOL, visual performance, intermediate visual acuity, spectacle Independence
Introduction
Monofocal lens designs are the most frequently implanted intraocular lenses (IOLs) globally, accounting for 80% of implantations.1 They provide an affordable lens option that offers a more natural visual experience relatively free of visual disturbances. While their simplistic design generally features a single refractive zone that maintains visual quality and provides excellent aimed vision, they generally provide lower spectacle independence than what is achievable with multifocal IOLs.
While spherical IOL models retain the total corneal spherical aberration (SA) of the eye for the average patient, aspheric IOLs were developed to correct corneal SA, thereby improving quality of vision. However, a small amount of positive SA is known to improve intermediate vision by introducing distance blur and extending the longitudinal range of focus.2 This is often exploited with the introduction of enhanced monofocal IOLs, which are marketed as providing a balance of good distance and improved intermediate vision compared to standard monofocal IOLs. This may, however, compromise visual quality and a balance between SA and depth of focus (DoF) therefore needs to be achieved. There is still contention in the literature regarding what amount of induced SA is optimal for increasing DoF while maintaining good distance vision. Significantly, there are currently no American National Standards Institute (ANSI) or International Organization for Standardization (ISO) standards to dictate what can and cannot be marketed as an “enhanced monofocal” IOL.
The Clareon monofocal IOL (Alcon Research, LLC, Fort Worth, TX) is a standard aspheric hydrophobic IOL composed of an acrylic polymer material with a high refractive index of 1.55 and an increased water content of 1.5% (35°C) relative to the AcrySof material (0.4% at 35°C).3 Specifications for the Clareon and AcrySof IQ monofocal lenses are listed in Table 1. This IOL is also available as a toric model. Unlike enhanced monofocal IOLs, the Clareon monofocal lens was designed to provide exceptional distance vision, but does not claim to correct for intermediate vision. This study aimed to assess postoperative distance and intermediate visual outcomes in eyes that received the Clareon monofocal IOL.
 |
Table 1 Lens Specifications for the Clareon Monofocal and AcrySof IQ IOLs |
Materials and Methods
A total of 63 eyes from 52 patients were recruited following routine phacoemulsification and implantation of Clareon and Clareon Toric monofocal IOLs with AutonoMe (CNA0T0 or CNA0T2-T6) for the treatment of cataract or refractive error; 11 patients underwent bilateral implantation and 41 patients underwent unilateral implantation as part of the study. At recruitment, 21 patients were pseudophakic in the fellow eye, undergoing IOL implantation in the fellow eye prior to recruitment in the study. At the completion of the study, 16 patients were unilaterally pseudophakic and 36 patients were bilaterally pseudophakic. Sample size was determined by performing a power calculation using preliminary UIVA data for Clareon monofocal IOL (clinical data not published), an α-value and a power value of 80%. Exclusion criteria included other ocular pathologies that may have compromised visual outcomes (corneal or retinal disease), history of keratorefractive procedures, or targeting for near vision. Lens powers were calculated using the Barrett True K Formula and a plano±0.25 D refractive target as per usual clinical protocol. Toric IOLs were selected for patients with preoperative corneal cylinder of ≥0.75 D. All surgeries were performed by the same surgeon (SA) and followed a standardized protocol. Briefly, a 2.3 mm corneal incision was made followed by routine phacoemulsification. The Clareon lenses were inserted into the capsular bag using the AutonoMe delivery system. Automated toric alignment was used intraoperatively to ensure accurate alignment of toric IOLs. The marking system used, ie either Verion or Callisto, was dependent on availability at the hospital. Alignment was checked manually using a slit lamp during postoperative assessment. All patients followed the same postoperative drop regimen; 1 drop each of ofloxacin 0.3% ophthalmic solution (Ocuflox, Alcon, Fort Worth, TX) and prednisolone acetate 1% ophthalmic suspension (Prednefrin, AbbVie, North Chicago, IL) every 2 hours on the day of surgery and every 4 hours thereafter. Ofloxacin 0.3% was continued for 2 weeks and prednisolone acetate 1% for 4 weeks. Patients were advised to commence ketorolac tromethamine 0.5% ophthalmic solution (Acular, Allergan, Irvine, CA) 1 week following surgery, applying 1 drop every 4 hours for 1 week.
Postoperative assessment was performed at 4–6 weeks initially, and then again at 12 weeks following surgery. Monocular uncorrected distance (UDVA) and intermediate (UIVA) visual acuity were measured under photopic conditions using a Snellen visual acuity chart placed at 6 meters and an intermediate vision chart placed at 66 cm, respectively. Distance-corrected visual acuity was measured similarly by placing the distance manifest refraction in a trial frame. Monocular best-corrected defocus was performed under photopic conditions using a Snellen chart placed at 6 meters with lenses ranging from +1.00 to −2.50. Subjective binocular visual quality was assessed using the Modified Questionnaire for Visual Disturbances (M-QUVID) and visual function was measured using the Intraocular Lens Satisfaction (IOLSAT) questionnaire. Pupil size and postoperative biometry were measured using an IOLMaster 700 (Zeiss, Hebron, KY) under mesopic conditions, corneal tomography was measured using the Pentacam (Oculus, Arlington, WA) and objective visual quality (modulation transfer function) was measured using the wavefront analysis function of the iTrace aberrometer (Tracey Technologies, Houston, TX).
This study follows the tenets of the Declaration of Helsinki. Approval was obtained from the Human Research Ethics Committee, University of Wollongong, and patients provided informed consent prior to inclusion.
Sample Size Calculation
A power calculation was performed using a calculator accessed from clincalc.com/stats/samplesize.aspx using an alpha value of 0.05 and power value of 80%. For comparison, previously published data for mean UIVA achieved following implantation of the monofocal AcrySof IQ SN60WF IOL (65 eyes; average UIVA = 0.41 UIVA = 0.41±0.12)4 was compared to our preliminary data for the Clareon IOL (35 eyes; average UIVA = 0.25±0.13; unpublished). The calculation suggested a sample size of 19 eyes was required in order to have sufficient statistical power. We have selected a sample size of 75 eyes with an anticipated dropout rate of 20% for a final total of 60 eyes; this is the approximate numbers of eyes that receive the Clareon lens within a 3-month period at our clinic and will allow for some patient drop-out and exclusion.
Statistical Analysis
Correlation coefficients were calculated to identify relationships between postoperative UIVA and spherical equivalent (SE), postoperative refraction, pupil size, and corneal spherical aberration (SA). To determine the relationship between UIVA and these variables, the average postoperative UIVA and UDVA was compared among eyes with postoperative oblique, with-the-rule (WTR), and against-the-rule (ATR) astigmatism, as well as between eyes that received toric and non-toric IOLs considering inter-eye correlation, a mixed-effects model was used and t-test assessed the significance of the fixed effects within the model framework. Rates of spectacle independence were compared between unilaterally and bilaterally pseudophakic patients using a χ2 correlation test.5 The analysis was conducted using the PROC MIXED procedure in SAS (Version 9.4). P values of ≤0.05 were considered statistically significant. A Q-Q plot was used to test for normal distribution.
Results
A total of 63 eyes (average age 73.5±6.8 years [range 50–83], 56% female) were enrolled for the study. No other intra- or postoperative complications were reported. No eyes developed posterior capsular opacification within the follow-up period; one eye was recorded as having visually insignificant posterior capsular opacification postoperatively which did not require YAG capsulotomy. Non-toric IOLs were implanted in 39 (62%) eyes, while the other 24 (38%) eyes received Clareon Toric IOLs (CNA0T2 = 11 [17%], CNA0T3 = 10 [16%], and CNA0T4 = 3 [5%]). No cases of rotation of toric IOLs were observed postoperatively. Average predicted refractive SE (based on IOL power calculation) was −0.19±0.19 D, with 14.3% of eyes (9 eyes) having a slightly hyperopic predicted SE (range +0.04 to +0.39 D) and 85.7% of eyes (54 eyes) having a slightly myopic predicted SE (range −0.64 to −0.02 D). Data followed normal distribution.
Visual and refractive outcomes are summarized in Table 2. Average postoperative SE was −0.17±0.40 D, with 82% and 96% of eyes achieving within ±0.5 D and ±1.0 D of the refractive SE target, respectively (Figure 1A). Average postoperative refractive cylinder was 0.56±0.41 D with 57% and 94% of eyes achieving within ±0.50 D and ±1.00 D of the cylindrical target respectively (Figure 1B). Of those eyes with postoperative refractive cylinder, 11 eyes (24%) had oblique astigmatism, 13 eyes (28%) had WTR astigmatism and 22 eyes (48%) had ATR astigmatism. Most eyes (71%) achieved UDVA of 0.0 LogMAR or better (Figure 2A), with distance visual acuity of 0.2 LogMAR or better being maintained between a range of +0.80 D and −1.00 D of defocus (Figure 2B). UDVA was similar or better than best-corrected visual acuity (BCVA) in 43% of eyes, with 17% of eyes being 2 or more LogMAR lines worse compared to BCVA (Figure 3). Eyes achieving intermediate visual acuity of 0.3 LogMAR (N6) or better were lower with distance correction compared to without correction (41% versus 48%).
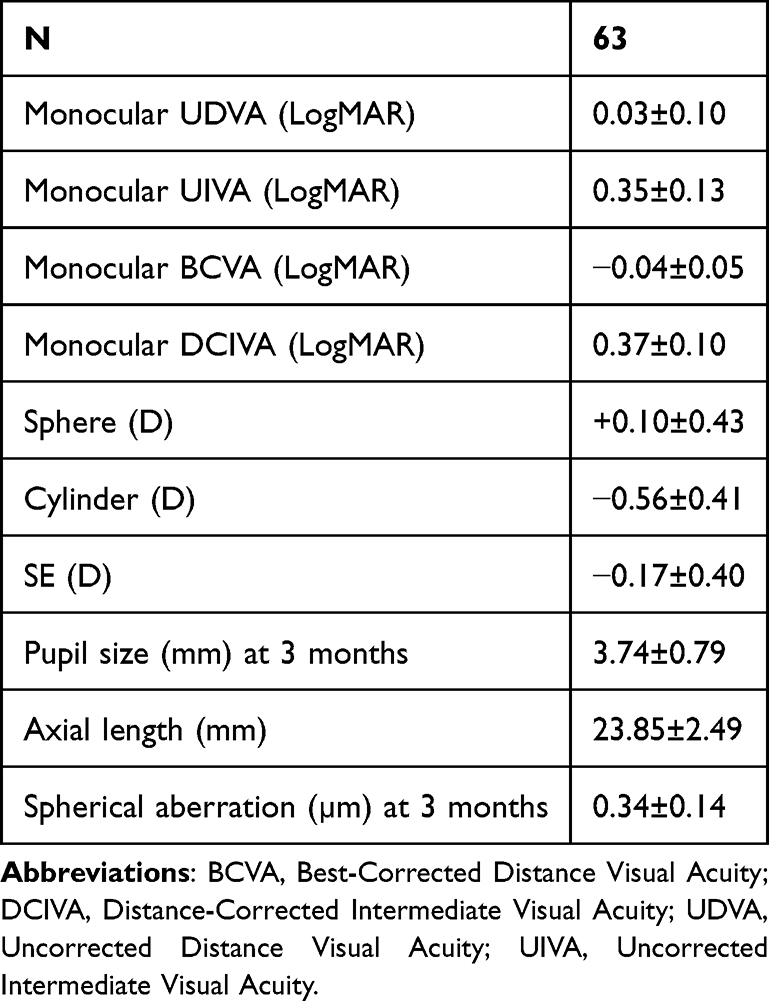 |
Table 2 Postoperative Visual Outcomes 12 weeks Following Implantation of Clareon Monofocal IOL. |
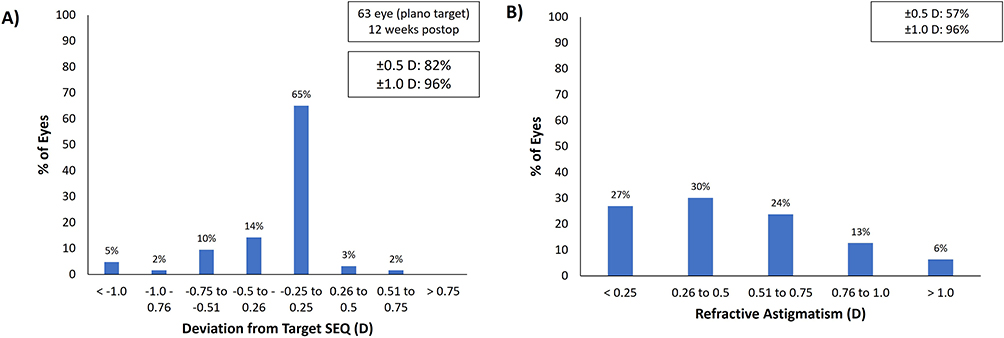 |
Figure 1 Deviation from target SEQ (A) and amount of refractive astigmatism (B) for 63 eyes 12 weeks following implantation of Clareon monofocal IOL. |
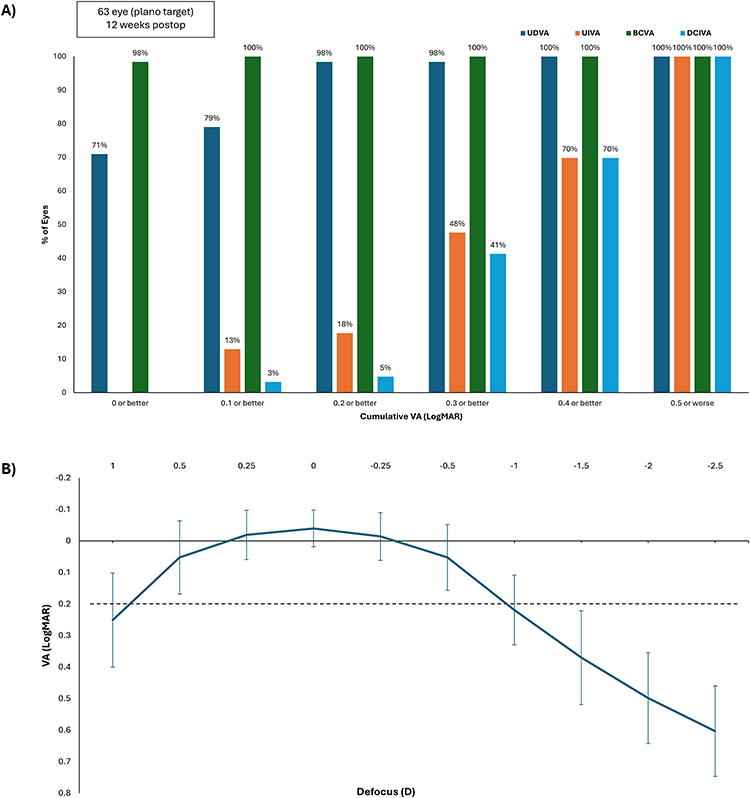 |
Figure 2 Cumulative monocular visual acuity (LogMAR) (A) and best-corrected defocus curve (B) for 63 eyes 12 weeks following implantation of Clareon monofocal IOLs. Abbreviations: BCVA, best-corrected distance visual acuity; DCIVA, distance-corrected intermediate visual acuity; UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; VA, visual acuity. |
 |
Figure 3 Difference between postoperative monocular UDVA and BCVA for 63 eyes 12 weeks following implantation of Clareon monofocal IOL. Abbreviations: BCVA, best-corrected distance visual acuity; UDVA, uncorrected distance visual acuity. |
While there was a significant positive correlation between postoperative UIVA and SE (P < 0.0001) and sphere (P < 0.0001), there was no significant correlation between postoperative UIVA and pupil size (P = 0.21) or axial length (P = 0.51) or SA (P = 0.14). While there was no significant correlation between postoperative UIVA and magnitude of postoperative cylinder (P = 0.74), patients with postoperative oblique cylinder were over-represented in eyes that achieved UIVA of N6 (0.3 logMAR) or better (18% of total eyes versus 73% of eyes that achieved N6 or better).
The average UIVA for oblique cylinders was 0.275 LogMAR (from LSMeans), while for WTR cylinders, it was 0.399 LogMAR. The difference of −0.125 LogMAR between oblique and WTR cylinders is marginally significant with a p-value of 0.0556. The average UIVA for oblique cylinders was 0.275 LogMAR, compared to 0.371 LogMAR for ATR cylinders. The difference of 0.096 LogMAR is not statistically significant with a p-value of 0.0841.
The average UDVA for eyes with non-toric IOLs was 0.0278 LogMAR, while for eyes with toric IOLs, it was 0.03034 LogMAR. The difference in UDVA between these groups is −0.00259 LogMAR with a p-value of 0.9283. This result indicates that there is no significant difference in UDVA between eyes with toric IOLs and those with non-toric IOLs.
Modulation Transfer Function (MTF) as a function of spatial frequency is shown in Figure 2; 50% contrast is maintained at a spatial frequency of approximately 9 cpd (Figure 4). The IOLSAT questionnaire was completed for 63 eyes, and the M-QUVID questionnaire was completed for 62 eyes. Outcomes are summarized in Tables 3 and 4. Spectacle independence was generally higher for distance tasks compared to intermediate tasks; a slight majority of bilaterally pseudophakic patients reported not requiring spectacles for intermediate tasks at 3 months (55.3%; Table 3). While rates of distance spectacle independence were significantly higher in bilaterally pseudophakic patients compared to unilaterally pseudophakic patients (χ2 = 12.48; P = 0.001), rates for intermediate spectacle independence were not statistically different (χ2 = 2.77, P = 0.1) despite bilaterally pseudophakic patients being 1.8-fold more likely to report not needing glasses for intermediate tasks.
 |
Table 3 Patient Response to IOLSAT Questionnaire. Data Is Compared for Patients Who are Unilaterally or Bilaterally Pseudophakic at 1- and 3-months Following Implantation of Clareon Monofocal IOL. Data Is Reported as a Percentage of Patients Who Gave a Response With Raw Numbers in Brackets. |
 |
Table 4 Patient Response to QUVID Questionnaire. Data Is Compared for Patients Who are Unilaterally or Bilaterally Pseudophakic at 1- and 3-months Following Implantation of Clareon Monofocal IOL. Data Is Reported as a Percentage of Patients Who Gave a Response With Raw Numbers in Brackets. |
 |
Figure 4 MTF for 63 eyes 12 weeks following implantation of Clareon monofocal IOL. Abbreviations: Cpd, cycles per degree; MTF, modulation transfer function. |
Discussion
Despite being marketed as a standard monofocal IOL, early findings suggest that Clareon and Clareon Toric monofocal IOLs may provide patients with a greater range of vision than what is expected of standard monofocals. This however has not been extensively investigated or peer-reviewed in the clinical setting. This paper will discuss the role the IOL design plays in intermediate visual acuity with the monofocal Clareon IOL, and how surgeons can utilise or take advantage of pre-existing oblique astigmatism and SA in order to maximise intermediate visual outcomes without resorting to more expensive IOLS such as enhanced monofocal models.
So-called enhanced monofocal lenses were introduced in an attempt to extend far distance focus.6 However, whether these lenses provide superior intermediate vision outcomes compared to monofocals is under debate.6 As previously mentioned, there are currently no ANSI or ISO standards for enhanced monofocal IOLs.7
The first available enhanced monofocal IOL, Tecnis Eyhance (Johnson & Johnson, New Brunswick, NJ), claims to extend DoF by having a continuous power gradient across the IOL while still correcting the SA of the eye. Both in vitro and in vivo studies have reported up to a 1-line improvement in UIVA for Tecnis Eyhance (ICB00) compared to similar standard monofocal lenses, although results vary substantially.2,8 Comparative studies have predominantly compared outcomes of Tecnis ICB00 with those of Tecnis ZCB00 (Johnson & Johnson, New Brunswick, NJ), the standard monofocal IOL that serves as a platform for Eyhance. These studies report that ICB00 improves UIVA numerically compared to ZCB00 while achieving similar UDVA and visual quality.8–10 In a study that compared Tecnis Eyhance ICB00 with the EDoF lens Tecnis Symfony ZXR00, UIVA and spectacle independence outcomes were similar (Eyhance ICB00 group, 36% of patients achieved 0 logMAR or less and 88% ≤0.1 logMAR vs Symfony ZXR00 where 72% of patients attained 0 logMAR or less and 100% ≤0.1 logMAR or more), with the Symfony lens resulting in higher incidence of glare and halos.11
Results from studies on AcrySof IQ and Clareon, two optically equivalent designs, show that these IOLs also have the capacity to provide usable intermediate vision. McCabe et al12 (2022) and Bala et al13 (2022) found that 82% and 83% of patients, respectively, achieved 0.2 logMAR or better UIVA with AcrySof IQ, with mean binocular UIVA of 0.139 ± 0.122 and 0.112 ± 0.163 LogMAR, respectively.
However, in a direct comparison between Tecnis Eyhance ICB00 and AcrySof IQ SN60WF, Cinar et al4 (2021) reported better monocular UIVA at 60 cm achieved by the Tecnis Eyhance compared to AcrySof IQ (0.31 ± 0.16 vs 0.41 ± 0.12, P = 0.001). The current study did not record binocular UIVA to avoid the results being skewed by patients who were unilaterally implanted (ie likely to have cataract in the companion eye). While the intermediate outcomes reported here align well with that reported by Cinar et al4 for the AcrySof IQ and Tecnis Eyhance IOLs, McCabe et al12 and Bala et al13 reported better outcomes when UIVA was measured binocularly.
Literature regarding postoperative intermediate outcomes of the Clareon monofocal IOL is more sparse. Blehm and Hall14 (2023) assessed patients implanted with the Clareon monofocal IOL specifically and reported better levels of intermediate visual acuity than what was reported in Cinar et al4 (2021) for the AcrySof IQ monofocal IOL. Mean postoperative binocular uncorrected visual acuity was 0.16 ± 0.13 logMAR and 0.24 ± 0.14 logMAR at 80 cm and 66 cm respectively, with 83% and 72% of eyes achieving 0.3 LogMAR or better for UIVA measured at 80 cm and 66 cm respectively. Furthermore, in a comparison between Clareon monofocal and Eyhance IOLs, Micheletti et al (2023) reported a mean DCIVA of 0.24 ± 0.11 logMAR at 66 cm. He concluded that Clareon monofocal was non-inferior to Eyhance in intermediate vision outcomes.15 Postoperative UIVA reported for the current paper (0.35 LogMAR) is slightly inferior (approximately 1-line LogMAR) to what was reported by Blehm and Hall14 and Micheletti et al11 and may be due to the reporting of binocular data compared to monocular data.
Receiving FDA approval in 2021, the RayOne EMV (Rayner Intraocular Lenses Limited, Worthing, UK) is another enhanced monofocal IOL that uses a continuous power profile and induced positive SA to extend depth of focus into the intermediate range. Law16,17 (2023) has presented data from bilateral implantation of the RayOne EMV IOL with either monovision (−1.25 target in non-dominant eye) or mini-monovision (−0.75 target in non-dominant eye), achieving binocular UIVA of 0.15 LogMAR. When measured monocularly and with an emmetropic target, however, UIVA (0.4 LogMAR) was inferior to what is reported here (0.35 LogMAR). Furthermore, distance visual acuity of 0.2 LogMAR or better was only maintained within a defocus range of +0.8 to −1.0 D. Notably, the UDVA in distance-corrected eyes reported here for the Clareon monofocal IOL (0.028 LogMAR versus 0.12 LogMAR) was better than what was reported by Law.16,17 While recent reports of good intermediate vision outcomes of the Clareon IOL have been published, there has been little investigation into the mechanisms that may underlie these findings. Multiple variables, both within the visual system and the optical system, may be responsible for the extended range of vision seen with the Clareon monofocal lens. Bala et al13 reported functional UIVA (average binocular UIVA of 0.112±0.163 LogMAR) in patients receiving the AcrySof IQ SN60WF lens; however, the addition of distance correction appeared to cause a slight reduction in intermediate vision function (average binocular DCIVA of 0.196±0.16 LogMAR), suggesting that small amounts of residual myopic refractive error may be necessary to achieve increased range of vision. Data presented here support that premise, with a positive correlation reported between monocular UIVA and both SE and sphere, and a reduction in intermediate vision when distance correction is applied. This would vary depending on the type and magnitude of residual refractive error post-surgically. Even with distance correction in place, however, intermediate results are still better than might be expected. Furthermore, in some studies, intermediate visual acuity is maintained with distance correction in place. Blehm and Hall14 (2023) found the mean binocular distance-corrected intermediate visual acuity for the Clareon monofocal CNA0T0 at 80 cm and 60 cm to be 0.16±0.13 logMAR and 0.23 ± 0.14 logMAR, in comparison to the uncorrected figures of 0.16 ± 0.13 logMAR and 0.24 ± 0.14 logMAR, respectively. This further elucidates that the IOL’s design contributes to the intermediate vision improvement. As previously mentioned, aspheric IOLs are designed to correct varying degrees of corneal SA, thereby improving quality of vision.18,19 However, a small amount of positive SA is known to improve intermediate vision by expanding the longitudinal range of focus.2 This optical design is shared by monofocals and so-called enhanced monofocal IOLs alike.
With respect to astigmatism, it has been reported that small amounts of WTR astigmatism can help to improve near vision.20 To date, little evidence has been published to suggest that oblique astigmatism may play a role in extending depth of focus. However, the data presented here suggest that oblique astigmatism may in fact improve intermediate visual function more than WTR astigmatism. Despite having a higher amount of postoperative astigmatism, eyes that received toric IOLs did not have better postoperative UDVA or UIVA compared to eyes that received non-toric IOLs. Furthermore, there was no difference in the amount of postoperative astigmatism between eyes with oblique and WTR (0.73 D versus 0.71 D; P = 0.89), or oblique and ATR (0.73 D versus 0.74; P = 0.93) astigmatism. This suggests that it is the type of astigmatism, not the amount, that is relevant to postoperative visual outcomes. While inducing oblique astigmatism may not be practical when planning surgery, surgeons may be mindful of pre-existing oblique astigmatism and may consider leaving a small amount uncorrected. Average postoperative astigmatism in eyes with residual oblique cylinder was 0.73±0.34 D. Without further study, it is difficult to say how much residual astigmatism offers the most benefit. However, the preliminary findings here suggest that aiming for residual oblique astigmatism of 0.5 to 0.75 D may provide better intermediate outcomes without substantially degrading overall vision.
De Luis Eguileor (2020)18 reported that postoperative UIVA correlated with corneal root mean square higher-order aberrations (RMS HOAs) and 4th order SA. The Clareon lens has an asphericity value of −0.2 µm, while the virgin cornea contributes on average +0.27 µm,21 meaning the average eye may expect to have +0.07 µm of residual SA following implantation. While increased SA can compromise visual quality, Nochez et al22 (2011) has reported that ocular SA of +0.07 to +0.1 µm may be the best balance between visual quality and depth of focus. When the current dataset was separated into two groups, those that achieved UIVA of N6 or better (equivalent to 0.3 LogMAR; Group 1) and those that achieved UIVA of N8 or worse (equivalent to 0.4 LogMAR; Group 2), Group 1 was found to have an average corneal SA of +0.31 µm versus +0.37 for Group 2. Although there was no statistically significant difference in average corneal SA between the groups (P = 0.13), once correction of SA by the IOL is taken into account, Group 1 would have an average postoperative ocular SA closer to the optimal range suggested by Nochez.22
In an in vitro study, Vega et al (2015)23 reported modulation transfer function (MTF) curves for the AcrySof SN60WF IOL, claiming that 50% contrast is maintained at a spatial frequency of approximately 13.5 cpd with a 4 mm pupil. While this result is better than what is reported here for the Clareon IOL (50% maintained at 9 cpd; Figure 2), it should be noted that the current measurements were performed in vivo, and therefore components of the ocular system may have had an effect.
At three months following surgery, patients in the current study were 1.7-fold and 1.8-fold more likely to be spectacle independent for distance and intermediate tasks respectively if they were bilaterally pseudophakic compared to unilaterally; however, only rates of distance spectacle independence were statistically different between the groups. While literature regarding spectacle independence is scarce for monofocal IOLs, Joshi (2023)24 reported a rate of spectacle independence of 85% for intermediate tasks in patients that had received the Eyhance ICB00 IOL. While this rate is higher than reported for this study (55.3% in bilaterally pseudophakic patients), little information is provided regarding postoperative refractive outcomes. The authors state that they used an emmetropic target and there was no postoperative refractive error; however, precise numbers were not provided. It should be noted that intermediate vision recorded for this study was at 66 cm. There is some debate regarding what should be considered a working intermediate distance. While Joshi24 recorded UIVA at 60 cm, it has been suggested that 80 cm provides a more realistic point closer aligned to daily lifestyle habits. Nevertheless, the American Optometric Association, the US Occupational Safety and Health Administration, and the Canadian Center for Occupational Health and Safety, have suggested specific distances for intermediate vision to enhance computer viewing. On average, these recommendations converge around 63 cm, emphasizing the significance of intermediate vision. Notably, the American Academy of Ophthalmology Task Force recommends assessing intermediate vision at a distance of 66 cm when considering extended depth-of-focus IOLs.25,26
Limitations of this study include the lack of a comparison group (direct comparison with eyes that have received an enhanced monofocal lens may provide more insight into different outcomes achieved with each) and inclusion of bilaterally implanted eyes which can induce bias. Despite this, these findings provide a valuable insight into how standard monofocal IOLs can be used to provide some patients with some functional intermediate vision without resorting to potentially more expensive enhanced monofocal IOL models.
Conclusion
Intermediate visual outcomes of monofocal lenses have only recently become a topic of interest in the literature, with little investigation being performed into the mechanisms underlying intermediate outcomes. The results published here suggest that both postoperative refractive targets and the design of the lens may be underlying mechanisms providing postoperative intermediate vision. Furthermore, mild residual oblique astigmatism may further enhance lens performance at intermediate range but needs further investigation to assess the useful range of oblique astigmatism. The Clareon lens can provide an affordable option for patients who desire a greater degree of spectacle independence than what is generally expected from standard monofocal IOLs, but who are willing to continue using spectacles for near tasks. To expand on the mechanism contributing to the extended range of vision reported for the Clareon lens, further studies will need to be performed.
Acknowledgments
This study was funded by Alcon. We also thank the Wollongong Eye Specialists staff for their help in data collection.
Disclosure
Dr Smita Agarwal reports personal fees for advisory board from Alcon, outside the submitted work. Sara N. Frye was an employee of Alcon at the time of study. Erin Thornell reports no conflicts of interest in this work.
References
1. European Society for Cataract and Refractive Surgery. (2022). Clinical trends survey 2021. Available at: org/eurotimes/supplement-clinical-trends-survey-2021-results.
2. Alarcon A, Canovas C, Koopman B, Weeber H, Auffarth GU, Piers PA. Enhancing the intermediate vision of monofocal intraocular lenses using a higher order aspheric optic. J Refract Surg. 2020;36(8):520–527. doi:10.3928/1081597X-20200612-01
3. Clareon™ Aspheric hydrophobic acrylic IOL with the autonome™ Automated pre-loaded delivery system. instructions for use. Alcon Laboratories Fort Worth Tx. 2022.
4. Cinar E, Bolu H, Erbakan G, et al. Vision outcomes with a new monofocal IOL. Int Ophthalmol. 2021;41(2):491–498. doi:10.1007/s10792-020-01599-8
5. Chi-square test calculator. Available at: https://www.socscistatistics.com/tests/chisquare2/default2.aspx. Accessed November 17, 2023.
6. Fernandez J, Rocha-de-Lossada C, Zamorano-Martin F, Rodriguez-Calvo-de-Mora M, Rodriguez-Vallejo M. Positioning of enhanced monofocal intraocular lenses between conventional monofocal and extended depth of focus lenses: a scoping review. BMC Ophthalmol. 2023;23(1):101. doi:10.1186/s12886-023-02844-1
7. American National Standard for Ophthalmics. ANSI Z80.35-2018: extended depth of focus intraocular lenses. 2018. Available at: https://webstore.ansi. org/standards/vc%20(asc%20z80)/ansiz80352018.
8. Auffarth GU, Gerl M, Tsai L, et al. Clinical evaluation of a new monofocal IOL with enhanced intermediate function in patients with cataract. J Cataract Refract Surg. 2021;47(2):184–191. doi:10.1097/j.jcrs.0000000000000399
9. Mencucci R, Cennamo M, Venturi D, Vignapiano R, Favuzza E. Visual outcome, optical quality, and patient satisfaction with a new monofocal IOL, enhanced for intermediate vision: preliminary results. J Cataract Refract Surg. 2020;46(3):378–387. doi:10.1097/j.jcrs.0000000000000061
10. Unsal U, Sabur H. Comparison of new monofocal innovative and standard monofocal intraocular lens after phacoemulsification. Int Ophthalmol. 2021;41(1):273–282. doi:10.1007/s10792-020-01579-y
11. Corbelli E, Iuliano L, Bandello F, Fasce F. Comparative analysis of visual outcome with 3 intraocular lenses: monofocal, enhanced monofocal, and extended depth of focus. J Cataract Refract Surg. 2022;48(1):67–74. doi:10.1097/j.jcrs.0000000000000706
12. McCabe C, Berdahl J, Reiser H, et al. Clinical outcomes in a U.S. registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg. 2022;48(11):1297–1304. doi:10.1097/j.jcrs.0000000000000978
13. Bala C, Poyales F, Guarro M, et al. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J Cataract Refract Surg. 2022;48(2):136–143. doi:10.1097/j.jcrs.0000000000000712
14. Blehm C, Hall B. Evaluation of visual outcomes and 3-month refractive stability of a new hydrophobic acrylic intraocular lens. Clin Ophthalmol. 2023;17:1859–1864. doi:10.2147/OPTH.S415400
15. Micheletti JM, Duncan N, Hall B. Head-to-head comparison of intermediate vision of two monofocal intraocular lenses. Clinical Ophthalmology. 2023;17:3983–3990. doi:10.2147/OPTH.S444696
16. Law ESCRS https://www.escrs.org/eurotimes-articles/micromonovision-with-non-diffractive-enhanced-monofocal-iol/. Presented at ESCRS 2023.
17. RayOne EMV toric first-in-eye multicentre real world clinical results.
18. de Luis Eguileor B, Martinez-Indart L, Martinez Alday N, Sacristan Eguen C, Cuadros Sanchez C. Differences in intermediate vision: monofocal intraocular lenses vs. monofocal extended depth of focus intraocular lenses. Arch Soc Esp Oftalmol. 2020;95(11):523–527. doi:10.1016/j.oftal.2020.06.009
19. Tabernero J, Piers P, Benito A, Redondo M, Artal P. Predicting the optical performance of eyes implanted with IOLs to correct spherical aberration. Invest Ophthalmol Vis Sci. 2006;47(10):4651–4658. doi:10.1167/iovs.06-0444
20. Leube A, Ohlendorf A, Wahl S. The influence of induced astigmatism on the depth of focus. Optom Vis Sci. 2016;93(10):1228–1234. doi:10.1097/OPX.0000000000000961
21. Guirao A, Redondo M, Artal P. Optical aberrations of the human cornea as a function of age. J Opt Soc Am a Opt Image Sci Vis. 2000;17(10):1697–1702. doi:10.1364/josaa.17.001697
22. Nochez Y, Majzoub S, Pisella PJ. Effect of residual ocular spherical aberration on objective and subjective quality of vision in pseudophakic eyes. J Cataract Refract Surg. 2011;37(6):1076–1081. doi:10.1016/j.jcrs.2010.12.056
23. Vega F, Millan MS, Vila-Terricabras N, Alba-Bueno F. Visible versus near-infrared optical performance of diffractive multifocal intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56(12):7345–7351. doi:10.1167/iovs.15-17664
24. Joshi RS. Visual satisfaction and spectacle Independence with monofocal intraocular lens with enhanced intermediate vision and trifocal intraocular lenses in the prepresbyopic age group patients with cataracts. Oman J Ophthalmol. 2023;16(3):482–488. doi:10.4103/ojo.ojo_167_22
25. Lapid-Gortzak R, Bala C, Schwiegerling J, Suryakumar R. New methodology for measuring intraocular lens performance using acuity reserve. J Cataract Refract Surg. 2021;47(8):1006–1010. doi:10.1097/j.jcrs.0000000000000561
26. MacRae S, Holladay JT, Glasser A, et al. Special report: American Academy of Ophthalmology Task Force Consensus statement for extended depth of focus intraocular lenses. Ophthalmology. 2017;124(1):139–141. doi:10.1016/j.ophtha.2016.09.039
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Head-to-Head Comparison of Intermediate Vision of Two Monofocal Intraocular Lenses
Micheletti JM, Duncan NB, Hall B
Clinical Ophthalmology 2023, 17:3983-3990
Published Date: 21 December 2023