")
Back to Journals » Clinical Ophthalmology » Volume 19
Intravitreal Bevacizumab Alone Vs Combined With Topical Timolol-Dorzolamide or Dorzolamide for Diabetic Macular Edema: A Systematic Review and Meta-Analysis
Authors Hubayni RA , Qedair J , Bukhari ZM, Alsudais AS, Badghaish OS , Bawazir RO , AlQahtani AS, Almarzouki H
Received 4 December 2024
Accepted for publication 10 February 2025
Published 22 March 2025 Volume 2025:19 Pages 1007—1019
DOI https://doi.org/10.2147/OPTH.S509136
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Rahaf A Hubayni,1,2 Jumanah Qedair,1,2 Ziad M Bukhari,3 Ali S Alsudais,1,2 Orjwan Salah Badghaish,1,2 Razan Osama Bawazir,1,2 Abdullah S AlQahtani,1– 3 Hashem Almarzouki1– 3
1College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia; 3Ophthalmology Department, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Jeddah, Saudi Arabia
Correspondence: Rahaf A Hubayni, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia, Email [email protected]
Purpose: Diabetic macular edema (DME) is a major cause of vision loss in diabetes. This systematic review and meta-analysis aimed to evaluate the efficacy and safety of intravitreal bevacizumab (IVB) combined with topical timolol-dorzolamide versus dorzolamide alone in DME patients.
Patients and Methods: A literature search was conducted across multiple databases until March 2024. Randomized controlled trials (RCTs) comparing IVB (1.25 mg, monthly) with topical dorzolamide-timolol (twice daily) or dorzolamide alone (twice daily) were included. Primary outcomes assessed were best-corrected visual acuity (BCVA), central macular thickness (CMT), and intraocular pressure (IOP) at various intervals.
Results: Four RCTs involving 98 patients (150 eyes) were analyzed, with a mean age of 57.9 years and a female predominance (55.1%). The subgroup meta-analysis indicated a weighted mean difference (WMD) in BCVA of − 0.125 [95% CI: − 0.21 to − 0.041]. The IVB+D group showed no significant difference in WMD compared to the IVB and IVB+TD groups. IOP measurements revealed a WMD of − 1.244 mmHg [95% CI: − 2.548 mmHg to 0.06 mmHg], with a significant increase in the IVB group compared to the IVB+D and IVB+TD groups. CMT analysis showed a WMD of − 78.875 μm [95% CI: − 118.606 μm to − 39.145 μm], with no significant differences among groups.
Conclusion: Concurrent IVB with topical timolol-dorzolamide or dorzolamide alone demonstrated similar efficacy in improving BCVA and CMT in DME patients. However, the IVB+TD combination resulted in a more significant reduction in IOP compared to IVB alone.
Keywords: diabetic macular edema, intravitreal bevacizumab, anti-vascular endothelial growth factor, retinal disorders, timolol-dorzolamide
Introduction
Diabetic macular edema (DME) is a serious complication of diabetes mellitus characterized by excessive accumulation of fluid within retinal layers of the macula. DME is the leading cause of vision loss among individuals with diabetes.1–3 Concurrent with the alarming global escalation in the prevalence of diabetes mellitus, the therapeutic burden associated with DME has increased exponentially.2 Epidemiological investigations have demonstrated the prevalence of DME in diabetic patients to vary between 1.4% and 14.3%.4–6
The pathophysiology of diabetic macular edema (DME) is intricate, involving a multifaceted interplay of interconnected mechanisms. Chronic hyperglycemia, a hallmark of diabetes, can cause increased vascular permeability and disruption of the blood-retinal barrier, resulting in the accumulation of fluid in the retinal tissue.7,8 Moreover, empirical evidence has demonstrated that inflammatory processes, characterized by the upregulation of chemokines and cytokines, contribute to the development and progression of DME.8,9 Notable inflammatory mediators involved in DME include vascular endothelial growth factor (VEGF), interleukins (ILs), matrix metalloproteinases (MMPs), and tumor necrosis factor (TNF).8,9 Furthermore, oxidative stress and impaired autoregulation of retinal blood flow have also been implicated in the pathogenesis of DME.9
Clinically, DME is characterized by macular thickening, the presence of hard exudates, and a decline in visual acuity. The severity of symptoms can vary, ranging from subtle changes in vision to significant vision impairment that significantly impacts daily functioning.8,10 Individuals with DME may encounter symptoms such as blurred vision, metamorphopsia, and challenges with central vision-dependent tasks like reading and driving.8,10
The mainstay of treatment for DME is intravitreal anti-vascular endothelial growth factor (anti-VEGF) therapy. The introduction of anti-VEGF agents has revolutionized the treatment of DME by largely replacing retinal laser treatment as the primary intervention.2,11 However, limitations such as incomplete treatment response, high costs, and safety concerns related to frequent injections have resulted in suboptimal outcomes.12,13
The effectiveness of intravitreal anti-VEGF therapy depends on its distribution, either directly to the vitreous body or indirectly affecting the retinal layers through the aqueous humor.13 The drug is typically cleared through the anterior chamber outflow, which may lead to limited efficacy as the drug is washed out rapidly.14,15 To address this, prolonging the half-life of anti-VEGF agents by administering antiglaucoma drugs (such as carbonic anhydrase inhibitors and beta-blockers) concomitantly has been explored.16,17 This approach aims to enhance efficacy and improve clinical outcomes by reducing the turnover of aqueous humor.16,17
A growing body of evidence has compared the efficacy and safety of the combined approach of concurrent administration of intravitreal bevacizumab with topical timolol-dorzolamide or dorzolamide alone in patients with DME.18–23 However, to our knowledge, other anti-VEGF agents have not been extensively investigated in clinical trials for this specific combination approach. Therefore, a systematic review and meta-analysis is warranted to synthesize the available evidence and draw a comprehensive conclusion. Herein, we aim to systematically analyze the efficacy and safety of concurrent administration of intravitreal bevacizumab with topical timolol-dorzolamide or dorzolamide alone in patients with DME.
Materials and Methods
Literature Search Strategy
A systematic review and meta-analysis, registered with PROSPERO (ID:CRD42024527799), were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.24 The following electronic databases were comprehensively searched: MEDLINE, Cochrane Library, Scopus, Registry of controlled Trials, Web of Science; using relevant keywords “diabetic macular edema”, “DME”, “bevacizumab”, “timolol”, “dorzolamide” from inception till 26 March 2024. All published articles were considered with no restrictions in terms of language or publication period. Further, we manually scanned the bibliography of retrieved articles for additional relevant studies.
Eligibility Criteria and Study Selection
We included studies with the following criteria: (a) randomized controlled trials (RCTs) that compared IVB (1.25 mg, monthly injection) with topical dorzolamide-timolol (twice daily) or dorzolamide alone (twice daily); (b) patients > 18 yrs, who had any type of diabetes, clinically significant DME and receiving naïve treatment; (c) reported data on any of the following outcomes: best-corrected visual acuity (BCVA), central macular thickness (CMT), intraocular pressure (IOP) at various weeks endpoints; (d) treatment duration at least 3 months. Articles were excluded if: (1) non-randomized controlled trials or comparative interventional case series; (2) studies with DR without macular edema or studies of macular edema due to causes other than DR; (3) macular edema related to recent intraocular surgery or other procedures; (4) studies that compared IVB or T or TD with different intervention; (5) studies that concerned with non-ocular outcomes or non-DME patients; (6) history of ocular surgery, coexistence of ocular diseases including glaucoma, significant cataract which affected patients’ vision, retinal diseases or vitreoretinal interface abnormalities; (7) severe comorbidities, uncontrolled diabetes mellitus, uncontrolled hypertension, history of cerebrovascular accident or arterial thromboembolic event; (8) history of any treatment for DR at any time or history of retinal photocoagulation. Duplicates were removed using Mendeley software and retrieved references were screened in two stepwise manner: titles/abstracts screening for matching our inclusion criteria, followed by a full-text appraisal of relevant articles for eligibility to meta-analysis. Each step was performed by two independent reviewers.
Data Extraction
Each type of dataset was extracted independently by two authors. Discrepancies were settled through discussion and consensus among the reviewers. The extracted data involved the study ID (name of the first author and year of publication), location, study design, major inclusion criteria, major exclusion criteria, various intervention groups (arm, dosage, number of injections and the interval in-between), number of patients, number of eyes and follow up duration, baseline characteristics for each intervention arm of enrolled patients (age, sex, type of DME), and Treatment outcome measures.
Data Synthesis and Quality Assessment
The primary outcomes of interest were best corrected visual acuity (BCVA), central macular thickness (CMT), intraocular pressure (IOP). These outcomes were extracted at baseline, 4, 8, and 12 weeks, as well as one-month post-treatment, to assess both short-term and long-term efficacy across treatment groups. The final measurements from Fazel et al and Sadr et al were collected at 12 weeks, while those from Fekri et al and Mirshahi et al were obtained one-month post-treatment.20–23 Means and standard deviations (SDs) for BCVA, CMT, and IOP at each endpoint were calculated per eye.
The quality of the studies was assessed using the Joanna Briggs Institute appraisal.25 The main objective of this checklist is to evaluate the methodological quality and the possibility of bias in the design and conduct and analysis of studies.
Statistical Analysis
Stata (StataCorp. 2024) was used for all statistical analyses. Continuous variables were presented as weighted means (effect size of means) and 95% confidence intervals (CIs), while categorical variables were presented as frequencies and percentages. All meta-analyses were conducted using the random-effects model.26,27 Subgroup analysis of weighted mean difference and 95% CI was performed to assess differences among intervention groups.28,29 Heterogeneity among studies was evaluated using the Chi-square (χ2) test and the Higgins I2 test.30 A two-tailed p-value of <0.05 was considered statistically significant for all statistical analyses. Egger’s test in addition to funnel plots were used to assess publication bias among included papers, and no bias was detected (all showed a p-value of > 0.05; Supplementary Figure 1a–c).31
 |
Figure 1 PRISMA flowchart for articles screening process. |
Results
Study Selection
The initial literature search of databases yielded a total of 635 articles (Figure 1). After removing duplicates, we were left with 623. By reviewing titles and abstracts, 546 studies were excluded. Seventy-seven papers were then retrieved and assessed for inclusion through a full text review process. Ultimately, 73 did not meet our inclusion criteria and were subsequently excluded. Therefore, four articles, categorized as level II evidence, were included in the analysis.20–23
Demographics and Clinical Characteristics
Our cohort includes a total of 98 patients that were diagnosed with diabetic macular edema, who received IVB alone, IVB+D, or IVB+TD. The overall weighted mean age of the entire cohort was 57.9 years [95% CI: 50.4 years – 65.6 years, p = 0.98], with an overall female predominance (n = 54/98, 55.1%). A total of 150 eyes underwent the clinical trials, with 75/150 (50.0%) eyes had IVB alone, 41/150 (27.3%) eyes had IVB+D, and 34/150 (22.7%) eyes had IVB+TD. See Table 1 for further details.
 |
Table 1 Overall Demographic and Clinical Data of the Included Studies |
Intervention Outcomes
In the subgroup meta-analysis, the overall weighted mean difference (WMD) in best-corrected visual acuity (BCVA) between groups was −0.125 [95% CI: −0.21 to −0.041]. The IVB+D group had a non-significantly different WMD [−0.05, 95% CI: −0.225 to 0.125] compared to both the IVB group [WMD: −0.094, 95% CI: −0.191 to 0.002] and the IVB+TD group [WMD: −0.206, 95% CI: −0.430 to 0.019, p = 0.56; Figure 2].
 |
Figure 2 Forest plots of mean change in BCVA measurements. Abbreviations: BCVA, best corrected visual acuity; IVB, intravitreal bevacizumab; IVB+D, intravitreal bevacizumab with topical dorzolamide; IVB+TD, intravitreal bevacizumab with topical timolol–dorzolamide; SD, standard deviation; CI, confidence interval. |
In terms of intraocular pressure (IOP), the subgroup meta-analysis revealed an overall WMD of −1.244mmHg [95% CI: −2.548mmHg to 0.06mmHg]. The IVB group demonstrated a statistically significant increase in IOP [WMD: 0.069mmHg, 95% CI: −0.554mmHg to 0.693mmHg] compared to both the IVB+D group [WMD: −1.274mmHg, 95% CI: −4.696mmHg to 2.147mmHg] and the IVB+TD group [WMD: −3.441mmHg, 95% CI: −4.101mmHg to −2.78 mmHg, p < 0.01; Figure 3]. Further pairwise comparisons revealed no significant difference between the IVB vs the IVB+D groups or the IVB+D vs the IVB+TD groups (p = 0.45 and p = 0.22, respectively). However, the pairwise comparison between the IVB vs IVB+TD groups did show statistical significance (p < 0.01).
 |
Figure 3 Forest plots of mean change in IOP measurements. Abbreviations: IOP, intraocular pressure; IVB, intravitreal bevacizumab; IVB+D, intravitreal bevacizumab with topical dorzolamide; IVB+TD, intravitreal bevacizumab with topical timolol–dorzolamide; SD, standard deviation; CI, confidence interval. |
Subgroup meta-analysis demonstrated an overall WMD of −78.875µm in central macular thickness (CMT) [95% CI: −118.606µm to −39.145µm]. There was no statistically significant difference between the WMD of the IVB group [−74.533µm, 95% CI: −86.756µm to −8.31µm], the IVB+D group [WMD: −88.9µm, 95% CI: −151.056µm to −26.744µm], and the IVB+TD group [WMD: −113.606µm, 95% CI: −197.59µm to −29.622µm, p = 0.27; Figure 4].
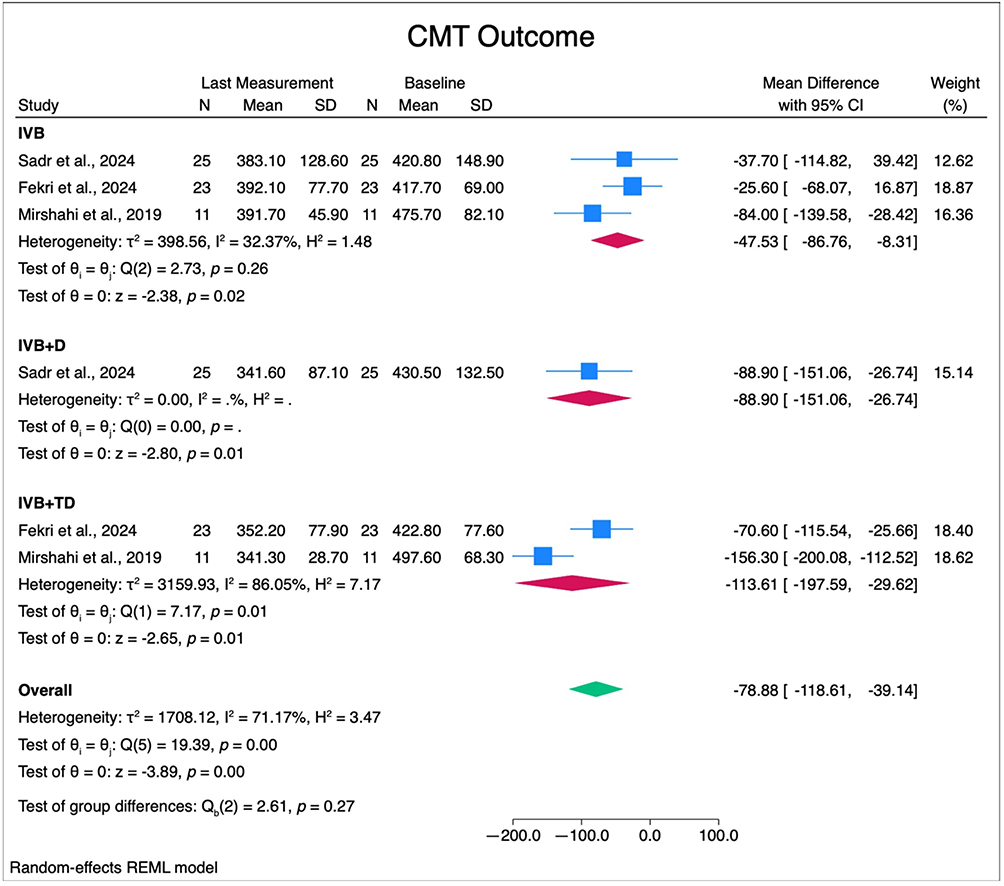 |
Figure 4 Forest plots of mean change in CMT measurements. Abbreviations: CMT, central macular thickness; IVB, intravitreal bevacizumab; IVB+D, intravitreal bevacizumab with topical dorzolamide; IVB+TD, intravitreal bevacizumab with topical timolol–dorzolamide; SD, standard deviation; CI, confidence interval. |
Discussion
Our systematic review and meta-analysis aimed to evaluate the treatment plan for diabetic macular edema (DME) by comparing the effects of intravitreal bevacizumab (IVB) alone versus IVB combined with timolol-dorzolamide or dorzolamide drops.
Anti-VEGF intraocular injections, such as bevacizumab, are widely recognized as effective treatments for DME.12,32 However, some patients exhibit resistance or a suboptimal response to anti-VEGF therapies.13,33 This phenomenon may be attributed to factors such as elevated anterior chamber outflow, which can expedite the clearance of anti-VEGF agents from the aqueous humor.13–15 Several studies have investigated the efficacy of combining anti-VEGF treatments with aqueous suppressant eye drops for managing macular edema, yielding mixed results.18,20–22
In our study, we compared three treatment groups for DME, all of which demonstrated significant improvements in best-corrected visual acuity (BCVA) and central macular thickness (CMT) at the final follow-up compared to baseline measurements. The most notable reduction in CMT was observed in the group receiving IVB combined with timolol-dorzolamide, followed by the IVB plus dorzolamide group, and lastly, the IVB-only group. Although the addition of timolol-dorzolamide showed better BCVA and CMT outcomes compared to the other two groups, the differences were not statistically significant. This is illustrated in Figures 1 and 2.
Intraocular pressure (IOP) measurements at the final follow-up indicated a decrease from baseline in the groups receiving topical drops, while the IVB-only group exhibited increased IOP levels, as shown in Figure 3. Notably, the IOP results in the IVB + timolol-dorzolamide group displayed high heterogeneity, likely due to variations in dosing frequencies of topical dorzolamide. For example, Sadr et al employed a regimen of three daily drops, whereas Fazel et al used a twice-daily schedule.21,22
In the discussion DME treatment, it is important to address the phenomenon of post-injection intraocular pressure (IOP) spikes. Intravitreal injections, including those of bevacizumab (IVB), can cause transient elevations in IOP immediately following the procedure. This spike in pressure is typically short-lived but can be a concern, especially in patients with pre-existing glaucoma or those at risk for optic nerve damage.34 The addition of topical IOP-lowering medications, such as timolol-dorzolamide or dorzolamide alone, to the treatment regimen may help mitigate these post-injection IOP spikes.34
Our study specifically focused on randomized controlled trials (RCTs) involving DME patients. While multiple studies have explored the effectiveness of carbonic anhydrase inhibitors, such as dorzolamide, in treating macular edema from various causes, our findings contribute uniquely to the understanding of DME treatment.35–40 Beyond its role as an aqueous suppressant, dorzolamide may also reduce macular edema by enhancing fluid transport through the retinal pigment epithelium and increasing choroidal blood flow.41,42 Additionally, beta-blockers, which serve as aqueous suppressants, may exert a downregulatory effect on VEGF and mitigate hypoxic conditions in the retina, as demonstrated in experimental animal studies.43
Despite the insights gained from our research, several limitations warrant consideration. The small sample size and the limited number of studies included in our analysis poses a significant constraint, primarily due to the underutilization of aqueous suppressant drops as adjunctive therapy to IVB in clinical practice. Consequently, the restricted number of eligible studies that met our inclusion criteria may limit the generalizability of our findings. Furthermore, during the statistical analysis, we noted the absence of demographic data for each intervention group. This lack of information hindered our ability to assess the homogeneity of the groups, which is crucial for drawing reliable comparisons and conclusions.
Nonetheless, our study provides valuable insights into the potential benefits of incorporating aqueous suppressant drops with IVB in managing DME. Future research should aim to address these limitations by conducting larger randomized trials with diverse participant populations and standardized treatment protocols.
Conclusion
In conclusion, our meta-analysis suggests that the addition of a combination drop containing a beta-blocker and a carbonic anhydrase inhibitor may enhance BCVA, CMT, and IOP outcomes more effectively in DME patients than either the addition of only a carbonic anhydrase inhibitor or the use of IVB alone. However, the observed improvements with IVB combined with timolol-dorzolamide were not statistically significant. The additional benefits of using a topical aqueous suppressant alongside IVB for DME treatment remain uncertain, complicating the ability to discern whether the observed effects are primarily attributable to IVB, the beta-blocker, or the carbonic anhydrase inhibitor.
Acknowledgments
We would like to express our sincere gratitude to all those who contributed to this research project. This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Zhang J, Zhang J, Zhang C, et al. Diabetic macular edema: current understanding, molecular mechanisms and therapeutic implications. Cells. 2022;11(21):3362. PMID: 36359761; PMCID: PMC9655436.doi:10.3390/cells11213362
2. Kuroiwa DAK, Malerbi FK, Regatieri CVS. new insights in resistant diabetic macular edema. Ophthalmologica. 2021;244(6):485–494. Epub 2021 May 21. PMID: 34023834.doi:10.1159/000516614
3. Daruich A, Matet A, Moulin A, et al. Mechanisms of macular edema: beyond the surface. progress in retinal and eye research. Progress in Retinal and Eye Research. 2018;63(63):20–68. doi:10.1016/j.preteyeres.2017.10.006
4. Thomas RL, Dunstan FD, Luzio SD, et al. Prevalence of diabetic retinopathy within a national diabetic retinopathy screening service. Br J Ophthalmol. 2015;99:64–68. doi:10.1136/bjophthalmol-2013-304017
5. Yau JWY, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35:556–564. doi:10.2337/dc11-1909
6. Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis. 2015;2(1):1–25. doi:10.1186/s40662-015-0026-
7. Xu H-Z, Le Y-Z. Significance of outer blood–retina barrier breakdown in diabetes and ischemia. Investigative ophthalmology &. Visual Science. 2011;52(5):2160–2164.
8. Musat O, Cernat C, Labib M, et al. DIABETIC MACULAR EDEMA. Rom J Ophthalmol. 2015;59(3):133–136.
9. Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. diabetes. 2005;54(6):1615–1625. doi:10.2337/diabetes.54.6.1615
10. Browning DJ, Altaweel MM, Bressler NM, et al. Diabetic macular edema: what is focal and what is diffuse? Am J Ophthalmol. 2008;146(5):649–655.e646. doi:10.1016/j.ajo.2008.07.013
11. Shah SU, Maturi RK. Therapeutic options in refractory diabetic macular oedema. Drugs. 2017;77(5):481–492. doi:10.1007/s40265-017-0704-6
12. Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, et al. Guidelines for the management of diabetic macular edema by the European society of retina specialists (EURETINA). Ophthalmologica. 2017;237(4):185–222. doi:10.1159/000458539
13. Bakri SJ, Snyder MR, Reid JM, et al. Pharmacokinetics of intravitreal bev- acizumab (Avastin). Ophthalmology. 2007;114(5):855–859. doi:10.1016/j.ophtha.2007.01.017
14. Krohne TU, Eter N, Holz FG, et al. Intraocular pharmacokinet- ics of bevacizumab after a single intravitreal injection in humans. Am J Ophthalmol. 2008;146(4):508–512. doi:10.1016/j.ajo.2008.05.036
15. Moisseiev E, et al. Pharmacokinetics of beva- cizumab after topical and intravitreal administration in human eyes. Graefes Arch Clin Exp Ophthalmol. 2014;252(2):331–337. doi:10.1007/s00417-013-2495-0
16. Sridhar J, et al. Topical dorzolamide–timolol with intravitreous anti-vascular endothelial growth factor for neovascular age-related macular degeneration. JAMA Ophthalmology. 2016;134(4):437–443. doi:10.1001/jamaophthalmol.2016.0045
17. Terashima H, Suzuki K, Kato K, et al. Membrane-bound carbonic anhydrase activity in the rat corneal endothelium and ret- ina. Jpn J Ophthalmol. 1996;40(2):142–153.
18. Byeon SH, Kwon OW, Song JH, et al. 2009 prolongation of activity of single intravitreal bevacizumab by adjuvant topical aqueous depressant (Timolol–Dorzolamide). Graefes Arch Clin Exp Ophthalmol. 2009;247(1):35–42. doi:10.1007/s00417-008-0917-1
19. Falavarjani KG, Hadi Y, Habibi A. Efficacy of topical timolol eye drops for the treatment of diabetic macular edema. Oph Thalmol Retina. 2019;3(6):538–539. doi:10.1016/j.oret.2019.01.017
20. Mirshahi A, Tadayoni R, Mohsenzadeh N, et al. Efficacy of adjuvant topical timo- lol–dorzolamide with intravitreal bevacizumab injection in diabetic macular edema: a contralateral eye study. J Curr Ophthalmol. 2019;31(2):168–171. doi:10.1016/j.joco.2019.01.008
21. Fazel F, Nikpour H, Pourazizi M, Nakazawa M. 2020 Combination of intravitreal bevacizumab and topical dorzolamide ver- sus intravitreal bevacizumab alone for diabetic macular edema: a randomized contralateral clinical trial. Biomed Res Int. 2020;2020:6794391. doi:10.1155/2020/6794391
22. Sadr A, Sargazi M, Banaie S, et al. Topical dorzolamide as adjunctive treatment with intravitreal bevacizumab in bilateral diabetic macular edema. Cureus. 16(2):e54829.>. doi:<doi
23. Fekri S, Rabiei A, Hooshmandi S, Nouri H, Abtahi SH. The effect of combination therapy with intravitreal bevacizumab and topical timolol-dorzolamide eye drops on diabetic macular edema: a double-blind randomized controlled trial. Int Ophthalmol. 2024;44(1):101. PMID: 38376643.doi:10.1007/s10792-024-03005-z
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
25. Barker TH, Stone JC1, Sears K, et al. Zachary1. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synth. 2023;21(3):494–506. doi:10.11124/JBIES-22-00430
26. Riley RD, Higgins JPT, Deeks JJ. Interpretation of random effects meta-analyses. BMJ. 2011;342(7804):964–967. doi:10.1136/BMJ.D549
27. Nikolakopoulou A, Mavridis D, Salanti G. How to interpret meta-analysis models: fixed effect and random effects meta-analyses. BMJ Ment Health. 2014;17(2):64. doi:10.1136/EB-2014-101794
28. Van den Noortgate W, Onghena P. Estimating the mean effect size in meta-analysis: bias, precision, and mean squared error of different weighting methods. Behav Res Methods Instrum Comput. 2003;35(4):504–511. doi:10.3758/BF03195529
29. Andrade C. Mean difference Standardized Mean Difference (SMD), and their use in meta-analysis: as simple as it gets. J Clin Psychiatry. 2020;81(5). doi:10.4088/JCP.20F13681
30. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/SIM.1186
31. Sterne JAC, Sutton AJ, Ioannidis JPA, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343(jul22 1):7818. doi:10.1136/BMJ.D4002
32. Wong TY, Sun J, Kawasaki R, et al. Guidelines on diabetic eye care: the international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology. 2018;125(10):1608–1622. doi:10.1016/j.ophtha.2018.04.007
33. Rush RB, Rush SW. Faricimab for treatment-resistant diabetic macular edema. Clin Ophthalmol. 2022;16:2797–2801. doi:10.2147/OPTH.S381503
34. Levin AM, Chaya CJ, Kahook MY, Wirostko BM. 2021 intraocular pressure elevation following intravitreal Anti-VEGF injections: short- and long-term considerations. J Glaucoma. 2021;30(12):1019–1026. doi:10.1097/IJG.0000000000001894
35. Grover S, Apushkin MA, Fishman GA. Topical dorzolamide for the treatment of cystoid macular edema in patients with retinitis pigmentosa. Am J Ophthalmol. 2006;141(5):850–858. doi:10.1016/j.ajo.2005.12.030
36. Obeid A, Hsu J, Ehmann D, et al. Topical dorzolamide-timolol with intravitreous anti-vascular endothelial growth factor for retinal vein occlusion: a pilot study. Retinal Cases Brief Rep. 2018.
37. Lemos Reis RF, Moreira-Gonçalves N, Estrela Silva SE, Brandão EM, Falcão-Reis FM. Comparison of topical dorzolamide and ketorolac treatment for cystoid macular edema in retinitis pigmentosa and Usher’s syndrome. Ophthalmologica. 2015;233(1):43–50. doi:10.1159/000368052
38. Kim DG, Yoon CK, Kim HW, Lee SJ. Effect of topical dorzolamide therapy on cystoid macular edema in hydroxychloroquine retinopathy. Can J Ophthalmol. 2018;53(3):e103–e107. doi:10.1016/j.jcjo.2017.10.022
39. Suzuki T, Hayakawa K, Onouchi Y, Ogata H, Nakagawa M, Kawai K. Topical dorzolamide for macular edema in the early phase after vitrectomy and epiretinal membrane re- moval. Clin Ophthalmol. 2013;7:549–553. doi:10.2147/OPTH.S42188
40. Genead MA, McAnany JJ, Fishman GA. Topical dorzolamide for treatment of cystoid macular edema in patients with choroideremia. Retina. 2012;32(4):826–833. doi:10.1097/IAE.0b013e3182215ae9
41. Shahsuvaryan ML. Carbonic anhydrase inhibitors in the management of macular edema: a review of the literature. Med Hypothesis Discov Innov Ophthalmol. 2022;11:34–41. doi:10.51329/mehdiophthal1443
42. Harris A, Ciulla TA, Pratt LM, et al. The effects of dorzolamide on choroidal and retinal perfusion in non-exudative age related macular degeneration. Br J Ophthalmol. 2003;87:753–757. doi:10.1136/bjo.87.6.753
43. Ristori C, Filippi L, Dal Monte M, et al. Role of the adrenergic system in a mouse model of oxygen-induced retinopathy: antiangiogenic effects of b-adrenoreceptor blockade. Investig Ophthalmol Vis Sci. 2011;52(1):155e170.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.