")
Back to Journals » Nature and Science of Sleep » Volume 17
Investigating ADHD Symptoms and Sleep Disturbances in Young Adults: A Cross-Sectional Study
Authors Demirkan AK , Semiz UB
Received 15 May 2025
Accepted for publication 29 June 2025
Published 12 July 2025 Volume 2025:17 Pages 1615—1628
DOI https://doi.org/10.2147/NSS.S537569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marco Veneruso
Arda Kazim Demirkan,1,2 Umit Basar Semiz3
1Department of Psychiatry, Samsun LIV Hospital, Samsun, Turkey; 2Department of Psychiatry, Agri Training and Research Hospital, Agri, Turkey; 3Faculty of Political Science, Ankara Medipol University, Ankara, Turkey
Correspondence: Arda Kazim Demirkan, Samsun LIV Hospital, Hancerli, Fatih Sultan Mehmet Cd, No: 155, 55020, Ilkadim, Samsun, Turkey, Tel +90 546 219 30 99, Fax +90 362 999 80 00, Email [email protected]
Purpose: Attention-deficit/hyperactivity disorder (ADHD), a prevalent condition affecting 2.5– 5% of adults, impacting daily functioning. Sleep quality is essential for cognitive and socio-emotional well-being, and the association between ADHD symptoms and sleep disturbances necessitates identifying populations at risk. This study aimed to assess the associations between ADHD symptoms and sleep disorders by conducting a thorough assessment of sleep measures in a cross-sectional group of university students.
Patients and Methods: Recruiting participants from a Turkish university (n=503; mean age=21.3 ± 1.8 years), subgroups were formed based on ADHD scores from the Adult ADHD Self-report Scale. Sleep was assessed using the Van Dream Anxiety Scale, Pittsburgh Sleep Quality Index (PSQI), and Epworth Sleepiness Scale (ESS). Beck Depression Inventory (BDI) was employed to evaluate depressive symptoms.
Results: ADHD symptoms group exhibited higher dream-related anxiety, PSQI, ESS, and BDI scores. Nightmares were more prevalent in the ADHD symptoms group. Subjective sleep measures showed differences in various domains, emphasizing poorer sleep quality in the ADHD symptoms group. Correlation analyses revealed intricate relationships between socio-economic factors, psychiatric health, family history, ADHD symptoms, nightmares, and sleep aspects.
Conclusion: University students with ADHD symptoms face increased susceptibility to insufficient sleep, impacting daytime functioning and academic performance. Findings underscore the need for increased attention to sleep health in this population.
Plain Language Summary: We wanted to understand how sleep problems affect university students who have symptoms of attention-deficit/hyperactivity disorder (ADHD). ADHD can make it harder to focus, stay organized, and manage time. People with ADHD often report having trouble sleeping, but we wanted to learn more about how sleep and mood might be linked to these symptoms. To do this, we asked students to fill out questionnaires about their sleep habits, feelings, and ADHD symptoms. We compared students with ADHD symptoms to those without.
We found that students with ADHD symptoms: (1) Had more trouble falling or staying asleep, (2) Felt sleepier during the day, (3) Had more nightmares, (4) Reported feeling more depressed. We also discovered that poor sleep and low mood were strongly related to ADHD symptoms. In fact, sleep and mood explained about 68% of the differences in ADHD symptom levels.
Students with ADHD symptoms were also more likely to sleep fewer hours than recommended. This can affect learning, memory, and daily life. Things like staying up late to study, using phones or computers at night, or having a busy social life may make sleep worse.
Even though the study relied on self-reported answers and included students from only one university, the results suggest that better sleep and emotional support might help reduce ADHD symptoms and improve students’ well-being.
Our research highlights the importance of supporting healthy sleep habits and mental health in students who experience attention difficulties.
Keywords: ADHD, sleep disturbances, young adults, university students, sleep quality
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common condition, affecting approximately 2.5–5% of adults globally.1 Widely studied in the field of child and adolescent psychiatry, ADHD typically manifests during childhood, and around 60–70% of individuals continue to experience symptoms into adulthood.2 According to the current diagnostic criteria defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM), the core symptoms are listed as inattention, hyperactivity, and/or impulsivity.3 Without intervention, individuals with ADHD encounter difficulties across essential aspects of functioning, such as emotional, academic, occupational, and social domains. Recent international consensus papers also highlight that ADHD is a highly heritable, neurodevelopmental disorder that often persists into adulthood and is associated with significant impairments across multiple life domains.4
Insufficient and poor-quality sleep has a negative impact on cognitive abilities and socio-emotional behavior.5,6 These impairments are particularly relevant in individuals with attention-deficit/hyperactivity disorder (ADHD), as research indicates that sleep disturbances are more common in this population and can worsen core ADHD symptoms such as inattention and impulsivity.7,8 Moreover, ADHD itself is known to negatively influence sleep regulation, leading to a bidirectional relationship between sleep and symptom severity.9,10 Therefore, it is essential to identify populations at higher risk for sleep disturbances, especially among those already experiencing cognitive and behavioral challenges.
The characteristics and prevalence of sleep disturbances in ADHD have been extensively investigated, and data revealed that ADHD not only impacts daytime functioning but also nighttime behaviors, particularly influencing the quantity and quality of sleep, which describes the ADHD as a 24-hour disorder. However, analyses of both objective and subjective measures of sleep have yielded conflicting results, depending on the complex interaction between ADHD and sleep patterns.11,12 Moreover, sleep problems may also contribute to the development of or mimic the ADHD-like symptoms, which can lead to misdiagnosis, whereas sleep problems may worsen the ADHD symptoms, and potentially affect the treatment and functioning in children, adolescents, and adults.13,14
Sleep disorders commonly associated with ADHD include delayed sleep, insomnia, periodic limb movements in sleep, obstructive sleep apnea, and sleep-disordered breathing. These associations are well-documented in studies utilizing actigraphy, polysomnography, and EEG.13,15,16
The United States National Sleep Foundation recommends seven to nine hours sleep duration for young adults and adults.17 Various indices and scales have been developed to classify the measures of sleep quality and the presence of sleep-disruptive events.
Although previous studies have documented the presence of sleep disturbances in individuals with ADHD, much of the existing literature has focused on children and adolescents or has relied on small clinical samples. There is a relative lack of research examining sleep characteristics and their association with ADHD symptoms in non-clinical young adult populations, particularly university students.
While the relationship between ADHD and sleep has been explored in various populations, few studies have focused on non-clinical, university-aged young adults using multiple validated self-report measures. Additionally, this study offers a more comprehensive view by simultaneously examining ADHD symptoms, sleep quality, daytime sleepiness, dream-related anxiety, and depressive symptoms within a single model. By doing so, we aim to provide a clearer understanding of the psychological and behavioral profiles of young adults with ADHD symptoms and identify specific sleep-related targets for future interventions in academic and healthcare settings.
This study aims to address this gap by investigating the relationship between ADHD symptoms and subjective sleep quality in a university student sample. We hypothesized that students with ADHD symptoms would report more sleep disturbances, greater daytime sleepiness, and higher levels of depressive symptoms compared to their peers without ADHD symptoms.
Materials And Methods
Participants and the Definition of ADHD
The study participants had a mean age of 21.35±1.86 years, with a female-to-male ratio of 266 to 237. Out of 503 individuals, 87 had self-reported symptoms of ADHD. Participants were recruited from a university located in the Southeastern of Türkiye and the study group consisted of active student from different faculties and educational levels. The university is composed of 38 departments with over 27000 active students. Recruitment efforts involved distributing flyers in cafeterias and utilizing institutional Email addresses.
The inclusion criteria included registered students aged 18 years or older, those complied with the study requirements and signed written informed consent. The exclusion criterion was the students who did not fully participate in the completion of all forms.
The study was approved by the local ethical committee of Local University (approval date/no: 09.03.2018/18-22), and written informed consent was obtained. Participants were informed of the voluntary nature of their involvement, and they were reminded that they are allowed to terminate their participation at any point. Standardized assessment procedures were applied uniformly to all potential participants.
Detailed instructions were provided to each participant on how to complete the questionnaire. Questionnaires were administered in medium-sized groups ranging from 40 to 50 individuals in classrooms designated for the study during specified time slots on school days.
Exclusion criteria were as follows: the absence of at least one completed scale or questionnaire, withdrawal from the study, and individuals who subsequently requested exclusion from the study population. To reduce potential confounding effects of ADHD pharmacotherapy on sleep outcomes, participants who were currently receiving pharmacological treatment for ADHD (eg, stimulant or non-stimulant medications) were excluded from the study.
Subgrouping of individuals was based on their scores on the validated Turkish version of the World Health Organization’s Adult Attention Deficit Hyperactivity Disorder Self-Report Scale (ASRS), which is an 18-item self-report questionnaire, designed to evaluate ADHD symptoms, while Part A contains 6 items and Part-B contains 12 additional questions. The Turkish adaptation has demonstrated strong psychometric properties, with inter-group correlation of 0.85 (0.73–0.91) and Cronbach’s alpha of 0.88.18
In this study, a cut-off score of 24 or higher on either of the two subscales were considered“high risk for ADH”. This threshold has been supported by validation studies conducted in Turkish adult populations and is commonly used in population-based research to indicate a high likelihood of clinically relevant ADHD symptoms.18–20 We note that the ASRS is a screening tool and not a diagnostic instrument; therefore, participants meeting the cut-off are referred to as having“high risk for ADHD” not a formal diagnosis. Permission for the use of the scale was obtained from the relevant institution.
ADHD symptom status was determined exclusively through self-report using the ASRS; no clinical interviews or additional diagnostic assessments were conducted.
Measures
The Van Dream Anxiety Scale (VDAS): The VDAS is a validated tool that comprises 17 self-rated questions designed to assess nightmare frequency and dream anxiety resulting from frightening dreams over the past month (Cronbach α=0.87).21 Four additional questions collect clinical information but do not contribute to the scoring.
Twelve questions focus on various aspects, including nightmare frequency, difficulty in falling asleep after a nightmare, fear of sleeping due to anticipated nightmares, trouble in sleeping, nightmare recall frequency, daytime sleepiness, daytime anxiety, difficulty in routines, familial distress, social distress, psychological disturbances, and memory/concentration difficulties. Each of these questions is scored on a scale from 0 to 4 points. There is also a question regarding somatic symptoms (shortness of breath, dizziness, exhaustion, palpitation, sweating, shivering, nausea, stomachache, tightness in chest, dry mouth, fear of death, and sore throat), with each symptom scored from 0 to 4 points.
The total score is categorized as follows: 0–10 = 0; 11–20 = 1; 21–30 = 2; 31–40 = 3; and 41–48 = 4.
The Pittsburgh Sleep Quality Index (PSQI): The Pittsburgh Sleep Quality Index (PSQI) is a self-rated questionnaire which assesses sleep quality and sleep disturbances over 1-month interval.22 The scale consists of 7 components as follows: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction. Every component is evaluated with a scale of 0–3. Higher scores indicate worse sleep quality. The Turkish version was validated by Agar et al in 2021 (Cronbach α=0.752).23
The Epworth Sleepiness Scale (ESS): The ESS is a self-administered questionnaire comprising 8 questions on a 4-point scale (0–3).24 The individuals are questioned of their typical likelihood of dozing off or falling asleep while participating in eight distinct activities as follows: sitting and reading, watching TV, sitting, inactive, in a public place (eg, in a meeting, theater, or dinner event), sitting as a passenger in a car for an hour or more without stopping for a break, lying down to rest when circumstances permit, sitting and talking to someone, sitting quietly after a meal without alcohol, sitting in a car, while stopped for a few minutes in traffic or at a light. The ESS score, calculated as the sum of the scores for the 8 items, and a higher ESS score indicates the presence of daytime sleepiness. The Turkish version of the scale was validated by Agargun et al in 1999 (Cronbach α=0.80).25 Permission was obtained from the relevant institution for the use of the scale.
Beck Depression Inventory (BDI): The BDI is a widely utilized self-report assessment tool consisting of 21 multiple-choice questions.26 This inventory is designed to measure the severity of depression in individuals. Each question offers a set of at least four possible answer choices, each representing varying levels of intensity. The higher scores indicate more severe depressive symptoms. The Turkish version of the scale was validated by Hisli (Cronbach α=0.86).27 The necessary permission for the use of the scale was secured from Giunti Psychometrics on behalf of Pearson Assessment US.
Statistical Analysis
The sample size was calculated to be 450 participants, accounting for a 10% dropout rate, with a significance level of 0.05. Descriptive results are presented as frequencies (n) and percentages. Differences between the ADHD symptoms groups and comparison groups in all variables were calculated by using chi-square test or Student’s t-test. The correlations were calculated using Pearson’s correlation coefficient testing. All the analysis was performed using SPSS version 21 (SPSS® 25.0 (IBM Corporation, Armonk NY, USA) for Windows®). Significance was set to alpha < 0.05 (two-sided).
Results
In this study comprising 503 university students, we compared sleep-related, mood, and ADHD symptom measures between a group with ADHD symptoms (n = 87) and a comparison group (n = 416) (Table 1). The groups did not differ significantly in terms of age, gender, marital status, socioeconomic background, or presence of social security. Similarly, there were no significant differences in self-reported psychiatric or physical disorders, nor in family history of psychiatric conditions.
 |
Table 1 Comparison of Sociodemographic Variables Between ADHD and Control Groups |
The results of the study revealed significant group differences between the ADHD symptoms group and the comparison group across various measures (Table 2). The ADHD symptoms group exhibited higher scores in ASRS Inattention (Subscale A), ASRS Hyperactivity (Subscale B), and ASRS total score compared to the comparison group, indicating greater attention and hyperactivity symptoms in the ADHD symptoms group (p < 0.0001).
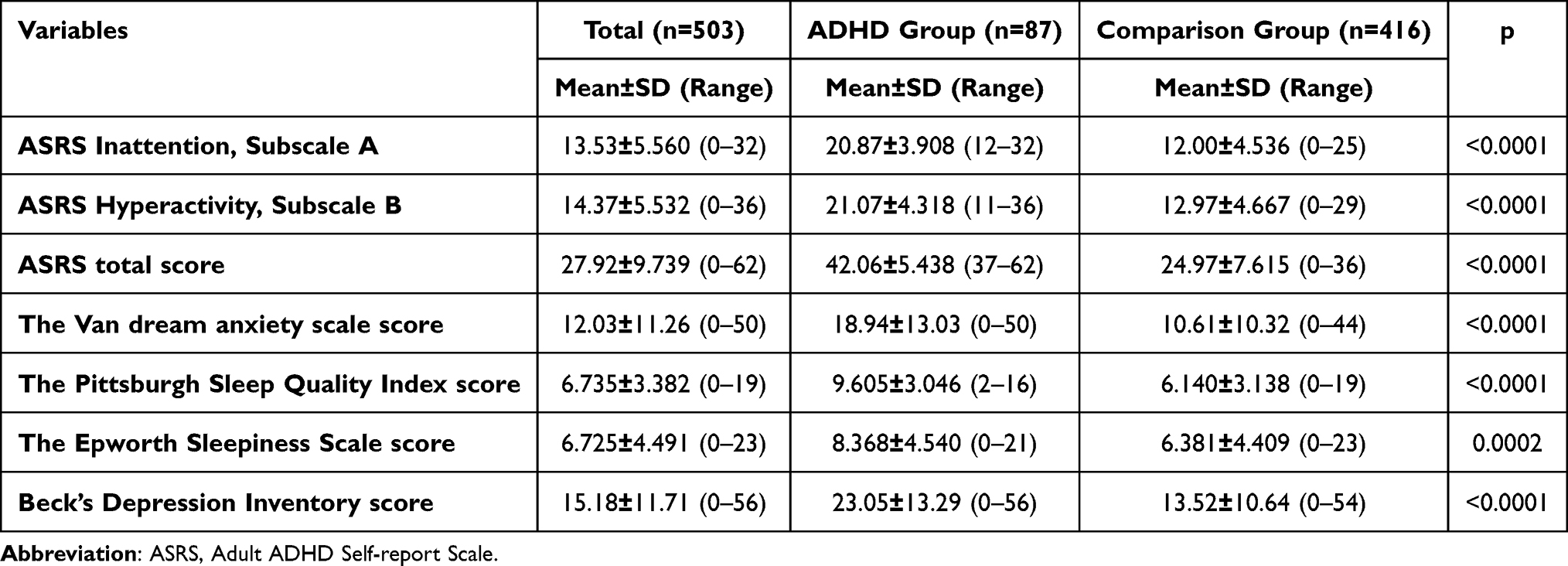 |
Table 2 Comparison of Parametric Data Between the Study Groups |
Similarly, the Van Dream Anxiety Scale score was significantly higher in the ADHD symptoms group, suggesting increased dream-related anxiety (p <0.0001). Additionally, the ADHD symptoms group demonstrated higher scores in the Pittsburgh Sleep Quality Index and Beck Depression Inventory, indicating poorer sleep quality and higher levels of depression compared to the comparison group (p < 0.0001). The Epworth Sleepiness Scale score was also significantly higher in the ADHD symptoms group, suggesting increased daytime sleepiness (p = 0.0002).
The presence of nightmares showed a significant difference between groups (p = 0.0316), with a higher prevalence in the ADHD symptoms group.
Sleep-related measures, including the Pittsburgh Sleep Quality Index (PSQI) subscales, exhibited significant differences in subjective sleep quality (p = 0.0003), sleep latency (p = 0.0010), sleep duration (p = 0.0118), habitual sleep efficiency (p < 0.0001), sleep disturbances (p = 0.0014), and daytime dysfunction (p < 0.0001) between the ADHD symptoms and comparison groups. The habitual use of sleeping medications did not show difference between the groups (p = 0.5088) (Table 3).
 |
Table 3 Comparison of Nonparametric Data Between the Study Groups |
Correlation coefficients were calculated and are presented in the correlation matrices (Tables 4 and 5) below. The evaluation of these indices revealed variable coefficiencision within the groups for both demographic and study variables.
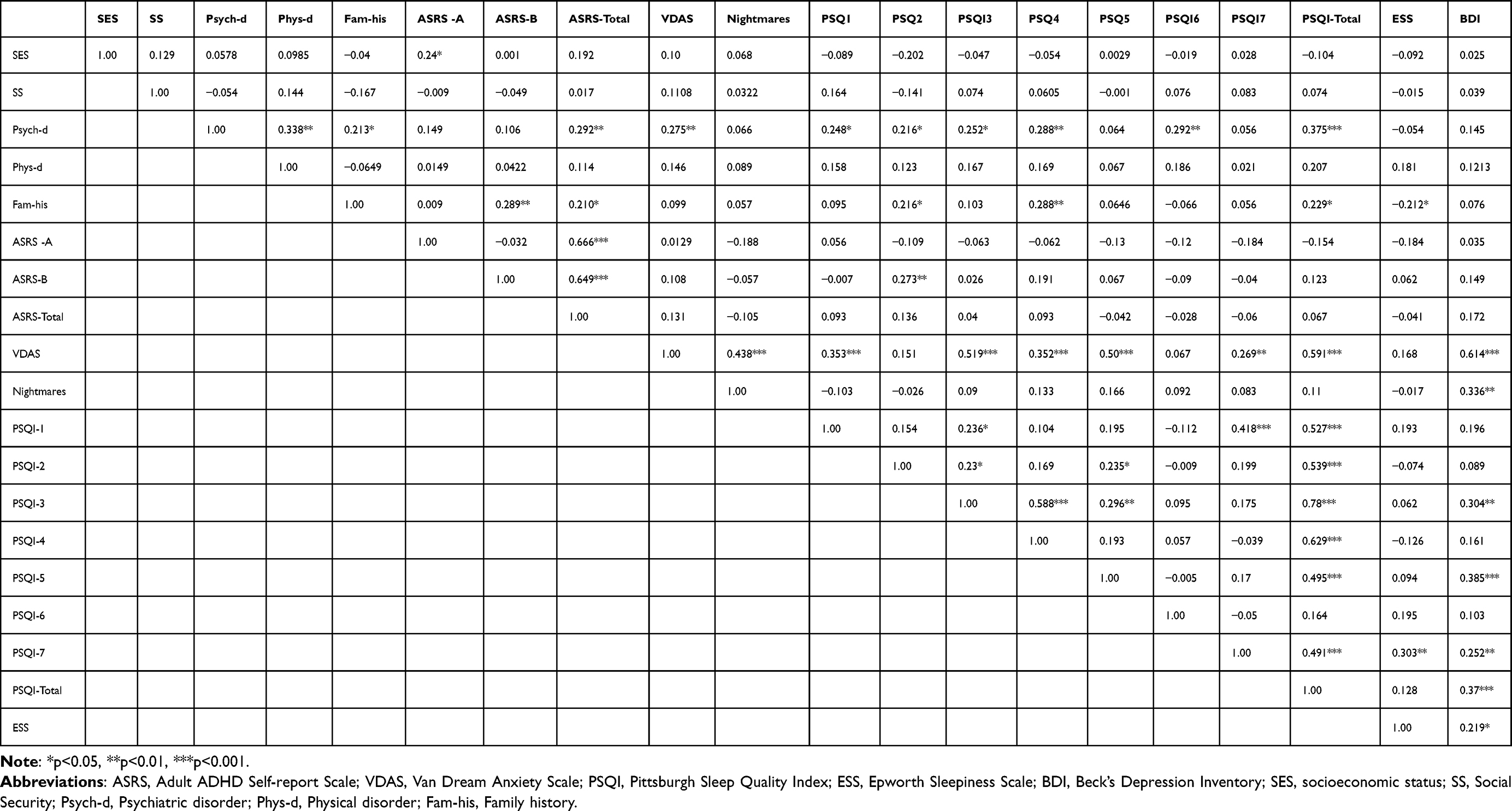 |
Table 4 Correlation Matrix for the ADHD Group |
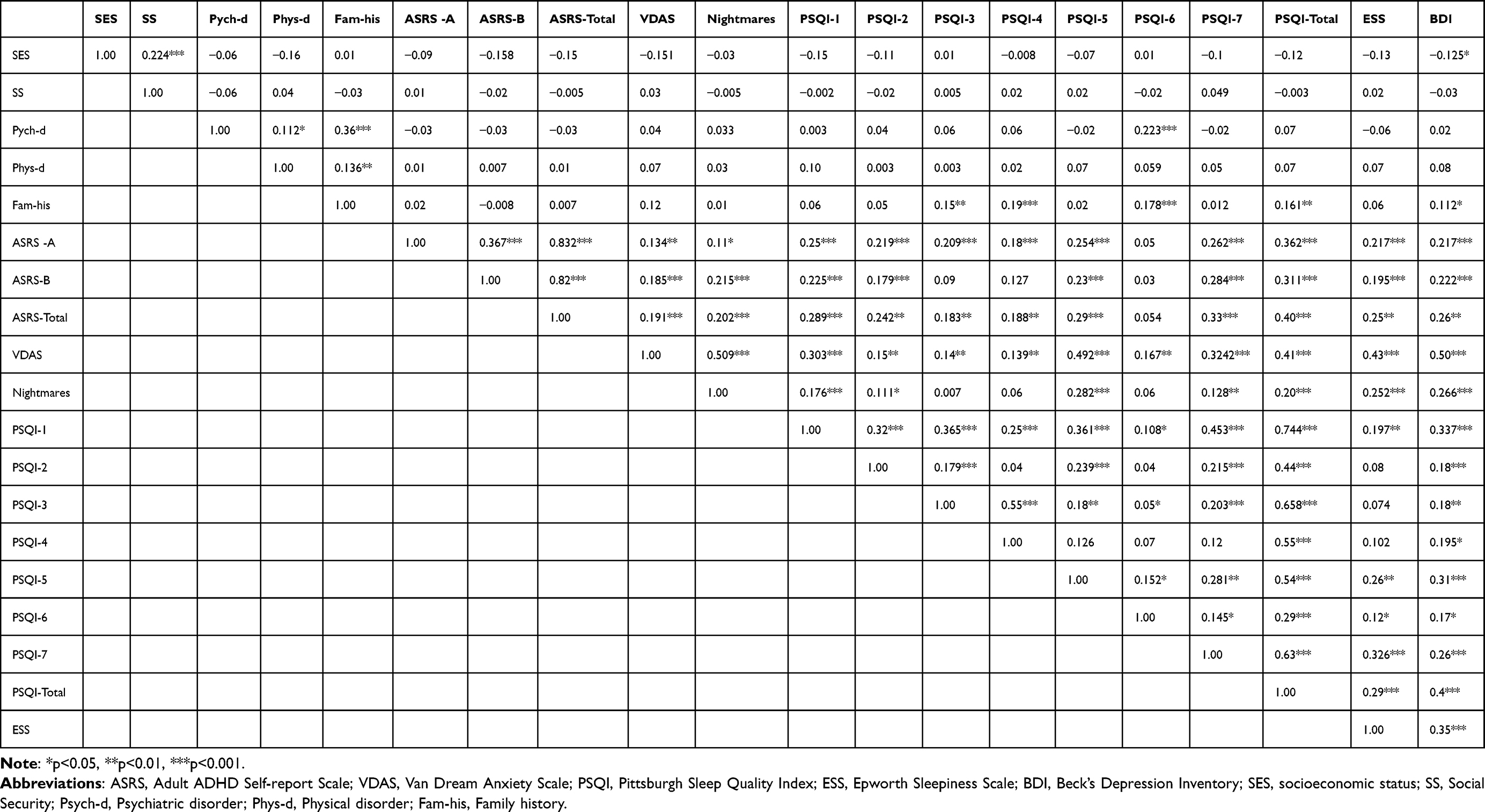 |
Table 5 Correlation Matrix for the Comparison Group |
The multiple linear regression table provides insights into the relationship between ADHD symptoms and other predictors (Table 6). According to analysis, 68.2% of the variability in ADHD symptoms can be explained by the presence of nightmares, sleep quality, sleepiness, and depression.
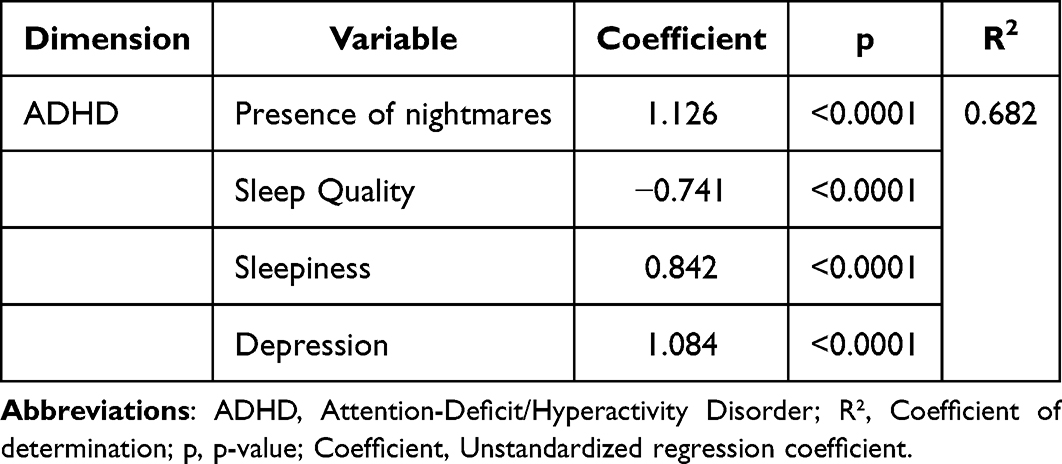 |
Table 6 Multiple Linear Regression with ADHD as the Outcome Variable |
In summary, young adult university students with ADHD symptoms (mean age: 21.35 years) exhibited significantly elevated levels of dream-related anxiety, poor sleep quality, and daytime sleepiness compared to their peers. They also reported higher rates of nightmares, longer sleep latency, reduced sleep duration, lower habitual sleep efficiency, and increased daytime dysfunction. These findings underscore a clear pattern of more severe and multifaceted sleep disturbances among students at high risk for ADHD.
Discussion
In the context of this study, the diagnosis of high risk for ADHD was done according to a self-reported scale validated and widely employed by the national authorities. Furthermore, we aimed to utilize different measurement tools for the quality of sleep and presence of depressive symptoms, in an attempt to increase data credibility. The self-reported high risk for ADHD prevalence was 17.29% in our study group, while in their exploratory study on a sample of Iranian student, Jahangard et al reported a self-rated ADHD prevalence rate of 16.5%.28 This rate is notably higher than the global adult ADHD prevalence estimates, which typically range from 2.5% to 5%. One possible explanation for this discrepancy is the use of self-report screening tools, which may overestimate symptom severity and frequency compared to structured clinical interviews. Additionally, cultural factors, academic pressures, and sleep-related problems common in university settings may lead students to report more symptoms consistent with ADHD. It is also possible that some students with subclinical or situational difficulties scored above the cut-off, inflating prevalence rates. In addition, although ADHD is typically reported to be more prevalent in males, particularly in childhood and adolescence,4 our sample exhibited a nearly equal gender distribution, with a slightly higher number of female participants. This demographic characteristic may reflect differences in symptom recognition, help-seeking behavior, or academic engagement in young adults. It is also possible that sleep-related disturbances manifest differently across genders, potentially influencing symptom reporting and overall sleep profiles. Future studies should examine sex-specific patterns in ADHD and sleep relationships more directly.
Findings of other studies demonstrated increased levels of sleep perturbances and daytime sleepiness in children and adolescents with ADHD.29,30 Consistent with previous research, we found supporting evidence for increased sleep problems in young adults with ADHD symptoms than age-matched comparison group, when subjective measures of sleep were used. Furthermore, BDI scores were significantly higher in the ADHD symptoms group, and there was a strong correlation between the ASRS subscales scores and various components of sleep indices.
In relation to existing literature, our findings align with prior studies demonstrating poor sleep quality and increased daytime sleepiness in individuals with elevated ADHD symptoms. However, our results extend current knowledge by focusing specifically on a non-clinical sample of university students and by examining a broader range of sleep-related factors, including dream-related anxiety and depressive symptoms. While previous studies often rely on clinical populations or adolescents, our work highlights the relevance of sleep disturbances and mood symptoms in a high-functioning academic population. Furthermore, the regression analysis demonstrating that 68.2% of the variability in ADHD symptoms was explained by sleep and mood factors provides strong support for the interrelated nature of these domains. These findings underscore the need for integrated approaches in both academic support services and mental health interventions targeting this demographic.
Taken together, findings from this study indicate that young adults with high risk for ADHD obtain less sleep than their peers, and are more likely to obtain insufficient sleep, nightmares and daytime dysfunction and sleepiness, while they experience sleep disturbances, and have more difficulties initiating/maintaining sleep compared to the similar age individuals without ADHD symptoms.
Current recommendations for sleep durations for young adults and adults are even to nine hours, and 7–8 hours of sleep is recommended for older adults.17 In our study group, which falls into 7–9 hours’ sleep duration group, the number of individuals with a regular sleep duration of 7 hours or longer was significantly lower in the ADHD symptoms group. In their cross-sectional study of 689 young adults with a mean age of 20 ± 1.35 years, Stefan et al reported a 17.4% range of sleep duration shorter than 6 hours and between 6–7 hours.31 They further note that, in an adjusted model, a sleep duration shorter than seven hours and longer than ten hours were both associated with impaired self-rated health.
Several studies have reported the presence of sleep disturbances characterized by poor-quality and insufficient sleep in individuals from families with low income or belonging to ethnic minorities, across all age groups.32,33 However, in our study group, we did not observe statistical significance in terms of socio-economic status or the presence of social security when comparing individuals with and without ADHD symptoms.
Although both over the counter and prescription medications such as diphenhydramine and zolpidem and stimulant medication for ADHD can contribute into the development of disrupted sleep and daytime sleepiness, we did not find a difference between two groups in terms of use of sleep medications.34
The association between mood disorders and sleep disturbances has long been recognized, with sleep debt in college students linked to a higher risk of reporting depressive symptoms. Recent studies also indicate that having less than 8 hours of night sleep is associated with an almost threefold increased risk of suicide attempts, even after accounting for various confounding variables.35,36 In our study, although we inquired about the history of psychiatric disorders and family history of psychiatric disorders, there was no significant difference between the groups in terms of these variables. Interestingly, presence of a psychiatric disorder prevalence was 2.58% in the total sample, with a slightly higher rate in the ADHD symptoms group (4.59%), though not reaching statistical significance. This finding underlines the complex structure of the ADHD etiology, and the broad spectrum of its clinical presentation. It is noteworthy, however, that while the presence of a family history of psychiatric disorders was 4.59% in the ADHD symptoms group compared to a 1.68% ratio in the comparison group, this difference did not reach statistical significance (p = 0.0912) and possibly influenced by the characteristics of the sampled pool. This finding is somewhat unexpected, particularly given the higher BDI scores observed in the ADHD symptoms group. One possible explanation is that participants underreported existing psychiatric diagnoses or family history due to stigma, lack of awareness, or limited access to formal evaluations. Additionally, the self-report format of the questionnaire and relatively young age of the sample may have contributed to this finding. This discrepancy further highlights the need for clinician-administered assessments in future research to ensure accurate identification of psychiatric comorbidities and familial risk.
Even though our study focused on university students, the findings reported here align closely with previous research. Our results highlight a concerning trend, indicating that university students with ADHD symptoms report higher levels of insufficient sleep, leading to a shortened and insufficient sleep duration that is likely to affect daytime functioning and academic performance adversely. It is possible that various contextual factors—such as part-time employment, irregular academic schedules, seasonal changes, social demands, communal living arrangements, and caffeine consumption—may influence sleep patterns in university students. While these factors were not directly assessed in the present study, they represent plausible contributors to sleep disruption and warrant investigation in future research. In our study, we found that The Van dream anxiety scale score, The Epworth Sleepiness Scale score and the sub elements of Pittsburgh Sleep Quality Index were significantly different in the ADHD symptoms group, which might be exacerbated with all those factors.
Previous studies have noted that individuals with ADHD tend to go to bed either later or earlier during the week and wake up slightly earlier on school days. Unfortunately, we did not record the bedtime and wake-up time in our study group. Late bedtime in the ADHD group was attributed to several factors, including technology use, completing school projects or studying for exams. Additionally, individuals in this group reported challenges with time management, including issues such as procrastination.37
The observed correlations in our study group suggest intricate relationships between lower socioeconomical status, impaired psychiatric and physical health, a family history of psychiatric disorders, ADHD symptoms, higher scores of nightmares, and various aspects of sleep disturbances. Further exploration and interpretation of these findings are essential for a comprehensive understanding of the interplay between these variables.
Similar to our study, a recent report by Regli et al among a group of Swiss medical students, self-reported psychiatric issues were linked to higher levels of depression and insomnia, as well as reduced cognitive reappraisal and social activity. Additionally, medical students exhibited higher insomnia scores and fell into more severe insomnia categories compared to non-medical students.38
According to the multiple linear regression model, there was a strong relationship between ADHD symptoms and the presence of nightmares, sleep quality, sleepiness, and depression. The presence of nightmares was strongly associated with higher ADHD symptom scores; However, the directionality of this relationship cannot be determined due to the study’s cross-sectional design. Also, a poorer sleep quality and increased sleepiness are associated with higher ADHD symptoms. A relatively higher R² value of 0.682 in our study indicates that 68.2% of the variability in ADHD symptoms can be explained by and supported with the presence of nightmares, sleep quality, sleepiness, and depression. These findings suggest that improving sleep quality, reducing nightmares, and addressing depression may be associated with reduced ADHD symptom severity. However, causal interpretations should be made with caution given the cross-sectional nature of the study.
Our study has several limitations that merit consideration. First, the sample comprised university students from a single metropolitan area, which may limit the generalizability of the findings to other age groups or cultural contexts. Second, sleep questionnaires were not stratified by weekdays versus weekends and we relied solely on subjective measures; objective assessments such as polysomnography, actigraphy, or the multiple sleep latency test were not employed. Third, the prevalence of sleep-breathing disorders such as obstructive sleep apnea was not evaluated, and unrecognized apnea could have contributed to elevated daytime sleepiness in some participants.
Additionally, ADHD symptoms were identified using a self-report screening instrument rather than clinical interviews. This introduces a risk of inflated prevalence estimates and misclassification bias, as self-reported symptoms may be influenced by other factors—particularly sleep-related difficulties—that mimic core ADHD features such as inattention, impulsivity, and poor emotional regulation. Future research should combine structured diagnostic assessments with objective sleep measures and explicitly control for sleep variables to enhance diagnostic accuracy and clarify the directionality of the observed associations.
Conclusions
In conclusion, our findings indicate that university students with elevated ADHD symptoms experience significantly poorer sleep quality, increased dream-related anxiety, higher levels of depressive symptoms, and more pronounced daytime sleepiness compared to their peers. These results highlight the importance of considering sleep health and emotional functioning when evaluating ADHD symptoms in young adults, especially in academic settings.
The strong associations observed between ADHD symptoms and various sleep-related indices suggest that sleep may play an important role in the manifestation or exacerbation of attentional and emotional difficulties.
Further research using objective sleep measurements and clinical diagnostic interviews is warranted to better understand the directionality and underlying mechanisms of these associations.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study received ethical approval from the local ethical committee of Agri İbrahim Çeçen University (approval date/no: 09.03.2018/18-22), and written informed consent was obtained. All procedures performed in studies involving human participants adhered to the 1964 Helsinki Declaration and its later amendments.
Consent for Publication
Participants were informed of the voluntary nature of their involvement, and they were reminded that they are allowed to terminate their participation at any point. Standardized assessment procedures were applied uniformly to all potential participants.
Author Contributions
AKD was responsible for conceptualization, methodology, investigation, data curation, formal analysis, and writing – original draft and review & editing. UBS participated in investigation, resources and supervision. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflict of interest to declare.
References
1. Song P, Zha M, Yang Q, Zhang Y, Li X, Rudan I. The prevalence of adult attention-deficit hyperactivity disorder: a global systematic review and meta-analysis. J Global Health. 2021;11:4009. doi:10.7189/jogh.11.04009
2. Singh A, Yeh CJ, Verma N, Das AK. Overview of attention deficit hyperactivity disorder in young children. Health Psychol Res. 2015;3(2):2115. doi:10.4081/hpr.2015.2115
3. American Psychiatric Association.DSM-5 Task Force. (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5TM.
4. V FS, Banaschewski T, Coghill D, et al. The world federation of ADHD international consensus statement: 208 evidence-based conclusions about the disorder. Neurosci Biobehav Rev. 2021;128:789–818. doi:10.1016/j.neubiorev.2021.01.022
5. Mehta KJ. Effect of sleep and mood on academic performance—at interface of physiology, psychology, and education. Humanit Soc Sci Commun. 2022;9(1):16. doi:10.1057/s41599-021-01031-1
6. Gobin CM, Banks JB, Fins AI, Tartar JL. Poor sleep quality is associated with a negative cognitive bias and decreased sustained attention. J Sleep Res. 2015;24(5):535–542. doi:10.1111/jsr.12302
7. Yoon SYR, Jain U, Shapiro C. Sleep in attention-deficit/hyperactivity disorder in children and adults: past, present, and future. Sleep Medicine Reviews. 2012;16(4):371–388. doi:10.1016/j.smrv.2011.07.001
8. Dvorsky M, Langberg J. Predicting impairment in college students with ADHD: the role of executive functions. J Attention Disord. 2019;23:1624–1636. doi:10.1177/1087054714548037
9. Cortese S, Faraone SV, Konofal E, Lecendreux M. Sleep in children with attention-deficit/hyperactivity disorder: meta-analysis of subjective and objective studies. J Am Acad Child Adolesc Psychiatry. 2009;48(9):894–908. doi:10.1097/CHI.0b013e3181ac09c9
10. Bijlenga D, Vollebregt MA, Kooij JJS, Arns M. The role of the circadian system in the etiology and pathophysiology of ADHD: time to redefine ADHD? Attention Deficit Hyperactivity Disorders. 2019;11(1):5–19. doi:10.1007/s12402-018-0271-z
11. Becker SP. ADHD and sleep: recent advances and future directions. Curr Opinion Psychol. 2020;34:50–56. doi:10.1016/j.copsyc.2019.09.006
12. Weiss MD, Craig SG, Davies G, Schibuk L, Stein M. New research on the complex interaction of sleep and ADHD. Current Sleep Med Rep. 2015;1(2):114–121. doi:10.1007/s40675-015-0018-8
13. Hvolby A. Associations of sleep disturbance with ADHD: implications for treatment. Attention Deficit Hyperactivity Disorders. 2015;7(1):1–18. doi:10.1007/s12402-014-0151-0
14. Um YH, Hong SC, Jeong JH. Sleep problems as predictors in attention-deficit hyperactivity disorder: causal mechanisms, consequences and treatment. Clinical Psychopharmacology Neurosci. 2017;15(1):9–18. doi:10.9758/cpn.2017.15.1.9
15. Miano S, Esposito M, Foderaro G, Ramelli GP, Pezzoli V, Manconi M. Sleep-related disorders in children with attention-deficit hyperactivity disorder: preliminary results of a full sleep assessment study. CNS Neurosci Ther. 2016;22(11):906–914. doi:10.1111/cns.12573
16. Miano S, Amato N, Foderaro G, et al. Sleep phenotypes in attention deficit hyperactivity disorder. Sleep Medicine. 2019;60:123–131. doi:10.1016/j.sleep.2018.08.026
17. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1(1):40–43. doi:10.1016/j.sleh.2014.12.010
18. Doǧan S, Öncü B, Varol-Saraçoǧlu G, Küçükgöncü S. Erişkin dikkat eksikliǧi hiperaktivite bozukluǧu kendi bildirim ölçeǧi (ASRS-v1.1): türkçe formunun geçerlilik ve güvenilirliǧi. Anadolu Psikiyatri Dergisi. 2009;10(2):77–87.
19. Dogan S, Öncü B, Varol Saraçoğlu G, Kucukgoncu S. Üniversite Öğrencilerinde Dikkat Eksikliği Hiperaktivite Bozukluğu Belirti Sıklığı Ve Belirti Düzeyi İle İlişkili Gelişimsel. Akademik Ve Psikolojik Etmenler Türkiye’de Psikiyatri. 2008;10:109–115.
20. Baran Tatar Z, İ Y, Oflaz S, Büyükgök D. The relationship between emotion recognition and the symptoms of attention deficit and impulsivity in adult patients with attention deficit. Türk Psikiyatri Derg. 2015;26(3):172–180.
21. Agargun M, Kara H, Bilici M. The van dream anxiety scale: a subjective measure of dream anxiety in nightmare sufferers. Sleep and Hypnosis. 1999;4:204–211.
22. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. the Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
23. Mutlu HH, İ A, Malakcıoğlu C. The validity and reliability of Turkish version of basic scale on insomnia complaints and quality of sleep. Turkish J Family Med Primary Care. 2021;15(4):846–852. doi:10.21763/tjfmpc.971532
24. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
25. Ağargün M, Çilli A, Kara H, et al. Epworth Uykululuk Ölçeği’nin geçerliği ve güvenirliği. Türk Psikiyatri Derg. 1999;10(4):261–267.
26. Beck AT, Ward C, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch. Gen. Psychiatry. 1961;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
27. Hisli N. Beck Depresyon Ölçeği’nin bir Türk örnekleminde geçerlilik ve güvenilirliği. Psikoloji Dergisi. 1988;6:118–122.
28. Jahangard L, Haghighi M, Bajoghli H, Holsboer-Trachsler E, Brand S. Among a sample of Iranian students, adult attention deficit hyperactivity disorder is related to childhood ADHD, but not to age, gender, socioeconomic status, or birth order--an exploratory study. Int Psychiatry Clin Practice. 2013;17(4):273–278. doi:10.3109/13651501.2013.800555
29. Qu X, Kalb LG, Holingue C, et al. Association of time in bed, social jetlag, and sleep disturbances with cognitive performance in children with ADHD. J Attention Disord. 2024;28(1):99–108. doi:10.1177/10870547231204010
30. Chaulagain A, Lyhmann I, Halmøy A, et al. A systematic meta-review of systematic reviews on attention deficit hyperactivity disorder. Eur Psychiatry. 2023;66(1):e90. doi:10.1192/j.eurpsy.2023.2451
31. Štefan L, Juranko D, Prosoli R, Barić R, Sporiš G. Self-reported sleep duration and self-rated health in young adults. J Clin Sleep Med. 2017;13(7):899–904. doi:10.5664/jcsm.6662
32. Grandner MA, Jackson NJ, Izci-Balserak B, et al. Social and behavioral determinants of perceived insufficient sleep. Front Neurol. 2015;6:112. doi:10.3389/fneur.2015.00112
33. Sheehan C, Li L, Petrov ME. How did trends in sleep duration in 2020 compare to previous years and how did they vary by sex, race/ethnicity, and educational attainment? Sleep Medicine. 2023;101:570–577. doi:10.1016/j.sleep.2022.12.008
34. Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13(2):307–349. doi:10.5664/jcsm.6470
35. Becker SP, Dvorsky MR, Holdaway AS, Luebbe AM. Sleep problems and suicidal behaviors in college students. J Psychiatr Res. 2018;99:122–128. doi:10.1016/j.jpsychires.2018.01.009
36. Gunderson J, McDaniel K, DiBlanda A. association between insufficient sleep, depressive symptoms, and suicidality among Florida high school students. Preventing Chronic Dis. 2023;20:E59. doi:10.5888/pcd20.220403
37. Uygur ÖF, Bahar A. The relationship between attention deficit hyperactivity disorder symptoms and bedtime procrastination. J Contemporary Med. 2023;13(2):241–246. doi:10.16899/jcm.1242778
38. Regli J, Sadeghi-Bahmani D, Rigotti V, et al. Psychiatric characteristics, symptoms of insomnia and depression, emotion regulation, and social activity among Swiss medical students. J Clin Med. 2024;13(15):4372. doi:10.3390/jcm13154372
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.