")
Back to Archived Journals » Open Access Surgery » Volume 17
Is Occlusion the Solution? REBOA as a Hemorrhage Control Adjunct
Authors Lee SK , Mukherjee K
Received 4 April 2024
Accepted for publication 11 September 2024
Published 7 October 2024 Volume 2024:17 Pages 145—156
DOI https://doi.org/10.2147/OAS.S429607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Sarah K Lee,1 Kaushik Mukherjee2
1Department of Plastic Surgery, University of California Irvine Health, Irvine, CA, USA; 2Division of Acute Care Surgery, Loma Linda University Health, Loma Linda, CA, USA
Correspondence: Kaushik Mukherjee, Division of Acute Care Surgery, Loma Linda University Health, 11175 Campus Street, CP, 21111, Loma Linda, CA, 92350, USA, Tel +001 909-558-4286, Fax +001 909-558-236, Email [email protected]
Abstract: Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) has emerged as a promising intervention for hemorrhagic shock and traumatic injury management, offering a minimally invasive means of aortic occlusion compared to resuscitative thoracotomy. While REBOA’s origin dates back to the 1950s, recent advancements have made it more accessible and applicable in various clinical scenarios. REBOA has become increasingly utilized in not only the exsanguinating trauma patient but also in non-traumatic hemorrhage as a bridge to definitive hemostatic control. This article reviews the procedure and mechanism, clinical applications, and challenges associated with the REBOA. There are several challenges to consider when implementing the REBOA, particularly in procedural execution and patient selection. Determining the ideal candidates for REBOA remains inconclusive, with varying outcomes reported in different patient populations. Additionally, the potential for ischemic complications, such as visceral organ injury, end organ damage, and lower extremity ischemia, underscores the critical importance of procedural planning and ongoing monitoring. Partial and intermittent REBOA techniques have been introduced to mitigate ischemic complications associated with complete occlusion, but their efficacy and safety warrant further investigation. Beyond technical considerations, logistical and institutional factors pose as potential barriers to the effective utilization of REBOA, highlighting the importance of standardized training and a multidisciplinary approach when establishing a REBOA program. REBOA offers promising advancements in hemorrhage control, and the technology continues to evolve to address potential challenges and complications. Further research is imperative to delineate its optimal use and potential impact on patient outcomes.
Keywords: traumatic hemorrhagic shock, REBOA, postpartum hemorrhage, partial REBOA, aortic occlusion, endovascular
Background
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a minimally invasive method to obtain proximal aortic control.1 Although REBOA has gained traction in the trauma literature over the last decade, balloon occlusion of the aorta for hemorrhage control is not a novel concept, with its first reported use in 1954 by Hughes during the Korean War.2–7 Endovascular aortic occlusion has been frequently utilized in vascular surgery, primarily in the setting of ruptured abdominal aortic aneurysms.3,8 With the development of lower profile devices, REBOA has been made more easily accessible in trauma surgery with the ability to initiate aortic occlusion in the emergency department and operating room.9–14
REBOA can be utilized as a temporizing measure in hemodynamically unstable trauma patients with abdominopelvic hemorrhage, supporting cerebral and coronary perfusion until definitive hemostasis can be achieved.1 In some high-volume trauma centers, REBOA has reduced or even replaced emergency department resuscitative thoracotomy with traumatic arrest due to sub-diaphragmatic hemorrhage.7 The use of REBOA has also been explored in non-traumatic etiologies of hemorrhage, including postpartum hemorrhage, placenta accreta spectrum disorders, upper gastrointestinal bleeding, and pelvic surgery.3,15–18
Multiple large animal studies have demonstrated improved survival and early clinical studies have shown the feasibility of REBOA.12,13,19–23 However, there are no randomized control trials to define specific indications for its use and the benefits of REBOA have not been consistently demonstrated in the literature, with some groups reporting increased mortality associated with REBOA use.23,24 Given the varying results and relatively new technology, there are several challenges and potential complications that should be considered when using REBOA.
REBOA: The Procedure
Stannard et al outlines the procedure of REBOA into five steps: 1) Arterial access, 2) Balloon selection and positioning, 3) Balloon inflation, 4) Balloon deflation, and 5) Sheath removal.25
Access is obtained via the common femoral artery (CFA) either by percutaneous access or femoral artery cutdown. Early users of REBOA utilized the existing aortic balloon occlusion devices used by vascular surgeons for the management of ruptured abdominal aortic aneurysms, which required long stiff guidewires under fluoroscopy and a larger introducer 12Fr sheath necessitating open repair of the arteriotomy at the time of sheath removal making the procedure less feasible for bedside use. Smaller wire-free devices have been developed which allow introduction of the balloon through a 7Fr sheath.9,26,27
Mechanism of REBOA
The aorta is divided into zones I, II, III from proximal to distal respectively (Figure 1). Zone I comprises the descending thoracic aorta between the origin of the left subclavian artery and celiac arteries; zone II the paravisceral aorta between the celiac artery and the lowest renal artery; and zone III the infrarenal abdominal aorta between the lowest renal artery and the aortic bifurcation.25
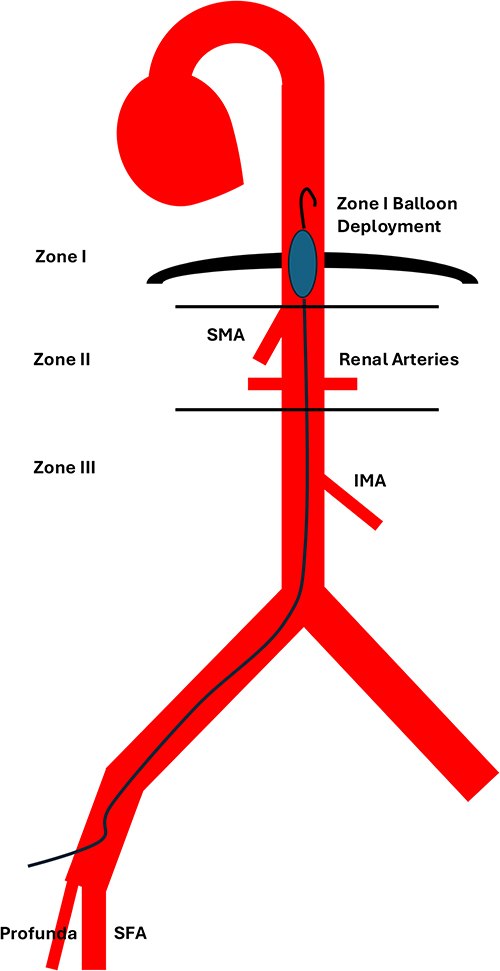 |
Figure 1 Critical anatomy for REBOA catheter placement. Note that the arterial sheath must be inserted into the common femoral artery (CFA) between the inguinal ligament and the bifurcation into the superficial femoral artery (SFA) and the profunda femoris artery (PFA). The balloon must then be deployed either in Zone I (distal to the left subclavian artery but proximal to the celiac axis) or in Zone III (between the inferior mesenteric artery [IMA] and the aortic bifurcation). |
Current literature suggests that Zone I occlusion be performed in the setting of suspected intra-abdominal hemorrhage while Zone III occlusion be performed for hemorrhage from pelvic injuries.1,7,28 Tibbits et al recommends that REBOA, if indicated, be placed in Zone I in a hypotensive trauma patient with a systolic blood pressure <90 mmHg, even if the suspected injury is in the pelvis or lower extremities allowing for adequate perfusion of the brain, heart, and lungs as Zone III occlusion alone does not provide adequate resuscitation in hemorrhagic shock.29 However, this recommendation must be balanced against the potential risk of visceral ischemia.
Zone I balloon occlusion leads to acute changes in cardiovascular circulation and organ perfusion as illustrated in the existing vascular surgery literature regarding aortic occlusion.30 In a patient with normal ventricle, zone I balloon occlusion results in increase in LV afterload, wall tension, and mean central aortic pressure with associated increase in subendocardial oxygen demand.28 In contrast, Zone III occlusion is not associated with the same profound cardiovascular effects with a modest increase in proximal blood pressure on occlusion.29,31
Clinical Applications and Indications
There is no high-grade evidence that supports specific indications for REBOA but its use has been suggested for traumatic life-threatening subdiaphragmatic hemorrhage for patients in hemorrhagic shock refractory to resuscitation.5 REBOA has been implemented not only in traumatic abdominopelvic hemorrhage but also postpartum hemorrhage and placenta accreta spectrum disorders, upper gastrointestinal bleed, and pelvic hemorrhage during pelvic and sacral tumor resection, and hepatobiliary surgery.15–18,32
Shaw et al suggests that REBOA should be considered in patients with abdominal or pelvic hemorrhage who demonstrate transient response or non-response after traditional resuscitation methods to stabilize the patient until definitive hemostasis can be obtained.26
REBOA has also been shown to have similar to superior outcomes compared to resuscitative thoracotomy (RT) in trauma patients. In the preliminary data from the prospective multicenter Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry that included 285 patients, zone I REBOA was associated with improved survival compared to RT, particularly in those who do not require cardiopulmonary resuscitation (CPR).33 More recent data from the same group which included 991 patients reflected similar results—zone I REBOA was associated with a statistically significant lower mortality compared to RT (78.6% [44] vs 92.9% [52]; P = 0.03).22 Koh et al found that REBOA and RT conferred similar survival in patients presenting with traumatic cardiac arrest.34 Brenner et al found that in patients presenting with TBI, mortality was significantly higher in RT compared to REBOA.35
In Japan, where trauma surgeons are not typically immediately available in-house, current recommendations suggest Zone I REBOA placement in the hemodynamically unstable trauma patient without access to immediate surgical treatment. A study demonstrated that in unstable trauma patients requiring surgical intervention, REBOA was associated with improved overall survival, with benefit particularly in patients with delay to the operating room of one to three hours from presentation.36
REBOA may also facilitate imaging in select patients, particularly patients who stabilize with zone III REBOA deployment after high-energy blunt trauma mechanisms; in these cases REBOA placement followed by imaging may facilitate a higher likelihood of hemorrhage control in interventional radiology as opposed to in the operating room.37
REBOA use has expanded and is being investigated in the setting of non-traumatic hemorrhage. Studies have demonstrated that the prophylactic use of zone III REBOA in patients with suspected placenta accreta spectrum disorder undergoing cesarean hysterectomy results in less intraoperative blood loss and lower transfusion requirements compared to no REBOA.15,16 REBOA has also been used in emergency surgery patients with hemorrhagic shock, although this group has high mortality.38
Challenges in REBOA
Procedural Challenges
Davidson et al outlined challenges and complications of each step of REBOA solicited from anecdotal experience of experts in the field in North America, Asia, and Europe.39
Percutaneous CFA access can be a near impossible task in a pulseless patient actively receiving CPR in a hectic trauma bay, further exacerbated by hemorrhagic shock, catecholamine surge, and vasospasm. In addition, a large body habitus, variant anatomy, arterial tortuosity, and atherosclerotic lesions can further complicate access. The CFA is located approximately one fingerbreadth below the inguinal ligament and visualization of external landmarks may require retraction of the pannus or a longer access needle in the pregnant or obese patient (Figure 1). Superficial femoral artery (SFA) access must be avoided given the smaller caliber vessel and risk for arterial thrombosis and inadvertent puncture into the external iliac can lead to noncompressible retroperitoneal hemorrhage. Accidental cannulation of the inferior vena cava is also possible as it is difficult to differentiate between venous and arterial blood in a hypotensive hypoxic patient. Ultrasound can aid in successful identification and cannulation of the CFA; however, some of the authors of the study group favor open arterial cut-down for patients in extremis.40
The rate-limiting step of REBOA initiation is CFA access and early access has been associated with improved survival.41,42 Therefore, many experts recommend early femoral access with routine small sheath placement in patients with sustained systolic blood pressure of less than 90 mm Hg.39 This principle is the cornerstone for institutional guidelines, including the guideline used at the authors’ institution (Figure 2).
 |
Figure 2 Institutional protocol for early arterial access and pREBOA-PRO. Hypotensive trauma patients with systolic blood pressure (SBP) < 90 mm Hg that do not improve with 2 units of packed red blood cells (PRBC) and 2 units of fresh frozen plasma (FFP) or 2 units of Low Titer O Positive Whole Blood (WB) are considered for massive transfusion protocol (MTP) and tranexamic acid (TXA) followed by large bore central venous catheter and possible femoral arterial line placement. Two arterial line transducers are used for this device; one is at the tip of the catheter proximal to the balloon and indicates the blood pressure experienced by the brain and heart. The second is transduced at the level of the sheath and reveals the blood pressure distal to the balloon. The pREBOA-PRO balloon is deployed in Zone I if the intra-abdominal focused abdominal sonogram for trauma (FAST) is positive; for FAST- patients the balloon is deployed in Zone III. The systolic blood pressure (SBP) above the balloon is intended to be above 90 mm Hg (or 100 mm Hg in patients with suspected traumatic brain injury). The distal SBP is intended to be at least 30 mm Hg. FAST+ patients with increased pelvic volume on X-ray undergo exploratory laparotomy (XLap) and preperitoneal pelvic packing (PPP) and may undergo computed tomography (CT) or other interventions if needed. FAST+ patients with normal pelvic volume undergo laparotomy and similarly may go to CT or other interventions if needed. FAST- patients with increased pelvic volume on X-ray under PPP with other interventions as needed. Finally, FAST- patients with normal pelvic volume who are still in shock undergo Zone I pREBOA placement followed by imaging to help determine the cause of shock. |
Appropriate balloon positioning is imperative for successful use of REBOA as balloon inflation in the incorrect zone can have catastrophic outcomes. Zone I and zone III are the two anatomical locations described for REBOA use. Zone I aortic occlusion is associated with a greater distal ischemic burden compared to Zone III occlusion.29 Malposition and inflation of the balloon in the heart or aortic arch can lead to direct myocardial damage due to excessive afterload and occlusion of the great vessels. Inflation in zone II can augment blood flow through the celiac axis leading to exacerbation of upper abdominal bleeding as well as precipitate renal ischemia. Distal inflation in the iliac artery can worsen proximal hemorrhage and potentiate direct arterial damage leading to acute limb ischemia. While appropriate catheter position can be confirmed on fluoroscopy, fluoroscopy-free catheters have been developed. These catheters have a flexible and J-curved tip with centimeter markings on the catheter to allow measurement of insertion length based on external landmarks. Cadaveric analysis demonstrates that for zone I REBOA, measuring the mid-sternum to the puncture site without curving the catheter results in deployment in the appropriate landing zone.43 Computerized tomographic (CT) analysis found that zone I deployment can also be achieved with fixed catheter insertion lengths, with adjustments based on torso length and zone III insertion can be approximated by measuring 5.5 cm above the umbilicus.44,45 However, REBOA placement by external landmark measurement is not always accurate in actual patients, especially in zone III.46 In clinical practice, catheter insertion distance is highly variable and REBOA position should be confirmed with fluoroscopy or x-ray.47
When positioning the balloon, the catheter should not be advanced if resistance is met. This can be for several reasons including arterial thrombosis, placement into an aortic branch vessel, or placement through an injured vessel. Additionally, underlying vascular pathology such as an arterial dissection flap, atherosclerosis, aneurysm, or vessel tortuosity can lead to difficulty advancing the catheter. If the user experiences resistance, imaging should be obtained to evaluate balloon location. In the case of inability to advance the catheter into the desired location, alternative site for access (ie, contralateral CFA) should be considered or an alternate plan must be formulated. In an unstable patient with arterial injury or incompatible anatomy, endovascular hemorrhagic control may not be feasible.
The ER-REBOA (Prytime Inc., Boerne TX), a wire-free device which was approved by the FDA in 2015 and commercially available in the United States, has radiopaque markers to guide balloon position.
Balloon inflation during REBOA is typically performed blind. The balloon should be inflated until met with resistance or distal pulses disappear. Overinflation of the balloon can lead to aortic injury or balloon rupture resulting in abrupt cessation of hemodynamic support and continuation of hemorrhage.48 The Basic Endovascular Skills for Trauma (BEST) course teaches that adequate balloon inflation is assessed through haptic feedback—a skill that novice users may not have developed.49 Alternatively, if the distal arterial waveform is present prior to balloon inflation, the disappearance of the waveform from the introducer sheath can be used as a surrogate marker of aortic occlusion. Additionally, the loss of bilateral femoral pulses indicates adequate inflation if present previously. Malposition of the catheter should be suspected if there is no change in femoral pulses upon balloon inflation. The loss of solely the ipsilateral femoral pulse indicates iliac artery placement and the catheter should be repositioned.
Management During Balloon Occlusion
Due to distal ischemia associated with aortic occlusion, timely hemorrhagic control is necessary as the maximum tolerated occlusion time is unknown. Guidelines suggest that complete zone I REBOA occlusion should not exceed 30 minutes and perhaps should not even be used if definitive hemorrhagic control cannot be accomplished within 15 minutes of balloon inflation.5 Zone III REBOA is tolerated for more extended periods of time compared to zone I, but inflation time should target less than 30 minutes but no greater than 60 minutes for complete occlusion.5
The swift restoration of aortic flow after balloon inflation can lead to supraphysiologic blood pressure and proximal organ perfusion, resulting in increased cardiac afterload that can precipitate myocardial dysfunction and cerebral edema.14,19,50 However, in animal models, the observed increase in carotid flow and intracranial pressures did not equate to radiographic progression of traumatic brain injury.14
Due to increase in proximal aortic pressure and recirculation of volume after balloon inflation, an undiagnosed injury above the level of the occlusion may be exacerbated. This highlights the importance of pre-procedural ultrasound and x-ray to recognize preclusion to REBOA placement, such as hemorrhage into the thoracic cavity, aortic, or cardiac injury.4 It is also important to note that maintaining zone I occlusion is a dynamic process and the volume needed to maintain adequate occlusion may increase after improvement of hemodynamics, especially after resuscitation with fluids or blood products.51 Therefore, careful titration of infusion rates for resuscitation is paramount during balloon inflation.
Distal organ ischemia and mortality during balloon occlusion are time-dependent.52 Acidosis and lactate worsen with aortic occlusion and prolonged balloon occlusion leads to a systemic inflammatory response that can induce cardiopulmonary dysfunction and acute respiratory distress syndrome (ARDS).52,53
During balloon deflation, communication between the surgical and anesthesia team is integral as the rapid decrease in afterload can lead to hypotension, further exacerbated by reperfusion, washout of metabolic byproducts, and acidosis.25 Guidelines recommend slow balloon deflation over five minutes to allow for gradual restoration of blood flow to tissue beds and prevent reperfusion injury.49 However, animal models demonstrate that gradual balloon deflation still leads to a rapid reintroduction of aortic flow and significant drop in mean arterial pressure (MAP) due to the compliant nature of the balloon.54 Intermittent and partial REBOA have been investigated to ameliorate distal ischemia and ischemia-reperfusion, and will be discussed later in this review.
After the balloon is deflated and REBOA is no longer required, the catheter should be removed after hemostasis is achieved and coagulopathy is corrected. Complete balloon deflation must be ensured prior to catheter removal to avoid entrapment into a vessel and vascular injury. Arterial access-related ischemic limb complications related to REBOA vascular access develop in nearly 10% of patients in some series, with some patients requiring lower limb amputation.55 However, access-related complications are more commonly associated with larger-profile catheters and the newer smaller sheaths have been found to have fewer complications.55,56 A retrospective cohort analysis of the AORTA registry evaluated vascular access site complication (VASC) in 24-hour survivors who underwent REBOA, defined as presence of hematoma, pseudoaneurysm, arteriovenous fistula, arterial stenosis, or use of patch angioplasty for closure. The overall VASC rate was 7% with hematoma being the most common, comprising 40% of the VASC complications. Although VASC were associated with limb ischemia, surgical intervention and amputation were rare.57 After sheath removal, the manual or ultrasound compression should be performed to prevent hematoma or pseudoaneurysm formation. The access site and distal extremities should be monitored closely with some experts suggesting routine duplex ultrasonography of the ipsilateral leg and a low threshold for re-exploration, which is the routine at the author’s institution.16
Challenges of Patient Selection and Resources
Equipment/Training
Though interest from providers for REBOA exists, widespread implementation is lacking. Review of the TQIP data from 2017 identified 51 TQIP centers reporting REBOA cases with a median of six cases/center/year (IQR 4–7). Of these 51 centers, 87% were Level 1, 11% Level 2, and 2% Level 3 trauma centers. There are currently more than 800 trauma centers contributing data in TQIP which suggests that in 2017 the vast majority of US trauma centers were not using REBOA.5 The basic endovascular skills for trauma (BEST) course is a virtual reality simulation that has been created to train providers in proper technique for REBOA, which demonstrated significant improvements in knowledge and procedural task times after course completion.49 In addition to training, a multidisciplinary approach is imperative for successful establishment of a REBOA program.58
A study evaluated outcomes based on the volume of REBOA performed at 20 different hospitals, comparing high-volume (defined as ≥80 cases during the study period), mid-volume (defined as 10–20 cases during the study period), and low-volume (<10 cases during the study period). Odds of successful REBOA placement were increased at high- and mid-volume centers compared to low-volume centers. Low REBOA-volume hospitals also had a longer median time from patient presentation to initiation of REBOA placement at 45 minutes in low-volume centers, 17 minutes in mid-volume centers, and 11.5 minutes in high-volume centers. Median time to aortic occlusion followed the same trend at 45 minutes in low-volume centers, 36 minutes in mid-volume centers, and 23 minutes in high-volume centers.59
Additionally, there is no true consensus of which patients would benefit from REBOA. According to an autopsy study, 13.6% of patients who suffered pre-hospital cardiac arrest were considered to be candidates for prehospital REBOA, defined as abdominal organ injury and/or pelvic fracture with non-compressible torso hemorrhage without severe head injury.60
Intermittent and Partial REBOA
Intermittent REBOA (iREBOA) and partial REBOA (pREBOA) have been introduced to mitigate ischemic injury and reperfusion injury associated with rapid balloon deflation associated with complete aortic occlusion.20 Animal studies have shown that intermittent and partial REBOA are equally efficacious in proximal aortic MAPs when compared to complete REBOA with less evidence of distal organ ischemia, and prolonged survival.10,11,20,61 In a swine model comparing no-REBOA, complete REBOA (cREBOA) and pREBOA, complete REBOA animals had profound hypotension following balloon deflation, even resulting in the death of one animal prior before the completion of the study whereas pREBOA experienced smaller decreases in blood pressure and continuing to maintain central MAP above the pre-hemorrhage baseline for the remainder of the study. Additionally, lactate in the pREBOA group remained similar to the non-REBOA group while lactate concentration in the cREBOA group continued to rise, tripling the peak concentration observed in both non-REBOA and pREBOA groups.
Although in theory these concepts make sense, animal and limited clinical data shows varying results. Animal models demonstrated that iREBOA was associated with more episodes of severe hypotension, more frequent rescue occlusion with more time at complete aortic occlusion, and less total distal perfusion compared to pREBOA. However, neither method demonstrated a survival benefit.21 Additionally, analysis of the international Aortic Balloon Occlusion database showed that there was no significant difference in mortality when comparing partial and total REBOA in patients with isolated abdominal trauma.62
Partial REBOA-PRO
The partial REBOA-PRO (pREBOA-PRO, Prytime Inc., Boerne TX) is a newer commercially available device has been introduced in select centers, which has a semi-compliant balloon with flow channels on the balloon surface to allow distal flow during partial inflation while still maintaining apposition to the aortic wall allowing for the option of either complete or partial occlusion. The pREBOA-PRO also consists of a pressure valve to prevent balloon overinflation. This is in contrast to the ER-REBOA, the first-generation aortic balloon occlusion device that consists of a balloon that when inflated, achieves complete aortic occlusion resulting in an “all or nothing” approach.10
In animal models, the original ER-REBOA and pREBOA-PRO performed similarly during complete aortic occlusion with a remarkable increase in the carotid flow rate and decrease in the distal aortic flow rate. However, during balloon deflation, there was a stronger correlation between distal aortic flow rate and balloon volume for the pREBOA-PRO (R2 = 0.91, P < 0.001) compared to the ER-REBOA (R2 = 0.74, P < 0.001). This indicates a more incremental return of distal aortic flow and controlled titration of distal aortic pressure in the partial REBOA compared to the more abrupt and rapid resumption of flow in the ER-REBOA.10
One swine study showed a lower degree of distal ischemia after two hours in zone I with pREBOA-PRO compared to complete REBOA. Upon gross inspection of the intraabdominal organs, all animals that underwent partial occlusion had minimal or surgically treatable ischemia, while all those that underwent complete occlusion sustained severe ischemic injuries classified as surgically untreatable. Additionally, partial REBOA subjects all had significantly lower lactate, LDH, and AST at the end of the experiment.11 A follow-up animal model compared zone I partial occlusion at two hours compared to four hours after volume-controlled hemorrhage (40% estimated blood loss) which found that all animals survived to the endpoint. There was no gross small bowel ischemia seen in the 2-hour group while the surgically resectable patchy short segment ischemia was observed in the 4-hour group, with neither group demonstrating nonsurvivable ischemic organ damage based on laboratory values and pathology.12,13,42
In a retrospective single center cohort study of patients receiving the ER-REBOA and pREBOA-PRO catheters for trauma, there was a significantly reduced incidence of AKI (6.7% vs 40%) with partial aortic occlusion using the pREBOA-PRO catheter.63
Currently, data on the pREBOA-PRO catheter is limited as its use is restricted to a small number of centers; however, additional data should be published within the next 12–24 months.
One potentially intriguing application of this technology is the use in the prehospital setting, either by trained physicians or military medics. This was tested in an observational study in the United Kingdom in patients with suspected subdiaphragmatic hemorrhage or traumatic cardiac arrest. Out of 11 patients, 11 had successful zone I balloon deployment. 9/11 patients underwent hemorrhage control procedures. Only 2 patients survived to discharge, however, with multiple organ dysfunction occurring in 10/11 patients receiving aortic occlusion. 7/11 patients had renal failure, with six treated with continuous renal replacement therapy. 4/11 patients had significant traumatic brain injuries. Two patients suffered acute intestinal ischemia, two developed distal arterial thrombus formation, and 2 patients received bilateral above the knee amputations which were completions of traumatic amputations. Of note, aortic occlusion times were significantly longer than 60 minutes, and although the majority of patients utilized partial aortic occlusion, the ER-REBOA catheter that was used in this study was not originally designed to facilitate partial occlusion.64 A Belgian special operations surgical team reported on three successful partial REBOA deployments using the ER-REBOA catheter in combat casualties.65 Current discussions on prehospital REBOA have focused on the feasibility of training prehospital providers and the logistical concerns with performing REBOA in the field.66–69 Large scale studies have not, to date, been performed.
A case report has been published of Zone III REBOA deployment to facilitate intra-hospital transfer to a trauma center to manage severe pelvic fractures.70 An additional case report of a prolonged Zone I partial and intermittent REBOA deployment to manage intra-abdominal hemorrhage from a ruptured renal artery aneurysm yielded a successful outcome.71
Outcomes and Complications
The UK-REBOA trial was a pragmatic randomized multicenter clinical trial conducted in the United Kingdom. 46 patients were randomized to REBOA plus standard care versus 44 receiving standard care alone. Median injury severity score (ISS) was 41 in both groups. The type of catheter used was not specified. At first glance there appeared to be equivalent or increased mortality in the REBOA group (54% vs 42%, OR 1.58 [95% CI 0.72–3.52], with a Bayesian probability of 86.9% of increased probability with REBOA). Death within 6 hours was statistically significantly higher in the REBOA group (OR 3.14 [95% CI 1.13–9.76]) and there were also more deaths due to bleeding in the REBOA group (32% vs 17%). There was no difference in ICU-free days or transfusion requirements, but hospital-free days were increased in the standard group. However, analysis of this trial is a bit more complex. There were some baseline differences between groups, with the REBOA group having more severe head injuries and more hypotension. In the REBOA group, only 19/46 had arterial access, catheter placement and balloon deployment (10 in Zone I, 9 in Zone III). In 8/46 cases, arterial access could not be achieved and in 2/46 cases arterial access was not attempted due to patient deterioration. In the remaining 17 cases, the patient removed with standard resuscitation measures. Time from injury to ED arrival was more than 90 minutes, time from ED arrival to balloon inflation was 32 minutes on average, with a balloon deployment time of 29 minutes and partial REBOA used in 8 patients. Fewer hemorrhage control procedures were performed in the REBOA group (30% vs 43%) and the time to hemorrhage control was 19 minutes longer in the REBOA group. Some challenges with these results include the different patient population and methodology of trauma care in the UK. Levels of penetrating trauma are very low and typically reflect stabbing. Time to hospital is markedly prolonged. Trauma patients are initially cared for by emergency physicians rather than surgeons. This is reflected in the increased time to REBOA deployment and the challenges with arterial access in this study.72 The incomplete use of REBOA in the REBOA arm, the delays to treatment and hemorrhage control, and the higher proportion of head injuries in the REBOA arm may have significantly affected the results.73
The AAST AORTA registry has provided some of the most comprehensive data regarding aortic occlusion therapy. Of note, in a large study of patients receiving complete Zone I aortic occlusion, occlusion times greater than 60 minutes were associated with much higher mortality (73% vs 53% for <15 minute occlusion, 43% for 15–30 minute occlusion, and 45% for 31–60 minute occlusion, p < 0.001) and more vasopressor use (p < 0.001) and multi-organ failure (p = 0.02). After adjusting for injury severity score, systolic blood pressure, and lactate, aortic occlusion greater than 60 minutes had higher odds of mortality (OR 3.7 [95% CI 1.6–9.4, p < 0.001]).74
Data from the AAST AORTA registry has also demonstrated that partial aortic occlusion was performed more frequently with the pREBOA-PRO catheter (n = 155) as compared with the earlier ER-REBOA catheter (n = 800) from the same manufacturer (85.6% vs 11.6%). Duration of aortic occlusion was similar, approximately one hour. Overall injury severity and hemodynamics were similar. pREBOA-PRO patients had a higher initial pH (7.17 vs 7.13, p < 0.001), and slightly more favorable base deficits and lactates (one point lower). Time to hemorrhage control was faster with the pREBOA-PRO (101 ± 74.4 vs 138 ± 147.2 min, p < 0.001). Patients treated with pREBOA-PRO had reduced transfusion of PRBC (13 ± 13.6 vs 18 ± 17.8 units, p < 0.001), FFP (11 ± 12.1 vs 14 ± 15.4, p = 0.038), and platelets (3 ± 3.4 vs 6 ± 11.9 units, p < 0.001), as well as lower crystalloid use (2 ± 2.7 vs 4 ± 4.8 L, p < 0.001). pREBOA-PRO patients had a lower incidence of ARDS (5.8% vs 11.4%, p = 0.027) and septic shock (3.9% vs 9.4%, p = 0.014) but otherwise had similar outcomes. Of note, this is the most detailed description of post-REBOA access site and ischemic complications. Access site complications included an approximately 1.5–2.5% incidence of hematoma, 1–2% incidence of pseudoaneurysm, and 0.3–0.7% incidence of arteriovenous fistula, and were not different between catheters. 3.5% of ER-REBOA patients had distal limb ischemia vs 1.3% of pREBOA-PRO patients (p = NS). ER-REBOA patients also had slightly more distal embolic events (2.8% vs 1.3%, p = NS). 0.7–0.9% of all cases required patch repair. Three ER-REBOA cases required bypass repair versus no pREBOA-PRO cases (p = NS). 9 patients in the ER-REBOA group had a limb amputation event vs zero in the pREBOA-PRO group (p = 0.073).75 A Japanese registry study indicated that sheath size smaller than 8 French appeared to have fewer complications and could be removed with manual compression alone. They reported one femoral artery thrombus and two extremity amputations out of 142 patients; of note in Japan the vast majority of REBOA procedures are performed by emergency medicine physicians due to the health care delivery model in that country.76
The currently ongoing Partial REBOA Outcomes Multicenter ProspecTive (PROMPT) study, of which the authors’ institution is a participant, seeks to compare outcomes, including mortality, acute kidney injury, and transfusion requirements, in partial REBOA deployments with institutional historical control cases performed with complete aortic occlusion.77
Conclusions
Aortic occlusion as a hemorrhage control adjunct has clearly advanced since its initial inception during the Korean War. Currently, it is a viable alternative to resuscitative thoracotomy in some patients, and can assist with avoiding hypotension, providing additional options for workup and hemorrhage control, and improving some outcomes. However, the use of this device is evolving, and there is both a learning curve and the potential for complications. New changes in the technique, including the development of specialized devices that allow for partial aortic occlusion, bear further investigation. Of note, meticulous attention to detail and technique are needed to minimize access site and sheath-related complications, which can potentially be severe. Additional research is needed to better elucidate the ideal patient population for this tool and to better define the changes in outcomes that can result from its use.
Disclosure
KM reports personal fees as consultant for Intuitive Surgical, Inc., and AcuMed Inc., outside the submitted work. He is also the site principal investigator for the PROMPT multicenter observational study of partial REBOA. Funding is provided by the Department of Defense to the site. The authors report no other conflicts of interest in this work.
References
1. Brenner M, Moore L, Dubose J, Scalea T. Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) for use in temporizing intra-abdominal and pelvic hemorrhage: physiologic sequelae and considerations. Shock. 2020;54(5):615–622. doi:10.1097/shk.0000000000001542
2. Hughes CW. Use of an intra-aortic balloon catheter tamponade for controlling intra-abdominal hemorrhage in man. Surgery. 1954;36(1):65–68.
3. Morrison JJ, Morrison JJ, Galgon RE, et al. A systematic review of the use of resuscitative endovascular balloon occlusion of the aorta in the management of hemorrhagic shock. J Trauma Acute Care Surg. 2016;80(2):324–334. doi:10.1097/ta.0000000000000913
4. Inaba K, Alam HB, Brasel KJ, et al. A western trauma association critical decisions algorithm: resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2022;92(4):748–753. doi:10.1097/ta.0000000000003438
5. Bulger EM, Perina DG, Qasim Z, et al. Clinical use of resuscitative endovascular balloon occlusion of the aorta (REBOA) in civilian trauma systems in the USA, 2019: a joint statement from the American college of surgeons committee on trauma, the American college of emergency physicians, the national association of emergency medical services physicians and the national association of emergency medical technicians. Trauma Surg Acute Care Open. 2019;4(1):e000376. doi:10.1136/tsaco-2019-000376
6. Russo RM, Neff LP, Johnson MA, Williams TK. Emerging endovascular therapies for non-compressible torso hemorrhage. SHOCK. 2016;46(3S):12–19. doi:10.1097/shk.0000000000000641
7. Moore LJ, Brenner M, Kozar RA, et al. Implementation of resuscitative endovascular balloon occlusion of the aorta as an alternative to resuscitative thoracotomy for noncompressible truncal hemorrhage. J Trauma Acute Care Surg. 2015;79(4):523–532. doi:10.1097/ta.0000000000000809
8. Brenner M, Teeter W, Hoehn M, et al. Use of resuscitative endovascular balloon occlusion of the aorta for proximal aortic control in patients with severe hemorrhage and arrest. JAMA Surg. 2017;153(2):130. doi:10.1001/jamasurg.2017.3549
9. Brenner M, Moore L, Teeter W, et al. Exclusive clinical experience with a lower profile device for resuscitative endovascular balloon occlusion of the aorta (REBOA). Am J Surg. 2019;217(6):1126–1129. doi:10.1016/j.amjsurg.2018.11.029
10. White JM, Ronaldi AE, Polcz JE, et al. A new pressure-regulated, partial REBOA device achieves targeted distal perfusion. J Surg Res. 2020;256:171–179. doi:10.1016/j.jss.2020.06.042
11. Kemp MT, Wakam GK, Williams AM, et al. A novel partial resuscitative endovascular balloon aortic occlusion device that can be deployed in zone 1 for more than 2 hours with minimal provider titration. J Trauma Acute Care Surg. 2020;90(3):426–433. doi:10.1097/ta.0000000000003042
12. Russo RM, Neff LP, Lamb CM, et al. Partial resuscitative endovascular balloon occlusion of the aorta in swine model of hemorrhagic shock. J Am Coll Surg. 2016;223(2):359–368. doi:10.1016/j.jamcollsurg.2016.04.037
13. Ho JW, Jin G, Nguyen J, et al. Prolonging the zone 1 aortic occlusion time to 4 hours using a partial resuscitative endovascular balloon in a swine model. J Trauma Acute Care Surg. 2023;95(2S):S129–S136. doi:10.1097/ta.0000000000004053
14. Johnson MA, Williams TK, Ferencz SAE, et al. The effect of resuscitative endovascular balloon occlusion of the aorta, partial aortic occlusion and aggressive blood transfusion on traumatic brain injury in a swine multiple injuries model. J Trauma Acute Care Surg. 2017;83(1):61–70. doi:10.1097/ta.0000000000001518
15. Kluck SL, Russo RM, Appel NB, et al. Aortic balloon occlusion in distal zone 3 reduces blood loss from obstetric hemorrhage in placenta accreta spectrum. J Trauma Acute Care Surg. 2023;94(5):710–717. doi:10.1097/ta.0000000000003917
16. Ioffe YJM, Burruss S, Yao R, et al. When the balloon goes up, blood transfusion goes down: a pilot study of REBOA in placenta accreta spectrum disorders. Trauma Surg Acute Care Open. 2021;6(1):e000750. doi:10.1136/tsaco-2021-000750
17. Miura F, Takada T, Ochiai T, et al. Aortic occlusion balloon catheter technique is useful for uncontrollable massive intraabdominal bleeding after hepato-pancreato-biliary surgery. J Gastrointest Surg. 2006;10(4):519–522. doi:10.1016/j.gassur.2005.09.019
18. Sano H, Tsurukiri J, Hoshiai A, Oomura T, Tanaka Y, Ohta S. Resuscitative endovascular balloon occlusion of the aorta for uncontrollable nonvariceal upper gastrointestinal bleeding. World J Emerg Surg. 2016;11(1):20. doi:10.1186/s13017-016-0076-3
19. Williams TK, Neff LP, Johnson MA, et al. Automated variable aortic control versus complete aortic occlusion in a swine model of hemorrhage. J Trauma Acute Care Surg. 2017;82(4):694–703. doi:10.1097/ta.0000000000001372
20. Kuckelman J, Derickson M, Barron M, et al. Efficacy of intermittent versus standard resuscitative endovascular balloon occlusion of the aorta in a lethal solid organ injury model. J Trauma Acute Care Surg. 2019;87(1):9–17. doi:10.1097/ta.0000000000002307
21. Johnson MA, Hoareau GL, Beyer CA, et al. Not ready for prime time: intermittent versus partial resuscitative endovascular balloon occlusion of the aorta for prolonged hemorrhage control in a highly lethal porcine injury model. J Trauma Acute Care Surg. 2019;88(2):298–304. doi:10.1097/ta.0000000000002558
22. Cralley AL, Vigneshwar N, Moore EE, et al. Zone 1 endovascular balloon occlusion of the aorta vs resuscitative thoracotomy for patient resuscitation after severe hemorrhagic shock. JAMA Surg. 2023;158(2):140–150. doi:10.1001/jamasurg.2022.6393
23. Norii T, Crandall C, Terasaka Y. Survival of severe blunt trauma patients treated with resuscitative endovascular balloon occlusion of the aorta compared with propensity score‐adjusted untreated patients. J Trauma Acute Care Surg. 2015;78(4):721–728. doi:10.1097/ta.0000000000000578
24. Joseph B, Zeeshan M, Sakran JV, et al. Nationwide Analysis of Resuscitative Endovascular Balloon Occlusion of the Aorta in Civilian Trauma. JAMA Surg. 2019;154(6):500–508. doi:10.1001/jamasurg.2019.0096
25. Stannard A, Eliason JL, Rasmussen TE. Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) as an adjunct for hemorrhagic shock. J Trauma Inj Infect Crit Care. 2011;71(6):1869–1872. doi:10.1097/ta.0b013e31823fe90c
26. Shaw J, Brenner M. Resuscitative balloon occlusion of the aorta in the modern era: expanding indications, optimal techniques, unresolved issues, and current results. Semin Vasc Surg. 2023;36(2):250–257. doi:10.1053/j.semvascsurg.2023.04.005
27. Romagnoli AN, Teeter W, Wasicek P, et al. No wire? No problem. J Trauma Acute Care Surg. 2018;85(5):894–898. doi:10.1097/ta.0000000000002003
28. Qasim ZA, Sikorski RA. Physiologic considerations in trauma patients undergoing resuscitative endovascular balloon occlusion of the aorta. Anesthesia Analg. 2017;125(3):891–894. doi:10.1213/ane.0000000000002215
29. Tibbits EM, Hoareau GL, Simon MA, et al. Location is everything. J Trauma Acute Care Surg. 2018;85(1):101–107. doi:10.1097/ta.0000000000001858
30. Deser SB, Arapi B, Ustunisik CT, Bitargil M, Yuksel A. REBOA improves outcomes in hybrid surgery for ruptured abdominal aortic aneurysms. Ann Vasc Surg. 2024;100:8–14. doi:10.1016/j.avsg.2023.10.027
31. Beyer CA, Johnson MA, Galante JM, DuBose JJ. Zones matter: hemodynamic effects of zone 1 vs zone 3 resuscitative endovascular balloon occlusion of the aorta placement in trauma patients. Injury. 2019;50(4):855–858. doi:10.1016/j.injury.2019.03.013
32. Tang X, Guo W, Yang R, Tang S, Dong S. Use of aortic balloon occlusion to decrease blood loss during sacral tumor resection. J Bone Jt Surg. 2010;92(8):1747–1753. doi:10.2106/jbjs.i.01333
33. Brenner M, Inaba K, Aiolfi A, et al. Resuscitative endovascular balloon occlusion of the aorta and resuscitative thoracotomy in select patients with hemorrhagic shock: early results from the American association for the surgery of trauma’s aortic occlusion in resuscitation for trauma and acute care surgery registry. J Am Coll Surg. 2018;226(5):730–740. doi:10.1016/j.jamcollsurg.2018.01.044
34. Koh EY, Fox EE, Wade CE, et al. Resuscitative endovascular balloon occlusion of the aorta and resuscitative thoracotomy are associated with similar outcomes in traumatic cardiac arrest. J Trauma Acute Care Surg. 2023;95(6):912–917. doi:10.1097/ta.0000000000004094
35. Brenner M, Zakhary B, Coimbra R, et al. Resuscitative endovascular balloon occlusion of the aorta (REBOA) may be superior to resuscitative thoracotomy (RT) in patients with traumatic brain injury (TBI). Trauma Surg Acute Care Open. 2022;7(1):e000715. doi:10.1136/tsaco-2021-000715
36. Yamamoto R, Cestero RF, Muir MT, et al. Delays in surgical intervention and temporary hemostasis using Resuscitative Endovascular Balloon Occlusion of the aorta (REBOA): influence of time to operating room on mortality. Am J Surg. 2020;220(6):1485–1491. doi:10.1016/j.amjsurg.2020.07.017
37. Smith MC, Medvecz AJ, Smith MR, Streams JR, Dennis BM. Computed tomography scanning is feasible in select patients with REBOA catheter deployment. Injury. 2024;55(5):111387. doi:10.1016/j.injury.2024.111387
38. Hatchimonji JS, Chipman AM, McGreevy DT, et al. REBOA use in nontrauma emergency general surgery: a multi-institutional experience. J Surg Res. 2020;256:149–155. doi:10.1016/j.jss.2020.06.034
39. Davidson AJ, Russo RM, Reva VA, et al. The pitfalls of resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2018;84(1):192–202. doi:10.1097/ta.0000000000001711
40. Hamed M, Thakker R, Elkheshen A, et al. Meta-analysis on ultrasound guidance for femoral vascular access. Am J Cardiol. 2023;192:98–100. doi:10.1016/j.amjcard.2023.01.031
41. Romagnoli A, Teeter W, Pasley J, et al. Time to aortic occlusion. J Trauma Acute Care Surg. 2017;83(6):1161–1164. doi:10.1097/ta.0000000000001665
42. Matsumura Y, Matsumoto J, Kondo H, et al. Early arterial access for resuscitative endovascular balloon occlusion of the aorta is related to survival outcome in trauma. J Trauma Acute Care Surg. 2018;85(3):507–511. doi:10.1097/ta.0000000000002004
43. Linnebur M, Inaba K, Haltmeier T, et al. Emergent non–image-guided resuscitative endovascular balloon occlusion of the aorta (REBOA) catheter placement. J Trauma Acute Care Surg. 2016;81(3):453–457. doi:10.1097/ta.0000000000001106
44. Eliason JL, Derstine BA, Horbal SR, et al. CT correlation of skeletal landmarks and vascular anatomy in civilian adult trauma patients. J Trauma Acute Care Surg. 2019;87(1S):S138–S145. doi:10.1097/ta.0000000000002247 Publish Ahead of Print(NA;):NA.
45. Pezy P, Flaris AN, Prat NJ, et al. Fixed-distance model for balloon placement during fluoroscopy-free resuscitative endovascular balloon occlusion of the aorta in a civilian population. JAMA Surg. 2016;152(4):351. doi:10.1001/jamasurg.2016.4757
46. Matsumoto S, Funabiki T, Kazamaki T, et al. Placement accuracy of resuscitative endovascular occlusion balloon into the target zone with external measurement. Trauma Surg Acute Care Open. 2020;5(1):e000443. doi:10.1136/tsaco-2020-000443
47. Meyer DE, Mont MT, Harvin JA, Kao LS, Wade CE, Moore LJ. Catheter distances and balloon inflation volumes for the ER-REBOATM catheter: a prospective analysis. Am J Surg. 2020;219(1):140–144. doi:10.1016/j.amjsurg.2019.04.019
48. Wasicek PJ, Teeter WA, Brenner ML, Hoehn MR, Scalea TM, Morrison JJ. Resuscitative endovascular balloon occlusion of the aorta: rupture risk and implications for blind inflation. Trauma Surg Acute Care Open. 2018;3(1):e000141. doi:10.1136/tsaco-2017-000141
49. Brenner M, Hoehn M, Pasley J, Dubose J, Stein D, Scalea T. Basic endovascular skills for trauma course. J Trauma Acute Care Surg. 2014;77(2):286–291. doi:10.1097/ta.0000000000000310
50. Wasicek PJ, Teeter WA, Yang S, et al. Extended resuscitative endovascular balloon occlusion of the aorta (REBOA)-induced type 2 myocardial ischemia: a time-dependent penalty. Trauma Surg Acute Care Open. 2019;4(1):e000194. doi:10.1136/tsaco-2018-000194
51. Qadri HI, Patel NT, Ganapathy AS, et al. Maintaining zone 1 occlusion is a dynamic process: the effects of proximal pressure and blood transfusion during REBOA. Am Surg. 2022;88(7):1496–1503. doi:10.1177/00031348221082284
52. Morrison JJ, Ross JD, Markov NP, Scott DJ, Spencer JR, Rasmussen TE. The inflammatory sequelae of aortic balloon occlusion in hemorrhagic shock. J Surg Res. 2014;191(2):423–431. doi:10.1016/j.jss.2014.04.012
53. Hoehn MR, Teeter WA, Morrison JJ, et al. Aortic branch vessel flow during resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2019;86(1):79–85. doi:10.1097/ta.0000000000002075
54. Davidson AJ, Russo RM, Ferencz SAE, et al. Incremental balloon deflation following complete resuscitative endovascular balloon occlusion of the aorta results in steep inflection of flow and rapid reperfusion in a large animal model of hemorrhagic shock. J Trauma Acute Care Surg. 2017;83(1):139–143. doi:10.1097/ta.0000000000001502
55. Laverty RB, Treffalls RN, McEntire SE, et al. Life over limb: arterial access-related limb ischemic complications in 48-hour REBOA survivors. J Trauma Acute Care Surg. 2022;92(4):723–728. doi:10.1097/ta.0000000000003440
56. Teeter WA, Matsumoto J, Idoguchi K, et al. Smaller introducer sheaths for REBOA may be associated with fewer complications. J Trauma Acute Care Surg. 2016;81(6):1039–1045. doi:10.1097/ta.0000000000001143
57. Treffalls RN, Scheidt J, Lee C, et al. Arterial access complications following percutaneous femoral access in 24-hour resuscitative endovascular balloon occlusion of the aorta survivors. J Surg Res. 2023;290:203–208. doi:10.1016/j.jss.2023.05.004
58. Zakaluzny SA, Beldowicz BC, Salcedo ES, DuBose JJ, Moore LJ, Brenner M. Guidelines for a system-wide multidisciplinary approach to institutional resuscitative endovascular balloon occlusion of the aorta implementation. J Trauma Acute Care Surg. 2019;86(2):337–343. doi:10.1097/ta.0000000000002138
59. Theodorou CM, Anderson JE, Brenner M, et al. Practice, practice, practice! Effect of resuscitative endovascular balloon occlusion of the aorta volume on outcomes: data from the AAST AORTA registry. J Surg Res. 2020;253:18–25. doi:10.1016/j.jss.2020.03.027
60. Henry R, Matsushima K, Henry RN, et al. Who would have benefited from the prehospital use of Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA)? An autopsy study. J Am Coll Surg. 2019;229(4):383–388.e1. doi:10.1016/j.jamcollsurg.2019.05.025
61. Russo RM, Williams TK, Grayson JK, et al. Extending the golden hour. J Trauma Acute Care Surg. 2016;80(3):372–380. doi:10.1097/ta.0000000000000940
62. Paran M, McGreevy D, Hörer TM, et al. International registry on aortic balloon occlusion in major trauma: partial inflation does not improve outcomes in abdominal trauma. Surg. 2024;22(1):37–42. doi:10.1016/j.surge.2023.08.001
63. Hunt I, Gold L, Hunt JP, et al. Acute kidney injury in hypotensive trauma patients following resuscitative endovascular balloon occlusion of the aorta placement. Am Surg. 2023;89(8):3454–3459. doi:10.1177/00031348231157894
64. Lendrum RA, Perkins Z, Marsden M, et al. Prehospital partial resuscitative endovascular balloon occlusion of the aorta for exsanguinating subdiaphragmatic hemorrhage. JAMA Surg. 2024;159(9). doi:10.1001/jamasurg.2024.2254
65. Schoutheete JC, de Fourneau I, Waroquier F, et al. Three cases of resuscitative endovascular balloon occlusion of the aorta (REBOA) in austere pre-hospital environment—technical and methodological aspects. World J Emerg Surg. 2018;13(1):54. doi:10.1186/s13017-018-0213-2
66. Smith SA, Hilsden R, Beckett A, McAlister VC. The future of resuscitative endovascular balloon occlusion in combat operations. J R Army Méd Corps. 2017;163(5):296. doi:10.1136/jramc-2017-000788
67. Ross EM, Redman TT. Feasibility and proposed training pathway for austere application of resuscitative balloon occlusion of the aorta. J Spéc Oper Med. 2018;18(1):37. doi:10.55460/qb5t-9jaq
68. Thabouillot O, Jouffroy R, Jost D, et al. REBOA use in a medicalized prehospital setting: proposal for a first protocol based on the delphi method. J Spéc Oper Med. 2024. doi:10.55460/kr4w-7ekm
69. Adams D, McDonald PL, Holland S, et al. Management of non-compressible torso hemorrhage of the abdomen in civilian and military austere environments: a scoping review. Trauma Surg Acute Care Open. 2024;9(1):e001189. doi:10.1136/tsaco-2023-001189
70. Lin NS, Wu IL, Li PL, Jiang YX, Lin YY. Resuscitative endovascular balloon occlusion of the aorta (REBOA) successfully used in interhospital transport. Heliyon. 2024;10(3):e24525. doi:10.1016/j.heliyon.2024.e24525
71. Ando H, Kaszynski RH, Goto H. On-site placement of resuscitative endovascular balloon occlusion of the aorta (REBOA) in a hemorrhagic shock patient: a successful endeavor involving long-distance air transport. Am J Emerg Med. 2022;55:227.e1–227.e3. doi:10.1016/j.ajem.2021.12.055
72. Jansen JO, Hudson J, Cochran C, et al. Emergency department resuscitative endovascular balloon occlusion of the aorta in trauma patients with exsanguinating hemorrhage. JAMA. 2023;330(19):1862–1871. doi:10.1001/jama.2023.20850
73. Cotton BA. Delays in intervention: a post-mortem of the UK-REBOA and CRYOSTAT-2 trials. Br J Surg. 2024;111(2):znae031. doi:10.1093/bjs/znae031
74. Treffalls RN, DuBose JJ, Brenner M, et al. Outcomes associated with aortic balloon occlusion time in patients with zone 1 resuscitative endovascular balloon occlusion of the aorta. J Surg Res. 2024;296:256–264. doi:10.1016/j.jss.2023.12.044
75. Meyer CH, Beckett A, Dennis BM, et al. pREBOA vs ER-REBOA impact on blood utilization and resuscitation requirements: a pilot analysis. J Trauma Acute Care Surg. 2024. doi:10.1097/ta.0000000000004391
76. Matsumura Y, Matsumoto J, Kondo H, et al. Fewer REBOA complications with smaller devices and partial occlusion: evidence from a multicentre registry in Japan. Emerg Med J. 2017;34(12):793. doi:10.1136/emermed-2016-206383
77. Gondek S, Hamblin S, Raley J, et al. A PROMPT update on partial REBOA: initial clinical data and overview of the dod-funded Partial REBOA outcomes multicenter prospective (PROMPT) study. Mil Med. 2024;189((Supplement_3)):284–290. doi:10.1093/milmed/usae095
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.