")
Back to Journals » Journal of Inflammation Research » Volume 17
Jin-Gu-Lian Capsule Did Not Significantly Improve Clinical Value in Rheumatoid Arthritis Therapy: A Real-World Study
Authors Chen Y, He M , Zhao SJ , Chen YJ, Zhang YQ, Chen XL, Yang CJ, Luo YZ, Nandakumar KS , Xing ZX, Tian M
Received 19 June 2024
Accepted for publication 10 August 2024
Published 17 August 2024 Volume 2024:17 Pages 5509—5519
DOI https://doi.org/10.2147/JIR.S468880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yong Chen,1 Mang He,1 Si-Jin Zhao,2 Yan-Juan Chen,1 Yong-Qiao Zhang,2 Xiao-Long Chen,2 Chuan-Jie Yang,2 Yu-Zhuo Luo,2 Kutty Selva Nandakumar,3 Zhou-Xiong Xing,4 Mei Tian1
1Department of Rheumatology and Immunology, Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, People’s Republic of China; 2Undergraduate Students of Zunyi Medical University, Zunyi, Guizhou, People’s Republic of China; 3Docent, Department of Medical Biochemistry and Biophysics, Karolinska Institute, Stockholm, Sweden; 4Department of Critical Care Medicine, Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, People’s Republic of China
Correspondence: Mei Tian; Zhou-Xiong Xing, Affiliated Hospital of Zunyi Medical University, 149 Dalian Road, Huichuan District, Zunyi City, Guizhou Province, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To investigate the clinical value of adding Jin-gu-lian (JGL) capsules into rheumatoid arthritis (RA) treatment by examining its impact on disease activity and quality of life (QoL) through a real-world study (RWS).
Patients and methods: RWS was conducted to compare the inflammatory markers, including IgM-RF, ESR, and CRP, between RA patients treated with only Western medicine (reference group) and Western medicine plus JGL (study group) during one-year follow-up. The clinical data was acquired from the hospital information system (HIS). Telephone call-based follow-up on QoL (SF-36) and accompanying symptoms, including gastrointestinal complaints, attacks of pneumonia, herpes zoster, URTIs, UTIs, and LTBIs. Finally, the anti-rheumatic drugs given to both groups were also compared. RWS was further validated for its feasibility by performing studies with hydroxychloroquine (HCQ) treatment, which is a commonly used anti-rheumatic drug for RA with mild effect.
Results: The study group failed to show a significant effect on inflammatory markers, especially on the CRP levels, indicating no additional clinical value of supplementing with JGL. Similarly, at the endpoint, no significant differences between the two groups on QoL and related symptoms were observed. Our study suggests that the patients in the study group might need more anti-rheumatic drugs to fill the treatment insufficiency, and the application ratio of NSAIDs would be significantly higher than the reference group. By conducting this study on HCQ treatment, the positive aspects of controlling disease activity and reducing NSAIDs application were found, which demonstrates the utility of performing the RWS to evaluate the effect of JGL.
Conclusion: Adding JGL did not significantly improve the clinical efficacy of RA treatment by this RWS. Folk herbal prescriptions such as JGL are suggested to underwent strict clinical trials before application.
Keywords: real-world study, rheumatoid arthritis, traditional Chinese medicine, disease activity, hydroxychloroquine
Introduction
Rheumatoid arthritis (RA) is one of the most common chronic autoimmune diseases affecting bone and cartilage by not only causing deformation but also accompanied with wide spread systemic complications such as anemia, interstitial lung disease, arteriosclerosis, etc.1 Traditional Chinese medicine or herbal medicine has been reported to be one of the possible complementary methods in the management of RA.2,3 However, most of the in vitro and animal experiments conducted were focused on basic research, and the clinical observations were not sufficiently conducted.
Different from the other reported compatibility of herbal medicines, single Chinese medicine or its active components that under exploring in RA treatment, the Jin-gu-lian (JGL) capsule is included in the Compilation of National Standard for Traditional Chinese Medicines (2002 edition)4 and has been approved as the counter (OTC) medicine, covered by governmental health insurance for decades in China. Publications show its potential therapeutic mechanisms in RA through network pharmacology and animal experiment approaches.4 A few clinical studies were reported,5 but the use of JGL by classic folk prescriptions has not undergone a strict clinical trial.
Recently, we have performed a retrospective study to analyze the clinical effectiveness of JGL in RA patients through a real-world study (RWS). Patients’ diseases activity indicated by rheumatoid factor (IgM-RF) levels, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) in their last year of treatment were collected, and quality of life (QoL) was assessed by following up based on 36-Item Short-Form Health Survey (SF-36). Besides, anti-rheumatic drugs applied and incidence of gastrointestinal (GI) symptoms and infections between the reference and the study groups were also compared. It was hypothesized that adding JGL to regular western medical treatment might benefit RA patients with better results in controlling disease activity or improving QoL.
Methods
Patient Selection
We selected patients based on the information recorded in the hospital information system (HIS). Patients who visited the rheumatology and immunology outpatient department of Zunyi Medical University from Aug. 2021 to Aug. 2022, diagnosed with RA based on ACR/EULAR 2010 classification criteria were recruited.6 Patients with visits less than three times in the one-year study period were excluded. This retrospective trial was approved by the Ethics Committee of the Affiliated Hospital of Zunyi Medical University (KLL-2023-545). All procedures performed in the studies were in accordance with the ethical standards of the institutional and national research committee and followed the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Patients gave their informed consent to participate in this study protocol.
Experimental Groups
In total, 1032 RA patients, who gave oral consent to participate in this investigation, were selected, including 483 cases receiving only Western medicine (reference group), and 549 cases receiving JGL and Western medicine (study group). Furthermore, hydroxychloroquine (HCQ), a mild conventionally synthesized disease-modifying anti-rheumatic drugs (csDMARDs) for RA treatment,7 was chosen to repeat the study as a methodological justification to validate whether this RWS protocol was applicable or not.
Collection of Disease Activity Parameters
Laboratory test results (IgM-RF levels, ESR, and CRP) recorded in HIS were used to evaluate disease activity.8 Successive patient data were recorded with baseline, within three months (m), 3–6 m, 6–9 m, and 9–12 m. If a patient visited more than once during one of these defined periods, a lower value would be put into our data for analysis.
Telephone Call Based Following Up on QoL
QoL of all RA patients recruited was assessed using the 36-Item Short-Form Health Survey (SF-36).9 SF-36 survey was followed up by telephone calls to inquire about the current health conditions of patients. Besides, the attacks of pneumonia, herpes zoster, upper respiratory tract infections (URTIs), urinary tract infections (UTIs), and gastrointestinal (GI) symptoms in their last year of treatment were also inquired (Supplementary Data S1). Oral consent to participate in the interview was provided by the investigated patients. All the patients underwent chest high-resolution computed tomography (HRCT), and the complications of pulmonary tuberculosis (latent or active) were recorded from HIS.
Drugs Used for Treatment
It is difficult to accurately figure out the drugs received, courses, and dosages of each drug given to patients. This is mainly because patients cannot recall clearly, while HIS does not include patients’ information about visiting other hospitals. So the investigators recorded all the anti-rheumatic drugs prescribed in one whole year for every patient, including glucocorticoids (GCs), nonsteroidal anti-inflammatory drugs (NSAIDs), conventionally synthesized disease-modifying antirheumatic drugs (csDMARDs), JAK inhibitors (JAKi), TNF inhibitors (TNFi) and Jin-gu-lian Capsules (JGL).
Statistical Analysis
Statistical analysis was performed using the GraphPad Prism 9 software. The measurement data of the normal distribution were expressed as mean ± SD, and an independent sample t-test was used to compare the two groups. Measurement data of non-normal distribution were expressed as mean (Q2, Q4) in tables and mean with 95% CI in figures, and the Mann–Whitney U-test was used to compare two groups. The missing data were deleted because they constituted a small proportion. The counting data were analyzed by using a chi-square (or Fisher’s exact) test based on the sample numbers. Significance was set at p < 0.05.
Results
Demographic Features and Baseline Disease Activity Levels
The gender distribution and disease course in the reference and study groups had no significant differences. However, the patients in the study group were 2.08 years older than the reference group (p < 0.001). The titer of IgM-RF in the study group was higher than the reference group (p < 0.05), the ESR and CRP levels were without any significant differences (Table 1). Besides as a diagnostic marker, RF titer is also associated with disease activity in RA.10 The baseline differences of RF titer may potentially implicate effectiveness assessment of JGL. Thus, stratification analysis of the two groups was conducted, and it turned out patients with RF titer above 300 IU/mL in the Study group were significantly higher than that of Reference group (Supplementary Table 1 and Supplementary Figure 1 in Supplementary Data S2). Cases with RF titer between 300 and 900 IU/mL (n=7) and above 900 IU/mL (n=21) were randomly chosen for rejection. The adjusted cases in the two groups showed no additional statistical differences in RF titer (Supplementary Figure 2 in Supplementary Data S2). The following research on effectiveness indicated by RF titer were addressed by adjusted cases.
 |
Table 1 Baseline Features of the Reference and Study Groups |
Subjective Feedbacks from the Patients
Based on the questionnaires (Supplementary Data S1), the question “Are you following the doctor’s advice?” could be considered as patients’ compliance with the treatment. Surprisingly, compliance in the reference group was better than the study group (p < 0.05, Figure 1A). However, for the data set with adjusted RF levels, the patients showed no significant differences on compliance between the two groups (Figure 1B). The subjective feedback from the patients on overall satisfaction level to treatment and recovery level was similar between the two groups (Figure 1C and D).
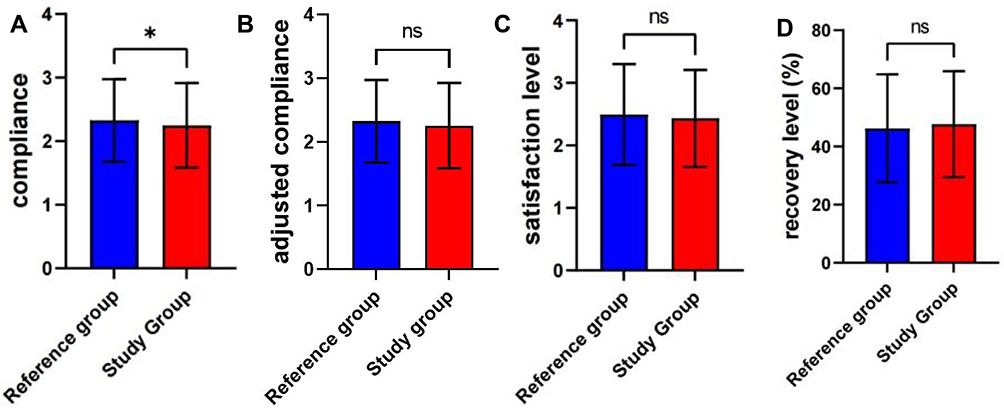 |
Figure 1 Subjective feedback from the patients. (A and B) Patients’ compliance in the reference group (n = 483) was higher than the study group (n = 549), but the difference gone with adjusted cases in the study group (n=521). (C and D) The satisfaction level and the recovery level were similar between the two groups. Abbreviation: ns, no significance. Note: *P < 0.05; |
IgM-RF Levels
The IgM-RF levels, which were proposed as a disease activity index in the reference and study groups (with cases adjusted for baseline consistency), were significantly decreased during the one-year treatment, but during follow-up, no significant differences were observed (Figure 2A). A total of 86 (reference) and 134 (study) cases were used to analyze the RF levels in the follow-up period (Figure 2B). At the baseline, RF levels in the study group were higher than those in the reference group. However, there was no evidence to show better or worse performance of the study group compared to the reference group (Figure 2C).
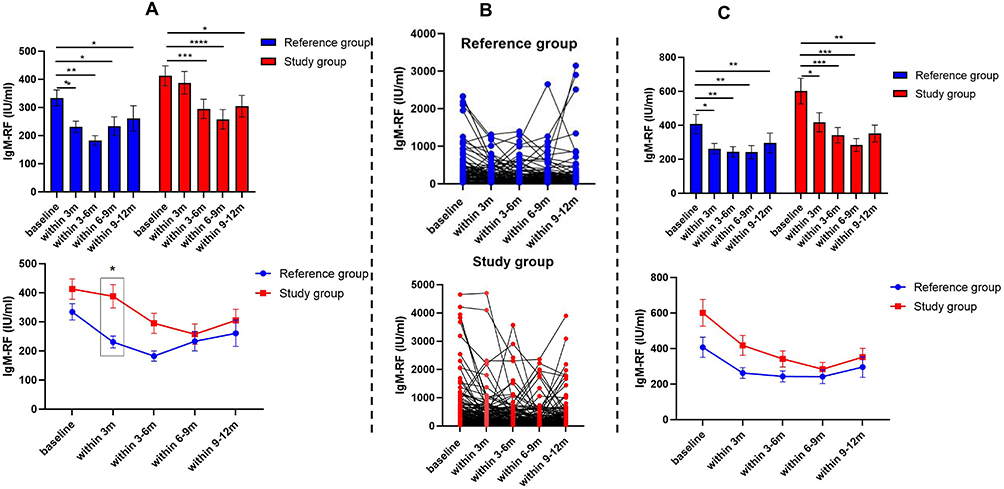 |
Figure 2 The IgM-RF levels of the reference and the study groups (with cases adjusted for baseline consistency) in the one-year follow-up. (A) Data of all patients showed a significant decrease of IgM-RF levels in each group; (B and C) Patients with RF results of all five consecutive time nodes in each group (n = 86 in the reference group, and n = 134 in the study group). Abbreviation: IgM-RF, Rheumatoid factor. Notes: *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001. |
ESR Levels
ESR is most commonly applied as inflammatory level index and is also used in evaluating the effectiveness of treatment for RA.11 Similar to the IgM-RF levels in the reference and the study groups, ESR levels were significantly decreased during one-year treatment in both the groups. However, the reference group showed lower levels of ESR from 3 to 12 m (Figure 3A). A total of 113 (reference) and 153 (study) cases with ESR results of all five consecutive time nodes were used (Figure 3B), but no significant differences between the groups at the five time nodes were found during the one-year follow-up (Figure 3C).
 |
Figure 3 The ESR levels of the reference and the study groups in the one-year follow-up. (A) Both the reference and the study groups showed a significant decrease in ESR levels within one year following up, and at time points of 3–6 m and 9–12 m, the ESR levels in the reference group were lower than the study groups; (B and C) For the patients with ESR results of all five consecutive time nodes in each group showed no significant differences (n = 113 in the reference group, and n = 153 in the study group). Abbreviation: ESR, Erythrocyte sedimentation rate. Notes: *P < 0.05; **P < 0.01; ***p < 0.001; ****P < 0.0001. |
CRP Levels
As an acute-phase plasma protein and a component of the acute-phase response, CRP is routinely assessed as a marker of systemic inflammation in RA.12,13 Similar to the ESR levels in the reference and the study groups, CRP levels were all significantly decreased during the one-year treatment, and the reference group showed lower levels of ESR in 3–6m (Figure 4A). A total of 93 (reference) and 143 (study) cases with CRP results of all five consecutive time nodes were used (Figure 4B). Although the reference group had lower CRP levels within one-year follow-up, it is challenging to conclude which group was better controlled than the other because of differences in the baseline CRP levels (Figure 4C).
 |
Figure 4 The reference and the study groups’ CRP levels in the one-year follow-up. (A) Both the reference and the study groups showed a significant decrease in ESR levels within one year following up, and at time points of 3–6m, the CRP levels in the reference group were lower than the study groups (B and C) For the patients with CRP results of all five consecutive time nodes in each group showed the study group always higher than the reference group (n = 93 in the reference group, and n = 143 in the study group). Abbreviation: CRP, C-reactive protein. Notes: *P < 0.05; **P<0.01; ***P < 0.001; ****P<0.0001. |
Comparison of QoL
SF-36 is one of global measures of health-related QoL.14 Patients in the study group showed better outcomes in body pain, mental health, vitality, and social functioning, while comparing the QoL with SF-36. The overall scores between the reference and study groups were without any significant differences (Table 2).
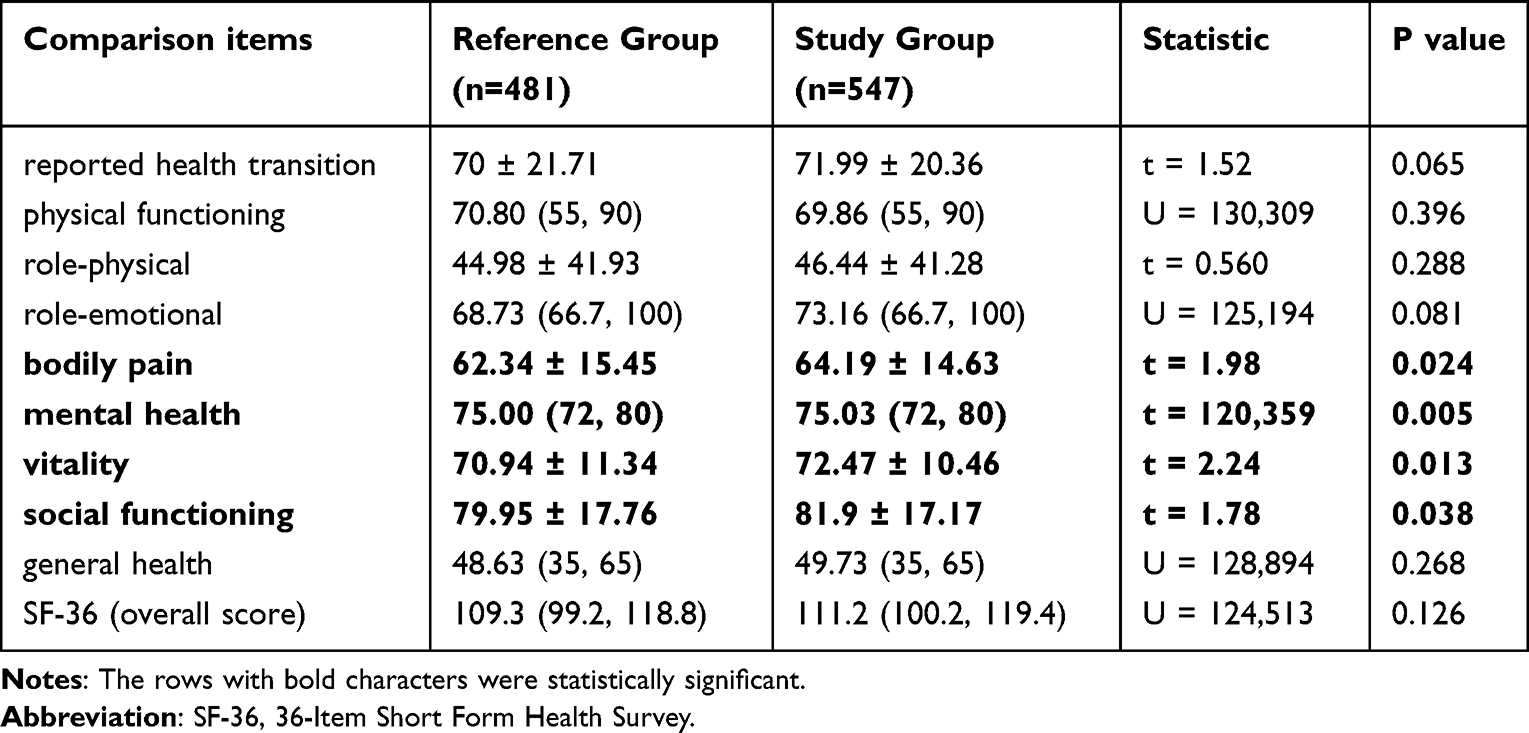 |
Table 2 Comparison of SF-36 Between the Reference and the Study Groups |
Incidence of GI Symptoms, Infections
The complications of GI symptoms and attacks of pneumonia, herpes zoster, URTIs, UTIs, and LTBIs were without any significant differences between the reference and the study groups (Table 3).
 |
Table 3 Incidence of GI Symptoms and Infections Between the Reference and the Study Groups |
Application of Anti-Rheumatic Drugs
The available anti-rheumatic medicines for RA patients in this institution were GCs, NSAIDs, csDMARDs, JAKi, and TNFi. The most often used csDMARDs for RA patients include methotrexate (MTX), leflunomide (LEF), hydroxychloroquine (HCQ), salazosulfapyridine (SASP), iguratimod (IGU), and glucosidorum tripterygll totorum (GTW). The application of types of anti-rheumatic drugs in the reference group was 3.44 (2, 4) per patient in the last year, which was significantly less than the study group value: 3.77 (3, 5) (excluding JGL) (Figure 5A). The most frequently used drug was MTX, followed by LEF and NSAIDs. The application of NSAIDs, LEF, and JAKi were significantly higher in the study group, and GC use was slightly higher but without any statistical significance (Figure 5B and Table 4). The application of csDMARDs had no significant difference between the two groups (Figure 5C).
 |
Table 4 The Difference Between Anti-Rheumatic Drugs Applied in the Reference and the Study Groups |
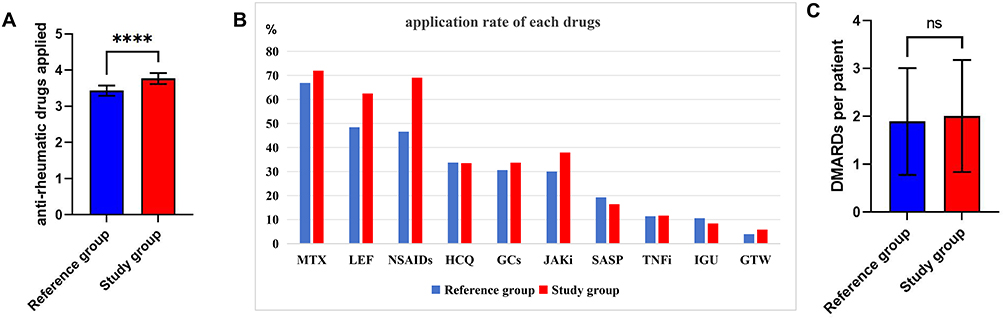 |
Figure 5 The anti-rheumatic drugs applied in the reference and the study groups. (A) The kinds of anti-rheumatic medications applied in the patients of the study group (n = 483) were significantly more than the reference group (n = 549) patients; (B) The application rates of the anti-rheumatic drugs used in the reference and the study groups; (C) No significant differences of csDMARDs per patient between the reference and the study groups. Abbreviations: ns, no significant, MTX, methotrexate; LEF, Leflunomide; NSAID, non-steroidal anti-inflammatory drug; HCQ, hydroxychloroquine; GC, glucocorticoid; JAKi, JAK inhibitors; SASP, Salazosulfapyridine; TNFi: TNF inhibitors; IGU, iguratimod; GTW, glucosidorum tripterygll totorum. Notes: ****P < 0.0001; |
Validation of the Research methods
The csDMARD of HCQ was chosen to repeat the above study to validate whether this real-world study protocol was applicable or not. The RA patients were divided into two groups: without HCQ (n = 718) and with HCQ (n = 360) based on whether they received HCQ in their therapeutic regimen during one-year treatment.
The IgM-RF levels in the HCQ-treated patients were significantly higher than the patients without HCQ treatment at most of the time and showed a pair of parallel lines in the graph (Figure 6A). Although, at baseline, the ESR levels in HCQ-treated patients were significantly higher than the HCQ untreated patients, but it went gradually to similar levels after 6m of treatment (Figure 6B). The CRP levels in patients with HCQ treatment were decreasing faster (Figure 6C). RA patients treated with HCQ received other anti-rheumatic drugs similar to HCQ untreated patients, but with a significantly lower application ratio of NSAIDs (Figure 6D and Table 5).
 |
Table 5 The Difference in Application of NSAIDs Ratio in the Patients with HCQ Group and Those Without |
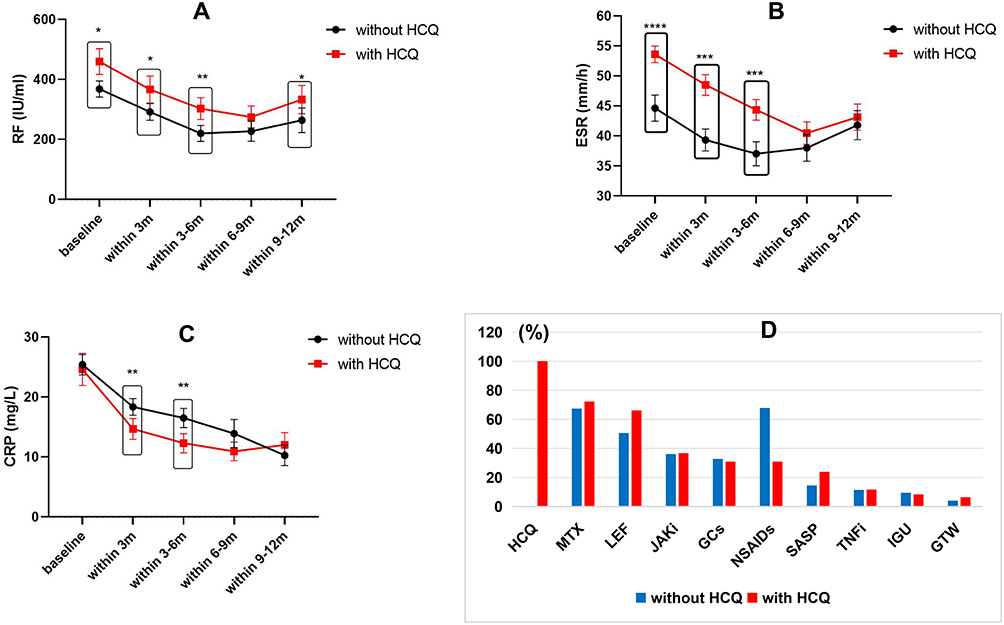 |
Figure 6 Validation of the research protocol by investing HCQ. (A-C) RA patients treated with HCQ (n = 568) in their regimens seem better at decreasing inflammatory markers of ESR and CRP than those without (n = 296); (D) The anti-rheumatic drugs applied in the patients with HCQ group and the without. Abbreviations: MTX, methotrexate; LEF, Leflunomide; NSAID, non-steroidal anti-inflammatory drug; HCQ, hydroxychloroquine; GC, glucocorticoid; JAKi, JAK inhibitors; SASP, Salazosulfapyridine; TNFi: TNF inhibitors; IGU, iguratimod; GTW, glucosidorum tripterygll totorum. Notes: *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001. |
Discussion
Besides investigating the protective effect on RA by inhibiting inflammation via the IL-17/NF-κB pathway, JGL also showed the impact against neurotoxicity via modulating oxidative stress, preventing abnormality of neurotransmitters, and modulating pharmacokinetics such as reducing the expression of cytochrome P450 enzymes.15 As an OTC-approved drug, the functions of JGL are to treat conditions like limited movement, joint swelling, and pain by expelling wind, and eliminating dampness (wind and dampness are pathogenic factors in traditional Chinese medicine theory16,17), reducing swelling, and relieving pain. However, its clinical effect has not been strictly verified. In China, Phase III clinical studies may not be needed to confirm the efficacy of a classic folk prescription such as JGL. These recipes are usually the result of a long period of clinical practice and experience, and are believed to be effective in treating specific symptoms or diseases in some cases. However, conducting Phase III clinical studies is a standard practice to verify the safety and effectiveness of a drug or treatment.18 Therefore, even if some folk classic recipes are widely used in practice, more rigorous scientific studies may be needed to confirm their efficacy and safety.
In this RWS, it was hypothesized that adding JGL to regular Western medical treatment might benefit RA patients with better results in controlling the disease activity or improving QoL. However, the results were not satisfactory. At baseline, the patients in the reference and study groups had a difference in age and IgM-RF levels, the level of inflammation markers ESR and CRP showed no significant differences. In this RWS, the data reflected a general phenomenon that Traditional Chinese Medicine (TCM) tends to be more popular among older generations compared to younger people.19 However, age is considered to be one of the factors that affects disease activity and treatment outcome.20 Thus, the rejection part of the cases in the study group based on the results of stratification analysis was applied and generated baseline consistency of RF levels. Within one year of treatment, the patients taking Western medicine plus JGL (study group) showed higher levels of ESR and CRP in 3–6m, indicates the addition of JGL might not be beneficial for controlling the disease development.
The study group showed lower levels of compliance level than the reference group. The cause and effect of the compliance and treatment outcome are unclear. It is assumed that non-adherence to treatment would be detrimental in the majority of rheumatic patients.21 But inferior effectiveness may also lead to poor compliance. Interestingly, by adjusting cases with IgM-RF consistency, the compliance showed no further difference between the two groups. This confirmed that patients’ compliance was associated with treatment effectiveness.
Adding JGL to the treatment was hypothesized to reduce the application of GCs or immunosuppressors, and contribute to the patient’s management. However, as we recorded every patient’s treatment drugs in one year, we found a need for more anti-rheumatic drugs and NSAIDs for the patients in the study group. In addition, they need to switch between different drugs due to the uncontrolled pain suggesting the drug survival rate in the study group might be lower than the reference group. The drug survival rate is a crucial metric for evaluating its long-term treatment effects. A higher drug survival rate is considered beneficial during long-term disease management, effectively controlling the activity of the disease and maintaining a steady remission of the condition.22
However, due to a lack of baseline data, the results were not promising because adding JGL did not decrease complications such as GI symptoms and attacks of pneumonia, herpes zoster, URTIs, UTIs, and LTBIs. For QoL, the JGL-treated group showed better performance regarding body pain, mental health, vitality, and social functioning. However, the overall score of SF-36 showed no significant difference.
RWS, also known as real-world evidence study, is an observational study conducted in real-world settings to evaluate the effectiveness, safety, and outcome of medical interventions in a diverse patient population RWS offers valuable insights to help inform clinical decision-making, healthcare policy-making, and regulatory decisions. It is important to note that real-world studies are observational and are subject to various potential sources of bias, such as patient selection bias, treatment selection bias, etc.23 Research flow was conducted to validate our results with HCQ, a commonly used csDMARD, widely prescribed to patients with autoimmune diseases, including RA.24 While HCQ is beneficial, it is generally considered to have a milder impact compared to other more potent immunosuppressive agents.25 The results indicated that RA patients who received HCQ showed lower CRP levels within 3m of treatment than patients without HCQ. Furthermore, the application ratio of NSAIDs was decreased in the HCQ-treated group. Research on HCQ suggests that the current RWS approach is valuable for evaluating the clinical efficacy of drugs. JGL did not show better benefits for patients with RA in this study, while HCQ did.
Potential limitations of this study include, firstly, the treatment course and dose of each medicine was impossible to figure out due to mobilization of patients and insufficiently detailed outpatients record; secondly, telephone calls were made to retrospectively complete the SF-36 questionnaire of all participants, and this could introduce recall bias. In future, prospective study with disease activity and QoL interviewed face-to-face with patients may release more accurate data. Thirdly, at baseline, patients in the study group with slightly higher age and IgM-RF levels than the reference group. As age might be the factor contributing to RF differences,20 we adjusted the RF titers by rejection part of the cases in the study group based on the results of stratification analysis. However, a prospective study with a similar baseline would confer more reliable findings.
Conclusion
However, with limitations, we conducted this RWS and found that adding JGL to RA patients failed to affect inflammatory markers or QoL significantly. Instead, more NSAIDs or other anti-rheumatic drugs were needed to fill the treatment insufficiency. Considering the economic burden to the families of RA patients and governmental health insurance, it is unnecessary to add JGL to RA therapy. Due to unavoidable confounding factors in RWS, a randomized controlled trial (RCT) is also recommended to confirm the findings. More over, folk herbal prescriptions are suggested to undergo strict clinical trials before application.
Acknowledgments
We would like to thank the RA patients and their family members for accepting our follow-up and monitoring as part of this study. This paper has been uploaded to ResearchGate as a preprint: https://www.researchgate.net/publication/378994429_No_significant_clinical_value_by_adding_on_Jin-gu-lian_Capsule_in_rheumatoid_arthritis_therapy_a_real_world_study.
Funding
This work was supported by grants from the Science and Technology Program of Guizhou Province (QIANKEHEZHICHEN[2022]YIBAN179) and Science and Technology Fund project of Guizhou Provincial Health Commission (gzwkj2024-126).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen Y, Chen Y, Zhao L. et al. Albumin/Globulin Ratio as Yin-Yang in Rheumatoid Arthritis and Its Correlation to Inflamm-Aging Cytokines. J INFLAMM RES. 2021;14:5501–5511.
2. Wang Y, Chen S, Du K, et al. Traditional herbal medicine: therapeutic potential in rheumatoid arthritis. J ETHNOPHARMACOL. 2021;279:114368. doi:10.1016/j.jep.2021.114368
3. Wang T, Wang Z, Qi W, Jiang G, Wang G. The role, targets and mechanisms of traditional Chinese medicine in regulating the balance of T helper type 17/regulatory Tcells in rheumatoid arthritis. INT J RHEUM DIS. 2023;26(4):613–624. doi:10.1111/1756-185X.14560
4. Chen T, Li S, Lian D, et al. Integrated Network Pharmacology and Experimental Approach to Investigate the Protective Effect of Jin Gu Lian Capsule on Rheumatoid Arthritis by Inhibiting Inflammation via IL-17/NF-kappaB Pathway. Drug Des Devel Ther. 2023;17:3723–3748. doi:10.2147/DDDT.S423022
5. CY G, HR A, MM W, L J. Clinical study of Jin Gu Lian capsule in the treatment of rheumatic obstruction syndrome rheumatoid arthritis. Chin J Clin Rat Drug Use. 2018;11(16):18–19.
6. Aletaha D, Neogi T, Silman AJ, et al. Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
7. Rempenault C, Combe B, Barnetche T, et al. Clinical and Structural Efficacy of Hydroxychloroquine in Rheumatoid Arthritis: a Systematic Review. Arthrit Care Res. 2020;72(1):36–40. doi:10.1002/acr.23826
8. Chen Y, Wang B, Chen Y, et al. HAPLN1 Affects Cell Viability and Promotes the Pro-Inflammatory Phenotype of Fibroblast-Like Synoviocytes. FRONT IMMU. 2022;13:888612. doi:10.3389/fimmu.2022.888612
9. Joelson A, Sigmundsson FG, Karlsson J. Stability of SF-36 profiles between 2007 and 2016: a study of 27,302 patients surgically treated for lumbar spine diseases. HEALTH QUAL LIFE OUT. 2022;20(1):92. doi:10.1186/s12955-022-01999-7
10. Chen Y, Qiu F, Yu B, et al. Metformin, an AMPK Activator, Inhibits Activation of FLSs but Promotes HAPLN1 Secretion. MOL THER-METH CLIN D. 2020;17:1202–1214. doi:10.1016/j.omtm.2020.05.008
11. Watanabe R, Hashimoto M, Murata K, et al. Prevalence and predictive factors of difficult-to-treat rheumatoid arthritis: the KURAMA cohort. IMMUNOL MED. 2022;45(1):35–44. doi:10.1080/25785826.2021.1928383
12. Pope JE, Choy EH. C-reactive protein and implications in rheumatoid arthritis and associated comorbidities. SEMIN ARTHRITIS RHEU. 2021;51(1):219–229. doi:10.1016/j.semarthrit.2020.11.005
13. Pathak A, Agrawal A. Evolution of C-Reactive Protein. FRONT IMMU. 2019;10:943. doi:10.3389/fimmu.2019.00943
14. Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: scoping review. SAGE OPEN MED. 2016;4:2103743725. doi:10.1177/2050312116671725
15. Lian D, Chen T, Yan L, et al. Protective effect of compatible herbs in Jin-Gu-Lian formula against Alangium chinense-induced neurotoxicity via oxidative stress, neurotransmitter metabolisms, and pharmacokinetics. FRONT PHARMACOL. 2023;14:1133982. doi:10.3389/fphar.2023.1133982
16. Dashtdar M, Dashtdar MR, Dashtdar B, Kardi K, Shirazi MK. The Concept of Wind in Traditional Chinese Medicine. J PHARMA. 2016;19(4):293–302. doi:10.3831/KPI.2016.19.030
17. Wang J, Wang Q, Li L, et al. Phlegm-dampness constitution: genomics, susceptibility, adjustment and treatment with traditional Chinese medicine. AM J CHINESE MED. 2013;41(2):253–262. doi:10.1142/S0192415X13500183
18. Dilts DM, Cheng SK, Crites JS, Sandler AB, Doroshow JH. Phase III clinical trial development: a process of chutes and ladders. Clin Cancer Res. 2010;16(22):5381–5389. doi:10.1158/1078-0432.CCR-10-1273
19. Xu L, Hu J, Liu L, Zhan S, Wang S. Trends and Patterns in Traditional Chinese Medicine Use Among Chinese Population in Late Adulthood: an Eight-Year Repeated Panel Survey. Am J Chinese Med. 2021;49(2):269–283. doi:10.1142/S0192415X21500142
20. Serhal L, Lwin MN, Holroyd C, Edwards CJ. Rheumatoid arthritis in the elderly: characteristics and treatment considerations. AUTOIMMUN REV. 2020;19(6):102528. doi:10.1016/j.autrev.2020.102528
21. Pyne D, Chaabo K. Adherence to immunosuppressant drugs in patients with connective tissue diseases. RHEUMATOLOGY. 2007;46(12):1859. doi:10.1093/rheumatology/kem267
22. Favalli EG, Pregnolato F, Biggioggero M, et al. Twelve-Year Retention Rate of First-Line Tumor Necrosis Factor Inhibitors in Rheumatoid Arthritis: real-Life Data From a Local Registry. ARTHRIT CARE RES. 2016;68(4):432–439. doi:10.1002/acr.22788
23. Sherman RE, Anderson SA, Dal Pan GJ, et al. Real-World Evidence - What Is It and What Can It Tell Us? NEW ENGL J MED. 2016;375(23):2293–2297. doi:10.1056/NEJMsb1609216
24. Nirk EL, Reggiori F, Mauthe M. Hydroxychloroquine in rheumatic autoimmune disorders and beyond. EMBO MOL MED. 2020;12(8):e12476. doi:10.15252/emmm.202012476
25. Smolen JS, Landewe R, Breedveld FC, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs. ANN RHEUM DIS. 2010;69(6):964–975. doi:10.1136/ard.2009.126532
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.