")
Back to Journals » Clinical Ophthalmology » Volume 19
Long-Term Evaluation of Central and Peripheral Lens Densities Post Implantation of Implantable Collamer Lens V4c
Authors Lin IC, Jiang Y, Cheng M, Li B, Lei Y, Xu G, Li M, Mao Z, Rui N, Chen X, Wang X
Received 12 October 2024
Accepted for publication 21 February 2025
Published 27 February 2025 Volume 2025:19 Pages 733—745
DOI https://doi.org/10.2147/OPTH.S500512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
I-Chun Lin,1– 4,* Yinjie Jiang,1– 4,* Mingrui Cheng,1– 4 Boliang Li,1– 4 Yadi Lei,1– 4 Guanghan Xu,1– 4 Mingwei Li,1– 4 Zhiwei Mao,1– 4 Ning Rui,1– 4 Xun Chen,1– 4 Xiaoying Wang1– 4
1Fudan University Eye Ear Nose and Throat Hospital, Shanghai, People’s Republic of China; 2National Health Commission Key Laboratory of Myopia (Fudan University), Shanghai, People’s Republic of China; 3Shanghai Research Center of Ophthalmology and Optometry, Shanghai, People’s Republic of China; 4State Key Laboratory of Medical Neurobiology and MOE Frontiers Center for Brain Science, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoying Wang; Xun Chen, Department of Ophthalmology, Eye & ENT Hospital of Fudan University, No. 19 BaoQing Road, XuHui District, Shanghai, 200031, People’s Republic of China, Tel +86-021-64377134, Email [email protected]; [email protected]
Purpose: This study aimed to analyze the impact of long-term ICL implantation on lens density, focusing on the relationship between the anterior subcapsule, anterior lens density, and implantable collamer lenses (ICL) position after ICL V4c implantation.
Methods: This retrospective study included 145 eyes with ICL V4c implantation and average follow-up of 4.2 years (range: 3– 8 years). The control group comprised 65 myopic eyes without surgery. All participants underwent comprehensive ophthalmologic examinations, and lens density were measured using quantitative Scheimpflug images.
Results: The central anterior subcapsular densities were 8.62 ± 1.39% preoperatively, 8.99 ± 1.31% at 3 months, and 9.29 ± 0.95% at the last follow-up post ICL implantation (p < 0.001). At last follow-up, the anterior subcapsular densities were 9.29 ± 0.95% in the central region, 8.92 ± 0.79% in the long axis of peripheral region, and 8.62 ± 0.76% in the short axis of peripheral region (p < 0.001). The densities were lower in the non-surgical group than in the ICL implantation group. One eye (0.69%) was discovered to have anterior subcapsular and nuclear opacification.
Conclusion: The density of the anterior subcapsule increased over time after ICL implantation. Preoperative refraction and pupil size were correlated with changes in anterior subcapsule density. The central anterior subcapsule density was higher than that at the periphery, and the peripheral density of the long axis was higher than that of the short axis.
Keywords: ASC, anterior subcapsular opacification, ICL, lens density, V4c
Introduction
High myopia can be challenging to correct effectively due to corneal thickness limitations. Phakic intraocular lenses (pIOLs) provide a safe and reversible solution that preserves corneal integrity.1 The implantable collamer lens (ICL; Staar Surgical, Nidau, Switzerland) is a widely recognized option approved by the Food and Drug Administration for correcting moderate to high myopia (up to −18D) and astigmatism (up to 6D). Numerous studies have demonstrated the safety and efficacy of ICL implantation.2–4 Despite the verified safety of the implantable collamer lens (ICL), research has reported some complications related to its use. Cataract formation, particularly in the anterior subcapsule, is one of the most frequently documented safety issues with ICL implantation.5 Previous studies have indicated that anterior subcapsular opacification and cataract formation in traditional ICL models without the central hole are associated with low vault.6,7 The ICL V4c model features a 360-μm central hole that promotes aqueous humor circulation and eliminates the need for iridotomy.8 This “CentraFLOW Technology” design is more resistant to lens opacification than the V4 model and can control the flow of aqueous humor between the ICL and the crystalline lens.9
Both subjective and objective methods can be used to assess the lens clarity. The lens opacification classification system III (LOCS III) is a subjective method used to evaluate approximate cataract morphology and opacity with a slit-lamp microscope.10 Conversely, measuring the lens density using the Scheimpflug camera of the Pentacam is an objective method for evaluating the opacity of a part of the lens. Additionally, it is possible to observe variations in the lens density before visible opacification occurs, providing a reference for preventing anterior subcapsular opacification and cataracts. The Pentacam provides a precise and reproducible measurement of the lens density in the selected area.11 Objective measurements can sensitively and accurately record changes in the lens density at different locations and evaluate cataract development.
While the long-term incidence of cataracts with ICL V4c (with a central hole) is lower compared to the previous model without a central hole,9,12 ICL V4c implantation may still have an impact on crystalline lens density, particularly in patients aged 40 years and above. Studies by Ye et al and Yang et al demonstrated that anterior average lens density (a-ALD), as measured by Pentacam, increased 4 years post-ICL implantation compared to preoperative measurements and 3 months post-surgery. Additionally, in patients exceeding 40 years of age, a-ALD was found to rise at 3 months post-operation compared to preoperative values.13,14 It is crucial to assess the likelihood of a continuous rise in lens density with the extended surgical duration, identify the threshold at which heightened lens density leads to anterior subcapsular opacification or cataracts, and determine the optimal timing for clinical intervention. Distinguishing whether elevated lens density is due to age-related factors or the impact of ICL implantation is vital for clinical diagnosis.
This study examined long-term anterior subcapsule and anterior lens density in individuals that underwent ICL implantation and compared it with those in individuals with myopia that did not undergo surgical intervention. The aim was to analyze the impact of long-term ICL implantation on lens density, focusing on the relationship between the anterior subcapsule, anterior lens density, and ICL position after ICL V4c implantation, providing guidance for clinical decision-making.
Materials and Methods
Patients
A total of 145 eyes were included in this retrospective case-control study, all of which underwent ICL V4c implantation to correct myopia or myopic astigmatism at the Eye Ear Nose and Throat Hospital, Fudan University. The surgeries were performed between January 2015 and September 2020, with an average follow-up period of 4.2 years (range: 3–8 years). To assess the impact of lens density in different regions without ICL implantation, this study included a control group consisting of 65 eyes of individuals with myopia that did not undergo the operation. Based on Chow et al’s work, the sample sizes were calculated using an α of 0.05, a power (1−β) of 80%, and a 2:1 ICL implantation to control ratio, with lens opacity incidence rates also considered.15–17 Both the ICL implantation and control groups met all inclusion criteria. Patient characteristics and ocular parameters were carefully matched to ensure comparability between the two groups.
The inclusion criteria for the study were as follows: (1) patients who had undergone ICL implantation more than 3 years prior to the study, (2) had available preoperative and 3-month postoperative imaging records and (3) had undergone a safe surgical procedure without intraoperative lens injury or any intraoperative or postoperative complications. Exclusion criteria included (1) a cumulative refractive error (including the refractive error corrected by the implanted ICL lens and the postoperative residual error) exceeding −2000 diopters, (2) age above 50 years, (3) the presence of other ocular diseases, (4) a history of trauma, or ocular surgeries other than ICL implantation, including procedures such as intravitreal injections for high myopia-related retinal hemorrhage.
The following assessments were recorded: (1) uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA); (2) manifest and cycloplegic refraction; (3) slit lamp biomicroscopy and fundoscopic examinations; (4) intraocular pressure (IOP, Tonemeterx-10, Canon, Japan); (5) corneal topography and central corneal thickness (Pentacam HR, Type 70900; Oculus Optikgeräte GmbH, Wetzlar, Germany); (6) horizontal corneal diameter (white-to-white, [WTW], (IOL Master 500, ZEISS, Germany); (7) axial length (IOL Master); (8) anterior chamber depth (ACD), anterior chamber volume (ACV), and anterior chamber angle (ACG) (Pentacam); (9) endothelial cell density (ECD, SP-3000P, Topcon Corporation, Tokyo, Japan); (10) optical coherence tomography (OCT, Optovue, Florida, USA); and (11) ultrasound biomicroscopy (UBM, Quantel Medical, Clermont-Ferrand, France).
Compliance With Ethics Guidelines
The study adhered to the principles of the Helsinki Declaration and received approval from the Ethics Committee of Fudan University Eye, Ear, Nose, and Throat Hospital (2021018). Participants provided written informed consent following a comprehensive explanation of the procedure. To protect their privacy, all data were anonymized.
ICL Axis, Crystalline Lens Density, and Vault Height
The ICL axis was measured using an OPD-Scan III (Nidek Co., Ltd., Gamagori, Japan). Measurements were conducted under mesopic lighting conditions (3 cd/m²), with pupils dilated to ensure a size of over 6.0 mm. ICL axis data were obtained by manually aligning the angle scale to the two peripheral holes of the ICL under retrobulbar illumination mode.18
Lens density was measured using a Pentacam device at three time points: preoperatively, 3 months postoperatively, and at the last follow-up. Patients underwent pupil dilation to achieve a pupil size exceeding 6.0 mm at the last follow-up. All the measurements were performed under dark conditions. Only images with a quality factor above 95% were considered acceptable We obtained the long and short ICL axis meridian planes from the Scheimpflug images to measure the density of the anterior subcapsular and anterior middle lens regions for eyes with ICL implantation. For eyes without ICL implantation, the crystalline lens density was measured along the horizontal 180° axis and the vertical 90° axis. The long axis of the ICL refers to the axis along the longer direction of the lens, representing its overall length. The short axis is the axis perpendicular to the long axis, corresponding to the shorter direction of the lens. In the Scheimpflug image mode, we employed line densitogram and area densitometry tools to determine the density at the anterior subcapsule and anterior lens (the anterior one-third region). As shown in Figure 1, we evaluated the density of the central lens (diameter within a 2-mm area) and peripheral lens (diameter outside of a 2-mm area) separately. The software automatically calculated the areas of the selected image and provided numerical values for the average lens density, expressed as the percentage of absorbed light. The data presented were derived from the average of five repeated measurements at each time point to ensure accuracy and reliability. The optical density of the lens was measured on a scale ranging from 0% to 100%, where 0% represented a completely clear lens and 100% indicated full opacity.
 |
Figure 1 (A) To measure the density of the central anterior subcapsule, a 1.8-mm line (purple line), using the line densitogram tools, was positioned along the central front of the crystalline lens outline, with its center aligned to the central hole of the implantable collamer lens (ICL). The average density of this region was automatically calculated. To measure the density of the peripheral anterior subcapsule, two 1.8-mm lines (red and blue lines), employing the line densitogram tools, were positioned along each side of the peripheral front of the crystalline lens outline. These lines were situated more than 1 mm outside the central hole of the ICL; (B) To measure the density of the central anterior lens, a 1.8×0.8 mm rectangle (purple rectangle), using the area densitometry tools, was created. This rectangle was placed along the central front of the one-third region of lens, with its center aligned to the central hole of the implantable collamer lens (ICL). To measure the density of the peripheral anterior lens, two 1.8×0.8 mm rectangles (red and blue rectangles), using the area densitometry tools, were drawn. These rectangles were positioned along each side of the peripheral front of the one-third region of lens and were situated more than 1 mm outside the central hole of ICL. |
Vault height measurements were obtained using anterior segment OCT (AS-OCT) (CASIA II, Tomey Corporation, Nagoya, Japan) under dark conditions with pupil mydriasis exceeding 6.0 mm. We used the meridian planes of the long and short ICL axis from the CASIA II images to assess both central and peripheral vault heights. The long axis of the ICL is the longer direction of the lens, while the short axis is perpendicular to it and represents the shorter direction. The central vault was measured at the location of the central hole, while the peripheral vault was measured on two sides within a diameter of 6–7 mm around the central hole.
Statistical Analysis
Data analyses were conducted using SPSS software (version 26.0; IBM, USA). Results are presented as the mean ± standard deviation. Data normality was confirmed using the Shapiro–Wilk test. Student’s t-test was applied for normally distributed data, whereas the Mann–Whitney U-test was used for non-normally distributed data to compare two groups. Analysis of variance (ANOVA) was used for comparisons involving more than two groups of continuous variables. Post-hoc analysis was carried out using the Least Significant Difference (LSD) method. To eliminate the potential influence of age on the lens density between the ICL implantation group and the non-surgical group, analysis of covariance (ANCOVA) was performed to adjust the data. Pearson or Spearman correlation coefficients were used to assess the relationship between lens density and other variables based on data distribution. A two-tailed test was used for all hypothesis testing, with statistical significance defined as p < 0.05.
Results
Patient Profiles
In this study, the group that underwent ICL implantation included 145 eyes from 145 patients, while the non-surgical group consisted of 65 eyes from 65 patients. Patient demographic data are shown in Table 1. The ICL implantation group had a mean age of 32.41 ± 6.04 years (range: 22–49 years) and a mean spherical equivalent of −9.30 ± 2.96D. In contrast, the non-surgical group showed a mean age of 31.48 ± 6.23 years (range: 21–50 years) and a mean spherical equivalent of −8.72 ± 3.27D. There were no significant differences between the two groups in terms of age, mean spherical equivalent, CDVA, or axial length (P > 0.05).
 |
Table 1 Demographic Data of Patients with Myopia That Underwent ICL Implantation and Those of the Non-Surgical Group |
Efficacy and Safety
Figure 2A and B display that the efficacy index, defined as the ratio of postoperative UDVA to preoperative CDVA, was found to be 0.86 ± 0.28, with values ranging from 0.06 to 1.71. The safety index at the final follow-up, determined by the ratio of postoperative CDVA to preoperative CDVA, was recorded at 1.19 ± 0.23, with a range between 0.29 and 2.14. Among the eyes examined in this study, 52.41% attained a postoperative UDVA of 20/20 or better, while 90.34% achieved a postoperative UDVA of 20/40 or better. Furthermore, 94.48% of the eyes reached a postoperative CDVA of 20/20 or better, and 99.31% had a postoperative CDVA of 20/40 or better. Additionally, 1.38% (2/145) of eyes experienced a decrease of ≥ 2 lines in CDVA due to complications, with one eye affected by macular schisis and the other by a cataract.
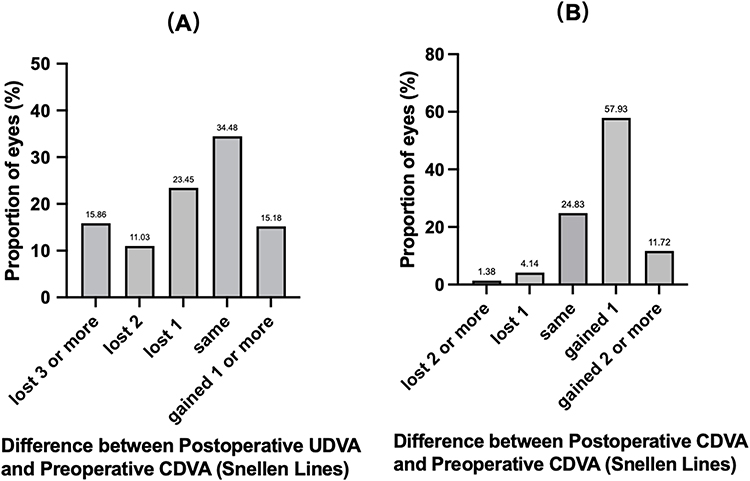 |
Figure 2 Refractive outcomes at last follow-up post-implantation of the implantable collamer lens (ICL). (A) Changes in Snellen lines of uncorrected distance visual acuity (UDVA). (B) Changes in Snellen lines of corrected distance visual acuity (CDVA). |
Predictability and Stability
Figure 3A illustrates a scatter plot comparing the attempted versus achieved spherical equivalent. At the last follow-up, the analysis of preoperative spherical equivalent (SE) against the target refractive power revealed that 44.14% of eyes fell within ±0.50 D, while 75.86% were within ±1.00 D, as shown in Figure 3B. Figure 3C shows the stability of SE refraction. The preoperative SE was −8.59 ± 2.87 D, −0.29 ± 0.47 D at 3 months, and −0.77 ± 0.69 D at the last follow-up.
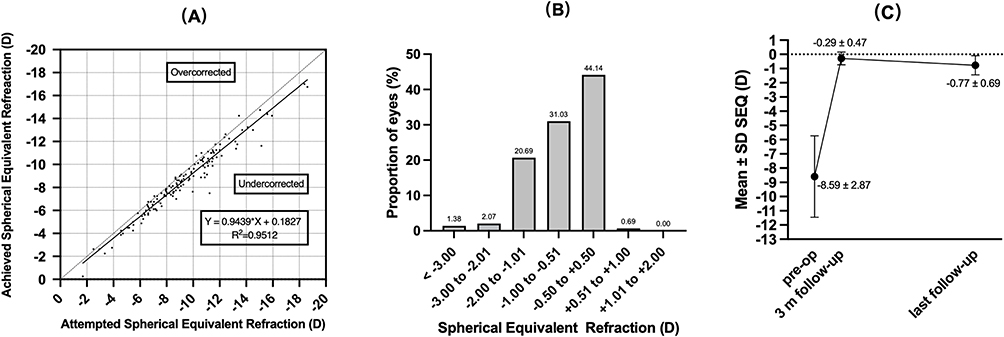 |
Figure 3 Refractive outcomes at last follow-up post-implantation of the implantable collamer lens (ICL). (A) Attempted versus achieved spherical equivalent (SE) refraction. (B) SE refraction. (C) Stability of SE refraction up to the last follow-up. Abbreviations: D, diopters; Pre-op, preoperative. |
Crystalline Lens Density and Vault Height
Table 2 presents the density in different regions of the lens at the last follow-up after ICL and that of non-surgical group. Additionally, the central and peripheral vault heights at the long and short ICL axes are listed. After ICL implantation, the densities of the anterior subcapsule and anterior lens in the peripheral region were lower than those in the central region (p < 0.001). Furthermore, the densities of the anterior subcapsule in the peripheral region along the short axis were lower than those in the peripheral region along the long axis (p < 0.05). In contrast, no differences were observed in the density of the anterior subcapsule and anterior lens between the peripheral and central regions along both the long and short axes in the non-surgical group (p > 0.05). Additionally, the densities were lower in the non-surgical group than in the ICL implantation group, particularly in the central and peripheral regions of the anterior subcapsule and the central regions of the anterior lens (p < 0.05).
 |
Table 2 Lens Density and Vault Height at Last Follow-up in the ICL Implantation Group and Lens Density in the Non-Surgical Group |
After being adjusted for the effect of age using analysis of covariance, the preoperative lens density of the central anterior subcapsule was 8.62 ± 1.39% in the ICL implantation group, while the value was 8.30 ± 0.83% in the non-surgical group (p = 0.107). Additionally, the preoperative anterior lens density in the ICL implantation group was 7.68 ± 1.42%, compared to 7.52 ± 1.00% in the non-surgical group (p = 0.569).
Changes in Central Lens Density Preoperatively, at 3 months, and at Last Follow-up After ICL Implantation
As shown in Figure 4A and B, the central anterior subcapsule density was 8.62 ± 1.39% preoperatively, 8.99 ± 1.31% at 3 months, and 9.29 ± 0.95% at the last follow-up (p < 0.001). The central lens density was 7.68 ± 1.42% preoperatively, 7.93 ± 1.38% at 3 months, and 8.12 ± 1.15% at the last follow-up (p = 0.022).
 |
Figure 4 Lens density measurements preoperatively, at 3 months, and at last follow-up after implantable collamer lens (ICL) implantation (A) Central anterior subcapsule density (p < 0.001); (B) Central anterior lens density (p = 0.022). |
We found a positive correlation between changes in the central lens density of the anterior subcapsule with the time elapsed after surgery (in years), axial length, and pupil size in a dark room (p < 0.05). Additionally, a negative correlation was observed between spherical diopters and equivalent spherical diopters. Furthermore, changes in the central lens density were positively correlated with the time elapsed after surgery (p < 0.05). However, changes in the central lens density of the anterior subcapsule demonstrated no relationship with age, cylindrical diopter, central and peripheral vault heights, ACD, corneal thickness, WTW, STS, anterior chamber angle (ACA), intraocular pressure (IOP), corneal curvature, or corneal endothelial count (Table 3).
 |
Table 3 Changes in Central Lens Density and Its Correlation With Various Factors at Three Time Points: Preoperatively, at 3 months, and at Final Follow-up Post-Implantation of ICL |
Case of Occurring Cataract
One eye (0.69%) was discovered to have anterior subcapsular and nuclear opacification under slip lamp examination, with a decrease in CDVA (Table 4 and Figure 5A and B). No significant lens opacity was observed in the other eyes.
 |
Table 4 Characteristics of the Patients and Eyes in the Event of a Clinical Cataract |
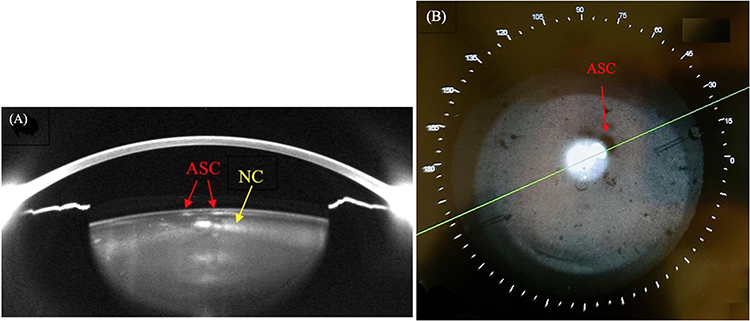 |
Figure 5 The eye that was discovered to have anterior lens opacity and nuclear lens opacity (A) Scheimpflug images by the Pentacam device; (B) images taken by OPD-Scan III under retrobulbar illumination mode. Abbreviations: ASC, anterior subcapsule cataract; NC, nuclear cataract. |
Discussion
ICL implantation is a safe and effective procedure for correcting myopia; however, some studies have reported potential complications associated with the ICL.19 One of the most common complications is cataracts, which reduces visual acuity and shortens the lifespan of ICL implantation. According to published reports, the rate of lens opacity in eyes with ICL implants (in V4 and early models without central hole) also increases over time; it was found to be 3% at 1 year, 4% to 11% at 2 years, 7% to 40.9% at 5 years, and 28% to 54.8% at 10 years.7,20 ICL extraction and phacoemulsification were frequently deemed necessary in 17%–18.3% of cases within 10 years following ICL implantation.7,20 Despite the limited available data, studies suggest a decreasing trend in the incidence of cataracts associated with ICL V4c (with a central hole) compared to models without a central hole.9,12,20 ASC is considered to be the ICL-related form of cataract, and most studies have reported that the indication of ASC after ICL implantation might be related to low vault height, fluidics of the aqueous humor, and the age of patients.6,7,20–22
We found that clinical ASC and nuclear cataract occurred in only one eye (0.69%) that was scheduled for phacoemulsification. In this patient, the measured anterior subcapsular density exceeded 11%, and concurrent observations revealed anterior subcapsular opacity during slit-lamp microscopic examination. In contrast, the measured density in the transparent anterior subcapsular region ranged from 8% to 9%. Based on our observations, when the anterior subcapsular density exceeded 11, the likelihood of anterior subcapsular opacity formation increased.
In patients without cataract onset, the peripheral anterior subcapsular density of the long axis was higher than that of the short axis plane. No significant differences were observed in the various regions of the anterior subcapsular density in the non-surgical control group with myopia. The length of ICL ranges from 12.1–13.7 mm and the width ranges from 7.5–8.0 mm20. We assumed that changes in the aqueous humor circulation had less impact on the transfer of nutrients to the peripheral crystalline lens along the short axis of the ICL; this is because the short axis does not extend over the peripheral region of the crystalline lens.
The initial discovery of opacification in myopic eyes treated with the earlier version of the ICL (no central hole) indicated that it predominantly occurred in the peripheral regions of the lens area.7,20,21 According to Sarikkola et al, cataract formation in myopic eyes first manifested beneath the thickest part of the ICL, which is located at its periphery.21 This phenomenon is probably attributed to the close proximity of the ICL to the crystalline lens in that particular region. In contrast, the ICL V4c, which features a central hole, is reported to pose a lower risk for anterior subcapsular cataracts (ASC) compared to its predecessor, as the central hole enhances aqueous humor metabolism and facilitates circulation to the anterior surface of the crystalline lens.9,23,24 Moreover, the implantation of the ICL V4c (with a central hole) alters the flow of aqueous humor, impacting the wall shear stress experienced in the central region of the crystalline lens.25 Long-term wall shear stress on crystalline lenses can potentially contribute to ASC formation. Our study revealed that the anterior subcapsular and anterior lens densities were greater in the central region compared to the peripheral region in the ICL implantation group. Furthermore, no significant differences were observed in these densities within the non-surgical myopic control group.
Numerous studies have considered low vault as a risk factor for ASC, primarily due to the persistent or intermittent contact between the ICL and the crystalline lens, along with insufficient nutrition delivered through the anterior chamber flow between these two structures.7,9 However, our study revealed no correlation between lens density and vault height. Simultaneously, we found that the peripheral vault height was lower than the central vault height, which is consistent with the findings of Jiménez-Alfaro et al and Trindade et al26,27 Conversely, the central lens density was higher than that of the peripheral region in the ICL implantation group.
Despite the lower vault, the ICL V4c with a central hole maintains a well-distributed aqueous humor flow between the ICL and the crystalline lens, facilitating circulation from the posterior to the anterior chamber. Fernández-Vigo et al demonstrated that the velocity of aqueous humor flow through the central hole of the ICL was increased in cases with reduced vault heights. Furthermore, when comparing flow rates, the central-hole ICL showed greater aqueous humor passage through its ducts (360-μm central hole) compared to the ICL without a central hole, particularly at lower vault heights.25,28 This suggests that the central-hole design of the ICL may enhance circulation at the anterior surface of the crystalline lens, potentially lowering the risk of cataract formation compared to its predecessor without a central hole.24,28 Additionally, Gonzalez-Lopez et al proposed that the central port of the ICL may offer some degree of protection against the long-term development of cataracts, even in eyes with lower vault heights.29
Nakamura et al found that the surfaces of explanted ICLs showed no signs of damage or depositions, suggesting minimal contact between the ICLs and adjacent tissues, such as the iris and crystalline lens. This observation implies that the development of ASC may be more closely related to insufficient aqueous humor circulation than to mechanical interaction between the crystalline lens and the ICL.30,31 We lean toward supporting this perspective. In our study, one patient developed a clinical cataract; however, the ICL did not contact either the central or peripheral regions of the crystalline lenses. Additionally, this patient had ICL implantation after the age of 40, a period when protein aggregation and membrane binding in the central lens region increase significantly, leading to higher lens density, greater stiffness, and reduced molecular diffusion. These factors may have contributed to the development of the cataract.32 These factors may have contributed to the development of the cataract. Previous studies have identified age as a significant risk factor for cataract development following ICL implantation.19,21 In individuals with high myopia, crystalline opacity tends to increase progressively with age, especially in those over 40 years old.6,33,34
In our study, there was a progressive increase in anterior subcapsular density over time following surgery. This observation implies that ICL implantation has the potential to modify the anterior subcapsular density. Moreover, our study revealed that increased preoperative diopters and escalating severity of myopia were associated with increased density levels in the anterior subcapsule. Some studies have suggested that a preoperative diopter exceeding −12D to −14D is associated with an increased risk of ASC.19,35,36 Additionally, we observed a positive relationship between pupil size in a dark room and anterior subcapsular density. The size of the pupil is influenced by the activity of the ciliary muscle, and changes in pupil size can alter the position of the ICL as well as the velocity and distribution of aqueous humor within the eye, impacting the wall shear stress on the crystalline lens.25,28 Fernández-Vigo et al showed that the wall shear stress on a crystalline lens is affected by both the vault height and pupil size.25 Consequently, these alterations may indirectly influence the anterior subcapsular density.
The occurrence of early-onset cataracts appears to have declined in recent years, likely due to advancements in lens design and improvements in surgical techniques, including the surgeon’s experience and proficiency. Steinwender et al revealed that several patients developed central anterior subcapsular opacification after a short period of ICL V4c implantation. Anterior subcapsular opacification occurred during ICL implantation as a result of cannula irrigation, which directed a strong flow onto the capsule through the central hole of the ICL. Subsequently, the surgical technique was modified to prevent anterior subcapsular opacification.37
This study has some limitations. The central and peripheral vaults were measured under mydriatic conditions. In previous studies, there was a positive correlation between the ICL vault and the pupil diameter. During miosis, the iris exerts downward pressure on the ICL, leading to a reduction in the central vault.38,39 This suggests that the vault height may have been overestimated. Moreover, this study lacks data on changes in crystalline lens density for the control group of myopic eyes without surgery, and the sample size in this study was limited. Addressing these aspects in future prespective study would enable a more comprehensive comparison and enhance the validation of our findings by including a larger sample size.
Conclusion
The density of the anterior subcapsule increased over time after ICL implantation. Preoperative refraction and pupil size were correlated with changes in anterior subcapsule density. The central anterior subcapsule density was higher than that at the periphery, and the peripheral density of the long axis was higher than that of the short axis, which may be attributed to wall shear stress on the crystalline lens by altering the flow of aqueous humor from the central hole.
Data Sharing Statement
Data and materials are available upon request from the corresponding author at [email protected] or [email protected].
Ethics Approval and Consent to Participate
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethical Committee Review Board of Fudan University Eye and ENT Hospital (2021018).
Consent for Publication
Written informed consent was obtained from the patient for publication of this paper.
Funding
Xiaoying.Wang; National Natural Science Foundation of China (Grant No.82171095). Xiaoying.Wang; Project of Shanghai Science and Technology (Grant No. 23XD1400500). Xiaoying.Wang; Project of Shanghai Shenkang Hospital Development Center (Grant No.SHDC12024148).
Disclosure
I-Chun Lin and Yinjie Jiang are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Cakir I, Sonmez O, Pehlivanoglu S, et al. Long-term results of a new posterior chamber phakic intraocular lens in patients with high myopia: 5-year results. J Cataract Refract Surg. 2023;49(4):409–415. doi:10.1097/j.jcrs.0000000000001110
2. Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol. 2016;10:1059–1077. doi:10.2147/OPTH.S111620
3. Packer M. The implantable collamer lens with a central port: review of the literature. OPTH. 2018;12:2427–2438. doi:10.2147/OPTH.S188785
4. Bai Z, Nie D, Zhang J, et al. Visual function assessment of posterior-chamber phakic implantable collamer lenses with a central port. Ann Translat Med. 2022;10(4):194. doi:10.21037/atm-22-107
5. Fernandes P, González-Méijome JM, Madrid-Costa D, Ferrer-Blasco T, Jorge J, Montés-Micó R. Implantable collamer posterior chamber intraocular lenses: a review of potential complications. J Refract Surg. 2011;27(10):765–776. doi:10.3928/1081597X-20110617-01
6. Gonvers M, Bornet C, Othenin-Girard P. Implantable contact lens for moderate to high myopia: relationship of vaulting to cataract formation. J Cataract Refract Surg. 2003;29(5):918–924. doi:10.1016/S0886-3350(03)00065-8
7. Guber I, Mouvet V, Bergin C, Perritaz S, Othenin-Girard P, Majo F. Clinical outcomes and cataract formation rates in eyes 10 years after posterior phakic lens implantation for myopia. JAMA Ophthalmol. 2016;134(5):487–494. doi:10.1001/jamaophthalmol.2016.0078
8. Chen X, Miao H, Naidu RK, Wang X, Zhou X. Comparison of early changes in and factors affecting vault following posterior chamber phakic implantable collamer lens implantation without and with a central hole (ICL V4 and ICL V4c). BMC Ophthalmol. 2016;16(1):161. doi:10.1186/s12886-016-0336-8
9. Chen X, Wang X, Xu Y, et al. Long-term comparison of vault and complications of implantable collamer lens with and without a central hole for high myopia correction: 5 years. Curr Eye Res. 2022;47(4):540–546. doi:10.1080/02713683.2021.2012202
10. Chylack LT, Wolfe JK, Singer DM, et al. The Lens Opacities Classification System III. The Longitudinal Study of Cataract Study Group. Arch Ophthalmol. 1993;111(6):831–836. doi:10.1001/archopht.1993.01090060119035
11. Faria-Correia F, Lopes B, Monteiro T, Franqueira N, Ambrósio R. Scheimpflug lens densitometry and ocular wavefront aberrations in patients with mild nuclear cataract. J Cataract Refract Surg. 2016;42(3):405–411. doi:10.1016/j.jcrs.2015.10.069
12. Shimizu K, Kamiya K, Igarashi A, Kobashi H. Long-term comparison of posterior chamber phakic intraocular lens with and without a central hole (hole ICL and conventional ICL) implantation for moderate to high myopia and myopic astigmatism: consort-compliant article. Medicine. 2016;95(14):e3270. doi:10.1097/MD.0000000000003270
13. Ye Y, Zhao J, Niu L, Shi W, Wang X, Zhou X. Long-term evaluation of anterior lens density after implantable collamer lens V4c implantation in patients with myopia over 40 years old. Br J Ophthalmol. 2022;106(11):1508–1513. doi:10.1136/bjophthalmol-2021-319205
14. Yang W, Zhao J, Zhao J, Shen Y, Niu L, Zhou X. Changes in anterior lens density after implantable collamer lens V4c implantation: a 4‐year prospective observational study. Acta Ophthalmologica. 2021;8.
15. Fang R, Yu YF, Li EJ, et al. Global, regional, national burden and gender disparity of cataract: findings from the global burden of disease study 2019. BMC Public Health. 2022;22(1):2068. doi:10.1186/s12889-022-14491-0
16. Sanders DR. Anterior subcapsular opacities and cataracts 5 years after surgery in the visian implantable collamer lens FDA trial. 2008;24.
17. Chow SC, Shao J, Wang H, Lokhnygina Y. Sample Size Calculations in Clinical Research.
18. Chen X, Miao H, Cheng M, et al. Effect of long-term rotation on astigmatism following EVO-toric intraocular collamer lens implantation. Front Med. 2023;10:1194006. doi:10.3389/fmed.2023.1194006
19. Zhang H, Gong R, Zhang X, Deng Y. Analysis of perioperative problems related to intraocular implantable collamer Lens (ICL) implantation. Int Ophthalmol. 2022;42(11):3625–3641. doi:10.1007/s10792-022-02355-w
20. Schmidinger G, Lackner B, Pieh S, Skorpik C. Long-term changes in posterior chamber phakic intraocular collamer lens vaulting in myopic patients. Ophthalmology. 2010;117(8):1506–1511. doi:10.1016/j.ophtha.2009.12.013
21. Sarikkola AU, Sen NH, Uusitalo RJ, Laatikainen L. Traumatic cataract and other adverse events with the implantable contact lens. J Cataract Refract Surg. 2005;31(3):511–524. doi:10.1016/j.jcrs.2004.06.084
22. Shiratani T, Shimizu K, Fujisawa K, Uga S, Nagano K, Murakami Y. Crystalline lens changes in porcine eyes with implanted phakic IOL (ICL) with a central hole. Graefes Arch Clin Exp Ophthalmol. 2008;246(5):719–728. doi:10.1007/s00417-007-0759-2
23. Karandikar S, Bhandari V, Reddy J. Outcomes of implantable collamer lens V4 and V4c for correction of high myopia – a case series. Nep J Oph. 2016;7(2):164–172. doi:10.3126/nepjoph.v7i2.14967
24. Kawamorita T, Uozato H, Shimizu K. Fluid dynamics simulation of aqueous humour in a posterior-chamber phakic intraocular lens with a central perforation. Graefes Arch Clin Exp Ophthalmol. 2012;250(6):935–939. doi:10.1007/s00417-011-1850-2
25. Fernández-Vigo JI, Marcos AC, Agujetas R, et al. Computational simulation of aqueous humour dynamics in the presence of a posterior-chamber versus iris-fixed phakic intraocular lens Liton PB, ed. PLoS One. 2018;13(8):e0202128. doi:10.1371/journal.pone.0202128
26. Trindade F, Pereira F, Cronemberger S. Ultrasound biomicroscopic imaging of posterior chamber phakic intraocular lens. J Refract Surg. 1998;14(5):497–503. doi:10.3928/1081-597X-19980901-06
27. Jiménez-Alfaro I, del CJMB, Garcı́a-Feijoó J, de BJGG, de la IJMS. Safety of posterior chamber phakic intraocular lenses for the correction of high myopia: anterior segment changes after posterior chamber phakic intraocular lens implantation. Ophthalmology. 2001;108(1):90–99. doi:10.1016/S0161-6420(00)00403-6
28. Fernández-Vigo JI, Macarro-Merino A, Fernández-Francos J, et al. Computational study of aqueous humor dynamics assessing the vault and the pupil diameter in two posterior-chamber phakic lenses. Invest Ophthalmol Vis Sci. 2016;57(11):4625. doi:10.1167/iovs.16-19900
29. Gonzalez-Lopez F, Bouza-Miguens C, Tejerina V, Mompean B, Ortega-Usobiaga J, Bilbao-Calabuig R. Long-term assessment of crystalline lens transparency in eyes implanted with a central-hole phakic collamer lens developing low postoperative vault. J Cataract Refract Surg. 2021;47(2):204–210. doi:10.1097/j.jcrs.0000000000000425
30. Nakamura T, Isogai N, Kojima T, et al. Long-term in vivo stability of posterior chamber phakic intraocular lens: properties and light transmission characteristics of explants. Am J Ophthalmol. 2020;219:295–302. doi:10.1016/j.ajo.2020.06.025
31. Nakamura T, Isogai N, Kojima T, Yoshida Y, Sugiyama Y. Posterior chamber phakic intraocular lens implantation for the correction of myopia and myopic astigmatism: a retrospective 10-year follow-up study. Am J Ophthalmol. 2019;206:1–10. doi:10.1016/j.ajo.2019.04.024
32. Friedrich MG, Truscott RJW. Membrane association of proteins in the aging human lens: profound changes take place in the fifth decade of life. Invest Ophthalmol Vis Sci. 2009;50(10):4786. doi:10.1167/iovs.09-3588
33. Haarman AEG, Enthoven CA, Tideman JWL, Tedja MS, Verhoeven VJM, Klaver CCW. The complications of myopia: a review and meta-analysis. Invest Ophthalmol Vis Sci. 2020;61(4):49. doi:10.1167/iovs.61.4.49
34. Pan CW, Boey PY, Cheng CY, et al. Myopia, axial length, and age-related cataract: the Singapore Malay eye study. Invest Ophthalmol Vis Sci. 2013;54(7):4498. doi:10.1167/iovs.13-12271
35. Alfonso JF, Lisa C, Fernandez-Vega L, Almanzar D, Perez-Vives C, Montes-Mico R. Prevalence of cataract after collagen copolymer phakic intraocular lens implantation for myopia, hyperopia, and astigmatism. J Cataract Refract Surg. 2015;41(4):800–805. doi:10.1016/j.jcrs.2014.07.039
36. Maeng HS, Chung TY, Lee DH, Chung ES. Risk factor evaluation for cataract development in patients with low vaulting after phakic intraocular lens implantation. J Cataract Refract Surg. 2011;37(5):881–885. [10/dqw3gc]. doi:10.1016/j.jcrs.2010.11.037
37. Steinwender G, Varna-Tigka K, Shajari M, Kohnen T. Anterior subcapsular cataract caused by forceful irrigation during implantation of a posterior chamber phakic intraocular lens with a central hole. J Cataract Refract Surg. 2017;43(7):969–974. doi:10.1016/j.jcrs.2017.03.045
38. Gonzalez-Lopez F, Bouza-Miguens C, Tejerina V, et al. Dynamic assessment of variations in pupil diameter using swept-source anterior segment optical coherence tomography after phakic collamer lens implantation. Eye Vis. 2021;8(1):39. doi:10.1186/s40662-021-00262-2
39. Gonzalez-Lopez F, Bilbao-Calabuig R, Mompean B, Luezas J, Ortega-Usobiaga J, Druchkiv V. Determining the potential role of crystalline lens rise in vaulting in posterior chamber phakic collamer lens surgery for correction of myopia. J Refract Surg. 2019;35(3):177–183. doi:10.3928/1081597X-20190204-01
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.