")
Back to Journals » Clinical Ophthalmology » Volume 18
Long-Term Observation of Prognostic Factors and Clinical Outcome of Vernal Keratoconjunctivitis in Childhood
Authors Shimokawa A, Ikeda A, Harada K , Takahashi R, Huang J, Tsukahara-Kawamura T , Ozaki H, Uchio E
Received 8 April 2024
Accepted for publication 15 August 2024
Published 23 August 2024 Volume 2024:18 Pages 2339—2347
DOI https://doi.org/10.2147/OPTH.S472826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Asami Shimokawa, Aya Ikeda, Kazuhiro Harada, Rie Takahashi, Jane Huang, Tomoko Tsukahara-Kawamura, Hiroaki Ozaki, Eiichi Uchio
Department of Ophthalmology, Fukuoka University School of Medicine, Fukuoka, Japan
Correspondence: Eiichi Uchio, Department of Ophthalmology, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku, Fukuoka, 814-0180, Japan, Tel +81 92 801 1011, Fax +81 92 865 4445, Email [email protected]
Purpose: Vernal keratoconjunctivitis (VKC) is a refractory ocular allergic disorder that mainly affects boys. Long-term follow-up has been rarely reported for VKC. We investigated the long-term clinical outcome of VKC to identify relevant clinical features of prognostic value based on follow-up for a median of 70 months.
Methods: In total, 45 consecutive patients clinically diagnosed with VKC aged 4 to 12 years at onset at the Department of Ophthalmology of Fukuoka University Hospital were included. Patients were treated with immunosuppressive eye drops without simultaneous corticosteroid eye drops, except for the occurrence of exacerbations. Collated variables were gender, age at onset, clinical score of ocular lesions (conjunctival giant papillae, limbal edema and corneal epithelial lesions) at the first visit, and clinical score of atopic dermatitis (AD) at baseline. Cumulative cure rate was estimated using Kaplan–Meier method. A binomial logistic predictive model was used to determine the most reliable clinical predictors of VKC outcome.
Results: The observation period ranged from 24 to 188 months, with median of 70 months. Among the 45 cases enrolled, all non-cured cases (14 cases) observed clinically were complicated by AD. Cumulative cure rate was 74.5% and 84.9% at eight- and ten-year follow-up, respectively. Ten-year cumulative cure rates of cases with and without AD were 50.5% and 100%, respectively, and a significant difference was found between these cumulative cure curves. Binomial regression analysis revealed that AD and gender were significantly related to worse outcome, and this binomial regression model had high sensitivity and specificity.
Conclusion: This study demonstrated that th eclinical outcomeof VKC might be predicted by several factors that can beobtained in the early clinical phase. Information on the long-term prognosis of VKC patients might play an important role for precision medicine for VKC in childhood.
Keywords: vernal keratoconjunctivitis, cumulative cure rate, atopic dermatitis, immunosuppressive eye drops, binomial logistic analysis
Introduction
Vernal keratoconjunctivitis (VKC) is an ocular disorder characterized by severe inflammation affecting both the cornea and conjunctiva that mainly affects boys in the first decade of life.1,2 Although the symptoms of VKC usually persist despite treatment, with seasonal deterioration, the condition generally resolves spontaneously with the onset of puberty.3 Some cases of VKC result in refractory atopic keratoconjunctivitis (AKC) in adulthood.4 Those cases complicated by atopic dermatitis (AD) may require therapeutic measures beyond this age into adulthood to control the disease, and permanent changes to the ocular surface and visual impairment may occur.5 Regarding these varying responses to medication observed in VKC,6 our group recently reported that VKC patients could be grouped into three clusters; traditional VKC, early-onset AKC/VKC and puberty-onset AKC, by cluster analysis.7 There were differences in the incidence of complications of AD and age at onset among the clusters, and puberty-onset AKC, which had the highest incidence of AD (71%), showed the worst outcome of the three clusters.7 This means that the prognosis may differ according to the disease phenotype of VKC.1
Long-term follow-up has been rarely reported for VKC because of the need for long-term clinical evaluation.1 Bonini et al reported that while VKC had chronic features, most cases showed favorable clinical responses (61.5%) in 151 patients with a median follow-up of 47 months, showing improvement with the use of topical antiallergic and anti-inflammatory eye drops, but almost 85% of patients needed to use topical ophthalmic steroids at some point during the course of the disease.1 Immunosuppressive eye drops, such as ciclosporin or tacrolimus, have been introduced for the management of VKC since around 2005 following Bonini and colleagues’ study,1 and these drugs have brought a paradigm shift in the management of this disease due to their effectiveness and few side effects.8–10 The prolonged use of immunosuppressive eye drops, namely proactive therapy, which has been reported previously11 and introduced widely for the long-term management of VKC recently, entails instillation of low doses of drugs to prevent recurrences; this is similar to the medical treatment of AD using tacrolimus ointment.12 Vichyanond et al commented that long-term follow-up studies of immunomodulators are needed to demonstrate the outcome of the treatment.13
We investigated the long-term clinical outcome of VKC treated and controlled in our hospital, which might reflect the recent changes in clinical features of VKC especially derived by the introduction of immunosuppressive eye drops. The most relevant clinical features that emerged from this evaluation were analyzed for their prognostic value based on long-term follow-up. The aim of the present study was also to evaluate the relationship between the cure/non-cure groups and clinical findings derived from long-term observation of VKC cases.
Materials and Methods
Patients
This study was approved by the Institutional Review Board of Fukuoka University School of Medicine (approval number: 2017Ml40) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was provided from a parent or legal guardian of all patients enrolled in this study. This retrospective noncomparative case series included a retrospective survey of 45 patients with VKC, who were consecutive juvenile patients aged 4 to 12 years at the onset of symptoms. They were diagnosed with VKC and treated and observed for at least two years in the Department of Ophthalmology of Fukuoka University Hospital (Fukuoka, Japan). The diagnosis of VKC was based on the Japanese guidelines for allergic conjunctival diseases.14 In summary, VKC was diagnosed by the presence of proliferative change, such as typical cobblestone excrescences (giant papillae of the upper palpebral conjunctiva more than 1 mm in size), corneal lesions (shield ulcer or plaque formation) and limbal lesions.15 A careful history was taken from each patient with regard to age, sex, place of residence, age at onset of the disease, seasonal variation and duration of the condition, previous personal or family history of allergic diseases, and the occurrence of previous or concomitant ocular or systemic diseases. Exclusion criteria were bacterial conjunctivitis, viral keratoconjunctivitis or other unclassified conjunctivitis such as phlyctenular keratoconjunctivitis and dry eye disease, and subjects wearing contact lenses were also excluded. Patients who dropped out from follow-up observation were excluded. Atopic dermatitis was diagnosed according to the criteria proposed by Hanifin and Rajka.16 The clinical severity of AD lesions was graded by dermatologists as (I) mild, (II) moderate, or (III) severe, according to the distribution of lesions, response to therapy, frequency of relapse, and the clinical course, as reported elsewhere, at their first visit to our hospital.17 Grade I, II and III were assigned a score of 1, 2 and 3, respectively, and non-atopic cases were assigned a score of 0 for statistical evaluation.
Ocular Clinical Grading
Clinical evaluation of ocular findings was carried out according to the ocular clinical grading system reported previously.14,18 Among ten objective ocular clinical findings, three findings, conjunctival giant papillae, corneal epithelial lesions and limbal edema, were each graded on a 4-point scale (0 = none, 1 = mild, 2 = moderate, and 3 = severe; for the left and right eyes separately in each case) (Table 1); reference clinical pictures are shown in the guidelines.14 The total score of the three findings, with a maximum of 9, taking the score of the more severe side in bilateral cases, was used as the clinical score. The clinical scores were recorded at each visit to our clinic for each eye separately; however, those at the first visit and final visit were adopted for this study.
 |
Table 1 Criteria for Clinical Evaluation of Allergic Ocular Findings |
Treatment and Clinical Observation
Patients with VKC were treated according to the guidelines;14 in brief, immunosuppressive eye drops, mainly tacrolimus (ciclosporin in some patients), were used as basic treatment without simultaneous corticosteroid eye drops, by increasing or decreasing the instillation (four times a day – once a week), combined with anti-allergic eye drops in some cases. This prolonged use of tacrolimus ophthalmic suspension 0.1% was reported as proactive therapy previously.11 For exacerbations of VKC, determined as worsening of the grade of giant conjunctival papillae, corneal epithelial lesions or limbal edema to at least moderate grade, meaning elevated giant papillae extending over less than half of the upper palpebral conjunctiva, superficial punctate keratitis with filamentary debris or limbal edema in 1/3 to 2/3 of the circumference (Table 1),18 local or systemic corticosteroid treatment was used for relief.
Evaluation of Outcome and Cumulative Cure Rate of VKC
In this long-term observation study, all patients were treated proactively with tacrolimus ophthalmic suspension 0.1%, and if they showed no recurrence and a clinical score of 0 for at least 1 year under proactive treatment, they were treated without tacrolimus ophthalmic suspension 0.1% (anti-allergic eye drops might also be used), and they were judged as cured if they showed no recurrence and a clinical score of 0 for at least another one-year follow-up observation (Group A). In contrast, cases that needed prolonged proactive treatment because of occasional recurrence beyond 16 years old were diagnosed as non-cured cases (Group B). Ocular examination, as an objective evaluation of disease status and the patient’s response to treatment, was performed by a single clinician (EU). The minimum observation period of two years in this study was based on the two-year observation period needed for the confirmation of clinical cure as noted above. Cumulative cure rate was estimated using Kaplan–Meier method.
Statistics
All statistical evaluations were performed using Excel Toukei-Kaiseki software (BellCurve, Tokyo, Japan). Comparisons of median values between two groups were performed using Mann–Whitney test. Differences in clinical characteristics and data between Group A and Group B were evaluated using univariate analysis. Cumulative cure curves were statistically compared between patient groups by Log rank test. To determine the most reliable clinical predictors of VKC outcome, multivariate analysis, a binomial logistic predictive model, was used. AIC (Akaike’s information criterion) was used to evaluate the reliability of the binomial logistic predictive model. AUC (area under the curve) was indicated by the ROC (receiver operating characteristic) curve to test the predictability of this analysis. All tests were two-sided, and p < 0.05 was considered to indicate statistical significance.
Results
Demographic Features of Patients
Baseline demographic and clinical characteristics of the 45 patients are shown in Table 2. Mean ± standard deviation (SD) age at onset of VKC symptoms as reported by the patients/parents was 7.78 ± 2.31 years (median, 8; range, 4–12 years). Mean (± standard deviation) age at the final visit was 15.2 ± 3.98 years (median, 15; range, 7–23 years). There were 37 males and 8 females with a male/female ratio of 4.6. The observation period ranged from 24 to 188 months, with median of 70 months. Twenty-two cases (53.3%) were observed for more than 70 months, and eight cases (17.8%) were followed for more than 100 months. The prevalence of AD was 44.4% (20/45). Comparing the mean clinical severity at the first visit (3.20) with that at the final visit (0.47), it was shown that the primary severe clinical appearance of VKC patients resolved after long-term treatment.
 |
Table 2 Demographic Features of Included Patients |
Cumulative Cure Rate of VKC
Cumulative cure curve of VKC is shown in Figure 1. Three-, five- and eight-year cumulative cure rates were 18.0%, 37.3% and 74.5%, respectively. Ten-year cumulative cure rate was 84.9%, and the cumulative cure rate showed no further increase after 10 years. Counting backwards, 15.1% of cases remained in a non-cured state after 10 years of observation in the cure curve. All non-cured cases (14 cases) observed clinically were complicated by AD. Cumulative cure curves of cases with and without AD are displayed in Figure 2. Five-year cumulative cure rates of cases with and without AD were 10.9% and 64.0%, respectively. Ten-year cumulative cure rates of cases with and without AD were 50.5% and 100%, respectively. All cases uncomplicated by AD resulted in clinical cure of VKC before 16 years of age. A statistically significant difference in cumulative cure curves was found between cases with and without AD (p < 0.001). Among AD cases, 6 cases (6/20; 33.3%) were cured before 16 years of age. Mean age of onset in cured cases with AD (6.17 ± 1.60 years) was significantly younger than that in non-cured cases with AD (8.21 ± 2.52 years) (p = 0.046). However, no significant difference was observed in the mean severity of AD between the two groups.
 |
Figure 1 Cumulative cure curve of vernal keratoconjunctivitis. This graph was estimated using Kaplan–Meier method. Ten-year cumulative cure rate was 84.9%. |
 |
Figure 2 Cumulative cure curves of vernal keratoconjunctivitis cases with and without atopic dermatitis. Solid and dashed lines represent cumulative cure rates of vernal keratoconjunctivitis cases with and without atopic dermatitis, respectively. A significant difference was found between the two groups. (p < 0.001). |
Changes in Cure Rate of VKC and Patients’ Age
The first cured case was observed at 7 years of age, and a single case was cured yearly from 8 to 10 years of age. In total, 27 cases were cured during the observation period. The number of cured cases by age and the cumulative rate of cured cases are shown in Figure 3. The peak in the number of cured cases was observed at 15 years of age (Figure 3).
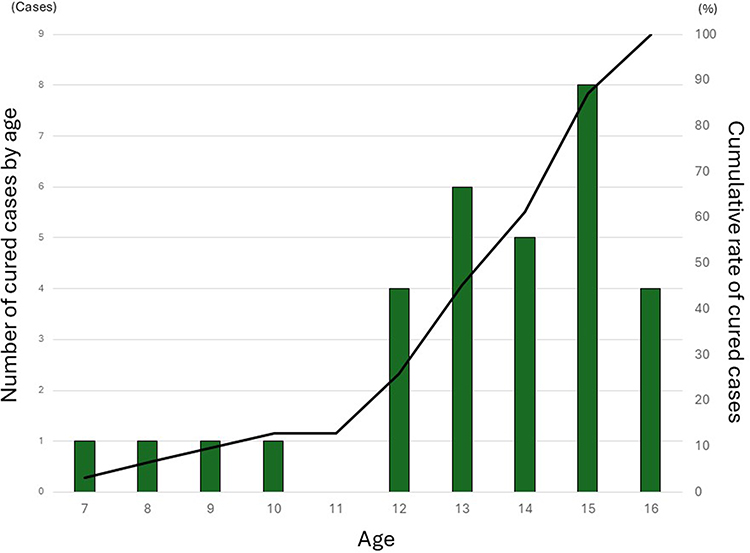 |
Figure 3 Number of cured vernal keratoconjunctivitis cases by age and cumulative rate of cured cases. The highest cure rate was observed at 15 years of age. The total number of cured cases was 31. |
Binomial Logistic Regression for Clinical Cure and Non-Cure Groups
The full results of binomial logistic regression are shown in Table 3. Regression identified that three factors; clinical score of conjunctival giant papillae, limbal edema at first visit, and age at onset, were not significantly related to clinical cure, although the complication of AD (present) and gender (male) were significantly related (p = 0.008, 0.032, respectively). The binomial logistic predictive model revealed that this model showed predictors of VKC cure with AIC of 37.9. The prediction model had sensitivity of 92.9%, specificity of 93.6% and AUC of 94.9%, as indicated by the ROC curve (Figure 4).
 |
Table 3 Binomial Logistic Regression for Clinical Cure of VKC |
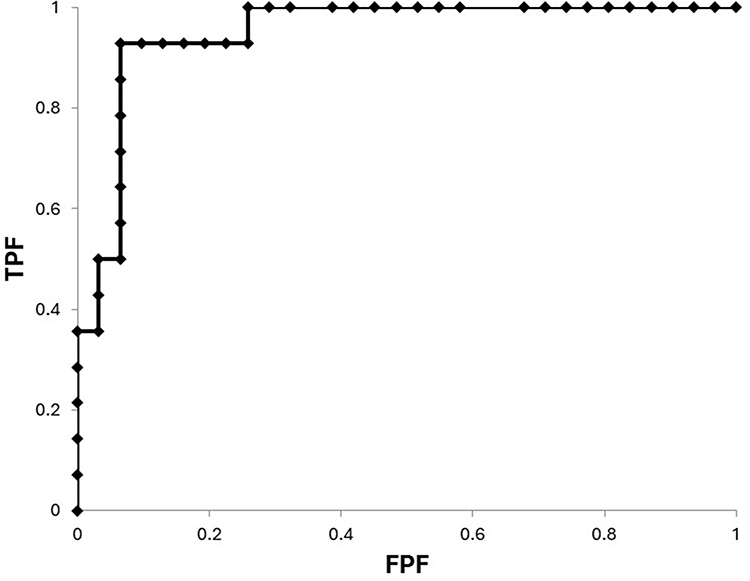 |
Figure 4 Performance of binomial logistic predictive model. ROC (receiver operating characteristic) curve of the predictive model is displayed. Abbreviations: TPF, true positive fraction (sensitivity); FPF, false positive fraction (1-specificity). |
Discussion
In this study, we evaluated the prognosis of VKC by long-term observation and found the cumulative cure rate at eight- and ten-year follow-up was 74.5% and 84.9%, respectively. Bonini et al reported that complete recovery was observed in 26.8%, whereas mild-to-moderate signs and symptoms were still evident in 35.4% after a median follow-up period of 42.0 months, in patients mainly treated with topical antiallergic and anti-inflammatory eyedrops.1 It is difficult to compare this result to that of our present study, because the cumulative cure rate of VKC was not evaluated in their study; however, the cumulative cure rate in the present study seemed higher. The main reason for this improvement in cure rate was the introduction of immunosuppressive eye drops.19 Proactive treatment with immunosuppressive eye drops might also contribute to decreasing the side effects of corticosteroid eye drops, which are frequently observed especially in children.20 The result that 15.1% of cases remained uncured after 10 years observation is an important novel finding in understanding the outcome of VKC from the life-course standpoint.
Although VKC was frequently observed as a single entity, the proportion of cases with associated atopic conditions has been reported to be as high as 41.5%,1 and the importance of AD has attracted attention among physicians.21 It is interesting that all non-cured patients beyond 16 years old were complicated by AD (14 cases), and the cumulative cure rate was significantly lower in cases with AD than in those without AD (Figure 2). This means that special attention is required for the treatment strategy for VKC with AD of juvenile onset. Historically, AKC is rarely recognized as a diagnostic entity before puberty and is thought to occur predominantly in adults,22 and a long-term follow-up study of AKC focused mainly on adult cases.23 A young patient with VKC-like symptoms and AD might be diagnosed with VKC,7 while Ebihara et al proposed that VKC cases with any history of AD should be diagnosed as AKC, regardless of patient age.9 Frankland et al, in an earlier study in the 1970s, noted that VKC was an atopic disease,24 and the prevalence of AD among cases of VKC ranged between 15% and 52% in the past literature.25–27 The rate in the present study, 44.4% (20/45), was in accordance with these studies. Combining these findings, we consider that VKC of juvenile age includes both cases with and without AD, because those cases showing giant papillae or limbal lesions could hardly be discriminated clinically. However, there was a significant difference in the long-term outcome between cases with and without AD. It should also be noted that six cases of VKC with AD were cured in this long-term follow-up; thus, the complication of AD did not necessarily indicate a refractory nature of VKC. This early-onset AD group of VKC cases had different prognostic features compared to the non-cured VKC group.
Binomial logistic regression for the clinical cure and non-cure groups showed that AD and gender were significant predictors of cure in VKC (Table 3). Meanwhile, the presence of corneal epithelial lesions was a possible clinical predictor of importance, meaning that cases with corneal lesions had an unfavorable prognosis regardless of the anatomical type (tarsal or bulbar). This result obtained with the binomial regression model is not consistent with the report by Bonini et al,1 who noted that factors related to a worse outcome of VKC were larger papillary size and bulbar type. The reason for the discrepancy between our study and that of Bonini et al is unclear, but Bonini et al did not include corneal damage in their statistical evaluation (univariate Cox regression analysis), and differences in the selection of variables and the statistical method might have influenced the results. It has been reported that increased levels and activity of matrix metalloproteinase (MMP)-1 and −9 and an imbalance between MMPs and tissue inhibitor of metalloproteinase (TIMP) may be involved in the pathogenesis of VKC, especially corneal epithelial involvement.28
The results of the present study also revealed the possibility that a not-cured outcome could be predicted by several factors that can be obtained in the early phase of clinical observation of VKC without the need for laboratory-based tests using tear or blood samples. Future re-evaluation of this binomial logistic regression analysis predictive model of VKC cases with a prospective study design will disclose its reliability and accuracy. The results of binomial regression analysis may give important clues to establish precision medicine for a long-term treatment plan for each case to reduce the frequency of acute recurrence, which considerably worsens patients’ quality of life and vision.
The present study had several limitations. First, the sample size was smaller than that of a previous comparable study1 and so the statistical power would be weaker. However, this was offset by the tight control over materials and methods, and by the observation by a single physician, reducing variability in the evaluation. VKC is not a common disorder, having a very low prevalence, and we have evaluated the adequacy of the sample population of this single center analysis carried out in a tertiary consultation hospital in our recent study.7 We are planning to carry out a multi-center, probably nation-based, prospective study for long-term observation of VKC in the future. Secondly, according to the definition of cure in VKC, the minimum observation duration was 24 months in this study. However, we cannot exclude the possibility that subjects belonging to the mildest spectrum of VKC, who responded promptly to the introduction of tacrolimus eye drops and in whom no further treatment was needed, were not included in this study. However, it can be accepted that the chronological analysis throughout the clinical course of refractory VKC cases has more clinical importance even if the milder spectrum of cases were not included.
In conclusion, several novel findings have been gained from this observational case series. In this chronological survey, the ten-year cumulative cure rate of VKC was 84.9%, and 15.1% of cases remained uncured after 10 years of observation in the cure curve. There was a significant difference in the long-term outcome between VKC cases with and without AD. Binomial regression analysis showed that AD and male gender were significantly related to a worse outcome. The binomial regression model had high sensitivity and specificity. The clinical outcome in VKC might be predicted by several factors that can be evaluated in the early clinical phase.
Acknowledgments
This work was supported by a Grant-in-Aid for Encouragement of Scientists (21K09709) from the Ministry of Education, Science, Sports, and Culture of Japan. We thank Dr W Gray for editing this manuscript.
Funding
The authors have no relevant financial or non-financial interests to disclose.
Disclosure
The authors have no competing interests to declare that are relevant to the content of this article.
References
1. Bonini S, Bonini S, Lambiase A, et al. Vernal keratoconjunctivitis revisited: a case series of 195 patients with long-term follow-up. Ophthalmology. 2000;107(6):1157–1163. doi:10.1016/S0161-6420(00)00092-0
2. Buckley RJ. Vernal keratoconjunctivitis. Int Ophthalmol Clin. 1988;28(4):303–308. doi:10.1097/00004397-198802840-00009
3. Foster CS. The pathophysiology of ocular allergy: current thinking. Allergy. 1995;50(Suppl 21):6–9. doi:10.1111/j.1398-9995.1995.tb04250.x
4. Bremond-Gignac D, Donadieu J, Leonardi A, et al. Prevalence of vernal keratoconjunctivitis: a rare disease? Br J Ophthalmol. 2008;92(8):1097–1102. doi:10.1136/bjo.2007.117812
5. Uchio E, Miyakawa K, Ikezawa Z, Ohno S. Systemic and local immunological features of atopic dermatitis patients with ocular complications. Br J Ophthalmol. 1998;82(1):82–87. doi:10.1136/bjo.82.1.82
6. Kosrirukvongs P, Vichyanond P, Wongsawad W. Vernal keratoconjunctivitis in Thailand. Asian Pac J Allergy Immunol. 2003;21(1):25–30.
7. Fujita H, Ueno T, Suzuki S, et al. Classification of subtypes of vernal keratoconjunctivitis by cluster analysis based on clinical features. Clin Ophthalmol. 2023;17:3271–3279. doi:10.2147/OPTH.S431798
8. Daniell M, Constantinou M, Vu HT, Taylor HR. Randomised controlled trial of topical ciclosporin A in steroid dependent allergic conjunctivitis. Br J Ophthalmol. 2006;90(4):461–464. doi:10.1136/bjo.2005.082461
9. Ebihara N, Ohashi Y, Uchio E, et al. A large prospective observational study of novel cyclosporine 0.1% aqueous ophthalmic solution in the treatment of severe allergic conjunctivitis. J Ocul Pharmacol Ther. 2009;25(4):365–372. doi:10.1089/jop.2008.0103
10. Ohashi Y, Ebihara N, Fujishima H, et al. A randomized, placebo-controlled clinical trial of tacrolimus ophthalmic suspension 0.1% in severe allergic conjunctivitis. J Ocul Pharmacol Ther. 2010;26(2):165–174. doi:10.1089/jop.2009.0087
11. Hirota A, Shoji J, Inada N, Shiraki Y, Yamagami S. Evaluation of clinical efficacy and safety of prolonged treatment of vernal and atopic keratoconjunctivitis using topical tacrolimus. Cornea. 2022;41(1):23–30. doi:10.1097/ICO.0000000000002692
12. Wollenberg A, Reitamo S, Girolomoni G, et al. Proactive treatment of atopic dermatitis in adults with 0.1% tacrolimus ointment. Allergy. 2008;63(7):742–750. doi:10.1111/j.1398-9995.2007.01406.x-i1
13. Vichyanond P, Pacharn P, Pleyer U, Leonardi A. Vernal keratoconjunctivitis: a severe allergic eye disease with remodeling changes. Pediatr Allergy Immunol. 2014;25(4):314–322. doi:10.1111/pai.12197
14. Miyazaki D, Takamura E, Uchio E, et al. Japanese guidelines for allergic conjunctival diseases 2020. Allergol Int. 2020;69(3):346–355. doi:10.1016/j.alit.2020.03.005
15. Neumann E, Gutmann MJ, Blumenkrantz N, Michaelson IC. A review of four hundred cases of vernal keratoconjunctivitis. Am J Ophthalmol. 1959;47(2):166–172. doi:10.1016/S0002-9394(14)76417-7
16. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol. 1980;60(Suppl 92):44–47. doi:10.2340/00015555924447
17. Ikezawa Z, Miyakawa K, Komatsu H, et al. A probable involvement of rice allergy in severe type of atopic dermatitis in Japan. Acta Derm Venereol. 1992;72(Suppl 176):103–107.
18. Uchio E, Kimura R, Migita H, Kozawa M, Kadonosono K. Demographic aspects of allergic ocular diseases and evaluation of new criteria for clinical assessment of ocular allergy. Graefes Arch Clin Exp Ophthalmol. 2008;246(2):291–296. doi:10.1007/s00417-007-0697-z
19. Leonardi A. Management of vernal keratoconjunctivitis. Ophthalmol Ther. 2013;2(2):73–88. doi:10.1007/s40123-013-0019-y
20. Ohji M, Kinoshita S, Ohmi E, Kuwayama Y. Marked intraocular pressure response to instillation of corticosteroids in children. Am J Ophthalmol. 1991;112(4):450–454. doi:10.1016/S0002-9394(14)76256-7
21. Bonini S, Coassin M, Sronni S, Lambiase A. Vernal keratoconjunctivitis. Eye (Lon d). 2004;18(4):345–351. doi:10.1038/sj.eye.6700675
22. Brémond-Gignac D, Nischal KK, Mortemousque B, Gajdosova E, Granet DB, Chiambaretta F. Atopic keratoconjunctivitis in children: clinical features and diagnosis. Ophthalmology. 2016;123(2):435–437. doi:10.1016/j.ophtha.2015.07.012
23. Power WJ, Tugal-Tutkun I, Foster CS. Long-term follow-up of patients with atopic keratoconjunctivitis. Ophthalmology. 1998;105(4):637–642. doi:10.1016/S0161-6420(98)94017-9
24. Frankland AW, Easty D. Vernal kerato-conjunctivitis: an atopic disease. Trans Ophthalmol Soc UK. 1971;91:479–482.
25. Kausar A, Akhtar N, Akbar N. Epidemiological aspects of allergic conjunctivitis. J Ayub Med Coll Abbottabad. 2022;34(1):135–140. doi:10.55519/JAMC-01-9432
26. Jongvanitpak R, Vichyanond P, Jirapongsananuruk O, Visitsunthorn N, Pacharn P. Clinical characteristics and outcomes of ocular allergy in Thai children. Asian Pac J Allergy Immunol. 2022;40(4):407–413. doi:10.12932/AP-160519-0564
27. Ajaiyeoba AI. Prevalence of atopic diseases in Nigerian children with vernal kerato-conjunctivitis. West Afr J Med. 2003;22(1):15–17. doi:10.4314/wajm.v22i1.27971
28. Leonardi A, Brun P, Abatangelo G, Plebani M, Secchi AG. Tear levels and activity of matrix metalloproteinase (MMP)-1 and MMP-9 in vernal keratoconjunctivitis. Invest Ophthalmol Vis Sci. 2003;44(7):3052–3058. doi:10.1167/iovs.02-0766
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.