")
Back to Journals » Journal of Inflammation Research » Volume 17
Long-Term Prognostic Value of Adipocytokines in Patients with Acute Coronary Syndrome: An 8-Year Clinical Prospective Cohort Study
Authors Wang X , Bu H, Wei C , Liu J, Qi Y , Shan W, Zhang Y, Sun L
Received 20 June 2024
Accepted for publication 25 September 2024
Published 2 October 2024 Volume 2024:17 Pages 6989—7003
DOI https://doi.org/10.2147/JIR.S483600
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Xinchen Wang,1,* Haiwei Bu,1,2,* Chen Wei,1 Jingyi Liu,1– 3 Yuewen Qi,3,4 Weichao Shan,1– 3 Ying Zhang,1– 3 Lixian Sun1– 3
1Department of Cardiology, The Affiliated Hospital of Chengde Medical University, Chengde, People’s Republic of China; 2The Cardiovascular Research Institute of Chengde, Chengde, People’s Republic of China; 3Hebei Key Laboratory of Panvascular Diseases, Chengde, People’s Republic of China; 4Central Laboratory of The Affiliated Hospital of Chengde Medical University, Chengde, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lixian Sun, Department of Cardiology, The Affiliated Hospital of Chengde Medical University, Chengde, China, No. 36, Nanyingzi Street, Shuangqiao District, Chengde, Hebei Province, People’s Republic of China, Tel +86 0314 227 9016, Fax +86 0314 227 4895, Email [email protected]
Purpose: To elucidate the predictive values of adipocytokines in patients with acute coronary syndrome (ACS).
Patients and Methods: Overall, 297 patients with ACS were consecutively enrolled in this prospective cohort study between June 2015 and July 2017 and completed follow-up with a median follow-up time of 6.5 years. For consistency, the last visit date was June 20, 2023. Serum levels of retinol-binding protein-4 (RBP4), interleukin-1β (IL-1β), monocyte chemoattractant protein 1(MCP-1), adrenomedullin (ADM), netrin 1 (NTN 1), and omentin were measured using enzyme-linked immunosorbent assay. Follow-up data were collected during clinical visits or through telephone interviews at 1, 3, 6, 12 months, and annually. The primary endpoint was defined as major adverse cardiovascular events (MACEs), including all-cause mortality, rehospitalization for percutaneous coronary intervention, and severe angina requiring rehospitalization.
Results: All biomarkers displayed a good diagnostic ability of MACEs. The Kaplan–Meier curve showed that the cumulative survival rates of high level of RBP4, IL-1β, and MCP-1 and low level of the ADM, NTN1, and omentin had lower cumulative survival rates (Log rank tests: all p< 0.05). After adjustment in the Cox hazard proportional model, the results were RBP4 ≥ 6.87 ng/mL, hazard ratio (HR)=2.512, p=0.003; IL-1β≥ 58.95 pg/mL, HR=3.809, p< 0.001; MCP-1 ≥ 401.75 pg/mL, HR=4.047, p< 0.001; ADM≤ 120.01 ng/mL, HR=3.930, p=0.008; NTN1 ≤ 63.7 pg/mL, HR=3.345, p=0.007; omentin ≤ 4.54 ng/mL, HR=2.830, p=0.004. P-values for interaction were > 0.05 in the sex, age, and dyslipidemia subgroups.
Conclusion: Pro-inflammation adipocytokines RBP4, IL-1β, and MCP-1 increased and anti-inflammation biomarkers ADM, NTN1, and omentin decreased were independently associated with a higher risk of MACEs in patients with ACS.
Keywords: acute coronary syndrome, adipocytokines, prognosis
Introduction
Coronary artery disease (CAD) is the global leading cause of death.1 Acute coronary syndrome (ACS) is a critical form of CAD, including unstable angina (UA), non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI).2 Patients with ACS experience high mortality and disability rates and poor prognosis, which impose a significant economic burden on society and families. Despite advancements in treatment strategies, such as percutaneous coronary intervention, these patients still have a poor prognosis.3 Therefore, conducting risk assessments and managing them based on risk stratification is crucial.
Adipose tissue dysfunction has emerged as a significant factor in the pathogenesis of various inflammatory conditions. Epicardial adipose tissue (EAT) and pericoronary adipose tissue (PCAT), which surround the heart and coronary arteries respectively, have garnered attention for their role in coronary inflammation and ACS.4 Unlike subcutaneous fat, EAT and PCAT are in direct contact with the coronary arteries, influencing vascular function through the secretion of inflammatory cytokines and mediators.4,5 Genetic polymorphisms and inflammatory pathways correlated with both psoriasis and cardiovascular disease, such as IL-23 and TNF-α. Metabolic syndrome is characterized by a cluster of metabolic disorders, including insulin resistance and central obesity, which are largely driven by adipose tissue dysfunction.6
Inflammation is critical in CAD development and progression. The adipose tissue is an energy storage and endocrine organ that secretes various bioactive molecules, known as adipokines, with anti-inflammatory or pro-inflammatory properties, including retinol-binding protein-4 (RBP4), interleukin-1β (IL-1β), monocyte chemoattractant protein 1(MCP-1), adrenomedullin (ADM), netrin 1 (NTN 1), and omentin. These adipocytokines are closely associated with inflammation and atherosclerosis. RBP4, IL-1β, and MCP-1 are pro-inflammation cytokines, whereas ADM, NTN1, and omentin are anti-inflammation cytokines.
RBP4 is associated with psoriasis vulgaris, pregnancies complicated with preeclampsia, oxidative stress, unstable carotid plaque in patients with cerebral infarction, and cardiometabolic diseases.7–10 It is vital in the development and severity of coronary lesions in patients with ACS.11–13 Higher circulating RBP4 levels are significantly associated with poor prognosis in patients with CAD.14 IL-1β activates endothelial cells, promotes the release of adhesion molecules, and causes circulating inflammatory cell aggregation, endothelial damage, and arteriosclerosis. MCP-1 is the main pro-inflammatory chemotactic factor; it causes coronary artery plate instability, promotes coronary heart disease development, and is crucial in cardiac injury, repair, and heart failure.15,16 It is also independently associated with thin-cap fibroatheroma, plaque burden, and necrotic core fraction.17 Previous studies have demonstrated that MCP-1 is an independent predictor of coronary artery ectasia, disease complexity, and atherosclerosis in patients with ACS and chest pain.18,19
ADM is a potent vasodilator peptide widely secreted in visceral adipose tissue, blood, adrenal medulla, and other tissues.20 It plays an anti-atherosclerosis role by inhibiting the proliferation of vascular smooth muscle cells. NTN 1 promotes atherosclerosis and CAD pathogenesis by inhibiting macrophage migration.21–23 Omentin, a recently identified fat deposition-specific adipokine, is highly and selectively expressed in visceral omental adipose tissues. As an anti-inflammation biomarker, it reduces vascular insulin resistance and hypertension and improves osteoarthritis progression by promoting anti-inflammatory responses and M2 macrophage polarization.24,25 Studies have found decreased omentin levels in patients with heart failure with preserved ejection fraction.26 Additionally, circulating omentin levels are closely associated with nonalcoholic fatty liver disease.27
However, the prognostic ability of adipocytokines, RBP4, IL-1β, MCP-1, ADM, NTN1, and omentin to predict the long-term outcomes of patients with ACS remains unclear. Therefore, in this study, we aimed to elucidate the predictive values of these adipocytokines in patients with ACS in the real world cohort study, and to provide enlightenments for future animal researches on drug targets.
Materials and Methods
Study Design and Population
This study was approved by the Ethics Committee of the Affiliated Hospital of Chengde Medical University (Number: CYFYLL2015006) and conducted following the Declaration of Helsinki. All participants provided informed consent.
Overall, 297 patients with ACS were consecutively enrolled at the Affiliated Hospital of Chengde Medical University between June 2015 and July 2017. The inclusion and exclusion criteria were consistent with those used in our previous study.28
The clinical types of ACS were diagnosed according to the universal American College of Cardiology guidelines.29–31The clinical types of ACS include unstable angina (UA), non-ST-segment elevation myocardial infarction (NSTEMI), and acute ST-segment elevation myocardial infarction (STEMI). UA is defined as myocardial ischemia at rest or on minimal exertion in the absence of acute cardiomyocyte injury or necrosis. Acute myocardial infarction (AMI) is defined as the detection of an increase and/or decrease of a cardiac biomarker, with at least one value above the 99th percentile of the upper reference limit, and with at least one of the following: symptoms of myocardial ischemia, new ischemic ECG changes, development of pathological Q waves on ECG, imaging evidence of loss of viable myocardium, or new regional wall motion abnormality, intracoronary thrombus detected on angiography or autopsy. On this basis, patients with persistent (>20min) ST-segment elevation in at least two contiguous is defined as STEMI. In contrast, patients without persistent ST-segment elevation are defined as NSTEM. Angiographic ACS is defined as stenosis ≥50% of one or more of the left main, left anterior descending artery, left circumflex artery, right coronary artery, or their main branches.
The study exclusion criteria were: stable coronary artery disease, coronary artery spasm or other secondary angina or myocardial infarction; cardiogenic shock; cardiac arrest; infectious diseases; malignant tumors; and severe heart diseases (eg, aortic dissection and hypertrophic cardiomyopathy), systemic inflammatory disorders, and hepatic and renal dysfunction.
Baseline Demographics and Clinical Characteristics
Cardiovascular postgraduates collected information on the demographics, blood biochemical indicators, echocardiography, and medication of patients with ACS during their hospitalization. Demographic characteristics included age, sex, dyslipidemia, hypertension, diabetes mellitus, ischemic stroke, family history of CAD, cardiogenic shock, and malignant arrhythmia. Blood biochemical indicators included white blood cell, hemoglobin, hematocrit, platelet count, neutrophils, lymphocyte, monocyte, albumin, aspartate aminotransferase, alanine aminotransferase, triglyceride, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, creatinine, serum uric acid and blood urea nitrogen level.
Hypertension was defined as systolic blood pressure≥140 mmHg, diastolic blood pressure≥90 mmHg at rest, or a previous diagnosis of hypertension with antihypertensive therapy.32 Type 2 diabetes mellitus was defined as the presence of diabetic symptoms and random blood glucose≥11.1 mmol/L, fasting plasma glucose≥7.0 mmol/L, 2-h oral glucose tolerance test levels ≥11.1 mmol/L, or no diabetes symptoms and at least two blood glucose readings meeting the above criteria.33 Dyslipidemia was defined as serum total cholesterol≥5.18 mmol/L, high-density lipoprotein cholesterol (HDL-C) ≤1.04 mmol/L, low-density lipoprotein cholesterol (LDL-C)≥3.37 mmol/L, triglyceride≥1.7 mmol/L or previous diagnosis of dyslipidemia.34
Enzyme-Linked Immunosorbent Assay
A professional nurse drew blood samples from the radial artery of all patients with ACS. The blood was collected the morning of coronary angiography, and patients were required to fast overnight. The blood samples were centrifuged at 3000 × g for 10 min, and the supernatant was collected and stored at−80°C. Serum levels of RBP4, IL-1β, MCP-1, ADM, NTN1, and omentin were tested using an enzyme-linked immunosorbent assay kit (Jiangsu Meimian Industrial Co., Ltd, China). Experimental personnel strictly followed the reagent manufacturer’s instructions for all operational procedures.
Follow-Up and Endpoints
A cardiovascular physician completed the follow-up, with each follow-up adhering to standardized principles. Data were collected during clinical visits or through telephone interviews at 1, 3, 6, 12 months, and annually. The last visit was June 20, 2023. The primary endpoint was defined as major adverse cardiovascular events (MACEs), including all-cause mortality, rehospitalization for PCI treatment, and severe angina requiring rehospitalization. For simplicity, rehospitalization was defined as rehospitalization for PCI treatment, and severe angina requiring rehospitalization in the following description.
Statistical Analysis
Normally distributed variables were presented as mean ± standard deviation, whereas non-normally distributed variables were presented as median with interquartile range. Differences in non-normally distributed continuous variables were analyzed using the Mann–Whitney U-test. Categorical variables were presented as numbers (%) and analyzed using the χ2 test. Receiver operating characteristic (ROC) analysis was used to determine the cut-off value and diagnostic ability of each biomarker. Kaplan–Meier curve and Log rank test were used to compare biomarker groups. Multivariate Cox hazard proportional hazards models were used for survival analysis to estimate hazard ratios for adipocytokines. Statistics analysis and plotting were performed using IBM SPSS Statistics for Windows (version 26; IBM Corp., Armonk, NY, USA) and GraphPad Prism 8.0 (GraphPad Software Inc, La Jolla, CA, USA). Statistical significance was set at p<0.05.
Results
Patients’ Characteristics
This study enrolled 297 patients with ACS with a median follow-up time of 2396 days (6.5 years). Plasma levels of RBP4, IL-1β, MCP-1, ADM, NTN1, and omentin were statistically significant (p<0.05) between the MACE and non-MACE groups (Figure 1). Compared with the non-MACEs group, the MACE group showed increased RBP4, IL-1β, and MCP-1 levels and decreased ADM, NTN1, and omentin levels.
 |
Figure 1 Comparison of serum adipocytokine levels in MACES and non-MACES groups.(A), RBP4.(B), IL-1β.(C), MCP-1.(D), ADM.(E), NTN1, and (F). Omentin. Abbreviations: MACEs, major adverse cardiovascular events; RBP4, retinol-binding protein-4; IL-1β, interleukin-1β; MCP-1, monocyte chemoattractant protein 1; ADM, adrenomedullin; NTN1, netrin 1. |
The baseline table showed that ejection fraction (EF%) was statistically significant; however, it was not statistically significant when converted into a second variable (EF%<50% or EF%≥50%) [29 (16.0%) vs 14 (12.1%), p=0.237]. The proportion of RBP4 ≥ 6.87 ng/mL, IL-1β≥ 58.95 pg/mL, MCP-1 ≥ 401.75 pg/mL, ADM ≤120.01 ng/mL, NTN1 ≤63.7 pg/mL, and omentin ≤4.54 ng/mL in the MACE group differed significantly from those of the non-MACE group (Table 1).
 |
Table 1 Baseline Patients’ Characteristics of the MACE and Non-MACE Groups |
Receiver Operating Characteristic Curve
Table 2 and Figure 2 present the ROC curve analyses to test the prognostic ability of MACEs using different cytokines. The cut-off value was calculated using ROC analysis.
 |
Table 2 Receiver Operating Characteristic Curve Analysis of Pro-Inflammatory and Anti-Inflammatory Adipocytokines for Diagnosing Acute Coronary Syndrome |
 |
Figure 2 ROC curves of adipocytokines for the diagnosis of MACEs. Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve; RBP4, retinol-binding protein-4; IL-1β, interleukin-1β; MCP-1, monocyte chemoattractant protein 1; ADM, adrenomedullin; NTN1, netrin 1. |
The area under the curve (AUC) for RBP4 was 0.609 (95% confidence interval (CI): 0.505–0.713) with an optimal diagnostic cut-off point of 6.87, sensitivity of 40.9% and specificity of 81.0%. The AUCs for IL-1β, MCP-1, ADM, NTN1, and omentin were 0.654 (95% CI: 0.539–0.768), 0.627 (95% CI: 0.511–0.742), 0.638 (95% CI: 0.522–0.754), 0.621 (95% CI: 0.518–0.724), and 0.633 (95% CI: 0.511–0.755), respectively, with optimal diagnostic cut-off points, sensitivities, and specificities of 58.95, 39.0%, and 94.4%, 401.75, 38.1%, and 92.2%, 120.01, 83.3%, and 45.0%, 63.7, 85.0% and 39.7%, and 4.54, 46.9%, and 81.0%, respectively.
Survival Analysis
The Kaplan–Meier curve was plotted to study the survival rates of each biomarker based on the cut-off values. The cumulative survival rates of RBP4 ≥ 6.87 ng/mL, IL-1β ≥ 58.95 pg/mL, and MCP-1 ≥ 401.75 were significantly lower in the lower groups (Figure 3A-C). ADM ≤ 120.01 ng/mL, NTN1 ≤ 63.7 pg/mL, and omentin ≤ 4.54 ng/mL groups had lower cumulative survival rates compared with the higher groups (Log rank tests: p < 0.05; Figure 4A-C).
 |
Figure 3 The Kaplan-Meier survival curves plotted by pro-inflammation adipocytokines in patients with ACS for MACEs. (A and D): RBP4; (B and E): IL-1β; (C and F): MCP-1. (A-C): predicting MACES and (D-F): predicting rehospitalization risk. Abbreviations: ACS, acute coronary syndrome; MACEs, major adverse cardiovascular events; RBP4, retinol-binding protein-4; IL-1β, interleukin-1β; MCP-1, monocyte chemoattractant protein. |
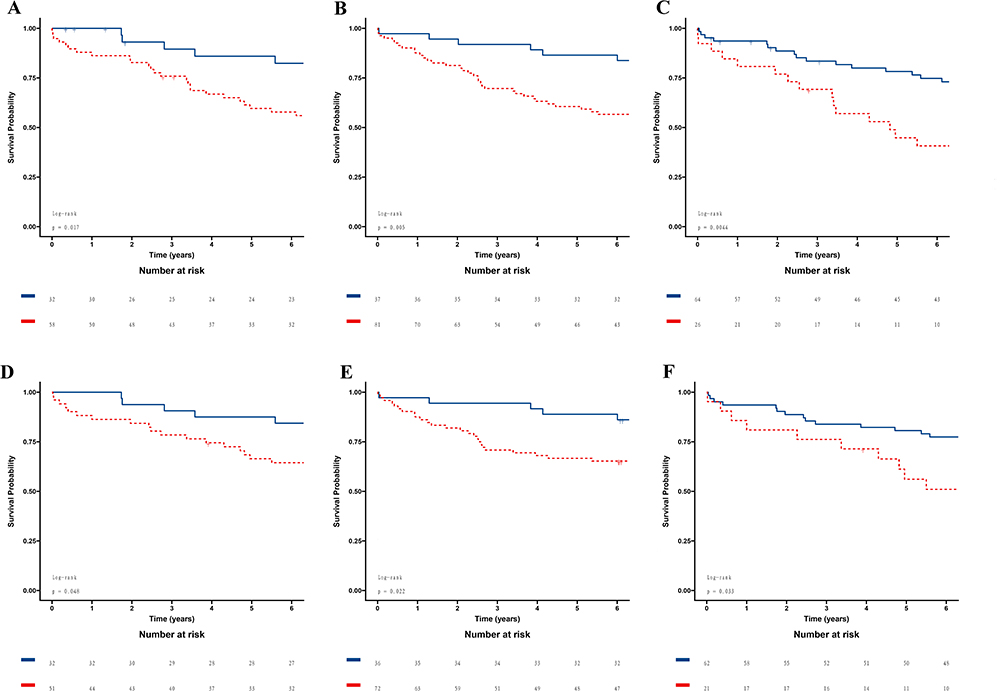 |
Figure 4 The Kaplan-Meier survival curves plotted by anti-inflammation adipocytokines in patients with ACS for rehospitalization. (A and D): ADM; (B and E): NTN1; (C and F): Omentin. (A-C): predicting MACES and (D-F): predicting rehospitalization risk. Abbreviations: ACS, acute coronary syndrome; MACEs, major adverse cardiovascular events; ADM, adrenomedullin; NTN1, netrin 1. |
Subsequently, we analyzed the cumulative survival rates of rehospitalization. The results showed that RBP4 ≥ 6.87 ng/mL, IL-1β≥ 58.95 pg/mL, MCP-1 ≥ 401.75 pg/mL (Figure 3D-E), ADM ≤120.01 ng/mL, NTN1 ≤63.7 pg/mL and omentin ≤4.54 ng/mL (Figure 4D-E) had lower cumulative survival rates, which were similar with the results mentioned above.
Cox Regression Analysis
In this study, we used two Cox regression models: Model 1 was a univariate model that included only adipocytokines. Model 2 was adjusted for hypertension (with or without), CAD family history (with or without), diabetes mellitus (with or without), age (≥65 years or <65 years), and sex (male or female) (Table 3).
 |
Table 3 Cox Hazard Proportional Model for Predictive Factors of MACEs |
First, we analyzed the correlation between these biomarkers and MACEs. The results of Model 1 were: RBP4 ≥ 6.87 ng/mL, HR=2.269, 95% CI:1.243–4.140, p=0.008; IL-1β≥ 58.95 pg/mL, HR=3.562, 95% CI:1.894–6.699, p<0.001; MCP-1 ≥ 401.75 pg/mL, HR=3.618, 95% CI:1.931–6.779, p<0.001; ADM ≤120.01 ng/mL, HR=3.043, 95% CI:1.164–7.954, p=0.023; NTN1 ≥63.7 pg/mL, HR:3.246, 95% CI:1.361–7.740, p=0.008; and omentin ≤ 4.54 ng/mL, HR=2.655 95% CI:1.321–5.334, p=0.006.
In Model 2, the results were RBP4 ≥ 6.87 ng/mL, HR=2.512, 95% CI: 1.359–4.644, p=0.003; IL-1β≥ 58.95 pg/mL, HR=3.809, 95% CI: 1.839–7.887, p<0.001; MCP-1 ≥ 401.75 pg/mL, HR=4.047, 95% CI: 2.117–7.735, p<0.001; ADM ≤120.01 ng/mL, HR=3.930, 95% CI: 1.435–10.768, p=0.008; NTN1 ≤63.7 pg/mL, HR=3.345, 95% CI: 1.399–8.000, p=0.007; and omentin ≤ 4.54 ng/mL, HR=2.830, 95% CI: 1.400–5.722, p=0.004.
Subsequently, we defined the outcome as rehospitalization. Rehospitalization was defined as rehospitalization for PCI treatment and severe angina requiring rehospitalization. We investigated these adipocytokines to predict rehospitalization risk. The results of Model 1 were: RBP4 ≥ 6.87 ng/mL, HR=2.398, 95% CI: 1.184–4.859, p=0.015; IL-1β≥ 58.95 pg/mL, HR=3.728, 95% CI: 1.890–7.351, p=<0.001; MCP-1 ≥ 401.75 pg/mL, HR=3.467, 95% CI: 1.752, 6.863, p<0.001; ADM ≤120.01 ng/mL, HR=2.618, 95% CI: 0.971–7.055, p=0.057; NTN1 ≤63.7 pg/mL, HR=2.923, 95% CI: 1.118–7.640, p=0.029; and omentin ≤ 4.54 ng/mL, HR=2.563, 95% CI: 1.136, 5.783, p=0.023.
In Model 2, the results were RBP4 ≥ 6.87 ng/mL, HR=2.473, 95% CI: 1.203–5.082, p=0.014; IL-1β≥ 58.95 pg/mL, HR=3.690, 95% CI: 1.730–7.872, p=0.001; MCP-1 ≥ 401.75 pg/mL, HR=3.868, 95% CI: 1.907–7.845, p<0.001; ADM ≤120.01 ng/mL, HR=3.120, 95% CI: 1.123–8.664, p=0.029; NTN1 ≤63.7 pg/mL, HR=3.136, 95% CI: 1.192–8.248, p=0.021; and omentin ≤ 4.54 ng/mL, HR=1.147, 95% CI: 2.607–5.923, p=0.022.
P for Interaction
The independent association between RBP4, IL-1β, MCP-1, ADM, NTN1, and omentin and the prognosis was assessed in subgroups based on age (≥65 or <65 years) (Figure 5A), sex (male or female) (Figure 5B), and hypertension (yes or no) (Figure 5C). Notably, all p-values for interaction in subgroup analysis were > 0.05. Further details are provided in Figure 5.
 |
Figure 5 Forest graphs based on subgroup analysis. (A) Age subgroup. (B) Sex subgroup. (C)Hypertension subgroup. Abbreviations: HR, hazard ratio; CI, confidence interval; RBP4, retinol-binding protein-4; IL-1β, interleukin-1β; MCP-1, monocyte chemoattractant protein 1; ADM, adrenomedullin; NTN1, netrin 1. |
Discussion
In this study, we investigated the association between serum levels of RBP4, IL-1β, MCP-1, ADM, NTN1, and omentin and the long-term outcomes of patients with ACS. We discovered that: (1) increasing serum levels of RBP4, IL-1β, and MCP-1 and decreasing serum levels of ADM, NTN1, and omentin were independently associated with a higher risk of MACEs in patients with ACS; (2) RBP4, IL-1β, MCP-1, ADM, NTN1, and omentin had good diagnostic value for MACEs in patients with ACS; (3) increasing serum levels of RBP4, IL-1β, MCP-1 and decreasing serum levels of ADM, NTN1, and omentin could predict rehospitalization risk for patients with ACS. To our knowledge, this is the first research to focus on the associations of serum levels of RBP4, IL-1β, MCP-1, ADM, NTN1, and omentin with long-term outcomes of patients with ACS.
In recent years, biomarkers have gained significant attention for their potential utility in ACS diagnosis, risk stratification, and prognosis assessment. High-sensitivity troponin (hs-cTn) has revolutionized the diagnosis of ACS due to its superior sensitivity and negative predictive value. This exploration encompasses both traditionally established markers like troponins and creatine kinase-MB, and newer candidates like natriuretic peptides, C-reactive protein, interleukin-6, and novel biomarkers such as endocan, galectin, and microRNAs.35 In a significant study examining the fibrinogen-to-albumin ratio (FAR), researchers investigated its prognostic value in patients with coronary three-vessel disease. FAR was found to have a positive association with all-cause mortality and MACEs.36 Similarly, another study emphasized the role of fibrinogen, albumin, and the FAR in predicting angiographic severity and clinical outcomes in ACS patients.37 Our present study found a modest association between these adipocytokines and MACEs risk. This research would offer insight into cardiac repair, myocardial cell necrosis, apoptosis, and fibrosis, making them potential targets for future drug development.
RBP4, an adipokine, plays a well-established role in atherosclerosis by inducing mitochondrial dysfunction, vascular oxidative damage, and accelerating the development of atherosclerosis.38–40 Higher RBP4 levels have been identified as an independent risk factor for CAD in Chinese populations.28,41 Our study revealed that RBP4 ≥ 5.78 ng/mL was correlated with MACEs risk in patients with ACS using the Cox hazard proportional model. The cumulative survival rate of increasing RBP4 was higher in the increasing RBP4 group than in the decreasing group.
Regarding IL-1β, previous studies have demonstrated that Puerarin-Tanshinone IIA regulated IL-1β and it suppressed atherosclerosis inflammatory plaque.42 However, its anti-atherosclerotic effects were weakened by naringenin and quercetin from Folium Artemisiae argyi.43 IL-1β is an inflammatory biomarker that reflects the degree of inflammation in cells or tissues. However, there was no study on the long-term, predictable ability of IL-1β in patients with ACS. IL-1β < 9.28 pg/mL was found to be an independent risk factor in the long-term prognosis of patients with ACS. Another research focus is the study of single nucleotide polymorphisms of IL-1β, which has been correlated with ACS, providing researchers with new directions and ideas.44,45
MCP-1 is closely correlated with CAD. Previous studies have found that MCP-1 could be a biomarker of subclinical atherosclerosis in women.46 The serum level of MCP-1 was higher in patients with ACS and lower in those with stable coronary disease.47 This interesting phenomenon still needs more research. The possible mechanism for adverse prognosis in patients with ACS with higher MCP-1 levels may be due to high levels of MCP-1 reflecting the burden of atherosclerotic disease and exerting prothrombotic effects leading to recurrent coronary events.48 MCP-1 plasma concentration is associated with MACEs in patients with CAD with persistent inflammation.49 However, some researchers consider MCP-1 to be unpredictable for 90 days of MACEs in patients with non-low-risk chest pain.50
NTN1 can suppress inflammatory macrophage apoptosis.51 It is cardioprotective and is considered a critical factor in atherosclerosis and ischemia-reperfusion injury.52 NTN1 had been found to be correlated with CAD.53 This novel biomarker could be a better diagnostic cytokine in patients with ACS. Our study found NTN1 < 65.90 pg/mL to be an independent risk factor in univariate and multivariate Cox proportional hazard models. This innovation can help identify high-risk patients with ACS after discharge. To our knowledge, this is the first study to assess the predictive ability of NTN1 in patients with ACS.
According to previous studies, ADM showed a close correlation with cardiovascular disease and was an independent predictor of future cardiovascular events in high-risk patients compared with C-reactive protein and adiponectin.54–56 ADM is also correlated with the severity of acute heart failure in patients with ACS and predicts clinically important 30-day outcomes in patients with acute heart failure.57 Involved in endothelial protection, ADM showed a significant interaction with renal function and outcome, being associated with the composite outcome only in patients with ACS with preserved kidney function.58,59 Our study found that ADM, as a prognostic biomarker, correlated with long-term outcomes in patients with ACS. Furthermore, a similar biomarker, named midregional pro-adrenomedullin (MR-proADM), is closely associated with ADM. Previous research has demonstrated that MR-proADM was an independent risk factor in the prognosis of patients with NSTEMI, and it correlated with acute heart failure and had many applications in the CAD field, such as risk stratification and predicting prognosis.60–64 Elevated plasma levels of MR-proADM could predict in-hospital mortality in patients with acute myocardial infarction complicated by cardiovascular shock.65 Therefore, more research should focus on the relationship between serum levels of MR-proADM and MACE risk.
Omentin, as an anti-inflammation biomarker, is mainly produced and secreted by vascular interstitial cells in visceral adipose tissues. Other tissues, such as endothelial cells, epicardial adipose tissue, and tumor cells, can also secrete it. Omentin possesses insulin-sensitizing, anti-inflammatory, anti-atherogenic, cardio-protective, and oxidative stress-decreasing effects.66 It participates in the autoimmune reaction, recognizes pathogens to exert an anti-inflammatory role and protects endothelial cells. It is also involved in anti-atherosclerosis, plaque stabilization, and enhancement of insulin sensitivity. Additionally, it improves endothelial cell function by increasing nitric oxide production through endothelial NO synthase.67,68
Moreover, the AUC for predicting ACS prognosis using the above inflammatory cytokines mentioned is > 0.6. Univariate and multivariate Cox proportional hazard models demonstrated that increasing serum levels of RBP4, IL-1β, and MCP-1 and decreasing serum levels of ADM, NTN1, and omentin were independently associated with MACE risk. Subgroup analysis confirmed these findings in age (≥65 or <65 years), sex (male or female), and hypertension (yes or no) subgroups. Therefore, we believe that serum elevated levels of RBP4, IL-1β, MCP-1, and decreased levels of ADM, NTN1, and omentin are closely associated with ACS prognosis and can serve as serological markers to help evaluate risk stratification in patients with ACS.
The present study had some limitations. First, our study was conducted at a single center, and had a small sample size, which hindered generalization to a wider population. Second, the serum levels of adipocytokines were evaluated only once after the patients were admitted, and information on the change in levels during hospitalization was limited. Third, the different parameters of echocardiography during the follow-up period were not been monitored. Fourth, this is an observational study, so the pathogenesis of the six adipocytokines in the acute coronary syndrome still needs to be explored in the future.
Conclusion
Inflammation adipocytokines RBP4, IL-1β, and MCP-1 with high serum levels and anti-inflammation biomarkers ADM, NTN1, and omentin with low serum levels were independently associated with a higher risk of MACEs in patients with ACS. RBP4, IL-1β, MCP-1, ADM, NTN1, and omentin may be used clinically as laboratory biomarkers for identifying high-risk patients with ACS.
Data Sharing Statement
All raw data will be made available at a reasonable request. Requests should be directed to the corresponding author.
Acknowledgments
The authors would like to thank the doctors and nurses of the Cardiology Research Team at the Affiliated Hospital of Chengde Medical University and the Hebei Key Laboratory of Panvascular Diseases for their assistance.
Funding
This study was supported by the Natural Science Foundation of Hebei Province (Grant number H2021406071) to Dr. Lixian Sun and the government-funded clinical medicine talent training project (Grant number ZF2023252) to Dr. Ying Zhang.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of acute coronary syndromes: a review. JAMA. 2022;327:662–675 doi:10.1001/jama.2022.0358
2. Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44:3720–3826 doi:10.1093/eurheartj/ehad191
3. Hoole SP, Bambrough P. Recent advances in percutaneous coronary intervention. Heart Br Card Soc. 2020;106:1380–1386 doi:10.1136/heartjnl-2019-315707
4. Napoli G, Pergola V, Basile P, et al. Epicardial and pericoronary adipose tissue, coronary inflammation, and acute coronary syndromes. J Clin Med. 2023;12(23):7212. doi:10.3390/jcm12237212
5. Mehta H, Narang T, Dogra S, et al. Cardiovascular considerations and implications for treatment in psoriasis: an updated review. Vascular Health Risk Manag. 2024;20:215–229. doi:10.2147/VHRM.S464471
6. Macut D, Ognjanović S, Ašanin M, et al. Metabolic syndrome and myocardial infarction in women. Curr Pharmaceutical Design. 2021;27(36):3786–3794. doi:10.2174/1381612827666210610114029
7. Gao G, Cui Y, Cheng H. Association between retinol binding protein-4 and psoriasis vulgaris: a systematic review and meta-analysis. Front Med. 2023;10:1208969. doi:10.3389/fmed.2023.1208969
8. Oluwamodupe C, Adeleye AO. Targeting retinol-binding protein 4 (RBP4) in the management of cardiometabolic diseases. Cardiovasc Toxicol. 2023;23(9–10):285–294. doi:10.1007/s12012-023-09803-8
9. Palalioglu RM, Erbiyik HI. Evaluation of maternal serum SERPINC1, E-selectin, P-selectin, RBP4 and PP13 levels in pregnancies complicated with preeclampsia. J Matern Fetal Neonatal Med. 2023;36(1):2183472. doi:10.1080/14767058.2023.2183472
10. Wang Q, Tian S, Xiao D, et al. Correlation of serum RBP4 level with oxidative stress and unstable carotid plaque in patients with cerebral infarction. Transl Neurosci. 2022;13(1):354–360. doi:10.1515/tnsci-2022-0252
11. Wang Y, Zhou C, Yu T, Zhao F. Correlation between changes in serum RBP4, hs-CRP, and IL-27 levels and rosuvastatin in the treatment of coronary heart disease. J Healthc Eng. 2021;2021:8476592. doi:10.1155/2021/8476592
12. Liu Y, Wang D, Chen H, Xia M. Circulating retinol binding protein 4 is associated with coronary lesion severity of patients with coronary artery disease. Atherosclerosis. 2015;238(1):45–51. doi:10.1016/j.atherosclerosis.2014.11.016
13. Nar G, Sanlialp SC, Nar R. Retinol binding protein 4 levels relate to the presence and severity of coronary artery disease. J Med Biochem. 2021;40(4):384–389. doi:10.5937/jomb0-28846
14. Qian K, Yan X, Xu C, Fang Y, Ma M. Association between circulating retinol-binding protein 4 and adverse cardiovascular events in stable coronary artery disease. Front Cardiovasc Med. 2022;9:829347. doi:10.3389/fcvm.2022.829347
15. Heil M, Ziegelhoeffer T, Wagner S, et al. Collateral artery growth (arteriogenesis) after experimental arterial occlusion is impaired in mice lacking CC-chemokine receptor-2. Circ Res. 2004;94(5):671–677. doi:10.1161/01.RES.0000122041.73808.B5
16. Gonzalez-Quesada C, Frangogiannis NG. Monocyte chemoattractant protein (MCP-1)/CCL2 as a biomarker in acute coronary syndromes. Curr Atheroscler Rep. 2009;11(2):131–138. doi:10.1007/s11883-009-0021-y
17. Cheng JM, Oemrawsingh RM, Akkerhuis KM, et al. Circulating chemokines in relation to coronary plaque characteristics on radiofrequency intravascular ultrasound and cardiovascular outcome. Biomarkers. 2014;19(7):611–619. doi:10.3109/1354750X.2014.957725
18. Franco-Peláez JA, Martín-Reyes R, Pello-Lázaro AM, et al. Monocyte chemoattractant protein-1 is an independent predictor of coronary artery ectasia in patients with acute coronary syndrome. J Clin Med. 2020;9(9):3037. doi:10.3390/jcm9093037
19. Martín-Reyes R, Franco-Peláez JA, Lorenzo Ó, et al. Plasma levels of monocyte chemoattractant protein-1, n-terminal fragment of brain natriuretic peptide and calcidiol are independently associated with the complexity of coronary artery disease. PLoS One. 2016;11(5):e0152816. doi:10.1371/journal.pone.0152816
20. Kitamura K, Kangawa K, Kawamoto M, et al. Adrenomedullin: a novel hypotensive peptide isolated from human pheochromocytoma. Biochem Biophys Res Commun. 1993;192:553–560 doi:10.1006/bbrc.1993.1451
21. Bruikman CS, Van Gils JM. Netrin-1 in coronary artery disease (CAD): mechanism of action and potential as a therapeutic target. Expert Opin Ther Targets. 2019;23(9):729–731. doi:10.1080/14728222.2019.1653280
22. Gurses KM, Ozmen F, Kocyigit D, et al. Netrin-1 is associated with macrophage infiltration and polarization in human epicardial adipose tissue in coronary artery disease. J Cardiol. 2017;69(6):851–858. doi:10.1016/j.jjcc.2016.08.016
23. Moore KJ, Fisher EA. Macrophages, atherosclerosis and the potential of netrin-1 as a novel target for future therapeutic intervention. Future Cardiol. 2012;8(3):349–352. doi:10.2217/fca.12.30
24. Okamura Y, Adachi K, Niijima R, et al. Human omentin-1 reduces vascular insulin resistance and hypertension in Otsuka Long-Evans Tokushima fatty rats. Naunyn Schmiedebergs Arch Pharmacol. 2024;397(5):3379–3387. doi:10.1007/s00210-023-02795-w
25. Ko CY, Lin YY, Achudhan D, et al. Omentin-1 ameliorates the progress of osteoarthritis by promoting IL-4-dependent anti-inflammatory responses and M2 macrophage polarization. Int J Biol Sci. 2023;19(16):5275–5289. doi:10.7150/ijbs.86701
26. Su Z, Tian S, Liang W, Wu L. Association between omentin-1 and heart failure with preserved ejection fraction in Chinese elderly patients. Clin Cardiol. 2023;47:e24181 doi:10.1002/clc.24181
27. Khodashahi R, Aliakbarian M, Ferns GA, et al. The association between circulating adipocytokine omentin levels and nonalcoholic fatty liver disease: a systematic review and meta-analysis. Curr Mol Med. 2023. doi:10.2174/1566524023666230913105910
28. Liu T, Han C, Sun L, et al. Association between new circulating pro-inflammatory and anti-inflammatory adipocytokines with coronary artery disease. Coron Artery Dis. 2019;30(7):528–535. doi:10.1097/MCA.0000000000000778
29. Taylor J. Updated ESC Guidelines for managing patients with suspected non-ST-elevation acute coronary syndromes. Eur Heart J. 2011;32(23):2909–2910. doi:10.1093/eurheartj/ehr319
30. Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541–2619. doi:10.1093/eurheartj/ehu278
31. Hamm CW, Bassand JP, Agewall S, et al. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011;32(23):2999–3054. doi:10.1093/eurheartj/ehr236
32. Jennings GLR. A new guideline on treatment of hypertension in those with coronary artery disease: scientific statement from the American heart association, American college of cardiology, and American society of hypertension about treatment of hypertension in patients with coronary artery disease. Heart Lung Circ. 2015;24(11):1037–1040. doi:10.1016/j.hlc.2015.05.022
33. Colberg SR, Sigal RJ, Fernhall B, et al. Exercise and type 2 diabetes: the American college of sports medicine and the American diabetes association: joint position statement. Diabetes Care. 2010;33(12):e147–167. doi:10.2337/dc10-9990
34. Ray KK, Kastelein JJP, Boekholdt SM, et al. The ACC/AHA 2013 guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular disease risk in adults: the good the bad and the uncertain: a comparison with ESC/EAS guidelines for the management of dyslipidaemias 2011. Eur Heart J. 2014;35(15):960–968. doi:10.1093/eurheartj/ehu107
35. Katsioupa M, Kourampi I, Oikonomou E, et al. Novel biomarkers and their role in the diagnosis and prognosis of acute coronary syndrome. Life. 2023;13(10):1992. doi:10.3390/life13101992
36. Li X, Wang Z, Zhu Y, et al. Prognostic value of fibrinogen-to-albumin ratio in coronary three-vessel disease. J Inflamm Res. 2023;16:5767–5777. doi:10.2147/JIR.S443282
37. Makkar K, Sharma YP, Batta A, et al. Role of fibrinogen, albumin and fibrinogen to albumin ratio in determining angiographic severity and outcomes in acute coronary syndrome. World J Cardiol. 2023;15(1):13–22. doi:10.4330/wjc.v15.i1.13
38. Zhou W, Ye SD, Wang W. Elevated retinol binding protein 4 levels are associated with atherosclerosis in diabetic rats via JAK2/STAT3 signaling pathway. World J Diabetes. 2021;12(4):466–479. doi:10.4239/wjd.v12.i4.466
39. Zhou W, Ye S, Li J. Expression of retinol binding protein 4 and nuclear factor-κB in diabetic rats with atherosclerosis and the intervention effect of pioglitazone. Exp Ther Med. 2016;12(2):1000–1006. doi:10.3892/etm.2016.3340
40. Wang J, Chen H, Liu Y, Zhou W, Sun R, Xia M. Retinol binding protein 4 induces mitochondrial dysfunction and vascular oxidative damage. Atherosclerosis. 2015;240(2):335–344. doi:10.1016/j.atherosclerosis.2015.03.036
41. Dong H, Li X, Tang Y. Serum retinol-binding protein-4 level is a high risk factor for coronary heart disease in Chinese. Clin Lab. 2015;61(11/2015):1675–1678. doi:10.7754/Clin.Lab.2015.141216
42. Xu J, Tian Z, Li Z, et al. Puerarin-Tanshinone IIA suppresses atherosclerosis inflammatory plaque via targeting succinate/HIF-1α/IL-1β axis. J Ethnopharmacol. 2023;317:116675. doi:10.1016/j.jep.2023.116675
43. Zhang L, Yang Z, Li X, Hua Y, Fan G, He F. Anti-atherosclerotic effects of naringenin and quercetin from folium artemisiae argyi by attenuating Interleukin-1 beta (IL-1β)/ matrix metalloproteinase 9 (MMP9): network pharmacology-based analysis and validation. BMC Complement Med Ther. 2023;23(1):378. doi:10.1186/s12906-023-04223-1
44. Soylu O, Yildirim A, Coker A, Tezel T, List EO, Arman A. Interleukin-1B (−511) gene polymorphism is associated with acute coronary syndrome in the Turkish population. Eur Cytokine Netw. 2008;19(1):42–48. doi:10.1684/ecn.2008.0119
45. Stegger JG, Schmidt EB, Tjønneland A, et al. Single nucleotide polymorphisms in IL1B and the risk of acute coronary syndrome: a Danish case-cohort study. PLoS One. 2012;7(7):e36829. doi:10.1371/journal.pone.0036829
46. Basurto L, Gregory MA, Hernández SB, et al. Monocyte chemoattractant protein-1 (MCP-1) and fibroblast growth factor-21 (FGF-21) as biomarkers of subclinical atherosclerosis in women. Exp Gerontol. 2019;124:110624. doi:10.1016/j.exger.2019.05.013
47. Matsumori A, Furukawa Y, Hashimoto T, et al. Plasma levels of the monocyte chemotactic and activating factor/monocyte chemoattractant protein-1 are elevated in patients with acute myocardial infarction. J Mol Cell Cardiol. 1997;29(1):419–423. doi:10.1006/jmcc.1996.0285
48. Dewald O, Ren G, Duerr GD, et al. Of mice and dogs: species-specific differences in the inflammatory response following myocardial infarction. Am J Pathol. 2004;164(2):665–677. doi:10.1016/S0002-9440(10)63154-9
49. Blanco-Colio LM, Méndez-Barbero N, Pello Lázaro AM, et al. MCP-1 predicts recurrent cardiovascular events in patients with persistent inflammation. J Clin Med. 2021;10(5):1137. doi:10.3390/jcm10051137
50. Ashburn NP, Snavely AC, Allen BR, et al. Monocyte chemoattractant protein-1 is not predictive of cardiac events in patients with non-low-risk chest pain. Emerg Med J EMJ. 2022;39(11):853–858. doi:10.1136/emermed-2021-211266
51. Cynn E, Li DY, O’Reilly ME, et al. Human macrophage long intergenic noncoding RNA, SIMALR, suppresses inflammatory macrophage apoptosis via NTN1 (Netrin-1). Arterioscler Thromb Vasc Biol. 2023;43(2):286–299. doi:10.1161/ATVBAHA.122.318353
52. Van Gils JM, Derby MC, Fernandes LR, et al. The neuroimmune guidance cue netrin-1 promotes atherosclerosis by inhibiting the emigration of macrophages from plaques. Nat Immunol. 2012;13(2):136–143. doi:10.1038/ni.2205
53. Inderjeet K, Adole PS, Vinod KV, Pillai AA. Association between serum netrin-1, netrin-4 and risk of the acute coronary syndrome in patients with type 2 diabetes mellitus-A pilot study. Indian Heart J. 2022;74(1):72–75. doi:10.1016/j.ihj.2021.11.186
54. Carbone RG, Puppo F. The role of adrenomedullin in acute coronary syndrome. Int J Cardiol. 2023;376:22–23. doi:10.1016/j.ijcard.2023.01.089
55. Nishikimi T, Shibasaki I, Iida H, et al. Molecular forms of adrenomedullin in pericardial fluid and plasma in patients with ischaemic heart disease. Clin Sci. 2002;102(6):669–677. doi:10.1042/cs1020669
56. Nishida H, Horio T, Suzuki Y, et al. Plasma adrenomedullin as an independent predictor of future cardiovascular events in high-risk patients: comparison with C-reactive protein and adiponectin. Peptides. 2008;29(4):599–605. doi:10.1016/j.peptides.2007.12.006
57. Self WH, Storrow AB, Hartmann O, et al. Plasma bioactive adrenomedullin as a prognostic biomarker in acute heart failure. Am J Emerg Med. 2016;34(2):257–262. doi:10.1016/j.ajem.2015.10.033
58. Mörtberg J, Salzinger B, Lundwall K, et al. Prognostic importance of biomarkers associated with haemostatic, vascular and endothelial disturbances in acute coronary syndrome patients in relation to kidney function. Int J Cardiol. 2023;373:64–71. doi:10.1016/j.ijcard.2022.12.005
59. Edfors R, Lindhagen L, Spaak J, et al. Use of proteomics to identify biomarkers associated with chronic kidney disease and long-term outcomes in patients with myocardial infarction. J Intern Med. 2020;288(5):581–592. doi:10.1111/joim.13116
60. O’Malley RG, Bonaca MP, Scirica BM, et al. Prognostic performance of multiple biomarkers in patients with non–ST-segment elevation acute coronary syndrome: analysis from the MERLIN-TIMI 36 trial (metabolic efficiency with ranolazine for less ischemia in non-ST-elevation acute coronary syndromes-thrombolysis in myocardial infarction 36. J Am Coll Cardiol. 2014;63(16):1644–1653. doi:10.1016/j.jacc.2013.12.034
61. Potocki M, Ziller R, Mueller C. Mid-regional pro-adrenomedullin in acute heart failure: a better biomarker or just another biomarker? Curr Heart Fail Rep. 2012;9(3):244–251. doi:10.1007/s11897-012-0096-6
62. Wild PS, Schnabel RB, Lubos E, et al. Midregional proadrenomedullin for prediction of cardiovascular events in coronary artery disease: results from the AtheroGene study. Clin Chem. 2012;58(1):226–236. doi:10.1373/clinchem.2010.157842
63. Tzikas S, Keller T, Ojeda FM, et al. MR-proANP and MR-proADM for risk stratification of patients with acute chest pain. Heart. 2013;99(6):388–395. doi:10.1136/heartjnl-2012-302956
64. Funke-Kaiser A, Mann K, Colquhoun D, et al. Midregional proadrenomedullin and its change predicts recurrent major coronary events and heart failure in stable coronary heart disease patients: the LIPID study. Int J Cardiol. 2014;172(2):411–418. doi:10.1016/j.ijcard.2014.01.064
65. Supeł K, Kacprzak M, Zielińska M. The prognostic value of MR-proadrenomedullin in patients with acute coronary syndrome complicated by cardiogenic shock. Biomarkers. 2017;22(3–4):296–303. doi:10.1080/1354750X.2016.1252962
66. Hussein AA, Ahmed NA, Sakr HI, Atia T, Ahmed OM. Omentin roles in physiology and pathophysiology: an up-to-date comprehensive review. Arch Physiol Biochem. 2023;1–14. doi:10.1080/13813455.2023.2283685
67. Saely CH, Leiherer A, Muendlein A, et al. High plasma omentin predicts cardiovascular events independently from the presence and extent of angiographically determined atherosclerosis. Atherosclerosis. 2016;244:38–43. doi:10.1016/j.atherosclerosis.2015.10.100
68. Shibata R, Ouchi N, Kikuchi R, et al. Circulating omentin is associated with coronary artery disease in men. Atherosclerosis. 2011;219(2):811–814. doi:10.1016/j.atherosclerosis.2011.08.017
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.