")
Back to Journals » Clinical Ophthalmology » Volume 19
Long-Term Surgical Outcome of Trabeculectomy with Mitomycin C: A Comparison Between Primary and Secondary Glaucoma in Thailand
Authors Arampinyokul P, Rojananuangnit K
Received 26 January 2025
Accepted for publication 10 April 2025
Published 17 April 2025 Volume 2025:19 Pages 1299—1311
DOI https://doi.org/10.2147/OPTH.S518659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ployroung Arampinyokul,1,2,* Kulawan Rojananuangnit1,*
1Department of Ophthalmology, Mettapracharak (Wat Rai Khing) Hospital, Nakhon Pathom, Thailand; 2Mahidol Bumrungrak Nakhonsawan Medical Center, Nakhon Sawan, Thailand
*These authors contributed equally to this work
Correspondence: Kulawan Rojananuangnit, Department of Ophthalmology, Mettapracharak (Wat Rai Khing) Hospital, 52 Moo 2 Rai Khing Sam Pran, Nakhon Pathom, 73210, Thailand, Email [email protected]
Purpose: This study aimed to evaluate the long-term surgical outcomes of trabeculectomy with mitomycin C (MMC) and identify factors associated with surgical failure in Thai patients with primary and secondary glaucoma.
Methods: This retrospective study included 421 eyes from 397 patients with glaucoma who underwent trabeculectomy with MMC from January 1, 2012, to December 31, 2015. The patients’ demographics, baseline characteristics, ocular parameters, and postoperative outcomes were analyzed. Surgical success was classified into complete success (IOP = 4– 21 mmHg without anti-glaucoma medication), qualified success (IOP = 4– 21 mmHg with medication), and failure (IOP > 21 mmHg or < 4 mmHg). Factors associated with surgical failure were assessed using Cox regression analysis.
Results: The cumulative probability of complete or qualified success at 8 years was 65.9% (95% CI: 59.9%, 71.9%); however, a significantly higher success rate was observed in the primary glaucoma group (75.1%) than in the secondary glaucoma group (47.4%) (p < 0.001). The secondary glaucoma group, particularly those with secondary closed-angle glaucoma, had the lowest success rates. Preoperative IOP, number of anti-glaucoma medications, and visual acuity were significantly different between the two groups. Etiologic factors associated with surgical failure included pseudo-exfoliation glaucoma (adjusted HR 3.23), neovascular glaucoma (adjusted HR 2.87), and secondary angle closure glaucoma (adjusted HR 2.62). Late complications were more prevalent in patients with secondary glaucoma than in those with primary glaucoma and included decreased visual acuity (5.43% vs 10.29%), hypotony (0.26% vs 1.14%), corneal decompensation (1.82% vs 3.40%), and bleb-related infection (0.19%).
Conclusion: Trabeculectomy with MMC remains an effective surgical option for primary glaucoma, demonstrating better long-term outcomes compared to its outcomes in patients with secondary glaucoma. Risk factors for surgical failure include specific glaucoma etiologies. These findings would personalize management strategies to optimize surgical approaches based on predictive factors for surgical success.
Plain Language Summary: The study looked at how well a type of eye surgery called trabeculectomy works for people with glaucoma, a condition that causes high pressure in the eye. We reported how successful the surgery was over 8 years and what might make it more likely to fail.
The study found that trabeculectomy surgery works better for people with primary glaucoma than for those with secondary glaucoma (glaucoma caused by other health issues). After 8 years, about 75% of primary glaucoma patients had successful results, while only 47% of secondary glaucoma patients did. Secondary glaucoma patients also had more postsurgery problems, like vision loss and infections. These findings would help doctors tailor treatment plans and choose the best surgical approach based on factors that predict surgery success.
Keywords: close-angle glaucoma, neovascular glaucoma, open-angle glaucoma, postintraocular surgery glaucoma, pseudoexfoliation glaucoma, uveitic glaucoma
Introduction
Glaucoma is one of the leading causes of blindness in Thailand and worldwide. By 2040, the prevalence of glaucoma is projected to reach 111.8 million, driven primarily by an aging population.1 In Thailand, the prevalence of glaucoma is 4.07% among individuals aged 40 years and older, increasing to nearly 5% in those over 50 years of age.2–4
Glaucoma is a chronic optic neuropathy characterized by the gradual deterioration of the optic nerve, often associated with functional visual field damage. Abnormally high intraocular pressure (IOP) is a significant risk factor for the disease.5,6 The primary aim of glaucoma treatment is to halt disease progression and prevent ongoing damage to the optic nerve, which can lead to permanent visual field loss and irreversible blindness. Current treatment primarily focuses on reducing IOP. However, several factors must be considered in managing glaucoma patients, including the stage of the disease, quality of life, patient factors, and life expectancy. For patients with early to moderate stages of the disease, anti-glaucoma medications or selective laser trabeculoplasty (SLT) are typically recommended.7,8 In contrast, surgery is recommended for patients with advanced stages of glaucoma who cannot tolerate medications or whose IOP remains insufficiently controlled, leading to the deterioration of both the patient’s functional visual field and structural optic nerve.6–9
While novel minimally invasive glaucoma surgeries (MIGS) have shown promising outcomes, trabeculectomy remains the standard surgical option for controlling IOP by bypassing the aqueous humor to the subconjunctival space.10–12 The application of anti-metabolites, such as Mitomycin C (MMC) and 5-fluorouracil (5-FU), can modify wound healing processes and increase the success rate of surgery.13 The overall success rate of trabeculectomy with MMC is reported to be 80–90% at 1 year; however, this decreases to 60–73% during longer-term follow-ups of 5–6 years.14 Differences in race and glaucoma etiology may also affect the success rates of surgery.15–19 There is a gap in the current understanding of the long-term outcomes of trabeculectomy with mitomycin C (MMC), particularly within the Thai population and across various glaucoma etiologies. This study aims to evaluate the surgical outcomes of trabeculectomy with MMC in patients with both primary and secondary glaucoma, as well as to identify factors associated with surgical failure. The findings may contribute to optimizing treatment protocols and enhancing the accuracy of prognostic assessments for glaucoma patients in Thailand.
Materials and Methods
This retrospective study included patients with glaucoma. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Mettapracharak (Wat Rai Khing) Research Ethics Committee. The study was also conducted in line with the International Conference on Harmonization of Good Clinical Practice (ICH-GCP) guidelines (COA013/2565). The ethics committee waived the need to obtain informed consent, as all data were anonymized and kept confidential.
The medical records of patients with glaucoma who underwent their initial trabeculectomy with MMC between January 1, 2012, and December 31, 2015, were reviewed retrospectively. The inclusion criteria included cases of patients with glaucoma who had uncontrolled IOP, underwent primary trabeculectomy with MMC augmentation, and had been followed up at the Department of Ophthalmology, Mettapracharak (Wat Rai Khing) Hospital, Thailand. The exclusion criteria included patients who had previously undergone any glaucoma surgery.
Demographic data, including sex, age, underlying conditions, history of glaucoma treatment, and type of glaucoma, were collected from the patient records. Baseline and follow-up data were recorded, including LogMAR visual acuity, IOP, the number of anti-glaucoma medications, and details of laser and bleb care procedures performed postoperatively. Complications and any further surgical management were also documented. Ocular parameters were assessed preoperatively and during follow-up visits, including the vertical cup-to-disc ratio (VCDR) and visual field test results, such as the mean deviation (MD), pattern standard deviation (PSD), and visual field index (VFI).
Patients with glaucoma were categorized into two groups based on the disease etiology: the primary glaucoma group and the secondary glaucoma group. Trabeculectomy is indicated for patients with uncontrolled IOP despite the maximum tolerated glaucoma medications, particularly when there is evidence of disease progression, both structurally and functionally. Trabeculectomy with 0.04% MMC was performed by eight glaucoma specialists at Mettapracharak Hospital, utilizing a fornix-based conjunctival flap. Although the fundamental approach remained consistent, there were slight variations in individual techniques, and the duration of MMC application ranged from 2 to 4 minutes among different surgeons.
Postoperative care following trabeculectomy included the application of topical steroids 4–8 times daily for 3–6 months with adjustments made based on the level of inflammation and the characteristics of the bleb. Additionally, topical antibiotics were prescribed to be used four times daily for 1–2 months to prevent infection. Postoperative follow-up for patients involved examinations 1 week postoperatively, followed by follow-up visits every 1–2 weeks for the first month and then every 1–2 months thereafter. To ensure a functional bleb, interventions such as laser suture lysis or needling procedures were performed as needed. If IOP remained uncontrolled, additional management strategies, including topical and/or oral anti-glaucoma medications or further glaucoma procedures, were considered to achieve optimal IOP control.
Surgical outcomes were categorized into three groups: complete success (IOP of 4–21 mmHg without anti-glaucoma medication), qualified success (IOP of 4–21 mmHg with additional glaucoma medications), and failure (IOP above 21 mmHg despite anti-glaucoma medications or IOP below 4 mmHg, indicating prolonged hypotony). Laser suture lysis (LSL) or bleb needling were not considered surgical failures, as these interventions are part of the standard postoperative care for trabeculectomy.
Statistical Analysis
Demographic data and ocular characteristics were presented using descriptive statistics, with continuous variables reported as mean and standard deviation (SD) and categorical variables as frequency and percentage. For categorical data, the chi-squared test and Fisher’s exact test were used to compare the groups, while unpaired t-tests and the Mann–Whitney U-test were used for continuous data to compare the primary and secondary glaucoma groups. The success rates for both groups were analyzed using Kaplan–Meier curve analysis, with comparisons made using the Log rank test. Factors associated with surgical failure were analyzed using Cox regression analysis, both univariable and multivariable, with results reported as hazard ratios. A p-value of less than 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS version 28.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 421 eyes from 397 patients with glaucoma were analyzed. Patients with glaucoma were categorized into the primary glaucoma group (274 eyes from 251 patients including cases of primary open-angle glaucoma (POAG) in 145 eyes (52.9%), primary angle closure glaucoma (PACG) in 108 eyes (39.4%), juvenile open-angle glaucoma (JOAG) in 20 eyes (7.2%), and ocular hypertension (OHT) in 1 eye (0.4%) and the secondary glaucoma group (147 eyes from 146 patients including cases of neovascular glaucoma (NVG) in 75 eyes (51.0%), uveitis glaucoma in 15 eyes (10.2%), postsurgical related glaucoma in 14 eyes (postvitreoretinal surgery, and penetrating keratoplasty surgery in 8 eyes, 6 eyes) (9.5%), secondary angle closure glaucoma in 13 eyes (8.8%) (lens subluxation in 6 eyes, phacomorphic glaucoma in 3 eyes, and Iridocorneal endothelial (ICE) syndrome in 4 eyes), traumatic glaucoma in 12 eyes (8.2%), pseudoexfoliation glaucoma (PXG) in 9 eyes (6.1%), pigment dispersion glaucoma (PDS) in 2 eyes (1.4%), steroid-induced glaucoma in 3 eyes (2.0%), and other secondary glaucoma in 4 eyes (2.7%)) (Table 1).
 |
Table 1 Baseline Characteristic and Demographic Data Between Primary and Secondary Glaucoma |
The average age differed significantly between the groups. The primary glaucoma group had an average age of 60.8±3.7 years (range: 16–88 years), while the secondary glaucoma group had a younger average age of 56.0±15.7 years (range: 7–84 years) (p-value=0.002). There were no significant differences in sex distribution between the two groups. Baseline characteristics between the primary and secondary glaucoma groups revealed several significant differences. The primary glaucoma group had better mean visual acuity, measuring 0.79±0.70 logMAR, compared to 1.50±0.85 logMAR in the secondary group (p < 0.001). Additionally, the secondary glaucoma group exhibited a higher mean preoperative IOP of 30.14±12.14 mmHg, while the primary group had a mean IOP of 23.77±10.77 mmHg (p < 0.001). Moreover, the primary glaucoma group showed greater structural optic nerve damage, with a vertical cup disc ratio (VCDR) of 0.84±0.13 compared to 0.73±0.21 in the secondary group (p < 0.001). However, no significant differences were found in visual field parameters between the groups, both classified as advanced glaucoma staging, with mean deviations of −16.68±11.08 dB and a visual field index of 47.55±33.59% for the primary group and −17.65±10.78 dB and 48.44±35.35% for the secondary group. Importantly, regarding those with tolerable visual acuity, only 26.37% (111 out) of 421 patients had visual field data.
The primary glaucoma group had a longer duration of glaucoma treatment prior to trabeculectomy, with an average of 14 months compared to 5 months in the secondary glaucoma group (p < 0.001). The mean number of preoperative anti-glaucoma medications was similar between the two groups, with both averaging four types of medication (p = 0.841). Topical prostaglandin analogues were prescribed for 93.8% of the primary glaucoma group, significantly higher than the 79.6% in the secondary group (p < 0.001). Conversely, oral acetazolamide was more frequently prescribed in the secondary group, with 72.8% compared to 47.8% in the primary group (p < 0.001). Additionally, 64 eyes in the secondary glaucoma group underwent panretinal photocoagulation due to neovascular glaucoma, while 93 eyes in the primary glaucoma group received laser peripheral iridotomy for angle closure. Furthermore, phakic lens status was more prevalent in the primary glaucoma group compared to the secondary group (p < 0.001) (Table 1).
The mean follow-up period was 5.2 ± 2.8 years. At the eighth-year follow-up, the cumulative probability of complete or qualified success following trabeculectomy with MMC was 65.9% (95% CI: 59.9%, 71.9%). When comparing the two groups, the primary glaucoma group demonstrated a higher cumulative probability of success at 75.1% (95% CI: 68.4%, 81.8%), compared to 47.4% (95% CI: 36.0%, 58.8%) in the secondary glaucoma group (p < 0.001) (Figure 1).
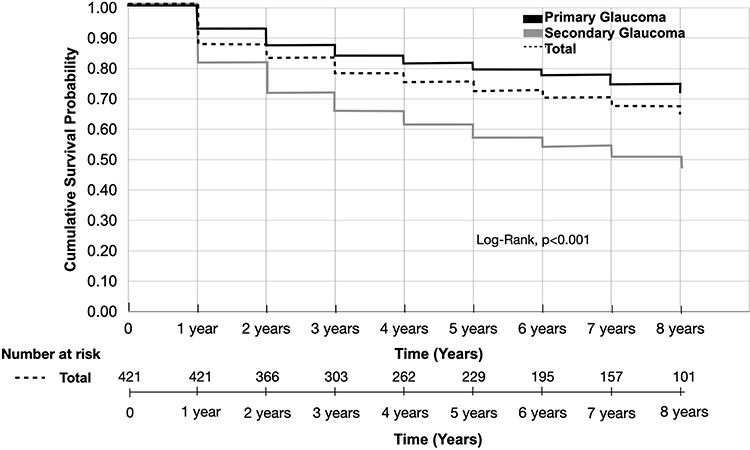 |
Figure 1 Cumulative probability of complete or qualified success of trabeculectomy with Mitomycin C between the primary and secondary glaucoma groups. |
Preoperative IOP in the secondary glaucoma group exhibited a higher mean IOP of 30.14±12.14 mmHg compared to 23.77±10.70 mmHg in the primary glaucoma group (p < 0.001). IOP significantly decreased when comparing baseline preoperative values to postoperative follow-up values at every time point for both groups (p < 0.001; Figure 2). The average number of anti-glaucoma medications decreased significantly when compared to the average baseline number at every time point.
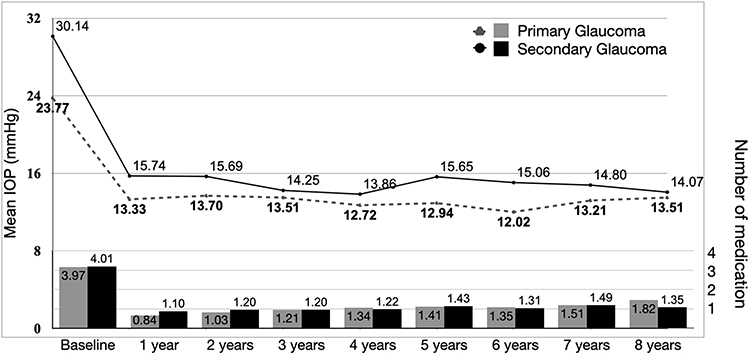 |
Figure 2 Intraocular pressure and number of anti-glaucoma medication comparing at baseline and postoperative follow-up between the primary and secondary glaucoma group. |
Regarding the etiology of primary glaucoma, the cumulative probability of complete or qualified success following trabeculectomy with MMC was comparable among those with POAG, PACG, and JOAG as follows: POAG: 74.7% (95% CI: 64.6%, 84.8%), PACG: 76.0% (95% CI: 65.5%, 86.5%), and JOAG: 70.0% (95% CI: 50.0%, 90.0%), (p=0.261) (Figure 3).
 |
Figure 3 Cumulative probability of complete or qualified success of trabeculectomy with Mitomycin C in the primary open-angle glaucoma, primary closed-angle glaucoma, and juvenile open-angle glaucoma groups. |
In the secondary glaucoma group, the cumulative probability of complete or qualified success following trabeculectomy with MMC was 66.7% (35.9%, 97.5%) for PXG, 50.8% (35.6%, 66.0%) for NVG, 50.0% (20.4%, 79.6%) for uveitis glaucoma, 58.3% (30.5%, 86.1%) for traumatic glaucoma, 49.7% (20.7%, 78.7%) for postsurgical related glaucoma, and 46.2% (15.6%, 76.8%) for secondary angle closure glaucoma; these results showed no statistically significant differences (p=0.996) (Figure 4).
 |
Figure 4 Cumulative probability of complete or qualified success of trabeculectomy with Mitomycin C in cases of neovascular glaucoma, uveitis glaucoma, postsurgical related glaucoma, secondary closed-angle glaucoma, and traumatic glaucoma. |
Early postoperative complications within the first year were comparable between the primary and secondary groups and included a decrease in visual acuity (3.38% vs 3.40%, p=0.976), bleb leakage (0.91% vs 0.34%, p=0.177), hypotony (1.46% vs 1.70%, p=0.697), overhanging bleb (0.09% vs 0.34%, p=0.246), and corneal decompensation (0.46% vs 0.85%, p=0.313). On the other hand, late postoperative complications were more prevalent in the secondary glaucoma group and included decreased visual acuity (5.43% vs 10.29%, p=0.003), hypotony (0.26% vs 1.14%, p=0.020) and corneal decompensation (1.82% vs 3.40%, p=0.004). A bleb-related infection was observed in one eye of the secondary glaucoma group (0.19%, p=0.139) (Table 2).
 |
Table 2 Early and Late Postoperative Complications |
Laser suture lysis was performed in 53.68% of cases and was comparable between both groups (53.3% vs 54.4%, p=0.826) with a median duration of 19 days postoperatively. Bleb needling was conducted in 27.08% of cases and was similar in both the primary and secondary glaucoma groups (26.64% vs 27.89%, p=0.787), with an average needling of 1.38 times in the primary glaucoma group and 1.51 times in the secondary glaucoma (p=0.588), while the median time was 98 days postoperatively. The secondary glaucoma group needed additional surgeries for glaucoma, such as second trabeculectomy, glaucoma drainage device implantation, bleb revision, laser diode transscleral photocoagulation (LDTC), and XEN gel implantation to control IOP more often than in the primary glaucoma group, and the difference was statistically significant (49 eyes (17.88%) vs 51 eyes (34.69%), p < 0.001). Cataract surgery was performed following trabeculectomy in 125 eyes (58.14%) in the primary glaucoma group and in 41 eyes (40.5%) in the secondary glaucoma group, p = 0.035 (Table 3).
 |
Table 3 Postoperative Management |
Factors associated with surgical failure following trabeculectomy with MMC were analyzed, including age, sex, glaucoma etiology, visual acuity, IOP, visual field parameters, VCDR, previous glaucoma treatments, lens status, and postoperative care. Univariate analysis identified several factors linked to surgical failure: pseudoexfoliation glaucoma (unadjusted HR 2.98, 95% CI: 1.05–8.50, p = 0.041), neovascular glaucoma (unadjusted HR 1.993, 95% CI: 1.15–3.45, p=0.014), secondary angle closure glaucoma (unadjusted HR 2.821, 95% CI: 1.24–6.44, p=0.014), previous selective laser trabeculoplasty (SLT) (unadjusted HR 2.28, 95% CI: 1.15–4.50, p=0.018), and laser diode transscleral photocoagulation (unadjusted HR 4.92, 95% CI: 1.53–15.82, p=0.008). Postoperative a number of times of bleb needling also emerged as a risk factor (unadjusted HR 1.46, 95% CI: 1.29–1.64, p < 0.001).
Multivariate analysis revealed significant factors associated with surgical failure included pseudoexfoliation glaucoma (adjusted HR 3.23, 95% CI: 1.10–9.45, p=0.033), neovascular glaucoma (adjusted HR 2.87, 95% CI: 1.29–6.37, p=0.010), previous SLT (adjusted HR 2.45, 95% CI: 1.12–5.33, p=0.024), and postoperative bleb needling (adjusted HR 1.71, 95% CI: 1.46–2.00, p < 0.001). Meanwhile, the secondary angle closure glaucoma was approaching significance (adjusted HR 2.620, 95% CI: 0.997–6.889, p=0.051) (Table 4).
 |
Table 4 Univariate and Multivariate Analysis of Factors Associated with Surgical Failure in Trabeculectomy with Mitomycin |
Discussion
In this study, the surgical outcomes of trabeculectomy were extensively studied in terms of short-term, mid-term, and long-term success rates, postoperative complications, and factors associated with failure.18–22 Compared to 5-fluorouracil, the application of MMC has been linked to higher success rates without increasing postoperative complications and is currently becoming a standard adjunctive for trabeculectomy.13,23 The success rates of trabeculectomy vary significantly depending on etiologies and ethnic backgrounds. The eight-year cumulative success rates in patients with primary glaucoma in this study, including both open-angle and closed-angle glaucoma as well as juvenile open-angle glaucoma, aligned closely with those reported by previous studies. For instance, Wagner et al reported a 73% qualified success rate and a 69% complete success rate after 6 years in Caucasian patients with open-angle glaucoma.14 Liu et al also observed a five-year qualified success rate of 42.9% in Chinese patients with closed-angle glaucoma, which improved to 65.4% in those without diabetes mellitus.24 Chiu HI et al additionally reported a 10-year cumulative qualified success rate of 67.1% in Taiwanese patients and found higher success rates among those over 70 years old.18 Qin ZX et al reported comparable cumulative success rates at 3 years in both primary close- and open-angle glaucoma in Chinese patients at 78.7% and 71.5%, respectively.19 Romero et al reported a 72% success rate after 5 years in Caucasian patients with primary closed-angle glaucoma.16 Pathania et al reported a remarkable five-year quality surgical success rate of 96% in an Indian cohort with juvenile open-angle glaucoma without MMC.25 Conversely, Tsai et al found no significant difference in the success rates between trabeculectomy with and without MMC in patients with juvenile open-angle glaucoma, suggesting that the role of MMC may vary in different populations (73% vs 68%, p = 0.89).26
Our results showed that the cumulative success rate in the secondary glaucoma group was lower than that in the primary glaucoma group and varied from those reported in previous studies with different glaucoma etiologies. However, it should be noted that a significant proportion of participants in the secondary glaucoma group in this study were patients with neovascular glaucoma. Our findings are consistent with those of Takihara et al, who reported a cumulative success rate of 51.7% at 5 years after trabeculectomy with MMC in patients with neovascular glaucoma.27 The highest cumulative success rate in the secondary glaucoma group in this study was observed in those with pseudoexfoliation glaucoma and was higher than the 5 year cumulative success rates in Chinese patients studied by Li et al (66.7% vs 35%);28 however, it was lower than that reported in Turkish patients (90.6%) in a study by Pelitli Gürlü V et al.29 The 8-year cumulative success rate among patients with uveitis glaucoma was lower than the 10-year cumulative success rate reported by Kanaya et al (50% vs 66.5%).30 Furthermore, Marjanovic et al reported a better success rate three years after the emulsified silicone oil postoperative Pars Plana vitrectomy (49.7% vs 67.9%).31
In our study, the secondary closed-angle glaucoma group included cases of lens-induced glaucoma and ICE syndrome. Chew ACY et al reported a higher long-term success rate of combined phaco-trabeculectomy in a small subgroup of 35 patients with secondary glaucoma with a cumulative of success of 91.4% vs 49.7%.32 In contrast, Ruksana A. et al found that a small number of Indian patients with phacomorphic glaucoma (7.9%) required postoperative glaucoma management after undergoing cataract surgery.33 Furthermore, regarding patients with ICE syndrome, Doe et al reported a lower 5-year success rate compared with the rate reported in our study (29% vs 46.2%).34 On the other hand, regarding the traumatic glaucoma group, the short-term success rate reported by Shah et al in a study that included Indian children were better than those reported in our study (71.8% vs 58.3%).35
Our results showed that while early complications were similar between the two groups, patients in the secondary glaucoma group experienced late complications more frequently than those in the primary glaucoma group. For example, decreased visual acuity and hypotony were more frequent in the secondary glaucoma group due to their advanced disease stage at baseline, poorer surgical outcomes, uncontrolled IOP affecting vision, and cataract formation posttrabeculectomy which align with previous studies.36–39 Corneal decompensation was more prevalent in the secondary glaucoma group due to the complexities of the condition and intervention that compromised endothelial cell.40–42 Only one eye had a bleb-related infection in this study, and this was lower than that reported after a 5-year follow-up study by Yamamoto T. et al but was similar to the 0.1% reported in a 2-year follow-up study by Luebke J. et al43,44 In our study, cataract surgery after trabeculectomy was performed in 56% of patients and did not influence the failure rate, similar to the findings reported by Wagner et al.14
Our study identified several similar factors associated with surgical failure that align with the reports of previous studies, including pseudoexfoliation glaucoma, neovascular glaucoma, and secondary closed-angle glaucoma. In patients with pseudoexfoliation, exfoliative materials can obstruct the trabecular meshwork and affect aqueous humor drainage, contributing to elevated IOP. After trabeculectomy, the integrity of the blood-aqueous barrier could be compromised and may aggravate the inflammatory response. The inflammation and exfoliative materials also exacerbate scarring at the filtering area and reduce the efficacy of trabeculectomy, leading to surgical failure.28,45
Neovascular glaucoma (NVG) is a type of secondary glaucoma associated with severe damage to the trabecular meshwork and refractory controlled glaucoma. NVG results from ischemia triggering the production of angiogenic factors that lead to the growth of abnormal blood vessels within the eye as well as obstructed and impaired functioning of the trabecular meshwork, resulting in increased IOP. Surgical outcomes of trabeculectomy and glaucoma drainage device implantation have been shown to be unpredictable and challenging due to neovascularization and fibrosis.27,46,47
In the secondary closed-angle glaucoma group, cases of lens-induced glaucoma, glaucoma due to phacomorphic changes, and subluxation lenses were included. Additionally, trabeculectomy was performed on those with uncontrolled IOP following cataract surgery. Generally, cataract surgery can control IOP in a majority of cases; however, uncontrolled IOP after cataract surgery can be due to functional impairment of the trabecular meshwork resulting from extensive inflammation or permanent damage.33
Second, our multivariate analysis showed that a history of undergoing selective laser trabeculoplasty (SLT) was associated with trabeculectomy failure. The efficacy of SLT has been reported in patients with open-angle glaucoma and ocular hypertension as an initial treatment or an adjunctive therapy in combination with anti-glaucoma medication.8,48,49 In patients with medically uncontrolled IOP in both primary and secondary open-angle glaucoma, SLT may be considered as a treatment option.50 A retrospective cohort study by Baser G. et al showed that SLT does not affect the success rate of trabeculectomy in patients with medically uncontrolled POAG. In our report, SLT was performed in a minority of patients with primary and secondary glaucoma (6.6% vs 2.7%); therefore, this finding cannot be generalized.
Third, some postoperative procedures, including needling the bleb, were identified as factors associated with failure and were similar to those report by Sugimoto et al.51 Failing trabeculectomy, defined as under drainage or not achieving the target IOP, may precede the needling procedure. Therefore, the needing procedure can be the cause or a contributing factor to failure.
The strengths of our study include providing long-term surgical outcomes of trabeculectomy with MMC in both primary and secondary glaucoma, based on a large sample size. Additionally, we applied Cox regression analysis to identify significant risk factors for failure, which adjusted for potential confounders and helped us draw more reliable conclusions about factors influencing the success or failure of trabeculectomy in this population.
However, the limitations of our study include its retrospective design and the absence of randomization, which prevents us from identifying causality. There was also a limited amount of visual field data available for comparison. Additionally, the study was conducted at a single tertiary hospital in Thailand, which may limit the generalizability of the findings to other healthcare settings or patient populations, particularly in low-resource environments or countries with different healthcare systems.
For future research, we propose conducting prospective studies to establish causality and comparing trabeculectomy with other surgical options, such as novel minimally invasive glaucoma surgeries (MIGS) or glaucoma drainage devices, to gain a more comprehensive understanding of the optimal surgical approach.
Conclusion
Overall, our findings demonstrate the effectiveness of trabeculectomy with MMC in patients with glaucoma with uncontrolled IOP for both primary and secondary glaucoma. However, significantly different outcomes were observed between these groups; therefore, careful patient selection and risk assessment are essential. Alternative surgical approaches may be considered in cases with a high risk of trabeculectomy failure, for example, pseudoexfoliation glaucoma and neovascular glaucoma. By identifying significant risk factors for surgical failure, our findings can guide clinicians in optimizing patient selection, surgical technique, and postoperative management to improve success rates.
Acknowledgments
We would like to thank Prangkwan Jiaranaisilawong and Thanwarat Chaipho for their invaluable assistance throughout the research process.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2089. doi:10.1016/j.ophtha.2014.05.013
2. Isipradit S, Sirimaharaj M, Charukamnoetkanok P, et al. The first rapid assessment of avoidable blindness (RAAB) in Thailand. PLoS One. 2014;9(12):e114245. doi:10.1371/journal.pone.0114245
3. Bourne RR, Sukudom P, Foster PJ, et al. Prevalence of glaucoma in Thailand: a population based survey in Rom Klao District, Bangkok. Br J Ophthalmol. 2003;87(9):1069–1074. doi:10.1136/bjo.87.9.1069
4. Jenchitr W, Hanutsaha P, Iamsirithaworn S, Parnrat U, Choosri P. The national survey of blindness low vision and visual impairment in Thailand 2006–2007. Thai J Pub Hlth Ophthalmol. 2007;21(1):10.
5. The advanced glaucoma intervention study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol. 2000;130(4):429–440. doi:10.1016/s0002-9394(00)00538-9
6. Lichter PR, Musch DC, Gillespie BW, et al. Interim clinical outcomes in the collaborative initial glaucoma treatment study comparing initial treatment randomized to medications or surgery. Ophthalmology. 2001;108(11):1943–1953. doi:10.1016/s0161-6420(01)00873-9
7. Garway-Heath DF, Crabb DP, Bunce C, et al. Latanoprost for open-angle glaucoma (UKGTS): a randomised, multicentre, placebo-controlled trial. Lancet. 2015;385(9975):1295–1304. doi:10.1016/S0140-6736(14)62111-5
8. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Laser in glaucoma and ocular hypertension (light) trial: six-year results of primary selective laser trabeculoplasty versus eye drops for the treatment of glaucoma and ocular hypertension. Ophthalmology. 2023;130(2):139–151. doi:10.1016/j.ophtha.2022.09.009
9. National Institute for Health and Care Excellence (NICE). Glaucoma: diagnosis and management. Available from: https://www.ncbi.nlm.nih.gov/books/NBK579558/.
10. Healey PR, Clement CI, Kerr NM, Tilden D, Aghajanian L. Standalone iStent trabecular micro-bypass glaucoma surgery: a systematic review and meta-analysis. J Glaucoma. 2021;30(7):606–620. doi:10.1097/ijg.0000000000001805
11. Cappelli F, Cutolo CA, Olivari S, et al. Trabeculectomy versus Xen gel implant for the treatment of open-angle glaucoma: a 3-year retrospective analysis. BMJ Open Ophthalmol. 2022;7(1):e000830. doi:10.1136/bmjophth-2021-000830
12. Yang X, Zhao Y, Zhong Y, Duan X. The efficacy of XEN gel stent implantation in glaucoma: a systematic review and meta-analysis. BMC Ophthalmol. 2022;22(1):305. doi:10.1186/s12886-022-02502-y
13. De Fendi LI, Arruda GV, Scott IU, Paula JS. Mitomycin C versus 5-fluorouracil as an adjunctive treatment for trabeculectomy: a meta-analysis of randomized clinical trials. Clin Exp Ophthalmol. 2013;41(8):798–806. doi:10.1111/ceo.12097
14. Wagner FM, Schuster AK, Kianusch K, Stingl J, Pfeiffer N, Hoffmann EM. Long-term success after trabeculectomy in open-angle glaucoma: results of a retrospective cohort study. BMJ Open. 2023;13(2):e068403. doi:10.1136/bmjopen-2022-068403
15. Lim SH, Cha SC. Long-term outcomes of mitomycin-c trabeculectomy in exfoliative glaucoma versus primary open-angle glaucoma. J Glaucoma Apr. 2017;26(4):303–310. doi:10.1097/ijg.0000000000000365
16. Romero P, Hirunpatravong P, Alizadeh R, et al. Trabeculectomy with mitomycin-C: outcomes and risk factors for failure in primary angle-closure glaucoma. J Glaucoma. 2018;27(2):101–107. doi:10.1097/ijg.0000000000000842
17. Pantalon A, Feraru C, Tarcoveanu F, Chiselita D. Success of primary trabeculectomy in advanced open angle glaucoma. Clin Ophthalmol. 2021;15:2219–2229. doi:10.2147/OPTH.S308228
18. Chiu HI, Su HI, Ko YC, Liu CJ. Outcomes and risk factors for failure after trabeculectomy in Taiwanese patients: medical chart reviews from 2006 to 2017. Br J Ophthalmol. 2022;106(3):362–367. doi:10.1136/bjophthalmol-2020-317303
19. Qin ZX, Ying X, Han Q, et al. Outcomes and risk factors for failure of trabeculectomy in glaucomatous patients in Southwest China: a 325 eyes analysis. Int J Ophthalmol. 2023;16(3):367–374. doi:10.18240/ijo.2023.03.06
20. Song Z-H, Xu SS, Li GY, et al. Efficacy and safety of the intraoperative application of mitomycin in glaucoma patients with trabeculectomy: a systematic review and meta-analysis. J Clin Pharm Ther. 2023;2023:1–11. doi:10.1155/2023/5249552
21. Lin Z-J, Li Y, Cheng JW, Lu XH. Intraoperative mitomycin C versus intraoperative 5-fluorouracil for trabeculectomy: a systematic review and meta-analysis. J Ocul Pharmacol Ther. 2012;28(2):166–173. doi:10.1089/jop.2011.0117
22. Huang CY, Tseng HY, Wu KY. Mid-term outcome of trabeculectomy with adjunctive mitomycin C in glaucoma patients. Taiwan J Ophthalmol. 2013;3(1):31–36. doi:10.1016/j.tjo.2012.11.003
23. Zheng J, Zhang A. Efficacy and safety of intraoperative injection of mitomycin C during trabeculectomy: a systematic review and meta-analysis. Int Ophthalmol. 2024;44(1):372. doi:10.1007/s10792-024-03291-7
24. Liu J, Zhang M, Li B, Wang J. Long-term outcomes of primary trabeculectomy in diabetic patients without retinopathy with primary angle-closure glaucoma. J Ophthalmol. 2017;2017:7947854. doi:10.1155/2017/7947854
25. Pathania D, Senthil S, Rao HL, Mandal AK, Garudadari CS. Outcomes of trabeculectomy in juvenile open-angle glaucoma. Indian J Ophthalmol. 1998;3689(2):224–8.
26. Tsai JC, Chang HW, Kao CN, Lai IC, Teng MC. Trabeculectomy with mitomycin C versus trabeculectomy alone for juvenile primary open-angle glaucoma. Ophthalmology. 1996;100(3):357–364.
27. Takihara Y, Inatani M, Fukushima M, Iwao K, Tanihara H, Tanihara H. Trabeculectomy with mitomycin C for neovascular glaucoma: prognostic factors for surgical failure. Am J Ophthalmol. 2009;147(5):912–918.e1. doi:10.1016/j.ajo.2008.11.015
28. Li F, Tang G, Zhang H, Yan X, Ma L, Geng Y. The effects of trabeculectomy on pseudoexfoliation glaucoma and primary open-angle glaucoma. J Ophthalmol. 2020;2020:1723691. doi:10.1155/2020/1723691
29. Pelitli Gürlü V, Güçlü H, Özal A, Benian Ö, Alimgil L. Comparison of long-term results of trabeculectomy to treat pseudoexfoliative glaucoma and primary open-angle glaucoma. Int J Ophthalmol. 2018;11(1):66–70. doi:10.18240/ijo.2018.01.12
30. Kanaya R, Kijima R, Shinmei Y, et al. Surgical outcomes of trabeculectomy in uveitic glaucoma: a long-term, single-center, retrospective case-control study. J Ophthalmol. 2021;2021:5550776. doi:10.1155/2021/5550776
31. Marjanovic I, Gvozdenovic R, Bozic M, et al. Trabeculectomy with mitomycin C for glaucoma secondary to emulsified silicone oil after pars plana vitrectomy: three-year follow-up. Vojnosanit Pregl. 2022;79(12):1233–1238. doi:10.2298/vsp200428001m
32. Chew ACY, Htoon HM, Perera SA, et al. Long-term outcomes of combined phacotrabeculectomy surgery in a Singapore tertiary hospital. Asia-Pac J Ophthalmol. 2024;13(5):100102. doi:10.1016/j.apjo.2024.100102
33. Ayub R, Tom LM, Venkatesh R, Srinivasan K. Outcomes and reasons for late presentation of lens-induced glaucoma: a prospective study. Ophthalmol Glaucoma. 2021;4(5):504–511. doi:10.1016/j.ogla.2021.01.005
34. Doe EA, Budenz DL, Gedde SJ, Imami NR. Long-term surgical outcomes of patients with glaucoma secondary to the iridocorneal endothelial syndrome. Ophthalmology. 2001;108(10):1789–1795. doi:10.1016/s0161-6420(01)00725-4
35. Shah C, Sen P, Mohan A, et al. Outcomes and risk factors for failure of trabeculectomy with mitomycin C in children with traumatic glaucoma: a retrospective study. Indian J Ophthalmol. 2022;70(2):590–596. doi:10.4103/ijo.IJO_1997_21
36. AGIS Investigators. The advanced glaucoma intervention study, 6: effect of cataract on visual field and visual acuity. Arch Ophthalmol. 2000;118(12):1639–1642. doi:10.1001/archopht.118.12.1639
37. Parc CE, Johnson DH, Oliver JE, Hattenhauer MG, Hodge DO. The long-term outcome of glaucoma filtration surgery. Am J Ophthalmol. 2001;132(1):27–35. doi:10.1016/s0002-9394(01)00923-0
38. Musch DC, Gillespie BW, Niziol LM, Lichter PR, Varma R. Intraocular pressure control and long-term visual field loss in the collaborative initial glaucoma treatment study. Ophthalmology. 2011;118(9):1766–1773. doi:10.1016/j.ophtha.2011.01.047
39. Gedde SJ, Feuer WJ, Lim KS, et al. Treatment outcomes in the primary tube versus trabeculectomy study after 5 years of follow-up. Ophthalmology. 2022;129(12):1344–1356. doi:10.1016/j.ophtha.2022.07.003
40. Zarei R, Zarei M, Fakhraie G, et al. Effect of mitomycin-C augmented trabeculectomy on corneal endothelial cells. J Ophthalmic Vis Res. 2015;10(3):257–262. doi:10.4103/2008-322x.170345
41. Kim MS, Kim KN, Kim CS. Changes in corneal endothelial cells after Ahmed glaucoma valve implantation and trabeculectomy: 1-year follow-up. Korean J Ophthalmol. 2016;30(6):416–425. doi:10.3341/kjo.2016.30.6.416
42. Vallabh NA, Kennedy S, Vinciguerra R, et al. Corneal endothelial cell loss in glaucoma and glaucoma surgery and the utility of management with descemet membrane endothelial keratoplasty (DMEK). J Ophthalmol. 2022;2022:1315299. doi:10.1155/2022/1315299
43. Yamamoto T, Sawada A, Mayama C, et al. The 5-year incidence of bleb-related infection and its risk factors after filtering surgeries with adjunctive mitomycin C: collaborative bleb-related infection incidence and treatment study 2. Ophthalmology. 2014;121(5):1001–1006. doi:10.1016/j.ophtha.2013.11.025
44. Luebke J, Neuburger M, Jordan JF, et al. Bleb-related infections and long-term follow-up after trabeculectomy. Int Ophthalmol. 2019;39(3):571–577. doi:10.1007/s10792-018-0851-0
45. Nguyen NX, Küchle M, Martus P, Naumann GO. Quantification of blood-aqueous barrier breakdown after trabeculectomy: pseudoexfoliation versus primary open-angle glaucoma. J Glaucoma. 1999;8(1):18–23. doi:10.1097/00061198-199902000-00006
46. Rojananuangnit K, Jiaranaisilawong P, Rattanaphaithun O, Sathim W. Surgical outcomes of glaucoma drainage device implantation in refractory glaucoma patients in Thailand. Clin Ophthalmol. 2022;16:4163–4178. doi:10.2147/OPTH.S393730
47. Călugăru D, Călugăru M. Etiology, pathogenesis, and diagnosis of neovascular glaucoma. Int J Ophthalmol. 2022;15(6):1005–1010. doi:10.18240/ijo.2022.06.20
48. Realini T. Selective laser trabeculoplasty: a review. J Glaucoma. 2008;17(6):497–502. doi:10.1097/IJG.0b013e31817d2386
49. De Keyser M, De Belder M, De Belder J, De Groot V. Selective laser trabeculoplasty as replacement therapy in medically controlled glaucoma patients. Acta Ophthalmol. 2018;96(5):e577–e581. doi:10.1111/aos.13509
50. Alkin Z, Satana B, Ozkaya A, et al. Selective laser trabeculoplasty for glaucoma secondary to emulsified silicone oil after pars plana vitrectomy: a pilot study. Biomed Res Int. 2014;2014:469163. doi:10.1155/2014/469163
51. Sugimoto Y, Mochizuki H, Ohkubo S, Higashide T, Sugiyama K, Kiuchi Y. Intraocular pressure outcomes and risk factors for failure in the collaborative bleb-related infection incidence and treatment study. Ophthalmology. 2015;122(11):2223–2233. doi:10.1016/j.ophtha.2015.06.038
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.