")
Back to Journals » Journal of Pain Research » Volume 17
Medical Misinformation and Quality of Public Video Content on Cannabis for Chronic Pain Management: A Cross-Sectional Analysis of the YouTube Platform
Authors Etumuse B , Greer M , Onyemachi J, El-Abed Y, Kamma S , Shah JD, Tran HT, Hussain N, Pittelkow TP , D’Souza RS
Received 21 May 2024
Accepted for publication 30 October 2024
Published 6 November 2024 Volume 2024:17 Pages 3577—3586
DOI https://doi.org/10.2147/JPR.S479200
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Bright Etumuse,1 Majesty Greer,2 Jane Onyemachi,1 Youshaa El-Abed,3 Sai Kamma,1 Jay D Shah,4 Henry Tuan Tran,1 Nasir Hussain,5 Thomas P Pittelkow,6 Ryan S D’Souza6
1University of Texas Medical Branch School of Medicine, Galveston, TX, USA; 2Howard University College of Medicine, Washington, DC, USA; 3Kansas City University, Kansas City, MO, USA; 4Department of Anesthesiology, Baylor College of Medicine, Houston, TX, USA; 5Department of Anesthesiology, The Ohio State University Wexner Medical Center, Columbus, OH, USA; 6Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, USA
Correspondence: Ryan S D’Souza, Department of Anesthesiology and Perioperative Medicine, Mayo Clinic 200 First St. SW, Rochester, MN, 55905, USA, Email [email protected]
Background: As cannabis legalization expands nationally and globally, its use for chronic pain increases, prompting people to seek information on social media platforms like YouTube. This study evaluates the accuracy and quality of information of popular YouTube videos on cannabis for chronic pain.
Methods: Using search terms related to cannabis for pain, the top 66 videos by view count were selected. Each video was classified as useful, misleading, or neither. The quality and reliability of each video were assessed using the modified DISCERN, mDISCERN, score and the Global Quality Scale, GQS. The video characteristics, usefulness classification, mDISCERN scores, and GQS scores were summarized. Continuous and categorical outcomes were compared using t-test and chi-square, respectively.
Results: Of the 66 videos, 22.73% (n=15) were classified as useful, and 77.27% (n=51) were classified as neither. Of useful videos, 40.00% (n=6) were uploaded by physicians, 40.00% (n=6) were uploaded by corporations, and 6.67% (n=1) were uploaded by an independent user. Of videos classified as neither useful nor misleading, news sources uploaded 27.45% (n=14) of these videos (P=0.02). Physicians uploaded 37.50% (n = 18) of videos with a GQS score ≥ 3 (P=0.04), while independent users uploaded significantly more videos with a mDISCERN score < 3 (22.20%, P=0.02). Useful videos had a mean GQS of 4.00 ± 0.65 compared to a mean GQS of 2.76 ± 0.86 for videos deemed neither (P< 0.0001).
Conclusion: This study suggests a moderate quality of YouTube content on cannabis use for chronic pain. Given cannabis’s growing popularity and potential for misinformation on popular social media platforms, healthcare professionals and organizations should consider uploading educational videos on this topic on YouTube.
Keywords: social media, cannabis, medical cannabis, analgesics, YouTube
Introduction
About 20% of adults in the United States (US) report experiencing chronic pain annually.1 Chronic pain significantly affects this patient population, causing reduced quality of life, decreased work productivity, and increased healthcare expenditure.2 With the opioid epidemic and prevalence of opioid use disorders over the past 20 years, there has been a push to find alternative modalities to treat chronic pain.3,4 For centuries, cannabis has been used worldwide for a variety of reasons, including medicinal uses.5 As the US and countries worldwide begin to implement medical and recreational cannabis policies, increasing numbers of people are turning to cannabis to manage their chronic pain.6–8
Currently, there is conflicting evidence on the effectiveness of cannabis use as an analgesic for chronic pain; however, they are promising as an adjuvant or alternative analgesic for patients who do not respond well to first-line analgesic medications or interventional pain treatment.8 The proposed mechanism of cannabis on pain modulation is via retrograde signaling in the endocannabinoid system.8 Injured tissues produce endocannabinoids that mitigate sensitization and inflammation through endocannabinoid receptors, primarily Cannabinoid Receptor 1 (CB1) and Cannabinoid Receptor 2 (CB2).9 CB1 receptors are highly concentrated in the dorsal root and trigeminal ganglion’s nociceptive sensory neurons. CB1 is primarily responsible for modulating neurotransmitter release in the brain and spinal cord.10 CB2, albeit in lower concentrations than CB1, also plays a role in pain management. CB2 receptors are found in cells of hematopoietic origin and regulate neuroimmune interactions and inflammatory responses.10 During retrograde signaling, the produced endocannabinoids travel backward in the synapse and bind to CB1, releasing inhibitory neurotransmitters and decreasing the firing of nociceptive neurons.11 Delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD), which are cannabinoids found in cannabis, are analogs with high receptor affinity for the CB1 receptor.8,12
As cannabis continues gaining popularity, many will turn to social media platforms to attain more information on the therapeutic effect of cannabis. One social platform, YouTube, has 2.6 billion monthly active users.13 YouTube is a popular video website often used to share information regarding healthcare topics.14 This platform also features a tool that adds an information panel for healthcare-related videos, providing details about the source of the information. These principles set by the National Academy of Medicine (NAM) and American Public Health Society (APHA) designate a video as coming from a credible source.15 Personal accounts must undergo a series of verifications to ensure the credibility of the information in their videos before they can be granted an information panel.15 This information panel tool was developed to combat the spread of health misinformation and helps users easily identify reputable sources for healthcare information.15 However, this tool is only offered in the US and UK, and it currently only applies to some healthcare-related conditions/information.15 To date, the quality and reliability of information on YouTube regarding cannabis use for chronic pain remains unknown. The objective of this study is to critically analyze the most viewed YouTube videos about cannabis use for chronic pain and to appraise the video content for its accuracy and quality of medical information.
Materials and Methods
The protocol was developed using previous studies evaluating the reliability and quality of information presented in YouTube videos regarding healthcare information.16,17 The outline of the video search and selection process is summarized in Figure 1.
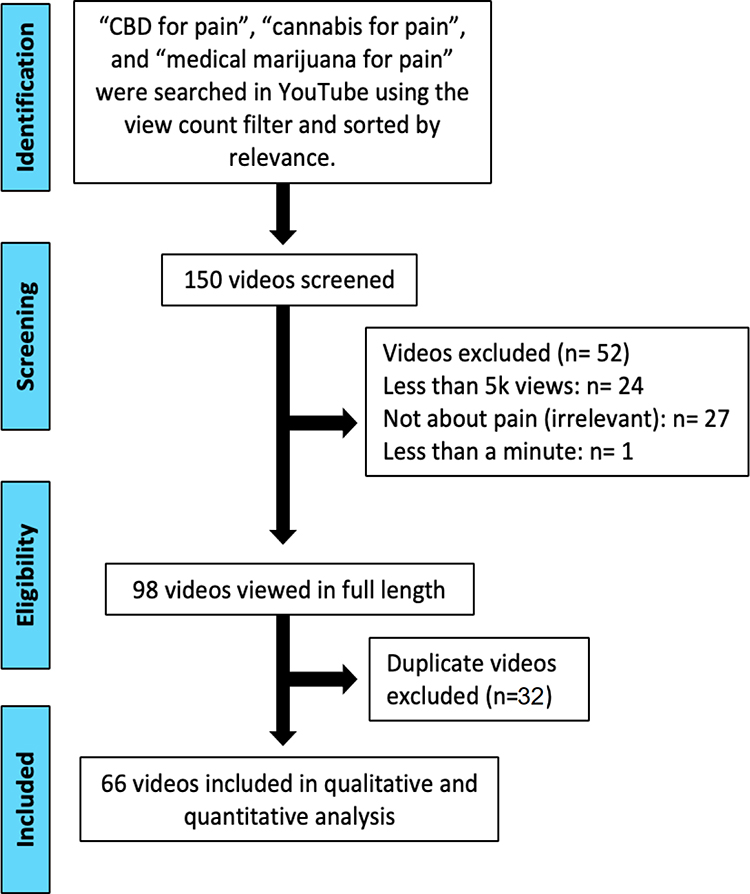 |
Figure 1 Flow chart of the video search and selection process. |
Search Strategy
Four terms were entered into Google Trends to compare YouTube popularity within the last two years across the United States. These terms include “cannabis”, “Marijuana”, “cannabinoids”, “CBD” and “THC”. (Search conducted on The Google Trends website: https://trends.google.com/trends/explore?date=2019-06-17%202022-06-17&geo=US&gprop=youtube&q=%2Fm%2F054yc0,marijuana,cannabinoids,THC). Search results revealed that “cannabis” and “marijuana” are the more commonly used search terms on YouTube; therefore, both keywords were adopted for this project.
Three search terms were used to query the YouTube platform (www.youtube.com) on August 2nd, 2022: “cannabis for pain”, “medical marijuana for pain”, and “CBD for pain”. Multiple search terms were used to increase the sensitivity of capturing relevant content. The results were filtered based on the sort-by-relevance algorithm, and then the videos were filtered by view count from highest to lowest.
Video Selection Process
The top 150 videos by view count were selected and screened after the search query. Fifty videos were preselected from the search results using “cannabis for pain”, fifty videos were preselected from the search results for “medical marijuana for pain”, and fifty videos were preselected from the search results using “CBD for pain”. Videos that met one or more of the following conditions were excluded from the final analysis:
- Videos less than one minute (rationale: these videos did not provide sufficient time to cover the necessary content on cannabis use for chronic pain)
- Videos not in English or without English texts
- Duplicate videos
- Videos without audio
- Videos with less than five thousand views were excluded. (rationale: this threshold was used to include the most popular videos)
- Videos unrelated to cannabis use for the management of chronic pain
After reviewing videos for relevance and removing those that met exclusion criteria, a final list of the top 66 videos by view count was selected to be included in the final qualitative and quantitative analysis.
Data Extraction
The following data from each video on the final list were recorded into an electronic database by two independent reviewers (B.E. and Y.E.): the uniform resource locator (URL), the date of upload, the number of days since upload, the view count, the length of the video in minutes, the number of likes, the number of comments, and the video production source. The production source of the video was classified as being from 1) a physician, 2) an independent user without medical expertise, 3) corporation, 4) news source, 5) public health agencies, 6) Ted Talks, or 7) a digital media company.
Usefulness of Video Content
Two independent reviewers (B.E. and Y.E.) evaluated each video and categorized it as either useful, misleading, or neither useful nor misleading, using criteria from previous systematic reviews.16–18 The accuracy of video content was verified based on current literature and previously published evidence-based guidelines on the use of medical cannabis.5,7,19 The usefulness of each video content was determined to ascertain how effectively it could help patients make well-informed decisions regarding their health.
The criteria for a useful video were: 1) a correct statement about the definition of cannabis, 2) an accurate statement of the pain-reducing mechanism of cannabis, and 3) an accurate statement about the indications, adverse effects, benefits, and potential outcomes of cannabis use for chronic pain management.
The criteria for a video to be deemed misleading were: 1) an inaccurate definition of cannabis, 2) at least one inaccurate statement about the pain-reducing mechanism of cannabis, 3) at least one inaccurate statement about the indications, adverse effects, benefits, and potential outcomes of cannabis for chronic pain management.
A video was classified as neither useful nor misleading if it had 1) no definition of cannabis, 2) no statement about the pain-reducing mechanism of cannabis, and 3) no statement on the indications, adverse effects, benefits, and potential outcomes of cannabis for chronic pain management.
The above scoring model was adapted from prior published methodology.20
Quality of Video Content
The quality and reliability of the content presented in each of the videos were determined using the modified DISCERN scale (mDISCERN) and Global Quality Scale (GQS), which have both been previously used to assess social media video content related to healthcare information.16,17,21
We used a 5-question scoring system, the mDISCERN, adapted from the 15-question DISCERN scale to evaluate the reliability and quality of the information presented in the videos.22 The mDISCERN criteria were:
1) Are the aims clear and achieved?
2) Are reliable sources of information used?
3) Is the information presented balanced and unbiased?
4) Are additional sources of information listed for patient reference?
5) Are areas of uncertainty mentioned?
Each section was scored on a scale of 1 to 5, where each “yes” would count as one point and each “no” would not award any points. A score greater than 3 indicated high reliability.
We used the GQS 5-point scoring system to assess the quality of the video content. The GQS scoring criteria were:
Score 1: Poor quality, poor flow, and most information is missing. It is ultimately not helpful for patients.
Score 2: Generally poor, with some information given but of limited use to patients.
Score 3: Moderate quality and some important information are appropriately discussed.
Score 4: Good quality, good flow, and most relevant information are covered, making it useful for patients.
Score 5: Excellent quality and excellent flow, making it very useful for patients.
The videos were assigned a GQS score between 1 and 5, where a score of 1 or 2 indicated the video was of low quality, a score of 3 indicated the video was of intermediate quality, and a score of 4 or 5 indicated the video was of good quality.23,24 The quality of the analyzed videos was evaluated to determine how health information was conveyed to patients, as videos with a clear structure, credible sources, outstanding delivery, and content relevant to patients will enhance comprehension and practical utilization.
Data Analysis
The YouTube video characteristics, usefulness classification, mDISCERN scores, and GQS scores were summarized using their mean values and standard deviation. Cohen’s Kappa was used to determine the inter-rater reliability of the two reviewers’ (B.E. and Y.E). mDISCERN and GQS scores. A score of 0 would indicate that there was no agreement amongst the reviewers, 0.01–0.20 would indicate slight agreement, 0.21–0.40 would be considered fair agreement, 0.41–0.60 would be moderate agreement, 0.61–0.80 indicate substantial agreement, and 0.81–1.00 is almost perfect agreement between the reviewers.25 The agreement percent, expected chance, standard error, and 95% confidence interval were calculated for the mDISCERN and GQS scores using Cohen’s Kappa for each video.
Pairwise comparisons were conducted between “useful”, “misleading”, and “neither useful nor misleading” videos. Continuous variables were compared using a t-test, and binary categorical variables were compared using a chi-square test. A p-value of <0.05 was considered to be statistically significant.
Results
Video Characteristics and Production Sources
The YouTube platform was queried on August 2nd, 2022, with three search phrases – “cannabis for pain”, “medical marijuana for pain”, and “CBD for pain”. One hundred fifty videos were screened with 44.00% (n=66) meeting the inclusion criteria. Of the total number of videos analyzed, 22.73% (n=15) of videos were classified as useful, 0% of videos were classified as misleading, and 77.27% (n=51) videos were classified as neither useful nor misleading (Table 1). Cohen’s kappa coefficient between both reviewers was 0.92, indicating almost perfect agreement. Of the videos deemed useful, 40.00% (n = 6) were created and uploaded by physicians, and 40.00% (n = 6) were uploaded by corporations. Only one video (6.67%) deemed useful was uploaded by an independent user. Among videos classified as neither useful nor misleading, news sources uploaded 27.45% (n = 14) of the total number of these videos compared to other sources (P=0.02). Additionally, none of the videos deemed useful were uploaded by news sources (P=0.02). Videos deemed useful were found to be longer than videos deemed neither useful nor misleading (P<0.01). There was also a significant difference between the mean GQS score for useful videos versus neither useful nor misleading videos. Useful videos were found to have a mean GQS score of 4.00 ± 0.65 compared to a mean GQS of 2.76 ± 0.86 for videos deemed neither useful nor misleading (P<0.01).
 |
Table 1 YouTube Video Characteristics and Video Production Source |
A mean mDISCERN score of 3.00 was calculated for all of the videos, indicating moderate quality and reliability for all the analyzed videos. The mean GQS for all videos was 3.05, indicating an overall medium quality of appraised videos. When comparing the video production source based on mDISCERN grading criteria (Table 2), we found that 37.50% (n = 18) of the videos with a mDISCERN score ≥3 were created by physicians (P=0.04). In contrast, independent users were found to upload a significantly higher number of videos with mDISCERN scores <3 compared to videos with mDISCERN scores ≥3 (P<0.01).
 |
Table 2 YouTube Video Characteristics and Video Production Source Based on mDISCERN |
When comparing the analyzed videos by GQS score (Table 3), we observed that 37.50% (n = 18) of videos with a GQS score ≥3 were uploaded by physicians (P=0.04). Independent users uploaded a significantly higher number of videos with a GQS score <3 compared to videos with a GQS score ≥ 3 (P=0.02). News sources also posted a higher number of videos with a GQS score <3 compared to videos with GQS scores ≥3 (P=0.03).
 |
Table 3 YouTube Video Characteristics and Video Production Source Based on GQS |
mDISCERN and GQS Scores
When comparing the mDISCERN and GQS scores between the analyzed videos, useful videos were found to have a higher mDISCERN score of 3.47 ± 0.83 compared to videos deemed neither useful nor misleading, which had an mDISCERN score of 2.86 ± 1.18, although this difference did not achieve statistical significance (P= 0.07). Similarly, in analyzing the GQS scores between all the videos analyzed, videos deemed useful were found to have a higher GQS score of 4.00 ± 0.65 compared to 2.76 ± 0.86 (P<0.01) for videos deemed neither useful nor misleading.
Discussion
This study highlights salient observations about the publicly available informational videos on YouTube pertaining to the use of cannabis for chronic pain. Of the videos analyzed, only 22.70% were useful, providing helpful education on the use of cannabis for pain management. While none of the videos proved misleading based on the analysis criteria, a substantial majority, 77.30%, were classified as neither useful nor misleading, suggesting the potential prevalence of less accurate or unnecessary information on cannabis use on YouTube. Notably, the useful videos exhibited a statistically significant increase in duration than videos classified as neither useful nor misleading videos, suggesting a correlation between video length and information depth contributing to their overall quality. Interestingly, no videos classified as useful were attributed to news sources, yet these sources contributed to 27.45% of videos categorized as neither useful nor misleading. This suggests that news sources are less likely to upload accurate informational videos on the use of cannabis for chronic pain management on YouTube. This finding does warrant further exploration as news sources serve as a shared resource for medical information for many patients. One possible explanation could be their tendency to use oversimplified language and avoid complex information such as the definition or pain-reducing mechanism of medical cannabis to cater to a broader audience.
Physicians were found to create a significantly higher number of videos with GQS scores ≥3, suggesting that videos uploaded by physicians contained more organized, relevant, and high-quality information, making them more useful for patients. This is an important finding as it underscores the potential for physicians to influence and drive change in the realm of online health information. Independent users were found to upload a significantly higher number of videos with a GQS score <3, indicating a higher propensity for independent users to upload videos missing essential pieces of clinically relevant information, making them less useful for patients. Concordantly, physicians uploaded a higher number of videos with an mDISCERN score ≥3, indicating that physicians were more likely to use reliable sources of information and present them in a balanced and unbiased manner. Additionally, physicians were more likely to mention areas of uncertainty regarding the use of cannabis for chronic pain management. Independent users created more videos with mDISCERN scores <3, suggesting that independent users were less likely to utilize reliable sources of information, may present a biased perspective, and may not mention areas of uncertainty.
Despite the significant findings presented, it is important to consider the constraints of this study. This study’s cross-sectional design is a limitation, offering insights derived from a singular point in time rather than a temporal continuum. Other limitations include using only English-speaking videos and restricting the analysis solely to the YouTube platform, both of which introduce selection bias. Notwithstanding these limitations, this study benefits from robust methodologies, employing validated tools such as the mDISCERN and Global Quality Scale scoring instruments. Additionally, this is the first study to our knowledge that delves into the qualitative and quantitative analysis of YouTube videos regarding cannabis use for chronic pain management. Interestingly, our search did not capture any videos that were classified as “misleading”. We propose several potential explanations for this observation. Firstly, our classification criteria for a “misleading” video was likely strict and required false definitions of cannabis, inaccurate descriptions of pain-reducing mechanisms of cannabis, and other non-factual statements. Secondly, our search strategy did not include certain common terms such as “weed” which may limit the type of social media content that was captured. Future studies should aim at evaluating publicly available information regarding cannabis for chronic pain management on other online platforms such as TikTok, Facebook, and Twitter. While the YouTube community serves as a hub for healthcare information regarding cannabis use for chronic pain, patients face certain challenges in efficiently searching for quality videos with clinically relevant information.
As social media platforms continue to grow in popularity, healthcare misinformation is rapidly emerging as a public health concern, necessitating prompt action from healthcare providers.18,26,27 Additionally, prior research has shown that patients do not share the knowledge they found on social media regarding their healthcare with their providers, further compounding the barriers providers face in combating healthcare misinformation.16 As a progressive measure, we advocate for the implementation of a verification process by online video platforms, such as YouTube, to ensure that videos determined to be clinically accurate and relevant occupy the forefront of search results, thereby mitigating the dissemination of healthcare misinformation. We recommend that healthcare providers be equipped with analytic tools to assess the quality of health information available on various social media platforms in their specific fields.28–30 We recognize the limitations of cross-sectional studies in fully capturing trends in healthcare misinformation. Therefore, it will be crucial for future studies to incorporate a longitudinal approach to investigate trends in content quality and usefulness of health information related to medical cannabis use available on the YouTube platform.
Conclusion
This study suggests moderate quality of social media content on medical cannabis for chronic pain management. Given the increasing popularity of medical cannabis as well as the potential for misinformation on popular social media platforms, we recommend health organizations and medical professionals consider uploading educational videos on cannabis use for chronic pain management on social media platforms.
Data Sharing Statement
Data are available upon reasonable request to the corresponding author of this manuscript.
Ethics Approval and Consent to Participate
Given that this study involved review of publicly available records, the Mayo Institutional Review Board deemed this study exempt from review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors report no funding sources for this project.
Disclosure
The authors declare no conflicts of interest related to this submission.
References
1. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. 2022;163(2):e328–e332. doi:10.1097/j.pain.0000000000002291
2. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults - United States, 2016. MMWR Morb Mortal Wkly Rep.;67(36):1001–1006. PMID: 30212442. doi:10.15585/mmwr.mm6736a2
3. Peters-Watral B. Opioid use disorder and chronic pain: challenges for palliative care practice. Int J Palliat Nurs.;25(9):453–457. PMID: 31585059. doi:10.12968/ijpn.2019.25.9.453
4. D’Souza RS, Nahin RL. Nationally Representative Rates of Incident Prescription Opioid Use Among United States Adults and Selected Subpopulations: longitudinal Cohort Study From the National Health Interview Survey, 2019 to 2020. J Pain. 2024;12:104665. PMID: 39260809. doi:10.1016/j.jpain.2024.104665
5. Hill KP, Palastro MD, Johnson B, Ditre JW. Cannabis and pain: a clinical review. Cannabis Cannabinoid Res. 2017;2(1):96–104. doi:10.1089/can.2017.0017
6. Aebischer JH, Dieckmann NF, Jones KD, St John AW. Chronic Pain Clinical and Prescriptive Practices in the Cannabis Era. Pain Manag Nurs. 2022;23(2):109–121. PMID: 34973920. doi:10.1016/j.pmn.2021.11.009
7. Pantoja-Ruiz C, Restrepo-Jimenez P, Castañeda-Cardona C, Ferreirós A, Rosselli D. Cannabis and pain: a scoping review. Braz J Anesthesiol. 2022;72(1):142–151. PMID: 34280454. doi:10.1016/j.bjane.2021.06.018
8. Ang SP, Sidharthan S, Lai W, et al. Cannabinoids as a Potential Alternative to Opioids in the Management of Various Pain Subtypes: benefits, Limitations, and Risks. Pain Ther. 2023;12(2):355–375. PMID: 36639601. doi:10.1007/s40122-022-00465-y
9. Lu HC, Mackie K. Review of the Endocannabinoid System. Biol Psychiatry Cogn Neurosci Neuroim. 2021;6(6):607–615. PMID: 32980261. doi:10.1016/j.bpsc.2020.07.016
10. Ye L, Cao Z, Wang W, Zhou N. New Insights in Cannabinoid Receptor Structure and Signaling. Curr Mol Pharmacol. 2019;12(3):239–248. PMID: 30767756. doi:10.2174/1874467212666190215112036
11. Bouchet CA, Ingram SL. Cannabinoids in the descending pain modulatory circuit: role in inflammation. Pharmacol Ther. 2020;209:107495. PMID: 32004514. doi:10.1016/j.pharmthera.2020.107495
12. Crocq MA. History of cannabis and the endocannabinoid system. Dialog Clin Neurosci. 2020;22(3):223–228. PMID: 33162765. doi:10.31887/DCNS.2020.22.3/mcrocq
13. YouTube by the numbers (2022): stats, Demographics & Fun Facts. Omnicore Agency. Availabe from https://www.omnicoreagency.com/youtube-statistics/#:~:text=Statistics%20(Editor’s%20choice)-.about%201.86%20billion%20active%20users.
14. Madathil KC, Rivera-Rodriguez AJ, Greenstein JS, Gramopadhye AK. Healthcare information on YouTube: a systematic review. Health Informatics J. 2015;21(3):173–194. PMID: 24670899. doi:10.1177/1460458213512220
15. Get info on health-related content - YouTube Help. Support.google.com. Availabe from: https://support.google.com/youtube/answer/9795167?hl=en.
16. D’Souza RS, D’Souza S, Sharpe EE. YouTube as a source of medical information about epidural analgesia for labor pain. Int J Obstet Anesth. 2021;45:133–137. doi:10.1016/j.ijoa.2020.11.005
17. Langford B, Hooten WM, D’Souza S, Moeschler S, D’Souza RS. YouTube as a Source of Medical Information About Spinal Cord Stimulation. Neuromodulation. 2021;24(1):156–161. doi:10.1111/ner.13303
18. D’Souza RS, Kilgore AE, D’Souza S. Manifestations of Pain During the COVID-19 Pandemic Portrayed on Social Media: a Cross-Sectional Study. Pain Med.;23(2):229–233. PMID: 34668551. doi:10.1093/pm/pnab305
19. Strand N, RS D, Karri J, et al. Medical Cannabis: a Review from the American Society of Pain and Neuroscience. J Pain Res.;16:4217–4228. PMID: 38094100. doi:10.2147/JPR.S425862
20. Chang MC, Park D. YouTube as a Source of Information on Epidural Steroid Injection. J Pain Res. 2021;14:1353–1357. doi:10.2147/JPR.S307506
21. Chen AY, Azizi B, Borba AJ, Armstrong AW. Rosacea videos on social media: a comparison of accuracy, quality, and viewer engagement. Dermatol Online J. 27(2):
22. Singh AG, Singh S, Singh PP. YouTube for information on rheumatoid arthritis--a wakeup call? J Rheumatol. 2012;39(5):899–903. doi:10.3899/jrheum.111114
23. Bernard A, Langille M, Hughes S, Rose C, Leddin D, Veldhuyzen van Zanten S. A systematic review of patient inflammatory bowel disease information resources on the World Wide Web. Am J Gastroenterol. 2007;102(9):2070–2077. doi:10.1111/j.1572-0241.2007.01325.x
24. Aglamis SO, Senel S, Koudonas A. Quality analysis of YouTube videos on vulvodynia. Sex Med.;11(1):qfac013. PMID: 37007847. doi:10.1093/sexmed/qfac013
25. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22(3):276–282. PMID: 23092060. doi:10.11613/BM.2012.031
26. D’Souza RS, D’Souza S, Strand N, Anderson A, Vogt MNP, Olatoye O. YouTube as a source of medical information on the novel coronavirus 2019 disease (COVID-19) pandemic. Glob Public Health. 2020;15(7):935–942. PMID: 32397870. doi:10.1080/17441692.2020.1761426
27. Greer M, Kamma S, Tran H, et al. Misinformation Persists in Complementary Health: evaluating the Reliability and Quality of YouTube-Based Information on the Use of Acupuncture for Chronic Pain. J Pain Res.;17:1509–1518. PMID: 38646592. doi:10.2147/JPR.S459475
28. D’Souza RS, Hooten WM, Murad MH. A Proposed Approach for Conducting Studies That Use Data From Social Media Platforms. Mayo Clin Proc. 2021;96(8):2218–2229. PMID: 34353473. doi:10.1016/j.mayocp.2021.02.010
29. D’Souza RS, Daraz L, Hooten WM, Guyatt G, Murad MH. Users’ Guides to the Medical Literature series on social media (part 1): how to interpret healthcare information available on platforms. BMJ Evid Based Med. 2022;27(1):11–14. PMID: 34933925. doi:10.1136/bmjebm-2021-111817
30. D’Souza RS, Daraz L, Hooten WM, Guyatt G, Murad MH. Users’ Guides to the Medical Literature series on social media (part 2): how to appraise studies using data from platforms. BMJ Evid Based Med. 2022;27(1):15–20. PMID: 34933929. doi:10.1136/bmjebm-2021-111850
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.