")
Back to Journals » Journal of Pain Research » Volume 18
Minimally Invasive Lumbar Decompression (MILD) in Patients with Lumbar Spinal Stenosis: A Systematic Review of Randomized and Prospective Trials
Authors Orhurhu V, Brancolini S, Zheng D, Snyder S, Jevotovsky DS , Chopra H, Sahni S , Li N, D’Souza RS , Evankovich M, Lynch B, Farrell ME, Alter BJ, Emerick T
Received 6 February 2025
Accepted for publication 7 July 2025
Published 11 July 2025 Volume 2025:18 Pages 3527—3540
DOI https://doi.org/10.2147/JPR.S521038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Dawood Sayed
Vwaire Orhurhu,1 Scott Brancolini,1 Danielle Zheng,1 Sean Snyder,1 David S Jevotovsky,2 Harman Chopra,3 Sidharth Sahni,2 Nathan Li,4 Ryan S D’Souza,5 Maria Evankovich,1 Brendan Lynch,1 Michael Edward Farrell,1 Benedict J Alter,1 Trent Emerick1
1Department of Anesthesiology & Perioperative Medicine, Division of Chronic Pain Management, University of Pittsburgh Medical Center, Pittsburgh, PA, USA; 2Department of Rehabilitation Medicine, NYU Langone Health, New York, NY, USA; 3Department of Physical Medicine and Rehabilitation, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 4Department of Orthopedic Surgery, Boston University School of Medicine, Boston, MA, USA; 5Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, USA
Correspondence: Sidharth Sahni, Email [email protected]
Background/Importance: Lumbar spinal stenosis (LSS) remains one of the most common causes of pain and functional disability in patients with chronic pain. Minimally invasive lumbar decompression (MILD) has been shown to reduce pain and improve function with lumbar spinal stenosis. However, very few large studies have evaluated the short- and long-term effects of MILD on functional improvement and pain reduction.
Purpose: To evaluate the evidence on the MILD procedure for chronic pain patients with LSS.
Methods: A systematic review of randomized and prospective trials investigating the effectiveness of the MILD procedure in managing low back pain and lower extremity pain was performed using PubMed, Medline, Embase, Google Scholar, clinical trial.gov, and Cochrane. We utilized the Cochrane review methodologic quality assessment, GRADE and Interventional Pain Management Techniques – Quality Appraisal of Reliability and Risk of Bias Assessment (IPM-QRB) and IPM-QRB for Nonrandomized Studies (IPM-QRBNR) to guide our data extraction and assessment of study quality methods. Our study summarized and presented the evidence quality on a scale of 1 to 5.
Results: Fifteen MILD studies met our inclusion criteria. There were 8 studies that were multicenter prospective trials, and 7 studies were single centers prospective trials. The evidence based on a systematic review of prospective trials investigating the efficacy of the MILD procedure showed a median level 2b evidence with several level 1b studies available. Pain and functional outcome GRADE assessment of studies was high quality.
Conclusion: This systematic review suggests that the MILD procedure can be effective in managing chronic pain patients with lumbar spinal stenosis.
Keywords: minimally invasive lumbar decompression, MILD, lumbar spinal stenosis, review, pain
Introduction
Chronic low back pain (LBP) is a major cause of morbidity and healthcare expenditure in the United States. Lumbar spinal stenosis (LSS) is a common degenerative spine disease that results in chronic LBP and functional impairment.1 LSS occurs in 2–11% of the general population in the US and is most common among people 50–60 years of age.2–4 Over 200,000 Americans are impacted by LSS, making it the leading cause of spinal surgery in those over 65.5
Anatomically, LSS is characterized by narrowing of the central canal, intervertebral foramen, or lateral recess and may be caused by disc protrusion, foraminal stenosis, facet hypertrophy, facet joint cartilage degeneration, ligamentum flavum hypertrophy, spondylolisthesis, or osteophyte formation.6,7 Hypertrophic ligamentum flavum (HLF) contributes to 85% of cases.8 However, the narrowing of any of these structures may compress neural elements and lead to limited mobility and pain, as well as symptomatic neurogenic claudication.9,10
Neurogenic claudication manifests as gluteal and leg pain, numbness, weakness, or fatigue that worsens with extension, walking or standing and improves when sitting or bending forward.11,12 Patients with LSS are typically first treated with conservative measures including physical therapy and home exercise programs, as well as medications such as oral analgesics.13 Conservative treatments, however, can have limited long-term efficacy in a subset of patients with LSS.14 Patients with LSS may also choose to undergo interventional pain interventions including epidural steroid injections (ESIs), which have been shown to provide significant short-term relief.15–17 However, studies have questioned the efficacy of ESIs in LSS patients with concomitant neurogenic claudication.18 Thus, if patients do not experience improvement in pain, they may elect to undergo more invasive procedures, such as decompressive surgery with or without of interspinous spacer, with or without fusion. However, these procedures are associated with higher complication rates.16,17
Minimally invasive lumbar decompression (MILD) has been developed as an alternative to decompression surgery to increase the dimensions of the vertebral canal and achieve nerve decompression.5,11 Recent advances in minimally invasive techniques for this procedure have gained traction primarily related to their supposed reduction in post-operative complications and hospital length of stay.19 However, a comprehensive review and meta-analysis of the literature are necessary to further elucidate the overall efficacy and proper indications for MILD.
Methods
This systematic review was conducted according to the recommendations of the Cochrane Collaboration,20,21 and it is reported per the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.22 No a priori protocol was published in a peer-reviewed journal. Registration registered with the International Prospective Register of Systematic Reviews (PROSPERO) was completed in November 2023 (ID: CRD42023477410).
The review focuses on the effectiveness of MILD procedure in the management of chronic pain related to lumbar spinal stenosis.
Eligibility Criteria
Double blind randomized prospective trials, prospective nonrandomized trials, and prospective case series of patients with lumbar spinal stenosis and neurogenic claudication symptoms treated with the MILD procedure were included in this study. Only studies in which lumbar spinal stenosis was evaluated based on buckling or thickening (≥2.5mm) of the ligamentum flavum were synthesized in this review. The primary outcome was defined as pain relief in NRS or VAS scale. Intensity scores reported on a 0 to 100 VAS were transformed to a 0 to 10 NRS, as these scales have a high correlation.23,24 The secondary outcome was defined as improvement of functional status. Functional outcome was based on the Oswestry Disability Index (ODI). Studies with malignancies, traumatic fractures, or surgical decompressions were excluded from our analysis. Our study also excluded studied book chapters, review studies, retrospective studies and case reports.
Search Strategy
We systematically searched and screened all titles and abstracts from MEDLINE, Embase, and Google Scholar, as well as a clinical trials website (http://www.clinicaltrials.com) from the year 2000 to December 30, 2023. Our search strategy was extensive without language restrictions. This included several nomenclatures for MILD, lumbar spinal stenosis, and leg pain. Our search strategy was as follows: ((“minimally invasive lumbar decompression”[MeSH Terms] OR “MILD”[All Fields]) OR (“minimally invasive”[Supplementary Concept] OR “Decompression”[All Fields] OR “Spine Decompression”[All Fields]) OR Lumbar Decompression[All Fields] OR ((“ligamentum flavum remodeling”[MeSH Terms] OR “spine decompression”[All Fields] OR “spine surgery”[All Fields]) AND ligamentum flavum remodeling [All Fields])) AND (low back pain[All Fields] OR (“lumbar spinal stenosis”[MeSH Terms] OR (“lumbar”[All Fields] AND “spinal stenosis”[All Fields] AND “pain”[All Fields] AND “syndromes”[All Fields]) OR “LSS” [All Fields] OR (“Stenosis”[All Fields] AND “lumbar”[All Fields] AND “pain”[All Fields]) OR (“Claudication”[MeSH Terms] OR “claudication”[All Fields]) OR (“chronic pain”[MeSH Terms] OR (“chronic”[All Fields] AND “pain”[All Fields]) OR “chronic pain”[All Fields]) OR (“Neurogenic Claudication”[MeSH Terms] OR “neurogenic claudication”[All Fields]) OR (“leg pain”[MeSH Terms] OR “leg pain”[All Fields]) OR (“radiculopathy”[MeSH Terms] OR “Radiculopathy”[All Fields] OR (“neuropathic”[All Fields] AND “pain”[All Fields]) OR “neuropathic pain”[All Fields])) AND (Clinical Trial[ptyp] AND “loattrfull text”[sb] AND “humans”[MeSH Terms]).
Study Selection
Two of four authors (S.B., S.S., E.M., B.L.) independently evaluated titles, abstracts, and full texts. After applying our established inclusion and exclusion criteria, full texts of selected articles were reviewed. All instances of discordance were discussed between the investigators and the senior author (T.E.) to reach a consensus. Two additional authors (V.O. and D.Z.) later confirmed and reviewed studies for final inclusion. One additional study of 2-year follow-up data published in 2024 was added post hoc.25
Data Collection Process
The reference data, populations, and outcomes were extracted from the articles into pre-specified tables using a standardized data extraction form by multiple authors (S.B., S.S., E.M., B.L., D.J., S.S.). Our investigation extracted information on studies’ general characteristics (including first author’s last name, publication year, design, number of arms, and primary outcomes), participants (demographic characteristics of the populations, sample size), clinical information (diagnosis, duration and intensity of pain), and trial setting (ie, single center vs multicenter). For continuous data (eg, pain scores), we extracted means and standard deviations (SDs) from tables or graphs. Our investigation also contacted authors of studies when information required about their analysis or results was not reported. In situations where numeric pain scores were not reported in the text of the manuscript, we obtained their estimated values from published graphs and figures.
Data Synthesis and Analysis
Data synthesis and analysis were performed, including assessment of the risk of bias or quality of individual studies, outcomes assessment, and qualitative analysis.
Bias Evaluation
The present investigation used the Interventional Pain Management Techniques – Quality Appraisal of Reliability and Risk of Bias Assessment Tool (IPM – QRB) for randomized controlled trials (Supplementary Table 1) and Interventional Pain Management Techniques – Quality Appraisal of Reliability and Risk of Bias Assessment for nonrandomized or observational studies (IPM-QRBNR) to evaluate the quality of individual articles included in this study (Supplementary Table 2).26,27 Studies were subsequently assessed using the GRADE system as a framework for rating the quality of evidence.
Based on the IPM-QRB and IPM-QRBNR criteria, studies meeting the inclusion criteria but scoring less than 16 were considered low quality and were excluded, studies scoring from 16 to 31 were considered moderate quality; and studies scoring from 32 to 48 were considered high quality and were included.
Two authors were responsible for the methodologic quality assessment of each manuscript. The assessment was carried out independently in an unblinded, standardized manner to assess the methodologic quality and internal validity of all the studies considered for inclusion. A third reviewer was used to resolve discrepancies until a consensus was reached.
Further remaining issues were discussed by all reviewers and were then resolved.
Definitions of Outcome and Follow-Up Period
For the present analysis, a change of at least 3 points on an 11-point pain scale of 0 to 10 was considered clinically significant. Though a 30% improvement is often used as the clinically important difference in functional scores, some papers have used thresholds as low as 10% to reflect that even the slightest difference in function may drastically impact quality of life.28
Pain scores defined by visual analogue scale (0–100) or numeric pain rating scale (0–10) were evaluated at different time points. Functional outcomes defined by Oswestry Disability Index were evaluated at different time points. A study was judged to be positive if the relevance and effectiveness of the MILD procedure was demonstrated upon comparison from baseline to follow-up. Safety evaluated by adverse events within the study period were also recorded as a secondary outcome. Studies within 6 months were considered short-term, while those above 6 months were considered long-term.
Level of Evidence Analysis
The evidence levels were assessed using a modified version of the Oxford Centre for Evidence-Based Medicine hierarchy, as outlined in the American Medical Association’s Journal of Ethics.29
The analysis was conducted using 10 levels of evidence (1a, 1b, 1c, 2a, 2b, 2c, 3a, 3b, 4, 5) that correlate to one of four grades of recommendation (A, B, C, D). At least 2 of the review authors independently, in an unblinded, standardized manner, analyzed the evidence. Any disagreements between reviewers were resolved by a third author and consensus was attained.
Results
Search Results
From the initial 2112 records identified through searching databases and other sources, we removed duplicate records and then screened the remaining 2105 relevant publications. Among the initial records screened, 1995 were excluded because the publications lacked clinical relevance to our topic. Upon review of the 93 remaining publications, full-text articles were assessed for eligibility, and 78 were excluded because the study settings did not meet our inclusion criteria (Figure 1). Fifteen prospective trials were included for the systematic review (Table 1).
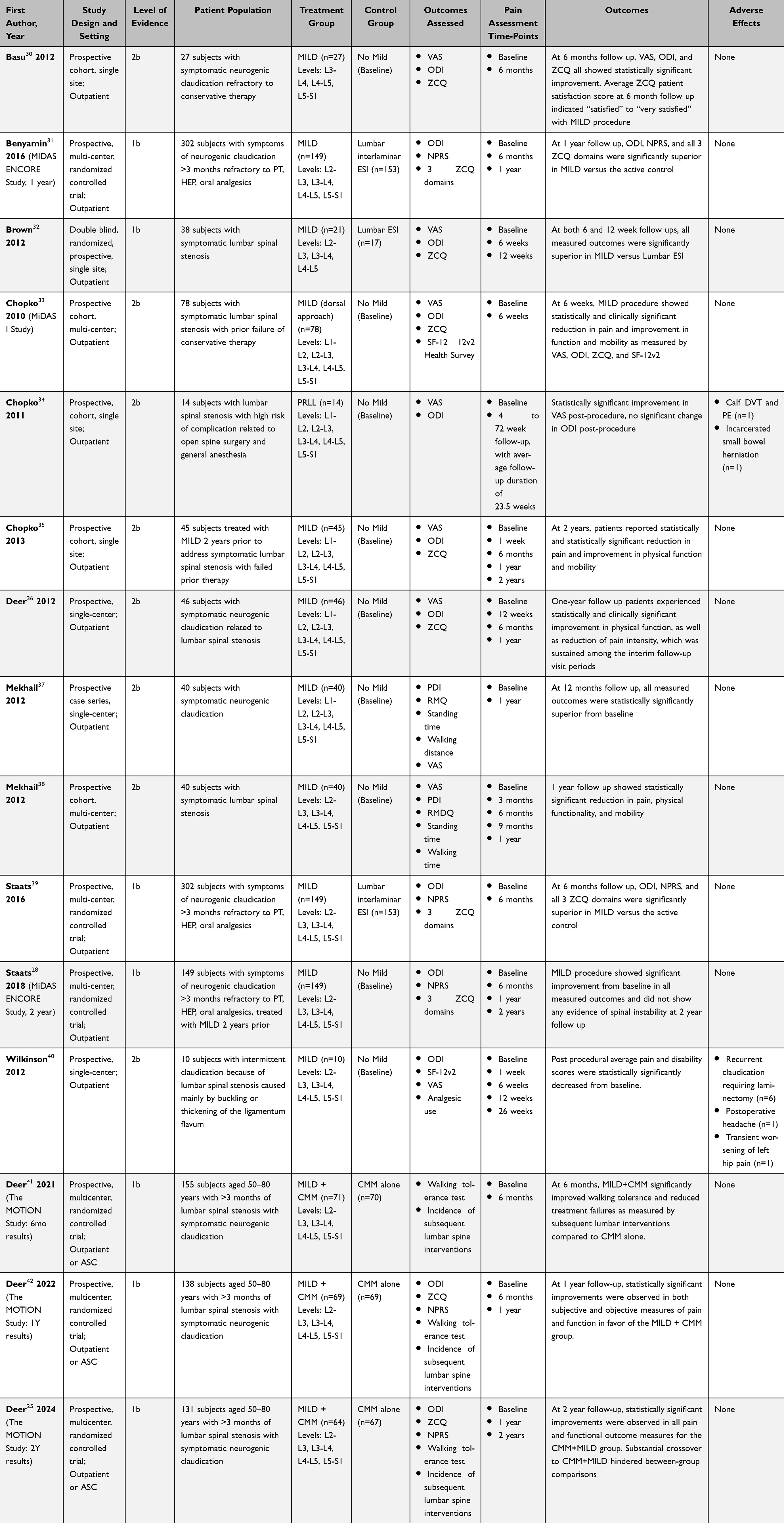 |
Table 1 Outcomes From Included Double-Blind Randomized Prospective Trials, Nonrandomized Prospective Trials, and Prospective Case Series Involving Patients with Lumbar Spinal Stenosis and Neurogenic Claudication Treated with the MILD Procedure |
 |
Figure 1 Flow chart reviewing MILD studies included in our systematic review. |
Study Characteristics
The included prospective studies described patients with LSS treated with the MILD procedure. The median final follow-up was 1 year, with a range of 6 weeks to 2 years. Table 1 provides individual study details.
Level of Evidence, Methodologic Quality, and Risk of Bias
Seven randomized control trial (RCT) papers and eight non-randomized prospective trials met the inclusion criteria.25,28,30–42 The seven RCTs were classified as level 1b evidence (grade A recommendation). Supplementary Tables 3 shows the methodologic quality assessment and risk of bias in each of these trials utilizing the IPM-QRB criteria. Assessment IPM-QRB showed that all seven trials were high-quality.
Supplementary Table 4 shows the assessment of the included nonrandomized or observational studies, utilizing IPM-QRBNR criteria. Eight non-randomized prospective studies were included in this category and classified as level 2b evidence (grade B recommendation). Five of these studies30,35–38 were considered high quality, and three of the studies33,34,40 were considered moderate quality.
Assessment with the GRADE framework can be found in Table 2. Pain and functional outcomes at follow-up assessed by VAS or NPRS and ODI, respectively, were of high quality per GRADE assessment. GRADE assessment of adverse events in the included studied were deemed low quality.
 |
Table 2 Evidence Profile – MILD Procedures for Patients with Lumbar Spinal Stenosis |
Primary Outcome: Pain Scores
All included prospective studies revealed statistically significant improvement of pain scores following MILD procedure. Nine studies used VAS (60.0%) and five utilized NPRS (33.3%). The 6-month interim report of the Motion study did not report pain outcomes. Nine of fourteen studies (64.3%) that reported pain outcomes demonstrated a clinically significant difference in pain outcome at final follow-up. Notably, three studies decreased by 2.9 points on the pain scale at follow-up, just short of the 3-point clinically significant definition.32,36,37 The Motion study demonstrated clinically significant improvement in leg pain, but not back pain, compared to baseline pain at one- and two-year follow-up.25,42 Main findings of the pain outcome assessments are summarized in Table 1.
Secondary Outcome: Functional Scores
The included prospective studies all revealed some level of improvement of functional scores following MILD, though not all achieved statistical significance. One study (6.7%) did not achieve statistical significance at final follow-up.34 All studies except two utilized the ODI. Eleven of the thirteen studies (84.6%) that utilized ODI met criteria for a clinically significant change in ODI.28 Findings of the functional outcome assessments are summarized in Table 1.
Secondary Outcome: Safety
Two studies (13.3%) reported adverse events after MILD procedure for LSS with NC, as detailed in Table 1. Chopko et al reported one participant with deep vein thrombus and PE on post-operative day 1 and another participant with incarcerated small bowel hernia through a pre-existing abdominal wall defect.34 Wilkinson et al reported cases of post-operative headache (n=1) and transient worsening of hip pain (n=1).40 Six participants in this study presented with recurrent claudication requiring subsequent laminectomy.
Discussion
The MILD procedure has been successfully used in clinical practice for over a decade. As with other operative treatments for LSS, MILD is indicated only after conservative treatment with physical therapy and analgesic medications have failed to provide adequate pain relief.43 Accordingly, the studies examined in this review recruited patients who had failed conservative medical management (CMM) such as physical therapy, analgesics, and epidural steroid injections (ESI). Three studies explicitly defined a period of failed medical treatment for greater than three months as an inclusion criterion for their study, emphasizing the importance of CMM within a comprehensive management plan. However, it should be noted that little consensus exists regarding strategies for optimizing nonsurgical management for these patients, and there is poor evidence to definitively conclude that medication, physiotherapy, or epidural injections significantly and/or consistently relieve pain from LSS.5,44–46
The main indication for MILD in the studies examined was symptomatic neurogenic claudication related to LSS. This diagnosis can be associated with various comorbidities, including, but not limited to, ligamentum flavum hypertrophy, osteophytes, disc herniation, or facet joint hypertrophy; however, of these pathologies, MILD only directly addresses hypertrophied ligamentum flavum.47 Thirteen studies in our analysis specified a minimum degree of ligamentum flavum hypertrophy to meet inclusion criteria for the study, while seven specifically identified significant osteophytes, disc protrusion, or facet joint hypertrophy as an exclusion criterion.
Patient Selection and Consideration
Minimally invasive lumbar decompression is generally contraindicated in patients with conditions that increase spinal instability such as severe herniations, spinal osteomyelitis, or spondylolisthesis greater than grade 1 (>25%). In addition, patients with increased bleeding risk such as coagulopathy or current anticoagulation therapy are not recommended for the procedure related to possible risk of creating an epidural hematoma, which may cause permanent nerve damage.43
Proper pre-operative preparation before MILD, as with any other surgery, can have a large effect on the procedure outcome. Increasing patients’ active role in managing their care by asking questions and sharing the decision making with their physician has been shown to improve post-operative functional outcomes.48 Furthermore, along with good communication, physicians should manage patient expectations appropriately when discussing the procedure and potential benefits. One study found that while increased expectations for physical function following LSS surgery were associated with increased physical function six months post-surgery, increased expectations for pain relief were in fact associated with poorer pain relief. The authors hypothesized that this discrepancy could be due to the feasibility of improving physical function (aided by active patient participation in physical therapy and exercise programs) versus improving pain (which is largely outside of the patient’s volitional control).49 As with other pain syndromes, outcomes in LSS are also influenced by individual patient psychiatric factors. Disorders such as depression, schizophrenia, and dementia have been shown to be associated with poorer outcomes and higher adverse events rates in spinal surgeries.50,51 In LSS specifically, disability scores post-operatively increased with decreased cognitive status and widespread pain pre-operatively, and patient satisfaction increased with greater levels of optimistic personality trait.52,53
Patient education is also a critical function of the physician during the pre-operative period. Related to the specialized nature of the procedure, existing patient education literature on minimally invasive spine surgery often requires at least a high school, sometimes undergraduate, level reading comprehension, yet, the reading difficulty of education material for minimally invasive procedures is more complex than for the open counterparts.54 Physicians should therefore be cautious when using written materials to educate patients about MILD and other minimally invasive spine procedures; supplementation with video media may aid in patient comprehension, especially among patients with low literacy, furthermore, there has been a recent push for artificial intelligence and extended reality-based tools.55,56
Operative Planning
Preoperative imaging for LSS is most commonly and accurately performed using MRI and is necessary for localizing the area of pathology.57 Notably, in this review, the included studies performed the MILD procedure at all lumbar levels from L1-L2 to L5-S1. However, it should be noted that MRI findings do not always correlate to the clinical symptomatology of the patient. In fact, one study found no significant association between the degree of stenosis observed on MRI imaging and ODI scores.58 As LSS is a dynamic pathology that is exacerbated or relieved with certain movements of the spine, static MR images may not fully represent the day-to-day severity of the patient’s spinal canal occlusion.
The MILD procedure involves posterolateral access to the interlaminar space through a small trocar portal. The approach is conducted under fluoroscopic epidurographic guidance to ensure accurate trajectory.59 Although none of the trials included in this study noted the administration of prophylactic antibiotics, a single dose of preoperative antibiotics (usually cefazolin) is standard in minimally invasive spine surgery.60 An important advantage of MILD is that it does not require general anesthesia; local anesthetic at the incision site and moderate sedation are sufficient.61 No implants are left at the site, which makes reoperation simpler, and no sutures are needed—the incision is usually closed with a sterile adhesive strip. The procedure can usually be performed in 30 to 40 minutes.59 After a two-hour observation period, patients can almost universally be discharged without an overnight stay in the hospital and can rapidly resume daily activities, including a return to walking within 24 hours.59,62,63
Patients receiving MILD also require opioids for postoperative pain control at lower rates (12%) compared to open laminectomy, where opioid usage rates can exceed 50%.63,64 Notable complications of MILD identified by previous studies include hematoma (rate identified in one study to be 4.5%), wound infection (0–1.4%), postoperative urinary retention (2.7–13.0%), and CSF leak (4.3–7.7%).65,66 Minimally invasive strategies for LSS have been identified to result in lower complication rates and shorter hospital stay lengths compared to open decompression procedures.65–67 Minimally invasive procedures also avoid complications of open laminectomy associated with weakening of the intraspinous and supraspinous ligaments, which may lead to spinal instability and spondylolisthesis.67,68 However, in the studies we identified, the most common adverse effects included recurrence of the claudication requiring laminectomy (6 patients in one study), as well as DVT/PE, small bowel herniation, headache, and hip pain (1 patient each). Thirteen of the 15 included trials did not report any major adverse events among their patient populations. These results demonstrate that MILD is a safe procedure with a favorable side effect profile compared to open procedures. This notion is further supported by recent evidence from Medicare claims data, which demonstrated significantly lower rates of harms following the MILD when compared to interspinous spacers and outpatient laminectomy.69,70
Given its recent development, there is little literature regarding long-term follow-up for patients receiving MILD. Advantages of MILD in the long-term include the absence of permanent implants inside the patient’s body, as well as the aforementioned favorable side effect profile. Patients who undergo decompression for lumbar spinal stenosis are at risk of restenosis requiring reoperation, which has been observed in anywhere from 0% to 23% of patients.71 It is yet to be seen what effect, if any, MILD has on restenosis risk compared to more traditional decompression procedures. Theoretically, determining the risk of restenosis is of increased importance in MILD because the procedure only involves removing fragments of the hypertrophied ligamentum flavum, leaving more tissue intact.72 In addition, traditional surgery was shown in the Spine Patient Outcomes Research Trial (SPORT) to have diminished efficacy with increasing preoperative duration of symptoms; it is unknown whether MILD efficacy decreases over time in a similar fashion.5
The presented review also has some limitations. Perhaps, the most apparent is the lack of double-blind randomized clinical trials to date investigating MILD; only one study in our analysis met these criteria. There were only six randomized control trials, often the same clinical trial with multiple publications at different follow-up times. Placebo effects, especially in trials of treatment for chronic pain, are large and often underestimated by clinicians and researchers.73 Although sham procedures are an often-used and necessary component of blinded trials of surgical procedures, questions have been raised over their ethical implementation due to potential risks to patients receiving the sham treatment, which are greater when compared to placebo medications.74 In addition, all but three trials compared MILD to other procedural interventions, while the remainder of trials compared MILD to baseline medical management. Furthermore, the overlap in populations from ongoing trials prevented us from performing a robust statistical analysis. It is also worth noting that improvements in pain and functional scores vary widely. Consequently, the thresholds for clinical significance cited in the literature also vary, and our review selected one of these reported thresholds as a reference. Given the promising initial results elucidated herein, though, further research on the MILD procedure compared to current standards will be crucial to guide best practice strategies, especially in different populations.
Conclusion
Through thorough review of the published literature, we found that MILD proved to be a safe and efficacious treatment for LSS. Compared to conservative methods, MILD had improved pain and disability scores that lasted up to two years in prospective trials.
Disclosure
Dr Ryan D’Souza reports Investigator-initiated grant funding from Nevro Corp and Saol Therapeutics paid to his institution. Dr Michael Edward Farrell reports personal fees from Abbott, outside the submitted work. Dr Benedict Alter reports grants from NIH NINDS, during the conduct of the study; equity interest from Synapse Symphony, outside the submitted work. Dr Trent Emerick reports stock/equity from Vanish Therapeutics, Inc, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Nicol V, Verdaguer C, Daste C, et al. Chronic low back pain: a narrative review of recent international guidelines for diagnosis and conservative treatment. J Clin Med. 2023;12(4):1685. doi:10.3390/jcm12041685
2. Katz JN, Zimmerman ZE, Mass H, Makhni MC. Diagnosis and management of lumbar spinal stenosis: a review. JAMA. 2022;327(17):1688–1699. doi:10.1001/jama.2022.5921
3. Kalichman L, Cole R, Kim DH, et al. Spinal stenosis prevalence and association with symptoms: the Framingham study. Spine J. 2009;9(7):545–550. doi:10.1016/j.spinee.2009.03.005
4. Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine. 1995;20(1):11–19. doi:10.1097/00007632-199501000-00003
5. Lurie J, Tomkins-Lane C. Management of lumbar spinal stenosis. BMJ. 2016;352:h6234. doi:10.1136/bmj.h6234
6. Bagley C, MacAllister M, Dosselman L, Moreno J, Aoun SG, El Ahmadieh TY. Current concepts and recent advances in understanding and managing lumbar spine stenosis. F1000Res. 2019;8:137. doi:10.12688/f1000research.16082.1
7. Katz JN, Harris MB. Clinical practice. Lumbar Spinal Stenosis the New England J Med. 2008;358(8):818–825. doi:10.1056/NEJMcp0708097
8. Hansson T, Suzuki N, Hebelka H, Gaulitz A. The narrowing of the lumbar spinal canal during loaded MRI: the effects of the disc and ligamentum flavum. European Spine J. 2009;18(5):679–686. doi:10.1007/s00586-009-0919-7
9. Friedly JL, Comstock BA, Turner JA, et al. A randomized trial of epidural glucocorticoid injections for spinal stenosis. New Engl J Med. 2014;371(1):11–21. doi:10.1056/NEJMoa1313265
10. Manchikanti L, Candido KD, Kaye AD, et al. Randomized trial of epidural injections for spinal stenosis published in the New England journal of medicine: further confusion without clarification. Pain Physician. 2014;17(4):E475–88. doi:10.36076/ppj.2014/17/E475
11. Yuan H, Yi X. Lumbar spinal stenosis and minimally invasive lumbar decompression: a narrative review. J Pain Res. 2023;16:3707–3724. doi:10.2147/JPR.S428112
12. Ammendolia C, Chow N. Clinical outcomes for neurogenic claudication using a multimodal program for lumbar spinal stenosis: a retrospective study. J Manipulative Physiol Ther. 2015;38(3):188–194. doi:10.1016/j.jmpt.2014.12.006
13. Deer TR, Grider JS, Pope JE, et al. The MIST guidelines: the lumbar spinal stenosis consensus group guidelines for minimally invasive spine treatment. Pain Pract. 2019;19(3):250–274. doi:10.1111/papr.12744
14. Messiah S, Tharian AR, Candido KD, Knezevic NN. Neurogenic claudication: a review of current understanding and treatment options. Curr Pain Headache Rep. 2019;23(5):32. doi:10.1007/s11916-019-0769-x
15. Manchikanti L, Kaye AD, Manchikanti K, Boswell M, Pampati V, Hirsch J. Efficacy of epidural injections in the treatment of lumbar central spinal stenosis: a systematic review. Anesth Pain Med. 2015;5(1):e23139. doi:10.5812/aapm.23139
16. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. New Engl J Med. 2008;358(8):794–810. doi:10.1056/NEJMoa0707136
17. Deyo RA, Martin BI, Ching A, et al. Interspinous spacers compared with decompression or fusion for lumbar stenosis: complications and repeat operations in the Medicare population. Spine. 2013;38(10):865–872. doi:10.1097/BRS.0b013e31828631b8
18. Ammendolia C, Hofkirchner C, Plener J, et al. Non-operative treatment for lumbar spinal stenosis with neurogenic claudication: an updated systematic review. BMJ Open. 2022;12(1):e057724. doi:10.1136/bmjopen-2021-057724
19. Aldahshory AR, Mashaly H, El Molla ST, Ismaiel IA, Saoud K. Comparative study of minimally invasive lumbar decompression versus decompressive laminectomy with posterolateral transpedicular fixation for the treatment of degenerative lumbar canal stenosis. Asian J Neurosurg. 2020;15(2):293–301. doi:10.4103/ajns.AJNS_132_20
20. Shuster J. Review: Cochrane handbook for systematic reviews for interventions, Version 5.1.0, published 3/2011. In: Julian PT, Higgins, Green S, editors. Research Synthesis Methods. 2011:2.
21. Furlan AD, Malmivaara A, Chou R, et al. 2015 updated method guideline for systematic reviews in the Cochrane back and neck group. Spine. 2015;40(21):1660–1673. doi:10.1097/BRS.0000000000001061
22. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339(jul21 1):b2535. doi:10.1136/bmj.b2535
23. Akinpelu AO, Olowe OO. Correlative study of 3 pain rating scales among obstetric patients. Afr J Med Med Sci. 2002;31(2):123–126.
24. Ponce de Leon S, Lara-Muñoz C, Feinstein AR, Wells CK. A comparison of three rating scales for measuring subjective phenomena in clinical research. II. Use of experimentally controlled visual stimuli. Arch Med Res. 2004;35(2):157–162. doi:10.1016/j.arcmed.2003.07.009
25. Deer TR, Chafin TB, Costandi SJ, et al. The MOTION study: two-year results of a real-world randomized controlled trial of the mild® procedure for treatment of lumbar spinal stenosis. Pain Pract. 2024;24(1):109–119. doi:10.1111/papr.13293
26. Manchikanti L, Hirsch JA, Cohen SP, et al. Assessment of methodologic quality of randomized trials of interventional techniques: development of an interventional pain management specific instrument. Pain Physician. 2014;17(3):E263–90. doi:10.36076/ppj.2014/17/E263
27. Manchikanti L, Hirsch JA, Heavner JE, et al. Development of an interventional pain management specific instrument for methodologic quality assessment of nonrandomized studies of interventional techniques. Pain Physician. 2014;17(3):E291–317. doi:10.36076/ppj.2014/17/E291
28. Staats PS, Chafin TB, Golovac S, et al. Long-term safety and efficacy of minimally invasive lumbar decompression procedure for the treatment of lumbar spinal stenosis with neurogenic claudication: 2-year results of MiDAS ENCORE. Reg Anesth Pain Med. 2018;43(7):789–794. doi:10.1097/AAP.0000000000000868
29. Daramola OO, Rhee JS. Rating evidence in medical literature. Virtual Mentor. 2011;13(1):46–51. doi:10.1001/virtualmentor.2011.13.1.pfor2-1101
30. Basu S. Mild procedure: single-site prospective IRB study. Clin J Pain. 2012;28(3):254–258. doi:10.1097/AJP.0b013e31822bb344
31. Benyamin RM, Staats PS, Dasei M. MILD® is an effective treatment for lumbar spinal stenosis with neurogenic claudication: miDAS ENCORE randomized controlled trial. Pain Physician. 2016;19(4):229–242. doi:10.36076/ppj/2019.19.229
32. Brown LL. A double-blind, randomized, prospective study of epidural steroid injection vs. the mild® procedure in patients with symptomatic lumbar spinal stenosis. Pain Pract. 2012;12(5):333–341. doi:10.1111/j.1533-2500.2011.00518.x
33. Chopko B, Caraway DL. MiDAS I (mild decompression alternative to open surgery): a preliminary report of a prospective, multi-center clinical study. Pain Physician. 2010;13(4):369–378. doi:10.36076/ppj.2010/13/369
34. Chopko BW. A novel method for treatment of lumbar spinal stenosis in high-risk surgical candidates: pilot study experience with percutaneous remodeling of ligamentum flavum and lamina. J Neurosurg Spine. 2011;14(1):46–50. doi:10.3171/2010.9.SPINE091012
35. Chopko BW. Long-term results of percutaneous lumbar decompression for LSS: two-year outcomes. Clin J Pain. 2013;29(11):939–943. doi:10.1097/AJP.0b013e31827fb803
36. Deer TR, Kim CK, Bowman RG, Ranson MT, Yee BS. Study of percutaneous lumbar decompression and treatment algorithm for patients suffering from neurogenic claudication. Pain Physician. 2012;15(6):451–460. doi:10.36076/ppj.2012/15/451
37. Mekhail N, Vallejo R, Coleman MH, Benyamin RM. Long-term results of percutaneous lumbar decompression mild(®) for spinal stenosis. Pain Pract. 2012;12(3):184–193. doi:10.1111/j.1533-2500.2011.00481.x
38. Mekhail N, Costandi S, Abraham B, Samuel SW. Functional and patient-reported outcomes in symptomatic lumbar spinal stenosis following percutaneous decompression. Pain Pract. 2012;12(6):417–425. doi:10.1111/j.1533-2500.2012.00565.x
39. Staats PS, Benyamin RM. MiDAS ENCORE: randomized controlled clinical trial report of 6-month results. Pain Physician. 2016;19(2):25–38. doi:10.36076/ppj/2016.19.25
40. Wilkinson JS, Fourney DR. Failure of percutaneous remodeling of the ligamentum flavum and lamina for neurogenic claudication. Neurosurgery. 2012;71(1):86–92. doi:10.1227/NEU.0b013e31825356f5
41. Deer T, Kim C, Wahezi SE, Qu H, Sayed D. Objective real-world outcomes of patients suffering from painful neurogenic claudication treated with the mild(®) procedure: interim 6-month report of a randomized controlled trial. J Pain Res. 2021;14:1687–1697. doi:10.2147/JPR.S312573
42. Deer TR, Costandi SJ, Washabaugh E, et al. The MOTION study: a randomized controlled trial with objective real-world outcomes for lumbar spinal stenosis patients treated with the mild® procedure: one-year results. Pain Med. 2022;23(4):625–634. doi:10.1093/pm/pnac028
43. Deer TR, Kapural L. New image-guided ultra-minimally invasive lumbar decompression method: the mild procedure. Pain Physician. 2010;13(1):35–41. doi:10.36076/ppj.2010/13/35
44. Atlas SJ, Delitto A. Spinal stenosis: surgical versus nonsurgical treatment. Clin Orthop Relat Res. 2006;443:198–207. doi:10.1097/01.blo.0000198722.70138.96
45. Ammendolia C, Stuber K, de Bruin LK, et al. Nonoperative treatment of lumbar spinal stenosis with neurogenic claudication: a systematic review. Spine. 2012;37(10):E609–16. doi:10.1097/BRS.0b013e318240d57d
46. Fritz JM, Lurie JD, Zhao W, et al. Associations between physical therapy and long-term outcomes for individuals with lumbar spinal stenosis in the SPORT study. Spine J. 2014;14(8):1611–1621. doi:10.1016/j.spinee.2013.09.044
47. Racz GB, Heavner JE, Bosscher H, Helm S. The MILD procedure. Pain Pract. 2013;13(7):594–596. doi:10.1111/papr.12051
48. Greenfield S, Kaplan S, Ware JE. Expanding patient involvement in care. Effects on patient outcomes. Ann Intern Med. 1985;102(4):520–528. doi:10.7326/0003-4819-102-4-520
49. Iversen MD, Daltroy LH, Fossel AH, Katz JN. The prognostic importance of patient pre-operative expectations of surgery for lumbar spinal stenosis. Patient Educ Couns. 1998;34(2):169–178. doi:10.1016/S0738-3991(97)00109-2
50. Menendez ME, Neuhaus V, Bot AG, Ring D, Cha TD. Psychiatric disorders and major spine surgery: epidemiology and perioperative outcomes. Spine. 2014;39(2):E111–22. doi:10.1097/BRS.0000000000000064
51. Amaral V, Marchi L, Martim H, et al. Influence of psychosocial distress in the results of elective lumbar spine surgery. J Spine Surg. 2017;3(3):371–378. doi:10.21037/jss.2017.08.05
52. Nicholas M, Vlaeyen JWS, Rief W, et al. The IASP classification of chronic pain for ICD-11: chronic primary pain. Pain. 2019;160(1):28–37. doi:10.1097/j.pain.0000000000001390
53. Lee J, Kim HS, Shim KD, Park YS. The effect of anxiety, depression, and optimism on postoperative satisfaction and clinical outcomes in lumbar spinal stenosis and degenerative spondylolisthesis patients: cohort study. Clin Orthop Surg. 2017;9(2):177–183. doi:10.4055/cios.2017.9.2.177
54. Agarwal N, Feghhi DP, Gupta R, et al. A comparative analysis of minimally invasive and open spine surgery patient education resources. J Neurosurg Spine. 2014;21(3):468–474. doi:10.3171/2014.5.SPINE13600
55. Murphy PW, Chesson AL, Walker L, Arnold CL, Chesson LM. Comparing the effectiveness of video and written material for improving knowledge among sleep disorders clinic patients with limited literacy skills. South Med J. 2000;93(3):297–304. doi:10.1097/00007611-200093030-00010
56. Phelan EA, Deyo RA, Cherkin DC, et al. Helping patients decide about back surgery: a randomized trial of an interactive video program. Spine. 2001;26(2):206–211. discussion 12. doi:10.1097/00007632-200101150-00016
57. Fritz JM, Delitto A, Welch WC, Erhard RE. Lumbar spinal stenosis: a review of current concepts in evaluation, management, and outcome measurements. Arch Phys Med Rehabil. 1998;79(6):700–708. doi:10.1016/S0003-9993(98)90048-X
58. Sirvanci M, Bhatia M, Ganiyusufoglu KA, et al. Degenerative lumbar spinal stenosis: correlation with Oswestry Disability Index and MR imaging. European Spine J. 2008;17(5):679–685. doi:10.1007/s00586-008-0646-5
59. Wong WH. Mild Interlaminar decompression for the treatment of lumbar spinal stenosis: procedure description and case series with 1-year follow-up. Clin J Pain. 2012;28(6):534–538. doi:10.1097/AJP.0b013e31823aaa9d
60. O’Toole JE, Eichholz KM, Fessler RG. Surgical site infection rates after minimally invasive spinal surgery. J Neurosurg Spine. 2009;11(4):471–476. doi:10.3171/2009.5.SPINE08633
61. Benyamin RM, Staats PS. MiDAS ENCORE: randomized controlled study design and protocol. Pain Physician. 2015;18(4):307–316. doi:10.36076/ppj.2015/18/307
62. Lingreen R, Grider JS. Retrospective review of patient self-reported improvement and post-procedure findings for mild (minimally invasive lumbar decompression). Pain Physician. 2010;13(6):555–560.
63. Foundation CC. New mild procedure for lumbar spinal stenosis. 2017
64. Mobbs RJ, Li J, Sivabalan P, Raley D, Rao PJ. Outcomes after decompressive laminectomy for lumbar spinal stenosis: comparison between minimally invasive unilateral laminectomy for bilateral decompression and open laminectomy: clinical article. J Neurosurg Spine. 2014;21(2):179–186. doi:10.3171/2014.4.SPINE13420
65. Shih P, Wong AP, Smith TR, Lee AI, Fessler RG. Complications of open compared to minimally invasive lumbar spine decompression. J Clin Neurosci. 2011;18(10):1360–1364. doi:10.1016/j.jocn.2011.02.022
66. Podichetty VK, Spears J, Isaacs RE, Booher J, Biscup RS. Complications associated with minimally invasive decompression for lumbar spinal stenosis. J Spinal Disord Tech. 2006;19(3):161–166. doi:10.1097/01.bsd.0000188663.46391.73
67. Phan K, Mobbs RJ. Minimally invasive versus open laminectomy for lumbar stenosis: a systematic review and meta-analysis. Spine. 2016;41(2):E91–e100. doi:10.1097/BRS.0000000000001161
68. Yang JC, Kim SG, Kim TW, Park KH. Analysis of factors contributing to postoperative spinal instability after lumbar decompression for spinal stenosis. Korean J Spine. 2013;10(3):149–154. doi:10.14245/kjs.2013.10.3.149
69. Staats PS, Hagedorn JM, Reece DE, Strand NH, Poree L. Percutaneous image-guided lumbar decompression and interspinous spacers for the treatment of lumbar spinal stenosis: a 2-year medicare claims benchmark study. Pain Pract. 2023;23(7):776–784. doi:10.1111/papr.13256
70. Staats PS, Dorsi MJ, Reece DE, Strand NH, Poree L, Hagedorn JM. Percutaneous image-guided lumbar decompression and outpatient laminectomy for the treatment of lumbar spinal stenosis: a 2-year Medicare claims benchmark study. Interv Pain Med. 2024;3(2):100412. doi:10.1016/j.inpm.2024.100412
71. Shabat S, Arinzon Z, Gepstein R, Folman Y. Long-term follow-up of revision decompressive lumbar spinal surgery in elderly patients. J Spinal Disord Tech. 2011;24(3):142–145. doi:10.1097/BSD.0b013e3181de4b61
72. Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis: an update. Curr Opin Anaesthesiol. 2017;30(5):598–603. doi:10.1097/ACO.0000000000000495
73. Turner JA, Deyo RA, Loeser JD, Von Korff M, Fordyce WE. The importance of placebo effects in pain treatment and research. JAMA. 1994;271(20):1609–1614. doi:10.1001/jama.1994.03510440069036
74. Niemansburg SL, van Delden JJ, Dhert WJ, Bredenoord AL. Reconsidering the ethics of sham interventions in an era of emerging technologies. Surgery. 2015;157(4):801–810. doi:10.1016/j.surg.2014.12.001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sex Differences in the Mediating Effect of Kinesiophobia on Chronic Pain, Dysesthesia, and Health-Related Quality of Life in Japanese Individuals Aged 65 Years Old and Older Treated with Surgery for Lumbar Spinal Stenosis
Higuchi D, Kondo Y, Watanabe Y, Miki T
Journal of Pain Research 2022, 15:1845-1854
Published Date: 30 June 2022
Use of QR Codes for Promoting a Home-Based Therapeutic Exercise in Patients with Lumbar Disc Herniation and Lumbar Spinal Stenosis: A Prospective Randomized Study
Chang MC, Park D, Choo YJ
Journal of Pain Research 2022, 15:4065-4073
Published Date: 23 December 2022
Lumbar Spinal Stenosis and Minimally Invasive Lumbar Decompression: A Narrative Review
Yuan H, Yi X
Journal of Pain Research 2023, 16:3707-3724
Published Date: 6 November 2023