")
Back to Journals » Clinical Ophthalmology » Volume 19
Multi-Stage Reconstructive Surgery of the Eyeball with No Light Perception After Severe Open Globe Injury
Authors Lytvynchuk LM , Ponomarov M, Carlos Reyna E , Stieger K, Andrassi-Darida M
Received 6 July 2024
Accepted for publication 28 January 2025
Published 12 March 2025 Volume 2025:19 Pages 847—856
DOI https://doi.org/10.2147/OPTH.S474942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lyubomyr M Lytvynchuk,1,2 Makar Ponomarov,1 Erick Carlos Reyna,1 Knut Stieger,1 Monika Andrassi-Darida1
1Department of Ophthalmology, University Hospital Giessen and Marburg GmbH, Campus Giessen, Justus-Liebig-University Giessen, Giessen, 35392, Germany; 2Karl Landsteiner Institute for Retinal Research and Imaging, Wien, 1030, Austria
Correspondence: Monika Andrassi-Darida, Department of Ophthalmology, University Hospital Giessen and Marburg GmbH, Campus Giessen, Justus-Liebig-University Giessen, Friedrichstrasse 18, Giessen, 35392, Germany, Tel +4964198543820, Fax: +4964198543809, Email [email protected]
Purpose: To analyze the visual and anatomical outcomes of multi-stage reconstructive surgery of the eyeball with no light perception (NLP) in patients after severe open globe injury (OGI).
Patients and methods: In this retrospective consecutive case series study, medical records of patients with severe OGI with visual loss up to NLP, who were referred to our clinic between February 1, 2016, and March 30, 2021, were included. The analysis of epidemiologic data, type and severity of OGI, timing and type of surgical treatment, and anatomical and functional results was performed.
Results: Nine patients met our inclusion criteria. The mean age was 52 years (range 34– 78 years). Mean follow-up was 24 months (range 1– 56 months). Estimated mean best corrected visual acuity (BCVA) was 2.92 LogMAR immediate after trauma, 2.27 LogMAR before reconstructive anterior segment surgery and 2.42 LogMAR at last follow-up. The functional gain after the primary repair was highly significant (p 0.005), but a non-significant gain was seen at the last follow-up. Retina reattachment was achieved in most of the cases (6/7, 85.7%), but these remained silicone oil dependent (5/6, 83.33%). In all cases, it was possible to prevent primary enucleation.
Conclusion: The multi-stage reconstructive surgical approach allowed for saving the eyes and improved the functional and anatomical condition. Despite the severity of OGI and NLP, an early surgical intervention should be considered by experienced surgeons.
Keywords: open globe injury, no light perception, multi-stage reconstructive surgery, vitreoretinal surgery, black diaphragm intraocular lens, retention sutures
Introduction
Severe open globe injury (OGI) is a major cause of profound visual disturbance or even eye loss in different age groups. Perforating and penetrating eye injury, which are often associated with loss of intraocular tissue (iris, lens, choroid, retina), may result in dramatic impairment of visual function up to no light perception (NLP).1,2 Low or absent visual function in the posttraumatic period is not the only predictive factor. The severity of the mechanical injury itself, as described by the Birmingham Eye Trauma Terminology (BETT) classification and the ocular trauma score (OTS), determines the chances of postoperative anatomical and functional results.1,3
Due to the development of modern surgical technologies and techniques, as well as advances in knowledge of pathophysiology and management of eye trauma, an attempt to restore eye anatomy and function even in the most severe cases becomes a choice for the surgeon.4,5 In OGI with NLP, a primary wound closure with consecutive conservative treatment or primary enucleation/evisceration of the eye is no longer a common approach. Through exploratory vitrectomy in severe ocular trauma with NLP, a visual recovery was achieved in some of the patients with profound functional and psychosocial implications.6–19 However, there is a high risk for further complications, such as phthisis bulbi, posttraumatic inflammation, sympathetic ophthalmia in the healthy eye, and psychological trauma due to the loss of visual function.20–22
Given the controversy concerning the management of eyes presenting with NLP after sever OGI, we present a study of nine consecutive patients with initial profound visual loss up to NLP, who partially improved in vision following primary repair and subsequent reconstructive anterior segment surgery.
The aim of our study is to analyze the anatomical and functional results of multi-stage reconstructive surgical treatment of patients with severe OGI with visual loss up to NLP. We describe the characteristics of eye injury, initial condition of the injured eye, and functional and anatomic outcomes.
Methods
Ethics Statement
This retrospective observational study was performed at the Department of Ophthalmology, University Hospital Giessen and Marburg GmbH, Campus Giessen, Justus-Liebig-University Giessen (Giessen, Germany) with the aim to analyze the efficacy of reconstructive surgery for the treatment of severe OGI. The medical records of consecutive cases treated between February 1, 2016, and March 30, 2021, were included. The study protocol was approved by the Ethics Committee of the Justus-Liebig-University (Giessen, Germany) (AZ 51/21) and matched the tenets of the Declaration of Helsinki. Patients were fully informed about the purpose of the study prior to providing their consent. In all cases, a signed consent was obtained from the patients before every surgical step.
Patients
The main inclusion criteria were severe OGI with visual loss up to NLP (LogMAR < 1.9), aniridia and aphakia. Additionally, the eye condition of the patients was classified according to BETT and OTS (Table 1).
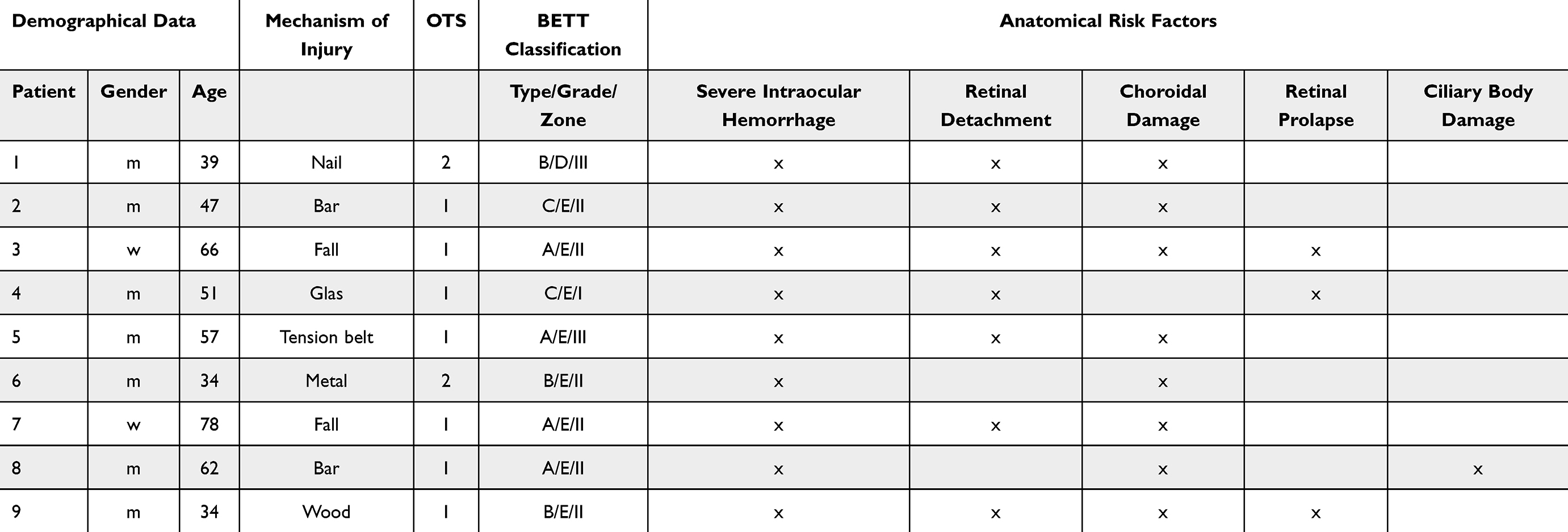 |
Table 1 Epidemiological Data, Type and Severity of OGI (BETT and OTS)1 Type A Rupture, B Penetrating, C Intraocular Foreign Body, D Perforating, E Mixed. Grade (Visual Acuity) A ≥20/40, B 20/50 to 20/100, C 19/100 to 5/200, D 4/200 to Light Perception, E No Light Perception Zone I Cornea and Limbus, Zone II Limbus to 5 mm Posterior Into Sclera, Zone III Posterior to 5 mm From the Limbus |
The need for multi-stage reconstructive surgery, which included primary repair, reconstructive anterior segment surgery with implantation of a black diaphragm intraocular lens and surgery for complications, was the second main inclusion criteria.
The main exclusion criteria were the presence of visual function better than hand movement (LogMAR < 2.3) and patients with known mental disorders. The age of the patients was not a limiting factor in our study and is depicted in Table 2.
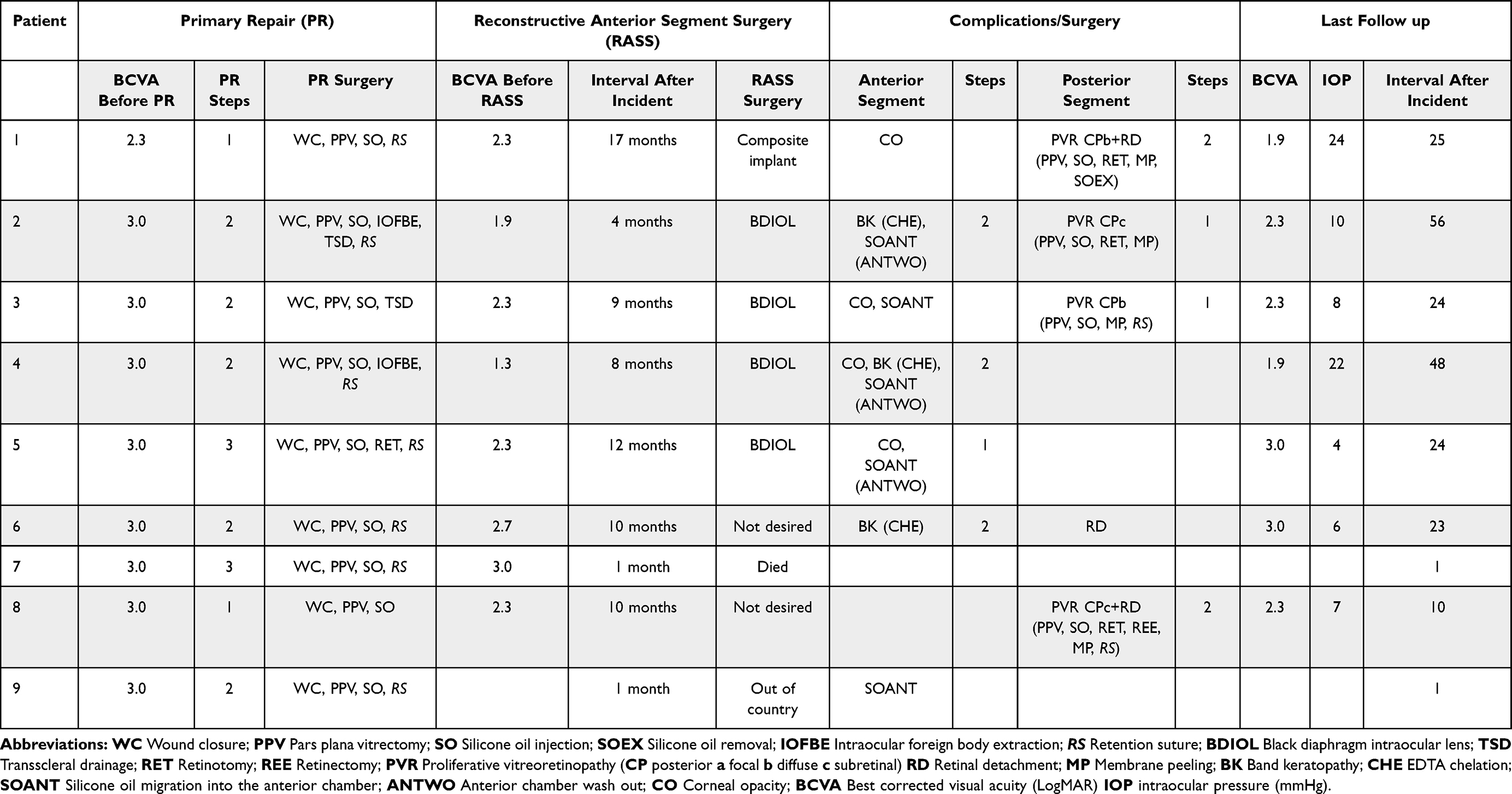 |
Table 2 Functional Outcome, Surgical Procedures and Complications |
Examination Techniques
Standardized ophthalmological examination, performed in every patient, consisted in measuring the best-corrected visual acuity (BCVA) in LogMAR using ETDRS charts or the semiquantitative scale (counting finger, hand motion, light perception, no light perception), Goldmann tonometry, slit-lamp biomicroscopy and binocular indirect fundus ophthalmoscopy. The initial posttraumatic BCVA as well as BCVA after primary repair and reconstructive anterior segment surgery was measured by three experienced ophthalmologists independently. In cases with poor vision (counting finger, hand motion, light perception and no light perception), commonly used LogMAR conversion was employed (1.9, 2.3, 2.7 and 3.0, respectively).23 While ultrasound examination was performed before and after primary repair (EyeCubed, Ellex, Mawson Lakes, Australia), wide-field digital retinal imaging (Clarus 500, Carl Zeiss Meditech, Oberkochen, Germany), spectral domain optical coherence tomography (SD-OCT Spectralis®, Heidelberg Engineering GmbH, Heidelberg, Germany) and slit-lamp photography (BX 900, Haag-Streit, Köniz, Switzerland) were performed after surgery.
Surgical Procedures
All surgeries were performed by one experienced surgeon (LL). The multi-stage reconstructive surgery consisted in primary repair, reconstructive anterior segment surgery and surgery for complications at the anterior and posterior segment. In order to prevent the development of a phthisis bulbi, a frequent complication after severe OGI, we planned a long-term silicone oil tamponade.
Primary repair was achieved within 2 weeks after the incident by wound closure followed by further surgical steps depending on the type of OGI (intraocular foreign body extraction, pars plana vitrectomy, silicone oil injection, whenever possible placement of silicone oil retention sutures and whenever needed transscleral drainage of choroidal bleeding and retinotomy). Retention sutures consisted of two pairs of perpendicular sutures (Prolene 10.0) placed at 1 mm posterior to the limbus, creating an inner square less then 4 × 4 mm.
Reconstructive anterior segment surgery was performed as soon as the posterior segment was stabilized in order to attenuate photophobia and ameliorate cosmesis. An aniridia intraocular lens type Morcher 67G (Morcher GmbH, Stuttgart, Germany) or a composite implant (Customflex Iris Implant with fiber, Human Optics, Erlangen, Germany and Soleko I71FLL SFF, Menicon Group, Pontecorvo, Italy) was sutured to the sclera.
Further, surgery was needed to treat complications at the anterior and posterior segment: anterior chamber wash out in case of silicone oil migration into the anterior chamber, EDTA chelation (application of 3% ethylenediaminetetraacetic acid) for band keratopathy, pars plana vitrectomy combined with membrane peeling, retinotomy and/or retinectomy for proliferative vitreoretinopathy (graded according to the Updated Retina Society Classification 1991 as PVR CP a,b,c) and retinal detachment.
All surgeries were video documented with the operating microscope (Rescan 700, Carl Zeiss Meditech, Oberkochen, Germany).
Statistical methods
Statistical analysis of BCVA before primary repair, before reconstructive anterior segment surgery and at the last follow-up examination was performed by a linear mixed model in order to describe the repeated measurement structure of the data. The model was fit using restricted maximum likelihood using SPSS (SPSS Statistics for Windows, Version 29.0.2.0, IBM Corp, Armonk, New York, USA) to evaluate the influence of time steps on BCVA (dependent variable). The number of anatomical risk factors for each patient was included into the model as confounder and marginal means were estimated. Pairwise comparisons were adjusted by the Bonferroni method. The normality of residuals was examined using qq-plots.
Results
Patients
Nine patients with OGI, referred and treated between February 1, 2016, and March 30, 2021, at the Department of Ophthalmology of the University Hospital Giessen and Marburg GmbH, Campus Giessen (Giessen, Germany) were included in this study, consisting of two women (22.2%) and seven men (77.8%) (Table 1). Mean age at presentation was 52 years (range 34 to 78 years). Mean follow-up was 24 months (range 1 to 56 months). In two cases, follow-up was very short (1 month) as patient 7 died and patient 9 was out of country. Therefore, these cases have not been considered for the assessment of complications and final outcome.
Type of OGI was determined by BETT classification and depicted in Table 1. Rupture of the globe (OGI type A) occurred in 4 cases (4/9, 44.4%), penetrating injury (OGI type B) in 3 cases (3/9, 33.3%) and intraocular foreign body (OGI type C) in 2 cases (2/9, 22.2%). BCVA at presentation was NLP (Grade E) in 8 cases (8/9, 88.9%) and hand motion (Grade D) in one case (1/9, 11.1%). In most of the cases (7/9 cases, 77.8%), the wound was localized in Zone II, whereas Zone I and III was involved in one case each (1/9, 11.1%).
All OGI cases showed multiple anatomical risk factors: severe intraocular hemorrhage and choroidal damage in all cases (9/9, 100%), retinal detachment in almost all cases (8/9, 88.9%), retinal prolapse in 3 cases (3/9, 33.3%), and ciliary body damage in one case (1/9, 11.1%). The very low OTS scores (2 in 2 cases and 1 in 7 cases) reflect the severity of OGI and reduced prognosis in all cases (Table 1).
Functional and Anatomical Outcomes
Partial anatomical and visual recovery was achieved in this case series (Table 2). Estimated mean best corrected visual acuity (BCVA) was 2.92 LogMAR immediate after trauma, 2.27 LogMAR before reconstructive anterior segment surgery and 2.42 LogMAR at last follow-up. The functional gain after the primary repair was highly significant (p 0.005), but a non-significant gain was seen at the last follow-up. At the last follow-up examination, an improvement in BCVA was seen in 5 patients (5/7, 71.4%), whereas 4 patients (4/5, 80%) with initially NLP recovered to better function.
Retina reattachment was achieved in most of the cases (6/7, 85.7%), but these remained silicone oil dependent (5/6, 83.33%). Mean intraocular tension at last follow-up was 11.6 mmHg (range 4–24 mmHg). No enucleation was needed. Figure 1 illustrates a representative multimodal imaging (case 3) showing the anatomical results after reconstructive surgery.
 |
Figure 1 Anatomical results after multi-stage reconstructive surgery in case 3. (A) Ultrasound of the injured eye (B) Slit-lamp photography after surgery for proliferative vitreoretinopathy (PVR) shows silicone oil retention sutures with posttraumatic aniridia (C) Anterior segment OCT shows retention sutures (D) Ultrasound after primary repair shows attached retina (E) Wide field fundus photography after primary repair shows attached retina with triamcinolone acetonide intravitreal (F) OCT shows posttraumatic intraretinal edema (G) Slit-lamp photography after implantation of black diaphragm intraocular lens. |
The most frequent complications at the anterior segment were band keratopathy in 3 patients (3/7, 42.9%), corneal opacity in 4 patients (4/7, 57.1%) and migration of silicone oil into the anterior chamber in 4 patients (4/7, 57.1%) (Table 2). At the posterior segment, proliferative vitreoretinopathy occurred in 4 patients (4/7, 57.1%) and tractional retinal detachment in 3 patients (3/7, 42.9%).
Surgical Procedures
Primary repair succeeded in one session in 2 patients (2/9, 33%), whereas 2 steps were needed in 5 patients (5/9, 55.6%) and 3 steps in 2 patients (2/9, 22.2%). Retention sutures were placed during the primary repair in 7 patients (7/9, 78.8%) and during surgery for complications in 2 patients (2/9, 22.2%) (Table 2).
Reconstructive anterior segment surgery was performed in 5 patients (5/7, 71.4%) at 4–17 months after trauma (Table 2). In patient 2, implantation of the black diaphragm intraocular lens was performed 4 months after trauma with consecutive surgery for proliferative vitreoretinopathy 3 months later.
Surgery for complications was needed in a total of 6 patients (6/7, 85.7%): in 5 patients for complications either at the anterior or at the posterior segment and in 1 patient for complications in both segments (Table 2).
Discussion
Surgical treatment of severe grade OGI remains challenging and its results continue to be hardly predictable. The complexity of the OGI with multiple damage of different intraocular tissues with a high risk of postoperative intraocular inflammation exacerbates the postoperative course after primary repair making the decision regarding further surgical intervention more difficult. Extensive damage and/or loss of the iris and ciliary body is considered to be one of the most important risk factors for developing posttraumatic hypotony with further development of the phthisis bulbi. Posttraumatic absence of light perception is an additional functional parameter, which should be considered and discussed if possible, with the patient before any surgery in terms of postoperative visual prognosis. Severity and complexity of the open globe injury remains the main prognostic factor, which determines the visual and anatomical outcomes of surgical treatment. Two other important factors are the timing and the type of surgical intervention.
In this study, we report the 2-year follow-up results of multi-stage reconstructive surgery in patients, with severe grade open globe injury presenting with visual loss up to no light perception. In our case series, we applied a surgical approach, which consisted of two major steps: first – primary wound repair and second – reconstructive anterior segment surgery. During the first steps, the primary wound closure with simultaneous or postponed main intraocular intervention with application of silicone oil retention sutures was performed within 2 weeks after the incident. The second step was aimed to correct aphakia and aniridia through implantation of a black iris diaphragm. Additional surgical interventions were performed due to the development of complications at the anterior or posterior segment, such as band keratopathy, silicone oil migration into the anterior chamber, proliferative vitreoretinopathy or retinal detachment.
In 2011, Feng et al reported the study results regarding prognostic indicators for NLP after OGI (Eye Injury Vitrectomy Study).11 The study focuses on characteristics of the eye trauma, type of surgical intervention, functional and anatomical outcomes of injured eyes of 33 patients (33 eyes) with OGI presenting with NLP after exclusion of silicone-oil sustained or hypotonic eyes. Additionally, the authors investigated and described the prognostic factors, which could determine the visual and functional results. The study reveals seven factors, which could be possible predictors of poor prognosis: rupture, open globe III, scleral wound ≥10 mm, ciliary body damage, severe intraocular hemorrhage, closed funnel retinal detachment or retinal prolapse, and choroidal damage. The authors also state that, the injured eyes can be partially anatomically restored through application of vitreoretinal surgical approaches with improvement of BCVA to LP or better having the number of poor predictors decreased. In our cohort, we also analyzed the severity of the OGI using these predictors and noticed similar tendency. Compared to silicone sustained eye (6/7 or 85.7% of eyes in our cohort, 30/39 or 76.9% of eyes in the study of Feng et al) in our cases, visual gain was much lower (counting finger to 20/200, respectively). A similar low increase in visual function was published in a series of 25 patients with OGI, in which only 4 patients (16%), who underwent vitreoretinal surgery, reached hand motion or light perception.16 Hence, it has to be considered that the severity of every predicting factor or damage can vary from mild to severe with impact on the predictability of the visual and anatomical outcome.
In 2012, Agrawal et al reported the surgical and visual outcomes of 172 patients (172 eyes) with OGI.12 Out of 172 patients, 27 (15.7%) eyes were presented with NLP. After surgical intervention, in 18 eyes (66.7%) BCVA remained NLP. In 9 eyes (33.3%), final BCVA increased from LP to 20/50-20/200. The median follow-up was 18.9 months. Additionally, the authors indicated the factors, which contributed to poor postoperative outcome: presence of relative afferent pupillary defect, extension of the wound into zone III, and associated vitreoretinal trauma. This study concluded that the absence of LP should not be an indication for primary enucleation or evisceration. This is in accordance with the guidelines for the treatment of NLP eyes induced by mechanical ocular trauma (Recommendation 12).19
Vitreoretinal surgery during primary repair or as a delayed surgical step (day 8–14 after incident) requires filling with oil as postoperative tamponade.4,5 Silicone oils are responsible for a variety of corneal changes, particularly in aphakic eyes.24 The risk of silicone oil-associated keratopathy can be reduced by placement of retention sutures and/or artificial iris-lens diaphragm in order to create a barrier between the anterior and posterior segment of the eye and prevent migration of silicone oil into the anterior chamber.
Chamber retaining sutures have been used in the beginning to protect the cornea during anterior segment surgery.25,26 In 2010, Gentile and Eliott described 3 cases in which they created an artificial iris diaphragm by placing 4 sutures in the anterior chamber at 1 mm posterior to the limbus to form a 5–6 mm central square which they referred to as retention sutures.27 Mayer et al published in 2020 a case series of 7 patients, in which a grid-like suture prevented silicone oil migration into the anterior chamber in all patients with posttraumatic aniridia and aphakia.28
Beyond creating a stable barrier between the anterior and posterior segment of the eye, artificial iris-lens diaphragm decreases photophobia and partially corrects refractive error in patients with posttraumatic aniridia and aphakia. Different devices have been used over time as implantation, and fixation and cosmetic results were constantly improved.28–30 In 2015 Qiu et al reported long-term efficacy and complications of black diaphragm intraocular lens implantation in eyes with posttraumatic aniridia.31 This study presented the results of 95 patients treated with black diaphragm intraocular lens implantation compared to 75 patients who wore rigid gas-permeable contact lenses. The authors concluded that implantation of black diaphragm intraocular lens could be effective in a matter of glare disability reduction, improvement of visual function and correction of cosmetic issues. However, the risk of long-term complications, such as glaucoma, corneal decompensation, insufficiency of limbal stem cells, and decentration of the lens should be seriously considered.
In our case series, retention sutures as well as an artificial iris-lens diaphragm were used in all patients in order to reconstruct anatomical structures as we have left the silicone oil in the eye in order to prevent progression to hypotony and ocular atrophy.2,13,19 In comparison to published data, silicone oil migration into the anterior chamber was found in 57.1% of our cases, which could be attributed to an onset of phthisis bulbi in silicone oil filled eyes. In the future, implantation of a silicone oil filled foldable capsular vitreous body, which has already been tested in patients with NLP after severe ocular trauma, will probably be able to solve this problem.32
The Limitations of This Study Include
The small number of cases and polymorphism of the OGI could be one of the limitations, as it makes any systemic analysis, including statistical analysis, more complex and difficult. However, the incidence and complexity of the eye injury are unpredictable and can differ depending on the clinic and country. The accuracy of measurement of the posttraumatic BCVA in patients with severe grade OGI is also considered as a limitation of this study, as it is relatively difficult to detect the visual function in patients, in which psychologic and/or general condition is usually affected. That is why the reported light perception could be misinterpreted by the patients, as well as by the ophthalmologists. Missing follow-ups in some cases could also be a limitation of this study. The reason could be a misunderstanding on the patient side regarding subsequent reconstructive surgical steps, which could not restore visual function completely. Therefore, repeated dialogues with the patients are necessary in order to make the surgeon’s efforts more understandable and allowing an optimal decision-making strategy in the management of posttraumatic and postoperative complications. Another limitation of this study is the hypothesis of vision recovery after surgical treatment in eyes with NLP after OGI. We suppose that the severe functional disorder is multifactorial and the multi-stage surgical treatment could address anatomical features of the eye, which are responsible for the visual function.
Conclusion
Treatment strategy of severe open globe injury with initial NLP continues to be challenging and undefined. In spite of an established classification of mechanical eye injury, there is no unique agreement on how to repair a certain type of OGI. With recently released guidelines, an evidence-based diagnostical and therapeutical approach is now available.19
In our study, we describe anatomical and functional results of multi-stage reconstructive surgery on eyes with OGI and visual loss up to NLP. The main aim of this approach remains restoring and preserving the anatomy, improving the visual function and managing late complications.
Overall, after severe OGI, the absence of LP should not be a direct indication for removal of the eye, and surgical reconstruction of the eye should be considered in majority of cases.
Acknowledgments
We would like to thank Dr. Jörn Pons-Kühnemann (Medical Statistics, Institute of Medical Informatics, Justus-Liebig-University Giessen, Germany) for the support in the statistical processing of the data.
Funding
No funds, grants or other support was received.
Disclosure
Dr Lyubomyr Lytvynchuk is the Advisory Board member for ROCHE, outside the submitted work. The authors have no other relevant financial or non-financial interests to disclose for this work.
References
1. Kuhn F, Morris R, Witherspoon CD. Birmingham Eye Trauma Terminology (BETT): terminology and classification of mechanical eye injuries. Ophthalmol Clin North Am. 2002;15:139–143. doi:10.1016/s0896-1549(02)00004-4
2. Feng K, Wang CG, Hu YT, et al. Clinical features and prognosis of eyeball rupture: eye injury vitrectomy study. Clin Exp Ophthalmol. 2015;43:629–636. doi:10.1111/ceo.12534
3. Kuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD. The Ocular Trauma Score (OTS). Ophthalmol Clin North Am. 2002;15:163–165. doi:10.1016/s0896-1549(02)00007-x
4. Joussen AM, Müller B, Kirchhof B, Stappler T, Zeitz O. Rupture of the globe: what to do, what not to do. Klin Monbl Augenheilkd. 2020;237:1070–1078. doi:10.1055/a-1233-8997
5. Kuhn F. Wahl des Zeitpunkts für die Rekonstruktion bei schweren mechanischen Augenverletzungen. Kompass Ophthalmol. 2018;4:8–13. doi:10.1159/000485017
6. Hui Y, Wang L, Shan W. Exploratory vitrectomy for traumatized eyes with no light perception and dense vitreous hemorrhage. Zhonghua Yan Ke Za Zhi. 1996;32:450–452.
7. Dong F, Dai R. The surgical treatment of traumatized eyes with no light perception. Zhonghua Yan Ke Za Zhi. 2002;38:657–659.
8. Wang YN, Shen LJ, Wang CG, et al. Prognosis of traumatic eyes with no light perception undergone vitrectomy and analysis of risk factors. Zhonghua Yan Ke Za Zhi. 2007;43:340–345.
9. Salehi-Had H, Andreoli CM, Andreoli MT, Kloek CE, Mukai S. Visual outcomes of vitreoretinal surgery in eyes with severe open-globe injury presenting with no-light-perception vision. Graefes Arch Clin Exp Ophthalmol. 2009;247:477–483. doi:10.1007/s00417-009-1035-4
10. Heidari E, Taheri N. Surgical treatment of severely traumatized eyes with no light perception. Retina. 2010;30:294–299. doi:10.1097/IAE.0b013e3181babd75
11. Feng K, Hu YT, Ma Z. Prognostic indicators for no light perception after open-globe injury: eye injury vitrectomy study. Am J Ophthalmol. 2011;152:654–662.e2. doi:10.1016/j.ajo.2011.04.004
12. Agrawal R, Wei HS, Teoh S. Predictive factors for final outcome of severely traumatized eyes with no light perception. BMC Ophthalmol. 2012;12:16. doi:10.1186/1471-2415-12-16
13. Yang SS, Jiang T. Vitrectomy combined with silicone oil tamponade in the treatment of severely traumatized eyes with the visual acuity of no light perception. Int J Ophthalmol. 2013;6:198–203. doi:10.3980/j.issn.2222-3959.2013.02.18
14. Soni NG, Bauza AM, Son JH, Langer PD, Zarbin MA, Bhagat N. Open globe ocular trauma: functional outcome of eyes with no light perception at initial presentation. Retina. 2013;33:380–386. doi:10.1097/IAE.0b013e318263cefb
15. Ren H, Jiang R, Xu G, et al. Evaluation of endoscopy assisted vitrectomy for the treatment of severe traumatic eyes with no light perception. Zhonghua Yan Ke Za Zhi. 2014;50:194–196.
16. Han YS, Kavoussi SC, Adelman RA. Visual recovery following open globe injury with initial no light perception. Clin Ophthalmol. 2015;9:1443–1448. doi:10.2147/OPTH.S87852
17. Bhagat N, Turbin R, Langer P, et al. Approach to management of eyes with no light perception after open globe injury. J Ophthalmic Vis Res. 2016;11:313–318. doi:10.4103/2008-322X.188388
18. Boucenna W, Taright N, Delbarre M, et al. Functional results and prognostic factors in open-globe ocular trauma with presenting visual acuity of no-light perception. J Fr Ophtalmol. 2020;43:517–524. doi:10.1016/j.jfo.2019.11.006
19. Yan H, Yang K, Ma Z, et al. Guideline for the treatment of no light perception eyes induced by mechanical ocular trauma. J Evid Based Med. 2022;15:302–314. doi:10.1111/jebm.12496
20. He B, Tanya SM, Wang C, Kezouh A, Torun N, Ing E. The incidence of sympathetic ophthalmia after trauma: a meta-analysis. Am J Ophthalmol. 2022;234:117–125. doi:10.1016/j.ajo.2021.06.036
21. Hudson JL, Fan JC, Smiddy WE, Sridhar J, Yannuzzi NA, Hw F Jr. Acute- and delayed-onset endophthalmitis after open globe injuries: clinical features and visual acuity outcomes. Retina. 2023;43:594–599. doi:10.1097/IAE.0000000000003707
22. Keys J, Dempster M, Jackson J, Williams M, Coyle S. The psychosocial impact of losing an eye through traumatic injury and living with prosthetic restoration: a thematic analysis. Acta Psychol. 2021;219:103383. doi:10.1016/j.actpsy.2021.103383
23. Moussa G, Bassilious K, Mathews N. A novel excel sheet conversion tool from Snellen fraction to LogMAR including `counting fingers`, `hand movement`, `light perception` and `no light perception`and focused review of literature of low visual acuity reference values. Acta Ophthalmol. 2021;99:e963–e965. doi:10.1111/aos.14659
24. Ferrara M, Coco G, Sorrentino T, et al. Retinal and corneal changes associated with intraocular silicone oil tamponade. J Clin Med. 2022;11:5234. doi:10.3390/jcm11175234
25. Wilson RP, Moster MR. The chamber-retaining suture revisited. Ophthalmic Surg. 1990;21:625–627.
26. Simcoe CW. Retaining devices for protection of corneal endothelium. J Am Intraocul Implant Soc. 1979;5:234–236. doi:10.1016/s0146-2776(79)80124-x
27. Gentile RC, Eliott D. Silicone oil retention sutures in aphakic eyes with iris loss. Arch Ophthalmol. 2010;128:1596–1599. doi:10.1001/archophthalmol.2010.300
28. Mayer CS, Baur I, Storr J, Markard A, Khoramnia R. Surgical management for silicone oil barrier of traumatic aniridia with aphakia: suturing of temporary iris-diaphragm prior to final iris-lens-diaphragm implantation. Clin Ophthalmol. 2020;14:4439–4450. doi:10.2147/OPTH.S284159
29. Spitzer MS, Yoeruek E, Leitritz MA, Szurman P, Bartz-Schmidt KU. A new technique for treating posttraumatic aniridia with aphakia: first results of haptic fixation of a foldable intraocular lens on a foldable and custom-tailored iris prosthesis. Arch Ophthalmol. 2012;130:771–775. doi:10.1001/archophthalmol.2011.1778
30. Krishnan VM, Todorova MG, Wiechens B, Valmaggia C, Varde M. The artificial iris - analysis of various implantation techniques after ocular trauma. Indian J Ophthalmol. 2021;69:3526–3531. doi:10.4103/ijo.IJO_62_21
31. Qiu X, Ji Y, Zheng T, Lu Y. Long-term efficacy and complications of black diaphragm intraocular lens implantation in patients with traumatic aniridia. Br J Ophthalmol. 2015;99:659–664. doi:10.1136/bjophthalmol-2014-305581
32. Zhang C, Xiao R, Wang A, Zhao Z. Silicone oil-filled foldable capsular vitreous body versus silicone oil endotamponade for treatment of no light perception after severe ocular trauma. Retina. 2022;42:553–560. doi:10.1097/IAE.0000000000003336
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.