")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Multidisciplinary Team Management of Hepatocellular Carcinoma in the MENA Region: Current Practices, Challenges, and Gaps
Authors El-Kassas M, Khalifa R , AlNaamani KM, Shousha H, Yilmaz Y , Sanai FM, Almattooq M , Labidi A, Akroush MWI, Debzi N, Abdelmalek MO, Abdeen NS, Tumi A, Elbadry M, El Fouly A, Marwan E, Al Suwaidi J, Elzouki AN , Alswat KA
Received 28 March 2025
Accepted for publication 26 June 2025
Published 8 July 2025 Volume 2025:12 Pages 1315—1335
DOI https://doi.org/10.2147/JHC.S528470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mohamed Shaker
Mohamed El-Kassas,1,2 Rofida Khalifa,3 Khalid M AlNaamani,2,4 Hend Shousha,5 Yusuf Yilmaz,2,6 Faisal M Sanai,2,7 Maen Almattooq,2,8 Asma Labidi,2,9 Maisam WI Akroush,2,10 Nabil Debzi,2,11 Mohamed Omar Abdelmalek,12 Nermeen Sherif Abdeen,13 Ali Tumi,2,14 Mohamed Elbadry,1,2 Amr El Fouly,1 Eman Marwan,1 Jassim Al Suwaidi,15 Abdel-Naser Elzouki,2,16 Khalid A Alswat,2,17 On behalf of the Steatotic Liver Disease Study Foundation in Middle East and North Africa (SLMENA) CollaboratorsChikhi Yazid1. 1, Saidani Khadidja2. 2, Sherif Ahmed3. 3, Hanaa Fathelbab4. 4, Mohamed Kohla5. 5, Eman Barakat6. 6, Wessam Abdellatif7. 7, Mina Tharwat8. 8, Asmaa Mohammad9. 9, Sawsan Abd El-Moniem10. 10, Asem Elfert11. 11, Yasmeen Ahmed6. 6, Mohammed Ahmed12. 12, Usama Eldaly13. 13, Essam Hassan14. 14, Fawzi Abdel-Rahman15. 15, Munira Altarrah16. 16, Dalal Alhaqqan17. 17, Elhusain Kamoka18. 18, Mustapha Benazzouz19. 19, Rashid ALSukaiti20. 20, Itrat Mehdi21. 21, Asim Jamal Shaikh22. 22, Al Warith Al Hashmi23. 23, Kakil Rasul24. 24, Kanan Alshammari25. 25, Khalid Bzeizi26. 26, Adnan Alzanbagi27. 27, Haythem Yacoub28. 28, Amal Khsiba29. 29, Nour Elleuch30. 30, Ilker Turan31. 31, Murat Kiyici32. 32, Levent Doganay33. 33, Gökhan Kabaçam34. 34, Umit Karaogullarindan35. 35, Coskun Demirtas36. 36, Cem Simsek37. 37, Sezai Yilmaz38. 38, Murat Akyildiz39. 39, Dilara Turan Gökçe40. 40, Murat Dayangac41. 41, Murat Gülşen42. 42, Yasar Tuna43. 43, Sencan Acar44. 44, Derya Ari45. 45 On behalf of the Steatotic Liver Disease Study Foundation in Middle East and North Africa (SLMENA) Collaborators
1.Interne Medicine Department, EPH Tipaza, Tipaza, Algeria.; 2.Faculty of Medicine, Algiers, Algeria.; 3.Hepatology and Gastroenterology Department, Faculty of Medicine, Zagazig University, Egypt.; 4.Tropical Medicine Department, Minia University, ElMinya, Egypt; 5.Hepatology and Gastroenterology Department, National Liver Institute, Shebeen El-Kom, Egypt.; 6.Tropical Medicine Department, Ain-Shams University, Cairo, Egypt.; 7.Radiology Department, National Hepatology & Tropical Medicine Research Institute, Cairo, Egypt.; 8.Tropical Medicine and Gastroenterology Department, Faculty of Medicine, Aswan University, Aswan, Egypt.; 9.Tropical Medicine and Gastroenterology Department, Sohag University, Egypt.; 10.Hepatology and Gastroenterology Unit, Mansoura, Egypt.; 11.Tropical Medicine Department, Tanta University, Egypt.; 12.Hepatology, Gastroenterology and Infectious Disease Department, Kafr Elsheikh, Egypt.; 13.Medical oncology Department, Damietta oncology Center, Egypt.; 14.Endemic Medicine Department, Fayoum University, Fayoum, Egypt.; 15.Private Sector, Amman, Jordan.; 16.Gastroenterology and Hepatology Department, Al Amiri Hospital, Kuwait City, Kuwait.; 17.Department of Gastroenterology, Mubarak AlKabeer Hospital, AlJabriya, Kuwait.; 18.Surgical Oncology Department, National Cancer Institute, Sabratha, Libya.; 19.Hepatology and Gastroenterology Department, Rabat International University, Rabat, Morrocco.; 20.Radiology and Nuclear Medicine, University Medical City, Muscat, Oman.; 21.Medical Oncology Department, The Royal Hospital, Muscat, Oman.; 22.Medical Oncology Department, Sultan Qaboos Comprehensive Cancer Care and Research Centre (SQCCCRC), Muscat, Oman.; 23.Hepatobiliary and liver Transplant Surgery, Royal Hospital, Muscat, Oman.; 24.Medical Oncology, NCCCR, Doha, Qatar.; 25.Department of Oncology, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia.; 26.Liver & Small Bowel Health Centre, King Faisal Specialist Hospital & Research Center Riyadh, Saudi Arabia.; 27.Gastroenterology Department, King Abdullah Medical City, Makkah, Saudi Arabia.; 28.Gastroenterology B Department, La Rabta Hospital, Tunis, Tunisie.; 29.Gastroenterology Department, Tunis El Manar University, Mohamed Tahar Maamouri Hospital Nabeul, Tunisia.; 30.Department of Gastroenterology, University of Sousse, Sousse, Tunisia.; 31.Gastroenterology Department, Ege University School of Medicine, Izmir, Turkey.; 32.Gastroenterology Department, Uludag University, Bursa, Turkey.; 33.Gastroenterology and Hepatology Department, Bau Medical School Pendik Medicalpar Hospital, İstanbul, Turkey.; 34.Liver Transplantation Department, Guven Hospital, Ankara, Turkey.; 35.Gastroenterology Department, Cukurova University, Adana, Turkey.; 36.Gastroenterology and Hepatology Department, Marmara University School of Medicine, Istanbul, Türkiye.; 37.Gastroenterology Department, Hacettepe, Ankara, Turkey.; 38.Liver Transplantation Institute, Inonu University, Malatya, Türkiye.; 39.Gastroenterology and Liver Transplantation, Koc University Hospital, Istanbul, Turkey.; 40.Gastroenterology Bilkent City Hospital, Ankara, Türkiye; 41.Department of Hepatobiliary Surgery and Liver Transplantation Istanbul Medipol University, Istanbul, Türkiye; 42.Gastroenterology Department, Gaziantep University, Gaziantep, Türkiye; 43.Antalya Medicalpark Gastroenteroloji, Medicalpark Antalya, Antalya, Turkey; 44.Gastroenterology Department, Istanbul Florence Nightingale Hospital, Istanbul, Türkiye; 45.Gastroenterology Department, Ankara Bilkent City Hospital, Ankara, Turkey; 1Endemic Medicine Department, Faculty of Medicine, Helwan University, Cairo, Egypt; 2Steatotic Liver Diseases Study Foundation in Middle East and North Africa (SLMENA), Cairo, Egypt; 3Tropical Medicine Department, Faculty of Medicine, Minia University, Minya, Egypt; 4Department of Medicine, Division of Gastroenterology and Hepatology, The Medical City for Military and Security Services, Muscat, Oman; 5Endemic Medicine and Hepato-Gastroenterology Department, Cairo University, Cairo, Egypt; 6Department of Gastroenterology, School of Medicine, Recep Tayyip Erdoğan University, Rize, Turkey; 7Gastroenterology Section, Department of Medicine, King Abdulaziz Medical City, King Abdullah International Medical Research Center, Ministry of National Guard - Health Affairs, Jeddah, Saudi Arabia; 8Gastroenterology and Hepatology Department, Jaber AlAhmad Hospital, Kuwait City, Kuwait; 9Department of Gastroenterology “A”, Rabta Hospital, Tunis, Tunisia; 10Digestive and Liver Disease Clinic, Private Sector, Faculty of Medicine, Jordan University, Amman, Jordan; 11Hepatology Department, Mustapha Bacha University Hospital, Algiers, Algeria; 12Tropical Medicine and Gastroenterology Department, Assiut University, Assiut, Egypt; 13Tropical Medicine Department, Faculty of Medicine, Alexandria University, Alexandria, Egypt; 14Medical Department, Central Hospital, Tripoli, Libya; 15Scientific, Academic, and Faculty Affairs, Hamad Medical Corporation, Doha, Qatar; 16Department of Medicine, Hamad Medical Corporation and College of Medicine, Qatar University, Doha, Qatar; 17Liver Disease Research Center, Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Mohamed El-Kassas, Endemic Medicine Department, Faculty of Medicine, Helwan University, Ain Helwan, 11795, Cairo, Egypt, Tel + 20 111 445 5552, Email [email protected]
Purpose: Hepatocellular carcinoma (HCC) is a leading cause of cancer-related mortality, with a high disease burden in the Middle East and North Africa (MENA) region. Multidisciplinary teams (MDTs) are essential for optimizing HCC management; however, their implementation and impact may vary across healthcare settings. This study evaluates the structure, decision-making processes, and challenges faced by MDTs in HCC treatment centers across the MENA region.
Patients and Methods: This cross-sectional, multicenter study surveyed representatives from 53 HCC treatment centers across 38 cities in 11 MENA countries. A structured questionnaire was electronically distributed to assess MDT composition, meeting frequency, decision-making processes, adherence to clinical guidelines, patient management pathways, and challenges in HCC treatment.
Results: Among the surveyed centers, 84.9% (n=45) reported having an established MDT. The most common specialties involved in MDT composition were hepatology (100%), interventional radiology (97.8%), medical oncology (91.1%), and hepatobiliary surgery (80%). Barcelona Clinic Liver Cancer staging was used in 95.6% of centers. Despite acknowledging MDT benefits, major challenges were documented by participants, including resource limitations (13.2%), financial constraints (13.2%), patient nonadherence (9.4%), and limited access to advanced technology (11.3%). Telemedicine was underutilized (9.4% of centers), and only 15.1% experienced participation in clinical trials.
Conclusion: Our result highlights the pivotal role of MDTs in HCC management in the MENA region, demonstrating adherence to evidence-based guidelines and exposing critical gaps in resource availability, technology integration, and patient-centered decision-making. Strengthening MDTs through enhanced resource allocation, digital health adoption, and increased clinical trial participation is essential to improving HCC outcomes in the region.
Plain Language Summary: This study identifies critical gaps in multidisciplinary hepatocellular carcinoma (HCC) management across the Middle East and North Africa (MENA). Despite recognizing multidisciplinary teams’ value, inconsistent implementation, fragmented referral pathways, limited diagnostic tool accessibility, and insufficient public awareness significantly hinder optimal patient care. Addressing these gaps urgently requires integrated national policies, expanded diagnostic infrastructure, enhanced clinician training, structured referral systems, and stronger public and patient engagement strategies. The study underscores the necessity for a strategic, coordinated approach to improve clinical outcomes and reduce the healthcare burden of HCC in the region.
Keywords: hepatocellular carcinoma, multidisciplinary team, MENA region, cancer management, clinical decision-making
Introduction
Liver cancer represents a significant global health burden, ranking sixth in incidence and third in cancer-related mortality worldwide, with an estimated 866,136 new cases in 2022.1 The disease exhibits a marked gender disparity, with males affected two to three times more frequently than females in most countries.¹ The two primary forms of liver cancer are hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma, with HCC accounting for over 90% of cases.2 Chronic infections with hepatitis B virus (HBV) or hepatitis C virus (HCV) remain the leading causes of HCC, responsible for 21–55% of cases globally.3 Other established risk factors include excessive alcohol consumption, metabolic dysfunction–associated steatotic liver disease (MASLD), smoking, dietary exposure to aflatoxins, and type 2 diabetes.4 In the Middle East and North Africa (MENA) region, the incidence, prevalence, risk factors, disease progression, and mortality rates of HCC differ significantly from those observed in Western populations, largely due to cultural, racial, and socioeconomic disparities.5 The cumulative risk of developing HCC in the MENA region is 2.18%, with a reported 37,184 new cases (25,699 in men and 11,485 in women) and 36,601 deaths (25,267 in men and 11,334 in women).5 Despite advancements in HBV and HCV prevention and treatment, HCC incidence in the region has remained high, indicating persistent challenges in disease control.6,7 Among MENA countries, Egypt serves as an example of a country with a high liver cancer burden. It has the second highest age-standardized rate of liver cancer incidence globally, following Mongolia.8 In Egypt, HCC ranks first among males, second among females, and first overall across both sexes. In 2022, the country reported 25,399 HCC cases, representing 19.7% of all cancers, highlighting the disease’s significant and growing burden.8 A survey conducted using three regional cancer registries (Damietta, Minya, and Aswan governorates) indicated that HCC accounted for 32.35% of all cancer-related deaths.8 Given the significant burden of HCC, especially in resource-limited settings such as the MENA region, effective treatment approaches are crucial.
Multidisciplinary teams (MDTs) have emerged as a key strategy in optimizing HCC management by integrating expertise from various medical specializations, including hepatologists, radiologists, surgeons, oncologists, and nurse coordinators.9,10 This collaborative approach ensures comprehensive patient care, facilitates early diagnosis, timely treatment, and enhances adherence to best clinical practices.11,12 In 1995, a Philadelphia Veterans Administration Medical Center team first used multidisciplinary liver tumor boards (MDLTBs) to treat HCC, focusing on palliative measures.13 MDTs are structured in different forms, including MDTBs, expert referral systems, and multi-physician clinics, depending on institutional resources and patient needs.14,15 Effective MDT functioning relies on accurate clinical information, interdisciplinary teamwork, consistent participation, and skilled leadership.16,17
Despite its advantages, MDT-based HCC management faces several challenges, including specialist scheduling difficulties, patient noncompliance, and prolonged treatment duration.14 MDT effectiveness may be compromised by disease progression, certain management contraindications, or patient refusal of recommended treatments.13 Additionally, delays between diagnosis and treatment initiation and financial constraints impact MDT cost-effectiveness. While MDTs primarily focus on diagnosis and treatment, they often place less emphasis on preventive strategies, leading to unchanged at-risk HCC screening rates.15
In the MENA region, comprehensive data on MDT composition, decision-making processes, operational challenges, technology integration, and resource limitations in HCC centers remain limited. Therefore, this study investigates the impact of MDTs on HCC management in MENA region by evaluating MDT presence, membership, adherence to clinical guidelines, associated challenges, and patient care quality across different phases of the clinical pathway. By addressing these knowledge gaps, this study provides a foundational assessment of MDT practices in the MENA region, offering insights that can inform future policy development and clinical improvements in HCC management.
Materials and Methods
Study Design
This cross-sectional, multicenter study evaluated the composition, functionality and impact of MDTs in managing HCC across various healthcare centers in the Middle East and North Africa (MENA) region. The study included representatives from HCC treatment centers across MENA region, ensuring a heterogeneous representation of healthcare practices, institutional structures, and cultural perspectives on HCC management.
This study was approved by the Research Ethics Committee for Human and Animal Research at the Faculty of Medicine, Helwan University, Cairo, Egypt (reference number: 151–2024).
Study Survey and Participants
The survey instrument underwent pilot testing among five senior HCC experts representing various MENA countries to ensure content validity, clarity, and relevance. Feedback from the pilot group led to minor adjustments for clarity and contextual appropriateness. The structured questionnaire was then initially distributed to 61 HCC treatment centers in 12 MENA countries, including university hospitals, governmental hospitals, specialized cancer centers, private institutions, and community hospitals. A total of 53 centers across 38 cities from 11 countries (86.9% response rate) completed the survey and were included in the final analysis. Non-respondents were initially sent two reminder emails at one-week intervals to encourage participation. Participants who did not respond after these reminders were considered non-participants, and no further contact attempts were made.
The Steatotic Liver Disease Study Foundation in the Middle East and North Africa (SLMENA) is a collaborative research initiative dedicated to advancing knowledge, clinical practice, and policy recommendations for liver diseases across the MENA region. SLMENA functions as a network of leading hepatologists and gastroenterologists, engaged in research, education, and the development of evidence-based guidelines for liver disease management. To ensure a representative and diverse sample of HCC treatment centers across the region, we leveraged the SLMENA network to facilitate participant recruitment. Invitations to participate in the survey were distributed through SLMENA’s professional database, which includes key stakeholders in hepatology and oncology from academic institutions, governmental hospitals, specialized cancer centers, private healthcare facilities, and community hospitals. Participants were purposively selected based on their direct involvement in HCC patient management, ensuring a representative sample of both academic and non-academic institutions.
To maintain data reliability and relevance, only respondents who actively participated in MDT discussions, clinical decision-making, or treatment planning for HCC patients were eligible. This selection process ensured that the study captured insights from experienced professionals working in diverse healthcare settings across the region.
Data Collection and Study Variables
Data were collected through a structured electronic questionnaire, ensuring consistent data collection across all participating centers. The questionnaire was designed to provide a comprehensive assessment of the impact of MDTs on HCC management by evaluating multiple variables, including:
- MDT composition and functionality: Specialties involved, meeting frequency, and operational structure.
- Decision-making processes: Use of staging systems, adherence to clinical guidelines, and consideration of patient preferences.
- Patient-centered approaches: Patient participation in decision-making, education on treatment options, and quality-of-life considerations.
- Follow-up protocols: Standardized follow-up pathways, palliative care practices, and long-term patient monitoring.
- Challenges in evidence-based treatment implementation: Barriers such as resource limitations, access to advanced technologies like electronic health records (EHRs), telemedicine, artificial intelligence, and adoption of advanced surgical techniques and decision-support tools.
To minimize potential sources of bias, such as selection and reporting bias, the study utilized standardized data collection methods and included a diverse range of treatment centers.
Statistical Analysis
The collected data were entered into an Excel spreadsheet and analyzed using the Statistical Package for Social Sciences (SPSS) version 26.0 (SPSS Inc., Chicago, IL, USA). The results were organized and displayed in detailed tables and figures to enhance interpretation and comparison across study parameters. Quantitative data were analyzed using descriptive statistics, specifically frequencies, percentages, means, and standard deviations. Comparisons across countries and clinical settings were conducted using chi-square and Fisher’s exact tests for categorical variables, with significance set at p < 0.05. Qualitative data were analyzed using thematic content analysis to identify recurring themes related to multidisciplinary care practices and barriers.
Results
This multicenter cross-sectional study included 53 representatives, each serving as the sole respondent for their respective HCC treatment center, from a total of 61 centers initially invited to participate (86.9%). All participants were actively involved in HCC management across the MENA region. The cohort comprised 39 males and 14 females, with a mean age of 50.1 ± 8.9 years (range: 34–70 years). The study encompassed 53 HCC treatment centers across 38 cities in 11 MENA countries, covering a range of institutional types: university hospitals (n=32), governmental hospitals (n=8), specialty cancer centers (n=5), private facilities (n=5), and community hospitals (n=3). Egypt (n=15) and Turkey (n=14) had the highest representation, while Jordan, Morocco, and Qatar each had one participating center.
Regarding clinical experience, 75.5% of respondents reported over 10 years of experience in HCC management, and 73.6% of centers had been engaged in HCC treatment for over a decade. Regarding patient volume, 35.8% of respondents indicated that their centers manage over 100 new HCC patients annually.
Notably, 84.9% of centers had an established MDT for HCC management. Among the eight centers (15.1%) without an established MDT, the most frequently reported challenges were resource limitations, insurance/financial issues, patient nonadherence, and restricted access to advanced technology. Regarding treatment planning, advanced surgical techniques or minimally invasive procedures (eg, laparoscopic resection) were always integrated into decision-making in three centers, while in another three centers, they were rarely considered due to limited expertise or equipment availability. In the remaining two centers, such procedures were only considered if conventional methods were not suitable (Table 1).
 |
Table 1 General Characteristics of the Study Participants and the HCC Treatment Centers in the MENA Region |
Composition and Function of MDTs
Among the 45 centers with an established MDT for HCC treatment, 19 centers (42.2%) reported having more than 10 members as part of their MDT. The core specialties represented in MDTs included hepatology in all centers (100%), interventional radiology in 44 centers (97.8%), medical oncology in 41 centers (91.1%), and hepatobiliary surgery in 36 centers (80%). MDT meetings were held weekly in 32 centers (71.1%), with case presentations by specialists in 35 centers (77.8%) and open discussions in 18 centers (40%). Additionally, more than 50% of HCC cases were reviewed during MDT meetings in 34 centers (75.6%). Regarding satisfaction with MDT operations, 77.8% of participants (n=35) reported being very satisfied or satisfied with the current meeting structure. In 27 centers (60%), hepatologists were identified as the primary leaders of the decision-making process during MDT discussions. In almost all centers with an established MDT (n=44; 97.8%), HCC staging was identified as the most important criterion in determining treatment plans. The Barcelona Clinic Liver Cancer (BCLC) staging system was the primary staging method used in 43 centers (95.6%). This system was incorporated into treatment decisions as a guideline alongside clinical judgment in 29 centers (64.4%), while in 15 centers (33.3%), it served as the primary basis for treatment decisions. Additionally, comorbid conditions influenced treatment decisions in 30 centers (66.7%). MDT discussions were regularly scheduled for treatment planning in 26 centers (57.8%), whereas in 18 centers (40%), discussions were conducted on a case-by-case basis. Notably, 44 participants (97.8%) either strongly agreed or agreed that all MDT members were given equal opportunities to contribute to the final treatment decision. In 34 centers (75.6%), discrepancies between treatment decisions based on clinical guidelines and those made by the MDT were observed in less than 25% of cases. MDT approval was always required before initiating HCC treatment in 23 centers (51.1%), while in 12 centers (26.7%), MDT approval was recommended but not mandatory. Additionally, an evidence-based approach was frequently utilized in selecting treatment plans in 43 centers (95.6%) (Table 2). Electronic health record (EHR) usage varied across participating HCC treatment centers. EHR systems were the primary filing method in 49.1% of centers, while 13 centers (24.5%) relied solely on paper-based filing systems, and 14 centers (26.4%) used a combination of both. The adoption of advanced technology was limited. Only 2 centers (3.8%) occasionally used artificial intelligence (AI) or machine learning tools for evaluating imaging results or predicting patient outcomes. Furthermore, 38 centers (71.7%) reported rarely or never utilizing telemedicine for treatment planning or follow-up consultations. Regarding decision-support algorithms, 9 centers (17%) extensively integrated EHR-based decision-support tools for HCC management, while 22 centers (41.5%) did not implement any form of decision-support integration (Table 3).
 |
Table 2 Functioning, Composition, Operational Structure, and Decision-Making Process of MDTs in the MENA Region |
 |
Table 3 Data Filing, Technology Use, Patient Referral and Follow-up, Clinical Trial Participation, and Decision-Making in HCC Treatment Centers in the MENA Region |
Referral to MDTs and Follow up Practice
In 41 centers (77.4%), participants highlighted the effectiveness of the current referral process in ensuring timely treatment for HCC patients. Additionally, 14 centers (26.4%) referred patients to clinical trials for new HCC treatments whenever possible, while 8 centers (15.1%) were actively involved in or conducting HCC-related clinical trials. Regarding patient follow-up after initial treatment decisions, 49.1% of centers conducted monthly follow-ups, while 41.5% followed up with patients on an as-needed basis. In-person consultations were the most commonly used follow-up method, implemented in 36 centers (67.9%), followed by scheduled check-ups in 31 centers (58.5%). In contrast, telehealth appointments were utilized in only 5 centers (9.4%) (Table 3).
In cases of treatment failure or disease progression, 36 centers (67.9%) based their subsequent treatment decisions on re-evaluation with new staging and imaging, while 10 centers (18.9%) relied on patient history and response to previous treatment. For long-term surveillance after the initial intervention, 36 centers (67.9%) conducted follow-ups every three months, whereas 12 centers (22.6%) determined follow-up schedules on a case-by-case basis. When evidence for a particular treatment was inconclusive or conflicting, 32 centers (60.4%) relied on expert opinions or multidisciplinary discussions, while 17 centers (32.1%) followed the most recent guidelines. Overall, participants from 34 centers (64.1%) reported being very satisfied or satisfied with the follow-up procedures implemented in their centers.
Decision-Making Process Within MDTs
Patient involvement in the decision-making process varied across centers. In 22 centers (41.5%), patients were engaged through detailed explanations of treatment options, while 21 centers (39.6%) discussed potential outcomes and risks with patients. The education of patients and their families on treatment options was primarily conducted through detailed verbal explanations in 46 centers (86.8%). Additionally, discussions on the potential impact of treatments on daily life and quality of life were held through regular consultations in 31 centers (58.5%), while 18 centers (34%) provided brief discussions before treatment. Post-treatment outcome assessment was limited, with only 8 centers (15.1%) utilizing standardized outcome scales to measure treatment effectiveness and quality of life. Instead, most centers relied on follow-up imaging and lab tests (73.6%) or patient self-reported outcomes (56.6%). Notably, 24 centers (45.3%) did not implement specific quality control measures to ensure adherence to scientific staging and decision-making processes.
Palliative Care Practice
The implementation of palliative care services for HCC patients varied significantly across centers. Only four centers (7.5%) incorporated palliative care early in the treatment process, whereas the majority (83%) introduced it only at advanced disease stages. Among palliative care components, pain management, and nutritional support were prioritized in approximately 90% of centers. The effectiveness of palliative interventions was commonly assessed based on clinical improvement and symptom control (56.6%), followed by family feedback (45.3%) and patient-reported outcome measures (43.4%). Several barriers to providing effective palliative care were identified. The most frequently reported challenges included limited access to specialized services (67.9%), lack of trained staff (50.9%), patient and family resistance (47.2%), and insurance/financial constraints (47.2%). The use of digital tools in palliative care was minimal, with only 8 centers (15.1%) recommending palliative care apps or supportive technologies and just 4 centers (7.5%) offering online counseling services. A large proportion (41 centers; 77.3%) relied solely on traditional care methods, with no integration of technology-based solutions. In evaluating the effectiveness of MDTs in improving HCC treatment outcomes, participants rated MDTs as excellent in 25 centers (47.2%) and good in 17 centers (32.1%) (Table 4).
 |
Table 4 Patient-Centric Approach, Outcome Measurement, and Palliative Care Services in HCC Treatment Centers in the MENA Region |
Recommendations for MDTs Improvement
Participants provided several recommendations for enhancing the efficiency and effectiveness of MDTs in HCC management. The most frequently suggested improvements included enhancing communication among MDT members (54.7%) and allocating additional resources for MDT functions, such as administrative support (52.8%). Additionally, incorporating patient feedback into treatment planning (50.9%) and offering further training on collaborative decision-making approaches (45.3%) were highlighted as key strategies to improve MDT effectiveness. Other proposed enhancements included improving access to patient data and medical records (43.4%), better defining MDT roles and responsibilities (39.6%) and increasing the frequency of MDT meetings (35.8%) to ensure continuous, coordinated decision-making. Figure 1 illustrates these suggested improvements in detail.
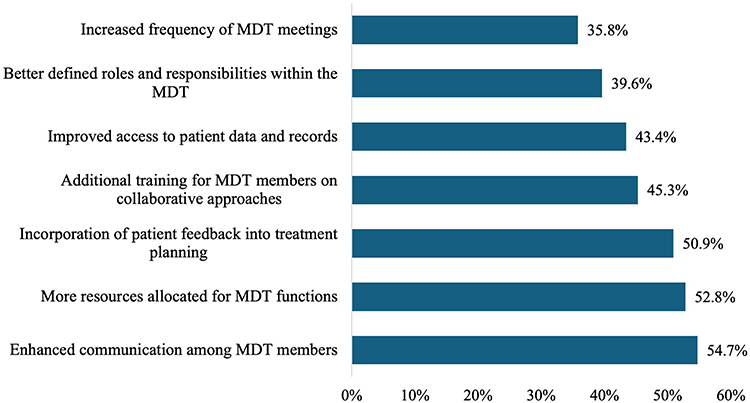 |
Figure 1 Strategies to improve the MDT processes at the HCC treatment centers in the MENA region. |
Discussion
Our study identifies several key challenges in the implementation of MDTs for HCC management across the MENA region, including resource limitations, financial constraints, and disparities in access to modern medical technologies. These barriers hinder the effective adoption of evidence-based treatment approaches and interdisciplinary collaboration. Despite these challenges, our findings suggest that weekly collaborative case discussions and adherence to evidence-based guidelines contribute significantly to improved patient outcomes. MDT members highlight the advantages of interprofessional coordination, which facilitates comprehensive treatment planning, fosters a supportive clinical environment, and enhances educational initiatives.18 The results are consistent with the study by Waked et al, which showed that improving clinical outcomes and overall survival for HCC patients in the MENA region requires multidisciplinary treatment.19 Zhang et al also found that MDT discussions influence treatment decisions and diagnostic accuracy, which are crucial for improving patient care.20
Further research on the impact of MDTs in HCC management indicates that, compared to non-MDT care, MDTs significantly enhance access to curative interventions, facilitate multidisciplinary expertise, and ensure more precise treatment planning, ultimately leading to improved survival rates.21–25 The integration of diverse specialist input enables streamlined decision-making, reducing delays in diagnosis and treatment initiation. Moreover, MDTs promote a patient-centered approach, ensuring that treatment decisions consider both clinical guidelines and individual patient factors, such as comorbidities and quality of life. Regular MDT meetings have been recognized as a critical factor in optimizing patient outcomes by fostering continuous evaluation and adaptation of treatment strategies, particularly in complex cases requiring tailored therapeutic interventions. An American study conducted in Massachusetts emphasized that frequent MDT meetings are essential for ensuring comprehensive patient assessments and individualized treatment plans.²² These structured discussions enable MDT members to systematically evaluate each case and tailor management strategies, improving the overall quality of care. Despite the recognized advantages of MDT structures, our study identified several challenges, particularly among the 15.1% of centers without established MDTs. The primary barriers to implementing evidence-based treatment regimens included resource limitations, financial constraints related to insurance coverage, and restricted access to modern medical technologies. These obstacles highlight disparities in healthcare infrastructure across the MENA region, underscoring the need for targeted interventions to enhance MDT adoption.
The core composition of MDTs in HCC centers across the MENA region typically includes hepatologists, interventional radiologists, oncologists, and hepato-biliary surgeons. In some centers, pathologists, palliative care specialists, liver transplant surgeons, nurses, radiation oncologists, and nutritionists are also included in the MDTs. Comparative analyses with Western studies indicate that MDT structures in HCC centers within the MENA region share a similar subset of specialists, with only minimal variations in the specific disciplines involved.20–29 However, key differences exist, primarily in the availability of specialized personnel, technological infrastructure, and financial constraints. Western MDTs often have greater access to advanced imaging, AI-driven diagnostic tools, and dedicated administrative support, whereas MENA centers often face resource limitations, fragmented healthcare funding, and inconsistent access to multidisciplinary expertise, particularly in non-urban regions. These disparities underscore the need for targeted resource allocation and policy interventions to enhance MDT implementation and effectiveness across diverse healthcare settings. The importance of assembling an MDT to improve patient quality of life and survival outcomes has been emphasized.10 It has also been observed that MDT discussions involving at least three medical specialties are linked to better survival outcomes, whereas consultations between only two specialists show no significant impact.30 Serper et al examined fatality rates based on the composition of MDTs and found that the inclusion of hepatologists, oncologists, and surgeons was associated with lower death rates. In contrast, the involvement of gastroenterologists and palliative care specialists had less favorable outcomes.25 Yang et al emphasized the crucial role of MDT coordinators, showing that MDTs—including surgeons, dietitians, rehabilitation specialists, psychiatrists, and nursing staff—improve quality of life and help reduce anxiety and psychological distress.31 Similarly, Yopp et al demonstrated that diverse medical providers in HCC MDTs, including surgeons, medical oncologists, and interventional radiologists, were associated with a reduced risk of treatment delays, ultimately leading to improved survival probabilities.32 A Philadelphia-based study found that HCC patients exhibited greater confidence in experts and caregivers within the MDT setting. This collaborative approach enhanced patient confidence, engagement, and adherence to therapy.18 Sinn et al highlighted that MDT-based decisions are more balanced as they incorporate comprehensive risk-benefit assessments from multiple specialists. In contrast, decisions made by a single physician tend to be influenced by personal preferences and the limitations of their specialty.28 In our study, the prevalent use of the BCLC staging system in 95.6% of the participating centers reflects its worldwide acknowledgment. Likewise, several evaluations indicated that compliance with BCLC recommendations is common among physicians in the MENA countries, reflecting our observations about the use of BCLC as a guide for treatment decisions.33–36
Several studies have conducted subgroup analyses to assess which HCC patient categories derive the greatest benefit from MDT involvement. Yopp et al found that MDT participation significantly improved survival outcomes in BCLC stages B, C, and D, whereas no clear survival advantage was observed in early-stage BCLC A.32 Similarly, Chirikov et al reported a 28% reduction in mortality with multi-specialist management, particularly among patients receiving chemotherapy.30
Multiple studies further support the efficacy of MDT care, highlighting its positive impact on survival rates and its role in reducing mortality, especially in patients with intermediate to advanced HCC.21,28,30,32 Despite increasing recognition of patient-centered care in oncology, its implementation remains limited in the MENA region. Only 15.1% of centers reported systematically assessing patients’ quality of life, while fewer than half (41.5%) actively involved patients in decision-making. This lack of patient engagement can impact treatment adherence, as individuals who feel excluded from the decision-making process may be less likely to comply with recommended therapies. Additionally, the absence of structured quality-of-life assessments may result in delayed recognition of treatment side effects, potentially affecting both patient satisfaction and clinical outcomes. While conventional follow-up models remain the norm, greater integration of patient-centered approaches, including structured symptom tracking and telemedicine consultations, could enhance adherence and optimize long-term care for HCC patients in the region. Vogel et al emphasized the importance of collaborative decision-making between MDT members and patients to ensure treatment choices align with patients’ goals and preferences.37 Similarly, Cohen et al highlighted that HCC patients’ trust in treatment strategies is influenced by open communication, alignment with patient preferences, and the involvement of supportive MDT members.18 Despite multiple studies advocating for the inclusion of patient preferences in MDT decision-making, this remains an underutilized practice.38–40 Studies evaluating the feasibility of patient participation in multidisciplinary tumor conferences identified several challenges, including communication barriers and time constraints.41,42
Despite growing awareness of its benefits, palliative care remains significantly underutilized in HCC management across the MENA region, with most centers introducing these services only in advanced disease stages (83%). Studies by Temel et al and Henson et al have demonstrated that early integration of palliative care improves symptom control, enhances quality of life, and may even extend survival. However, multiple barriers—including limited access to specialized palliative services (67.9%), a shortage of trained personnel (50.9%), and financial constraints (47.2%)—impede its broader adoption.43,44 Addressing these gaps requires a multifaceted approach. Capacity-building programs for palliative care specialists should be prioritized to ensure MDTs have access to trained personnel. Additionally, integrating palliative care discussions into routine MDT meetings could facilitate earlier intervention, ensuring a more holistic approach to patient management. Health policy initiatives aimed at securing financial support for palliative services, particularly in resource-limited settings, are also essential to bridging this gap. Strengthening palliative care infrastructure and standardizing its inclusion in MDT decision-making could ultimately enhance patient comfort, improve quality of life, and ensure a more patient-centered approach to HCC care. Similarly, adopting advanced digital health technologies remains limited in the MENA region’s HCC treatment centers. Only 3.8% of centers reported occasional use of artificial intelligence (AI) for image analysis, and 43.4% did not implement telemedicine. The underutilization of EHRs and decision-support tools highlights a digital divide in the region. Cohen et al reported that Temple Hospital’s EHR system enhanced communication among MDT members, facilitating coordinated diagnostic assessments and treatment interventions.18 Clinical decision-support systems have been shown to improve MDT efficiency by streamlining data retrieval, optimizing treatment selection, and supporting clinical decision-making.45 Moreover, AI and machine learning applications have demonstrated potential in enhancing imaging interpretation, diagnostic accuracy, genetic analysis, and treatment assessment for HCC patients.46–51
Participants in our study identified several areas for improvement in MDT processes, with enhancing communication among members (54.7%), allocating additional resources (52.8%), incorporating patient feedback into treatment planning (50.9%), and providing additional training on collaboration (45.3%) emerging as the top priorities. Additionally, improving access to patient records and data (43.4%), better-defining roles and responsibilities within the MDT (39.6%), and increasing the frequency of MDT meetings (35.8%) were suggested as ways to optimize the efficiency of multidisciplinary discussions.
Several reports have highlighted ongoing challenges in optimizing MDT performance, particularly in coordinating schedules among specialists from different institutions, leading to less frequent meetings and delayed decision-making.12,15 Given the demanding clinical workload and geographical constraints in the MENA region, leveraging virtual MDT meetings could serve as a viable solution, allowing specialists to participate remotely without disrupting their clinical duties. Additionally, prioritizing complex cases for in-depth MDT discussions while streamlining routine cases through pre-discussion triaging could improve efficiency. Standardized MDT scheduling protocols, dedicated administrative support, and digital case-sharing platforms may also facilitate more structured and effective discussions, ensuring that multidisciplinary input is consistently integrated into patient care. Regarding patient compliance, Charriere et al reported that adherence to MDT recommendations significantly improved patient outcomes (HR, 0.39; 95% CI, 0.27–0.54), with nonadherence mainly due to disease progression (44%), contraindications (32%), and patient refusal (17%).52 Similarly, Gashin et al found that one-third of MDT decisions, particularly those related to locoregional treatments, were not implemented due to patient-related factors (such as socioeconomic barriers, personal preferences, and missed follow-ups) and physician-related challenges (including feasibility and logistic constraints).22
The impact of MDTs on the diagnosis-to-treatment interval (DTI) has been debated. Tseng et al reported that MDT-managed patients experienced a longer DTI compared to non-MDT patients (22 vs 20 days, P<0.05).29 However, other studies have indicated that MDTs contribute to a reduction in time-to-treatment initiation by expediting the decision-making process and ensuring coordinated care.22,28 From an economic standpoint, Kaplan et al found that MDT care was associated with higher treatment costs, with a mean three-year expenditure of $180,313 (P<0.0001).27 These findings underscore the need for cost-effectiveness assessments in MDT implementation, particularly in resource-limited settings.
While this study provides valuable insights into MDT implementation for HCC management in the MENA region, some limitations should be acknowledged. The cross-sectional design does not allow for direct causal inferences between MDT presence and treatment outcomes. Additionally, as with any self-reported data, there is a potential for response bias. However, the inclusion of a diverse range of centers across multiple countries strengthens the validity of the findings. Despite regional variations in healthcare infrastructure and resources, our study provides a comprehensive overview of MDT practices in the MENA region, offering valuable guidance for future improvements and policy development.
Further research should address the economic and logistic barriers to MDT implementation in the MENA region and evaluate how region-specific MDT protocols can be adapted to local healthcare needs. The integration of early palliative care and its impact on quality of life should be explored further, along with studies assessing the role of AI-driven decision-support tools and telemedicine in MDT workflow. Additionally, longitudinal data are required to assess the long-term impact of MDTs on HCC survival rates, treatment efficiency, and overall healthcare system optimization. Implementing these targeted recommendations will significantly enhance MASLD management, bridge systemic gaps, and ultimately improve patient outcomes in the MENA region.
Conclusion
This study underlines the pivotal role of multidisciplinary approaches in optimizing HCC management while highlighting critical gaps in resource allocation, technology adoption, and patient-centered care in the MENA region. Our findings reinforce existing evidence on the benefits of MDTs in improving clinical decision-making, adherence to treatment guidelines, and overall patient outcomes. Additionally, the study brings attention to the need for broader integration of palliative care, active patient involvement in treatment decisions, and more structured screening protocols. Addressing these challenges through enhanced collaboration, policy support, and technological advancements will be key to improving HCC management and patient survival in the region.
Abbreviations
HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; ML, machine learning; MASLD, metabolic dysfunction-associated steatotic liver disease; MENA, Middle East and North Africa region; MDT, multidisciplinary team.
Data Sharing Statement
Data are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved by the Research Ethics Committee for human and animal research at the Faculty of Medicine, Helwan University, number 151-2024. Informed consent was electronically obtained from all study participants prior to initiating the online survey. Participants received clear information about the study objectives, data confidentiality, voluntary nature of participation, and their right to withdraw at any stage without consequence. Consent was indicated by participants explicitly agreeing electronically before accessing and completing the questionnaire.
Acknowledgments
The authors acknowledge the contributions of SLMENA collaborators.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Rumgay H, Ferlay J, de Martel C, et al. Global, regional, and national burden of primary liver cancer by subtype. Eur J Cancer. 2022;161:108–118. doi:10.1016/j.ejca.2021.11.023
3. de Martel C, Georges D, Bray F, Ferlay J, Clifford GM. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2020;8(2):e180–90. doi:10.1016/S2214-109X(19)30488-7
4. Thomas London W, Petrick JL, McGlynn KA. Cancer epidemiology and prevention. 2018;635–660.
5. Kamal S. Hepatocellular carcinoma in the Middle East: an overview. Liver Cancer Middle East. 2021;299–311.
6. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
7. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
8. Yameny AA. Hepatocellular carcinoma (HCC) in Egypt: prevalence, risk factors, diagnosis and prevention: a Review. J Biosci Applied Res. 2024;10(4):879–890. doi:10.21608/jbaar.2024.393371
9. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82(2):315–374. doi:10.1016/j.jhep.2024.08.028
10. Ramadan A, Kaddah M, Shousha H, El-Kassas M. Personalized treatment approaches in hepatocellular carcinoma. Arab J Gastroenterol. 2025:
11. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
12. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
13. Gadsden MM, Kaplan DE. Multidisciplinary approach to HCC management: how can this be done? Dig Dis Sci. 2019;64:968–975. doi:10.1007/s10620-019-05593-8
14. El-Kassas M, Abdelkader H. Multidisciplinary approach in cancer management. In: Interdisciplinary Cancer Research. Cham: Springer; 2024. doi:10.1007/16833_2024_378.
15. Oh JH, Sinn DH. Multidisciplinary approach for hepatocellular carcinoma patients: current evidence and future perspectives. J Liver Cancer. 2024;24(1):47–56. doi:10.17998/jlc.2024.02.27
16. Brown GT, Bekker HL, Young AL. Quality and efficacy of multidisciplinary team (MDT) quality assessment tools and discussion checklists: a systematic review. BMC Cancer. 2022;22(1):286. doi:10.1186/s12885-022-09369-8
17. Winters DA, Soukup T, Sevdalis N, Green JS, Lamb BW. The cancer multidisciplinary team meeting: in need of change? History, challenges, and future perspectives. BJU Int. 2021;128(3):271–279. doi:10.1111/bju.15495
18. Cohen GS, Black M. Multidisciplinary management of hepatocellular carcinoma: a model for therapy. J Multidisciplinary Healthcare. 2013;9:189–195. doi:10.2147/JMDH.S41206
19. Waked I, Alsammany S, Tirmazy SH, et al. Multidisciplinary consensus recommendations for management of hepatocellular carcinoma in Middle East and North Africa region. Liver Int. 2023;43(10):2062–2077. doi:10.1111/liv.15685
20. Zhang J, Mavros MN, Cosgrove D, et al. Impact of a single-day multidisciplinary clinic on the management of patients with liver tumors. Curr Oncol. 2013;
21. Chang TT, Sawhney R, Monto A, et al. Implementation of a multidisciplinary treatment team for hepatocellular cancer at a veterans affairs medical center improves survival. HPB. 2008;10:405–411. doi:10.1080/13651820802356572
22. Gashin L, Tapper E, Babalola A, et al. Determinants and outcomes of adherence to recommendations from a multidisciplinary tumor conference for hepatocellular carcinoma. HPB. 2014;16:1009–1015. doi:10.1111/hpb.12280
23. Duininck G, Lopez-Aguiar AG, Lee RM, et al. Optimizing cancer care for hepatocellular carcinoma at a safety-net hospital: the value of a multidisciplinary disease management team. J Surg Oncol. 2019;120:1365–1370. doi:10.1002/jso.25738
24. Wiggans MG, Jackson SA, Fox BM, et al. The preoperative assessment of hepatic tumors: evaluation of UK regional multidisciplinary team performance. HPB Surg. 2013;2013:861681. doi:10.1155/2013/861681
25. Serper M, Taddei TH, Mehta R, et al. Association of provider specialty and multidisciplinary care with hepatocellular carcinoma treatment and mortality. Gastroenterology. 2017;152:1954–1964. doi:10.1053/j.gastro.2017.02.040
26. Siddique O, Yoo ER, Perumpail RB, et al. The importance of a multidisciplinary approach to hepatocellular carcinoma. J Multidisciplinary Healthcare. 2017;20:95–100. doi:10.2147/JMDH.S128629
27. Kaplan DE, Chapko MK, Mehta R, et al. Healthcare costs related to treatment of hepatocellular carcinoma among veterans with cirrhosis in the United States. Clin Gastroenterol Hepatol. 2018;16:106–114.e5. doi:10.1016/j.cgh.2017.07.024
28. Sinn DH, Choi GS, Park HC, et al. Multidisciplinary approach is associated with improved survival of hepatocellular carcinoma patients. PLoS One. 2019;14:e0210730. doi:10.1371/journal.pone.0210730
29. Tseng YC, Kung PT, Peng CY, Chou WY, Tsai WC. Effect of multidisciplinary team care on patient survival in chronic hepatitis B or C hepatocellular carcinoma. Front Oncol. 2023;13:1251571. doi:10.3389/fonc.2023.1251571
30. Chirikov M, Hanna CD, Breunig N, Seal IM, Shaya B, Shaya FT. Multispecialist care and mortality in hepatocellular carcinoma. Am J Clin Oncol. 2015;38:557–563. doi:10.1097/COC.0000000000000000
31. Yang L, Yan C, Wang J. Effect of multi-disciplinary team care program on quality of life, anxiety, and depression in hepatocellular carcinoma patients after surgery: a randomized, controlled study. Front Surg. 2023;9:1045003. doi:10.3389/fsurg.2022.1045003
32. Yopp AC, Mansour JC, Beg MS, et al. Establishment of a multidisciplinary hepatocellular carcinoma clinic is associated with improved clinical outcome. Ann Surg Oncol. 2014;21:1287–1295. doi:10.1245/s10434-013-3413-8
33. Rashed WM, Kandeil MAM, Mahmoud MO, Ezzat S. Hepatocellular carcinoma (HCC) in Egypt: a comprehensive overview. J Egyptian Nat Cancer Inst. 2020;32(1):5. doi:10.1186/s43046-020-0016-x
34. Ezzat R, Eltabbakh M, El Kassas M. Unique situation of hepatocellular carcinoma in Egypt: a review of epidemiology and control measures. World J Gastrointest Oncol. 2021;13(12):1919–1938. doi:10.4251/wjgo.v13.i12.1919
35. Jean K, Tawheed A, Luong Nguye LB, et al. Changes in presentation, treatment, and survival of patients with hepatocellular carcinoma in Damietta, Egypt, 2007-2019: a retrospective monocentric cohort study. J Hepatocell Carcinoma. 2023;10:99–111. doi:10.2147/JHC.S391511
36. Alolyan A, Alshammari K, Arabi M, et al. Treatment patterns and recommendations for improving the management of hepatocellular carcinoma in Saudi Arabia. J Hepatocell Carcinoma. 2024;31:349–362. doi:10.2147/JHC.S442842
37. Vogel A, Saborowski A. Current strategies for the treatment of intermediate and advanced hepatocellular carcinoma. Cancer Treat Rev. 2020;82:101946. doi:10.1016/j.ctrv.2019.101946
38. Lamb BW, Taylor C, Lamb JN, et al. Facilitators and barriers to teamworking and patient centeredness in multidisciplinary cancer teams: findings of a national study. Ann Surg Oncol. 2013;20:1408–1416. doi:10.1245/s10434-012-2676-9
39. Soukup T, Petrides KV, Lamb BW, et al. The anatomy of clinical decision-making in multidisciplinary cancer meetings: a cross-sectional observational study of teams in a natural context. Medicine. 2016;95(24):e3885. doi:10.1097/MD.0000000000003885
40. Soukup T, Lamb BW, Arora S, Darzi A, Sevdalis N, Green JS. Successful strategies in implementing a multidisciplinary team working in the care of patients with cancer: an overview and synthesis of the available literature. J Multidisciplinary Healthcare. 2018;19:49–61. doi:10.2147/JMDH.S117945
41. Lamb BW, Jalil RT, Shah S, et al. Cancer patients’ perspectives on multidisciplinary team working: an exploratory focus group study. Urol Nurs. 2014;34(2):83–91. doi:10.7257/1053-816X.2014.34.2.83
42. Heuser C, Diekmann A, Schellenberger B, et al. Patient participation in multidisciplinary tumor conferences from the providers’ perspective: is it feasible in routine cancer care? J Multidisciplinary Healthcare. 2020;27:1729–1739. doi:10.2147/JMDH.S283166
43. Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non–small-cell lung cancer. N Engl J Med. 2010;363(8):733–742. doi:10.1056/NEJMoa1000678
44. Henson LA, Maddocks M, Evans C, Davidson M, Hicks S, Higginson IJ. Palliative care and the management of common distressing symptoms in advanced cancer: pain, breathlessness, nausea and vomiting, and fatigue. J Clin Oncol. 2020;38(9):905–914. doi:10.1200/JCO.19.00470
45. Wang L, Chen X, Zhang L, et al. Artificial intelligence in clinical decision support systems for oncology. Int J Med Sci. 2023;20(1):79. doi:10.7150/ijms.77205
46. Pérez MJ, Grande RG. Application of artificial intelligence in the diagnosis and treatment of hepatocellular carcinoma: a review. World J Gastroenterol. 2020;26:5617–5628. doi:10.3748/wjg.v26.i37.5617
47. Yang Q, Wei J, Hao X, et al. Improving B-mode ultrasound diagnostic performance for focal liver lesions using deep learning: a multicentre study. EBioMedicine. 2020;56:102777. doi:10.1016/j.ebiom.2020.102777
48. Estmann PM, Wang CJ, Savic LJ, et al. Deep learning-assisted differentiation of pathologically proven atypical and typical hepatocellular carcinoma (HCC) versus non-HCC on contrast-enhanced MRI of the liver. Eur Radiol. 2021;31:4981–4990.
49. Calderaro J, Seraphin TP, Luedde T, Simon TG. Artificial intelligence for the prevention and clinical management of hepatocellular carcinoma. J Hepatol. 2022;76:1348–1361. doi:10.1016/j.jhep.2022.01.014
50. Schattenberg JM, Chalasani N, Alkhouri N. Artificial intelligence applications in hepatology. Clin Gastroenterol Hepatol. 2023;21:2015–2025. doi:10.1016/j.cgh.2023.04.007
51. Suchman K, Garg S, Trindade AJ. Chat generative pretrained transformer fails the multiple-choice American College of gastroenterology self-assessment test. Am J Gastroenterol. 2023;118:2280–2282. doi:10.14309/ajg.0000000000002320
52. Charriere B, Muscari F, Maulat C, et al. Outcomes of patients with hepatocellular carcinoma are determined in multidisciplinary team meetings. J Surg Oncol. 2017;115:330–336. doi:10.1002/jso.24500
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.