")
Back to Journals » Journal of Inflammation Research » Volume 17
Naples Prognostic Score: A Novel Predictor of Survival in Patients with Triple-Negative Breast Cancer
Authors Qiu Y, Chen Y, Shen H, Yan S, Li J, Wu W
Received 18 April 2024
Accepted for publication 2 August 2024
Published 8 August 2024 Volume 2024:17 Pages 5253—5269
DOI https://doi.org/10.2147/JIR.S472917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yu Qiu,1,2,* Yan Chen,1,2,* Haoyang Shen,1,2 Shuixin Yan,1,2 Jiadi Li,1,2 Weizhu Wu1
1The Affiliated Lihuili Hospital, Ningbo University, Ningbo, 315000, People’s Republic of China; 2Health Science Center, Ningbo University, Ningbo, Zhejiang, 315000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weizhu Wu, The Affiliated Lihuili Hospital, 1111 Jiangnan Road, Ningbo, Zhejiang, 315000, People’s Republic of China, Tel +86 574 13957402451, Email [email protected]
Purpose: This study investigated the correlation between the Naples prognostic score (NPS), clinicopathological traits, and the postoperative prognoses of patients with triple-negative breast cancer (TNBC). Based on NPS, a predictive nomogram was developed to estimate the long-term survival probabilities of patients with TNBC post-surgery.
Patients and Methods: We retrospectively examined the clinical records of 223 women with TNBC treated at Ningbo Medical Center, Lihuili Hospital between January 1, 2016 and December 31, 2020. Blood tests and biochemical analyses were conducted before surgery. The prognostic nutritional index (PNI), controlling nutritional status (CONUT), neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and NPS were determined based on blood-related markers. A Kaplan-Meier survival analysis assessed the association between NPS, PNI, CONUT score, overall survival (OS), and breast cancer-specific survival (BCSS). Predictive accuracy was evaluated using the area under the receiver operating characteristic curve (AUC) and C index. The patients were randomly divided into the training and the validation group (6:4 ratio). A nomogram prediction model was developed and evaluated using the R Software for Statistical Computing (RMS) package.
Results: NPS outperformed other scores in predicting inflammation outcomes. Patients with an elevated NPS had a poorer prognosis (P< 0.001). Lymph node ratio (LNR), surgical method, postoperative chemotherapy, and NPS independently predicted OS, whereas M stage, LNR, and NPS independently predicted BCSS outcome. The OS and BCSS predicted by the nomogram model aligned well with the actual OS and BCSS. The decision curve analysis showed significant clinical utility for the nomogram model.
Conclusion: In this study, NPS was an important prognostic indicator for patients with TNBC. The nomogram prognostic model based on NPS outperformed other prognostic scores for predicting patient prognosis. The model demonstrated a clear stratification ability for patient prognosis, which emphasized the potential benefits of early intervention for high-risk patients.
Plain Language Summary: In this study, we aimed to understand how the Naples prognostic score (NPS) scoring system could predict the prognosis for patients with triple-negative breast cancer (TNBC). TNBC is a type of breast cancer that can be difficult to treat. Medical records of 223 women with TNBC were retrospectively analyzed. These women had their blood tested before surgery to check for certain markers related to nutrition and inflammation. NPS was used along with other scores to determine their accuracy in predicting survival. NPS was better at predicting outcomes than the other scores. The patients with higher NPS scores tended to have poorer outcomes. We also created a visual tool called a nomogram to help doctors predict patient outcomes based on the NPS scores. NPS can be a valuable tool for doctors treating patients with TNBC because it can help them predict how well a patient might do after surgery. This information could be used to tailor treatment plans for these patients. The nomogram provides a user-friendly way for doctors to use NPS in their practice. Overall, this study showed that NPS is a powerful tool for predicting outcomes for patients with TNBC, which could lead to better treatment decisions and improved outcomes for these patients.
Keywords: triple-negative breast cancer, Naples prognostic score, prognostic factor, nomogram predictive model
Introduction
Breast cancer is the leading cause of cancer-related illnesses and death among women globally. Recent data on cancer indicate that breast cancer is one of the most commonly diagnosed malignant tumors worldwide.1,2 Triple-negative breast cancer (TNBC) is a subtype characterized by estrogen receptor (ER) and progesterone receptor (PR) levels < 1% in immunohistochemical tests. Additionally, TNBC lacks overexpression of human epidermal growth factor receptor 2 and amplification of genes found in other breast cancer subtypes, accounting for approximately 10–20% of all breast cancer cases.3,4 TNBC is notable for its early onset, significant diversity, high metastasis risk, and unfavorable prognosis. Patients often experience early recurrence and metastasis, with a median survival period of 12–18 months.5,6 With the onset of distant metastases in TNBC patients, the primary therapeutic objectives focus on enhancing patient quality of life and extending survival. Even with notable progress in diagnosing and treating TNBC, it remains a major global issue for women.7–9 Consequently, we aimed to identify precise and economic predictive biomarkers, develop more accurate predictive models, establish a personalized risk categorization standard, and offer treatment guidance for patients with TNBC.
Recently, several studies have highlighted the impact of nutritional inflammation on the survival and prognosis of patients with malignant tumors. This type of inflammation is closely linked to tumor growth, proliferation, invasion, and metastasis.10,11 Efficient and readily identifiable serum indicators can aid in enhancing the treatment of cancerous tumors.
Persistent inflammation may develop if the underlying causes persist or if regulatory processes prove ineffective. This chronic inflammation can further support the growth and resilience of tumor cells, promote the formation and spread of blood vessels, disrupt the adaptive immune response, and contribute to medication resistance.12,13 Inadequate nutritional levels may indicate metabolic issues stemming from cancer, compromised immunity due to tumor growth, and an inability to tolerate cancer treatment.14,15 Earlier research has indicated a link between subpar nutrition and unfavorable clinical outcomes in breast cancer cases.16 Conversely, breast cancer is often associated with excessive nutritional levels. Being overweight significantly increases the risk of breast cancer in postmenopausal women.17,18
The lymph node ratio (LNR), calculated as the proportion of positive lymph nodes to the total number of resected lymph nodes, has been suggested to enhance the predictive precision of lymph node status in diverse tumors.19,20 Concurrently, research has verified the effectiveness of LNR in predicting breast cancer outcomes. In a number of studies with limited sample sizes, LNR has demonstrated superior predictive capabilities compared to pathological lymph node staging stratification.21–23
Certain evaluation methods incorporate inflammatory or nutritional indicators such as the prognostic nutritional index (PNI),24 controlling nutritional status (CONUT),25 lymphocyte-to-monocyte ratio (LMR), and neutrophil-to-lymphocyte ratio (NLR) to assess outcomes in cancer patients. The Naples prognostic score (NPS), created by Italian academic Galizia, relies on levels of NLR, (LMR), albumin, and total cholesterol.26 This comprehensive approach allows for a simultaneous assessment of systemic inflammatory, nutritional, and immune conditions, potentially surpassing the efficacy of individual inflammatory or nutritional indicators. NPS has proven to be an independent prognostic indicator and has been used extensively in recent years to evaluate the prognosis of a number of malignancies, including pancreatic,27 colorectal,28 oesophageal,29 gastric,30 and endometrial cancers.31 Previous research has been conducted on how inflammatory nutritional markers impact early-stage and post-neoadjuvant breast cancer.32,33 However, there are limited studies on the application of inflammatory nutritional markers in patients with TNBC. Thus, further investigation is necessary to thoroughly assess the relationship between NPS and the survival of patients with TNBC. To date, there is no consensus on which rating index is more advantageous.34,35
Therefore, in this study in patients with TNBC, we conducted a retrospective examination of clinical and follow-up data, assessed the predictive power of three inflammatory nutrition markers, and ascertained NPS’s clinical significance for prognosis prediction. Statistical techniques were employed to evaluate the diagnostic and prognostic values of NPS. Furthermore, early interventions were implemented for high-risk patients to enhance their prognosis. A nomogram was utilized to quantify prognostic indicators, enabling a more accurate and practical prediction of patient outcomes.
Materials and Methods
Patient Eligibility
From January 1, 2016 to December 31, 2020, clinical data were collected from 223 female patients with TNBC who underwent surgery and postoperative adjuvant therapy at The Affiliated Lihuili Hospital, Ningbo University, Ningbo, China. All patients were monitored until either they died or the study reached the last follow-up date (December 31, 2023), whichever came first. The inclusion criteria were the following: (1) female sex; (2) TNBC confirmed by postoperative pathology; (3) complete basic clinical data; and (4) detection of routine blood and biochemical indices before surgery. The exclusion criteria were the following: (1) presence of additional malignancies; (2) diagnosis of bilateral breast cancer; (3) presence of diseases affecting the immune, blood, or other related systems that could affect hematological indicators; (4) receipt of radiotherapy or chemotherapy prior to surgery; and (5) insufficient follow-up information.
This study was approved by the Ethics Committee of The Affiliated Lihuili Hospital, Ningbo University, Ningbo, China (approval number: KY2024SL138-01). Written informed consent was not required for this retrospective study. The study was conducted in accordance with the Declaration of Helsinki. The patient’s medical information has been kept confidential.
Data Collection and Follow-Up
The general clinical data of the patients, including age at diagnosis, menopausal status, body mass index, and surgical methods, were collected. Peripheral blood tests were performed 7 days before surgery, encompassing neutrophil count, lymphocyte count, total cholesterol level, serum albumin level, NLR, and LMR. Postoperative pathological data included tumor pathological type, pathological grade, TNM stage, Ki-67 index, and LNR.
After surgery, patients underwent routine follow-ups via phone calls and medical data from the inpatient system, outpatient services, and other channels were collected. Follow-ups were performed at the time of death or at the end of the study (December 31, 2023) with intervals ranging from 1–96 months. Among the 223 patients, 33 had died by the last follow-up. Follow-up procedures included postoperative adjuvant therapy (chemotherapy and radiation). Overall survival (OS) was determined using the time interval between the end of surgery and death or the last follow-up. Breast cancer-specific survival (BCSS) was computed using the time interval between the end of surgery and the patient’s death from breast cancer or the last follow-up.
Definitions and Grouping in NPS, PNI, and CONUT Studies
NPS equals the sum of the plasma albumin level, total cholesterol level, NLR, and LMR scores. Patients were categorized into two groups based on the selection of the optimal threshold of 2 using the Do Kaplan-Meier function in X-tile software: NPS≤2 (indicating no/mild malnutrition risk) and NPS>2 (signifying severe malnutrition risk). As provided by Galizia et al,26 the definitions and grading criteria for NPS are listed in Table 1.
 |
Table 1 The Grading Standard of NPS |
PNI equals the sum of serum albumin level (g/L) and lymphocyte count (*10^9/L) multiplied by five. The Do Kaplan-Meier feature of X-tile software indicated that the optimal threshold was 50.9, categorizing patients into two groups: PNI≥50.9 (indicating no risk of malnutrition) and PNI<50.9 (indicating a risk of malnutrition).
The CONUT score is the sum of the serum albumin level, total lymphocyte count, and total cholesterol level; the scoring guidelines are detailed in Table 2. By selecting the optimal threshold based on the Do Kaplan-Meier function in X-tile software, patients were categorized into two groups: CONUT<1 (indicating no risk of malnutrition) and CONUT≥2 (indicating a risk of malnutrition).
 |
Table 2 The Grading Standard of COUNT |
Statistical Analyses and Nomogram
The X-tile software was utilized to determine the optimal threshold values for NPS, PNI, and CONUT. Survival curves were generated using the Kaplan-Meier method and analyzed using the Log rank test. The predictive capacities of NPS, PNI, and CONUT scores were compared using the time-dependent area under the receiver operating characteristic (ROC) curve (AUC).
A total of 223 patients were randomly allocated to the training (n = 113) and validation (n = 90) groups, maintaining a 6:4 ratio. Initially, the univariate Cox regression was performed on the training dataset to identify the optimal variable combination; variables with P < 0.05 were selected for multivariate Cox regression. The stepwise backward regression technique was then applied. A nomogram prediction model was constructed using the final model variables (independent risk factors for OS and BCSS) to predict the 3- and 5-year OS and BCSS of patients with TNBC. The nomogram visually linked various predictive risk elements to the likelihood of OS and BCSS in patients with TNBC after surgery. The degree of distinctiveness of the nomogram was measured using the area under the AUC value or the concordance index (C-index), where the C-index was approximately equal to the ROC curve area. The calibration curve provided a visual assessment of the calibration for the nomogram. The 45° line denotes a perfect calibration, which occurs when the patient’s real risk and the model’s anticipated value match exactly. The decision curve analysis confirmed the clinical benefit of the nomogram. The strong clinical relevance of the model was demonstrated by the curve above the None and All lines, both of which showed a net benefit. R (version 4.2.0; Vienna, Austria) software was used (http://www.r-project.org/). Statistical significance was defined as P < 0.05.
Results
Clinicopathological Characteristics
Each of the 223 patients underwent a follow-up period of 62 months (range 4–96 months). By the end of the follow-up period, 39 patients had experienced both metastasis and recurrence. The recurrence rate over more than 3 years was 6.73% (15 of 223), whereas that for more than 5 years was 13.45% (30 of 223). Table 3 presents the demographic and clinical data alongside the initial laboratory parameters.
 |
Table 3 Comparison of Baseline Clinicopathological Features Between Training Group and Validation Group |
Relationship Between Preoperative PNI, CONUT, and NPS Groups and Clinicopathological Characteristics of Patients with TNBC
The OS and BCSS endpoints were used to construct ROC curves and the AUC was computed. Both PNI and NPS showed superior performance (Figure 1A and B). Additionally, a Kaplan-Meier curve analysis was performed. Figures 2A–C reveals that PNI (low vs high: P=0.0062) and NPS (low vs high: P=0.041) were related to OS, whereas the CONUT score (low vs high: P=0.76) was not. In Figures 2D–F, Kaplan-Meier curves demonstrated that, in contrast to CONUT (low vs high: P=0.96), NPS (low vs high: P=0.003) and PNI (low vs high: P=0.011) were associated with BCSS. Patients with a low PNI and a high NPS exhibited a poor prognosis. Taken together, these results suggest that NPS outperform PNI and CONUT in terms of predictive performance.
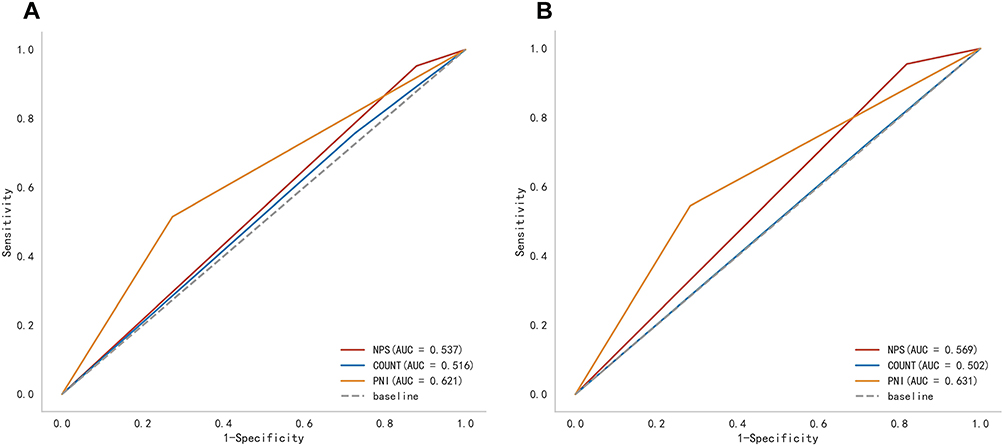 |
Figure 1 ROC curves to determine the cut-off values for NPS, CONUT, PNI. (A) For OS. (B) For BCSS. Abbreviations: BCSS, breast cancer-specific survival; CONUT, controlling nutritional status; NPS, Naples prognostic score; OS, overall survival; PNI, prognostic nutritional index. |
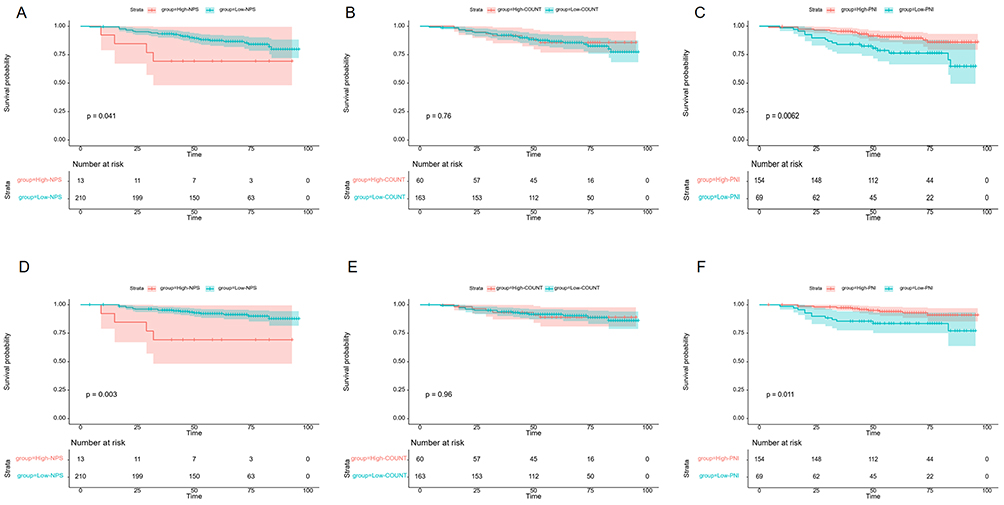 |
Figure 2 Kaplan-Meier survival curves of NPS, CONUT, and PNI groups versus patients with TNBC. (A–C) For OS. (D–F) For BCSS. Abbreviations: BCSS, breast cancer-specific survival; CONUT, controlling nutritional status; NPS, Naples prognostic score; PNI, prognostic nutritional index; TNBC, triple-negative breast cancer. |
Univariate and Multivariate COX Analysis of Prognostic Factors
Each patient was randomly assigned to a training set (n = 133) and a validation set (n = 90) in a 6:4 ratio. There were no significant differences in any of the variables between the two groups (P > 0.05), indicating that the two groups were similar and homogeneous (Table 3).
The prognostic markers for OS identified in the univariate analysis included surgical technique, postoperative chemotherapy, LNR, TNM stage, PNI score, and NPS score (Table 4). In the multivariate analysis, LNR, surgical technique, postoperative chemotherapy, and NPS were identified as independent predictors of OS (P < 0.05). Similarly, the prognostic markers for BCSS included surgical technique, postoperative chemotherapy, LNR stage, NM stage, PNI score, and NPS score in the univariate analysis. LNR, M stage, and NPS score were identified as independent predictive variables for BCSS in the multivariate analysis (P < 0.05) (Table 5). The prediction model indicated that patients in the high-NPS group had a worse OS than those in the low-NPS group.
 |
Table 4 Univariate and Multivariate Cox Regression Analysis of Overall Survival (OS) in 223 TNBC Patients |
 |
Table 5 Univariate and Multivariate Cox Regression Analysis of Overall Survival (BCSS) in 223 TNBC Patients |
Building and Validating a Nomogram Prognostic Model
A nomogram was developed to predict OS and BCSS for patients with TNBC. This nomogram incorporated factors with a statistical significance of P < 0.05, as determined by the multivariate analysis of the training set. To estimate the potential OS and BCSS in patients with TNBC at 3- and 5-years post-surgery, we calculated a nomogram score by adding the detailed scores of each variable. Figure 3A and B depict the nomogram, illustrating that individuals with TNBC have a worse prognosis and that a shorter survival time is associated with a higher NPS score. These findings demonstrate that survival time is inversely correlated with the bisection of the nomogram prediction model.
 |
Figure 3 Nomogram for predicting 3- and 5-year OS (A) and BCSS (B) of patients with TNBC using independent prognostic factors. Abbreviations: BCSS, breast cancer-specific survival; OS, overall survival; TNBC, triple-negative breast cancer. |
The prediction model was validated using bootstrapping. For OS prediction, the C-index was 0.701 (95% confidence interval [CI]: 0.556–0.845) in the training group and 0.771 (95% CI: 0.642–0.901) in the validation group. BCSS prediction yielded a C-index of 0.717 (95% CI: 0.570–0.864) in the training group and 0.692 (95% CI: 0.462–0.921) in the validation group. The prediction nomogram exhibited improved individualized prediction accuracy in both the validation (Figure 4B and D) and the training set (Figure 4A and C) in the time-dependent ROC curve evaluation.
 |
Figure 4 Time-dependent receiver operating characteristic (ROC) curves for assessing the discrimination of the condition survival nomogram in the training cohort (A and C) and the internal validation cohort (B and D). |
A calibration curve was created, and the multivariate Cox regression model was developed using 1000 re-samplings of the original data to predict the 3- and 5-year OS and BCSS of patients with TNBC following surgery, which was verified using R software. The 3- and 5-year OS and BCSS predicted by the nomogram model and the actual OS and BCSS in the training and validation sets showed an acceptable degree of agreement, with the calibration curve essentially floating around 45° (Figures 5A–D).
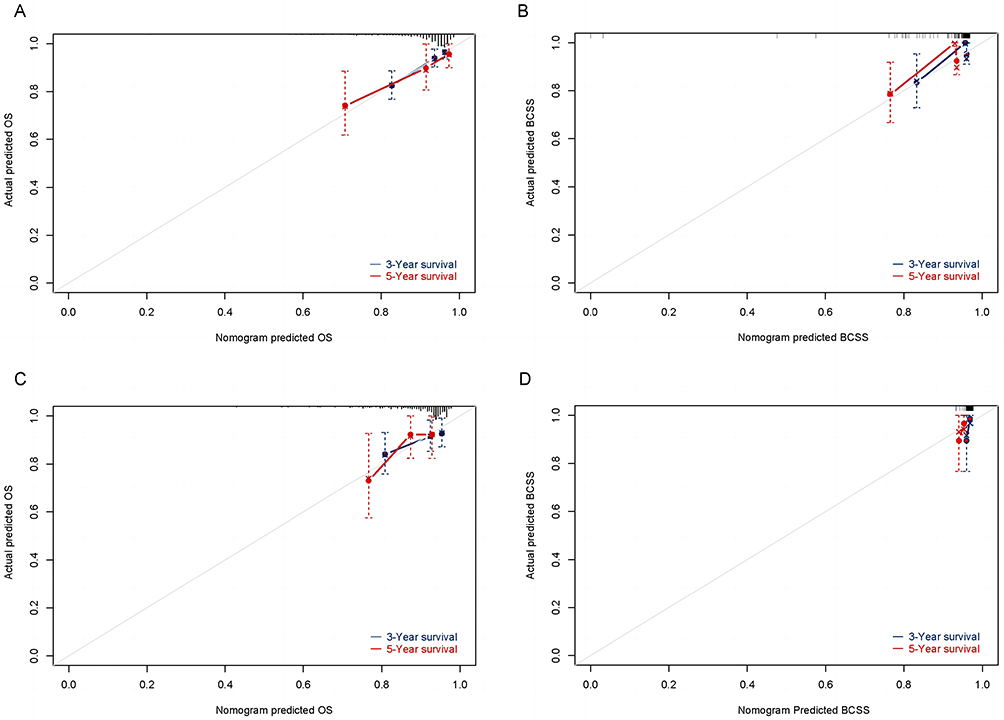 |
Figure 5 Calibration curves for predicting OS and BCSS at 3 and 5 years in the training cohort (A and B) and in the internal validation cohort (C and D). Abbreviations: BCSS, breast cancer-specific survival; OS, overall survival. |
Decision curve analysis was used to determine the extent of benefit. The results are shown in Figures 6A–D at 3 and 5 years, demonstrating its clinical applicability and net benefit over a broad range of thresholds.
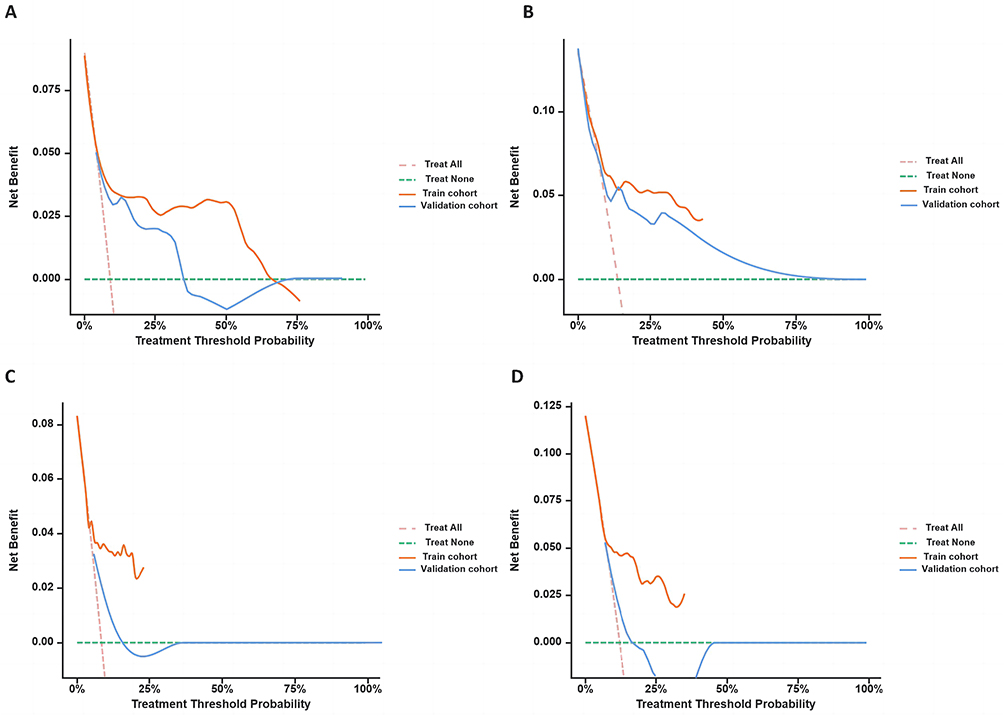 |
Figure 6 Decision curve analysis (DCA) curves for assessing clinical usefulness of the condition survival nomogram for 3- and 5-year OS (A and B) and 3- and 5-year BCSS (C and D) in the training and internal validation cohorts. Abbreviations: BCSS, breast cancer-specific survival; OS, overall survival. |
Discussion
The prognostic significance of preoperative nutritional status and inflammatory immunology in tumor prognosis has garnered increasing attention in recent years.36,37 Every stage of tumorigenesis, from initiation to tumor development and metastasis, is impacted by inflammation. Recent research has demonstrated that close collaboration between cancer cells, immunological and inflammatory cells, and stromal components is necessary for metastasis.38–40 Furthermore, inadequate nutritional status is one of the main factors influencing the prognosis of breast cancer.41,42 Several preoperative prognostic metrics derived from serum biomarkers have been shown to be related to breast cancer prognosis.43,44 Better clinical management of malignant tumors can be achieved through the fast and straightforward identification of blood indicators.
Researchers have developed the NPS score to provide an assessment of nutritional inflammation that integrates the impacts of nutrition, inflammation, immunology, and cancer. It includes factors such as NLR, lymphocytes, and albumin level among other biomarkers and has a strong prognostic predictive capacity.26 NPS independently predicts outcomes in patients with TNBC, providing a reliable means to assess survival odds and exhibiting good predictive accuracy, as demonstrated in a study involving 223 patients with TNBC. In the present study, the NPS score is a more comprehensive inflammatory and nutritional score that can more accurately assess survival in patients with TNBC. A higher NPS is associated with a worse patient prognosis. From a clinical standpoint, treatment strategies should be customized according to the patient’s NPS towards personalized treatments to extend survival in patients with TNBC.
The characteristics of lymph nodes in breast cancer are broadly acknowledged as key indicators for predicting patient outcomes. Traditionally, the number of positive lymph nodes has been the most important predictive factor in breast cancer, serving as the foundation for pN categorization in the AJCC staging framework. Nonetheless, the quantity of lymph nodes analyzed can be influenced by various factors, including surgical expertise and the management of surgical samples by pathologists. Inadequate removal and assessment of lymph nodes can result in an underestimation of the tumor’s stage, potentially causing unsuitable treatment and inaccurate predictive decisions. In response, LNR was implemented to evaluate the prognosis of breast cancer. Based on the results of this study, we propose that LNR could surpass pN stage in terms of predicting accuracy in limited-sample studies from a single institution. Nonetheless, additional studies are warranted to verify this hypothesis.
This study is the first to develop nomograms based on NPS scores, LNR, and other independent prognostic factors to predict overall survival and breast cancer-specific survival in patients with TNBC. In both the training and the validation set, the nomogram showed exceptionally high prognostic accuracy and predictive power. Decision curve analysis further confirmed that the column chart had a good clinical net benefit. In addition, our prognostic model is more applicable and useful in clinical practice due to its reduced number of factors and the fact that the parameters are common laboratory indicators.
Inflammatory and immune cells release various cytokines and chemical signals, such as pro-inflammatory cytokines and interleukins, due to the interplay between the inflammatory condition of the tumor and its surrounding environment. These factors not only initiate a widespread inflammatory immune reaction but also promote the development of blood vessels, metastasis, and tumors locally.45–47 Conversely, adequate nutrients can improve immune system performance, maintain immune equilibrium, reduce the inflammatory response of the tumor, and inhibit tumor growth and spread.48 Additionally, successful treatment should address the postoperative state of the patient as well as the preoperative state. Early nutritional supplementation has been shown to enhance physical function, boost anti-tumor drug tolerance, and improve postoperative prognostic survival in cancer patients with pre-cachexia.49,50 Therefore, using NPS to evaluate the nutritional and immunological status of patients with TNBC can support tailored care and serve as a foundation for the management of cancer patients in the perioperative phase. Future research is needed to shed light on the molecular pathways and interactions between inflammation and nutritional status and how these are affected by genetic factors to develop innovative approaches to cancer treatment and prevention. We developed a nomogram prediction model for OS and BCSS in patients with TNBC based on prognostic factors including NPS. All biomarkers are objective laboratory indicators, can be tested with widely available tests, and are assessed at no additional cost.
Our study had several limitations. First, we only examined the relationship between NPS and the long-term outcomes of patients due to the validity of clinical records and compliance with patient instructions. We did not investigate the relationship between NPS and postoperative complications or disease-free survival duration. Second, some patients were unable to tolerate postoperative chemotherapy due to inadequate immune and nutritional health, resulting in treatment discontinuation or cessation. Third, limited sample size and inconsistent chemotherapy protocols made it difficult to conduct more detailed stratified evaluations of postoperative chemotherapy. Fourth, this study analyzed data from a single center, making it difficult to eliminate confounding biases, even with the strict screening of patients according to the predetermined inclusion criteria. Further validation of the results of this study in larger prospective studies is warranted.
Conclusion
NPS is an easy-to-use scoring system capable of predicting prognosis and treatment efficacy in patients with TNBC. High NPS may indicate a shorter OS and BCSS. Furthermore, based on NPS, we developed and validated a novel nomogram prediction model as a visual and intuitive tool for clinical prognostic assessment and decision-making assistance.
Abbreviations
AUC, area under the curve; BCSS, breast cancer-specific survival; CONUT, controlling nutritional status; ER, estrogen receptor; LNR, lymph node ratio; NLR, neutrophil-to-lymphocyte ratio; NPS, Naples prognostic score; OS, overall survival; PLR, platelet-to-lymphocyte ratio; PNI, prognostic nutritional index; PR, progesterone receptor; ROC, receiver operating characteristic; TNBC, triple-negative breast cancer.
Data Sharing Statement
The data analyzed in this study are available from the corresponding author (Yu Qiu, E-mail: [email protected]) upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the ethics committee of The Affiliated Lihuili Hospital, Ningbo University (approval number: KY2024SL138-01) with a waived requirement for patient informed consent because medical data were retrospectively reviewed. Patient data remained confidential and this study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors thank all patients and institutions involved in the study, especially for the surveillance.
Author Contributions
YQ and WW contributed by providing the idea for the study. YC, HS, SY, and JL contributed to data collection and collation. YQ and YC analyzed data and wrote contributions. All authors made a significant contribution to the work reported and took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work. YQ and YC share first authorship.
Funding
This research was funded by the Ningbo Clinical Medical Research Center for Thoracic Malignancies (grant number, 2021L002) and The Fourth Round of Ningbo Medical Key Disciplines Construction Plan (grant number, 2022-F03).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA. 2023;73(1):17–48. doi:10.3322/caac.21763
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Borri F, Granaglia A. Pathology of triple negative breast cancer. Semin Cancer Biol. 2021;72:136–145. doi:10.1016/j.semcancer.2020.06.005
4. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363(20):1938–1948. doi:10.1056/NEJMra1001389
5. Karim AM, Eun Kwon J, Ali T, et al. Triple-negative breast cancer: epidemiology, molecular mechanisms, and modern vaccine-based treatment strategies. Biochem Pharmacol. 2023;212:115545. doi:10.1016/j.bcp.2023.115545
6. Leon-Ferre RA, Goetz MP. Advances in systemic therapies for triple negative breast cancer. BMJ. 2023;381:e071674. doi:10.1136/bmj-2022-071674
7. Tang Y, Tian W, Zheng S, et al. Dissection of FOXO1-Induced LYPLAL1-DT impeding triple-negative breast cancer progression via mediating hnRNPK/β-Catenin complex. Research. 2023;6:0289. doi:10.34133/research.0289
8. Wu S, Lu J, Zhu H, et al. A novel axis of circKIF4A-miR-637-STAT3 promotes brain metastasis in triple-negative breast cancer. Cancer Lett. 2024;581:216508. doi:10.1016/j.canlet.2023.216508
9. Ou X, Tan Y, Xie J, et al. Methylation of GPRC5A promotes liver metastasis and docetaxel resistance through activating mTOR signaling pathway in triple negative breast cancer. Drug Resist Updat. 2024;73:101063. doi:10.1016/j.drup.2024.101063
10. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
11. Martínez-Garay C, Djouder N. Dietary interventions and precision nutrition in cancer therapy. Trends Mol Med. 2023;29(7):489–511. doi:10.1016/j.molmed.2023.04.004
12. Aggarwal BB, Vijayalekshmi RV, Sung B. Targeting inflammatory pathways for prevention and therapy of cancer: short-term friend, long-term foe. Clin Cancer Res. 2009;15(2):425–430. doi:10.1158/1078-0432.CCR-08-0149
13. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
14. Thanikachalam K, Khan G. Colorectal Cancer and Nutrition. Nutrients. 2019;11(1):164. doi:10.3390/nu11010164
15. Kheirouri S, Alizadeh M. Prognostic potential of the preoperative controlling nutritional status (CONUT) score in predicting survival of patients with cancer: a systematic review. Adv Nutr. 2021;12(1):234–250. doi:10.1093/advances/nmaa102
16. De Cicco P, Catani MV, Gasperi V, Sibilano M, Quaglietta M, Savini I. Nutrition and breast cancer: a literature review on prevention, treatment and recurrence. Nutrients. 2019;11(7):1514. doi:10.3390/nu11071514
17. Brown KA. Metabolic pathways in obesity-related breast cancer. Nat Rev Endocrinol. 2021;17(6):350–363. doi:10.1038/s41574-021-00487-0
18. Picon-Ruiz M, Morata-Tarifa C, Valle-Goffin JJ, Friedman ER, Slingerland JM. Obesity and adverse breast cancer risk and outcome: mechanistic insights and strategies for intervention. CA. 2017;67(5):378–397. doi:10.3322/caac.21405
19. Zheng Y, Lu Z, Shi X, et al. Lymph node ratio is a superior predictor in surgically treated early-onset pancreatic cancer. Front Oncol. 2022;12:975846. doi:10.3389/fonc.2022.975846
20. Perez M, Hansen CP, Burdio F, et al. Lymph node ratio nomogram-based prognostic model for resected distal cholangiocarcinoma. J Am Coll Surg. 2022;235(5):703–712. doi:10.1097/XCS.0000000000000299
21. Teng J, Abdygametova A, Du J, et al. Bayesian inference of lymph node ratio estimation and survival prognosis for breast cancer patients. IEEE J Biomed Health Inform. 2020;24(2):354–364. doi:10.1109/JBHI.2019.2943401
22. Singh D, Mandal A. The prognostic value of lymph node ratio in survival of non-metastatic breast carcinoma patients. Breast Cancer Res Treat. 2020;184(3):839–848. doi:10.1007/s10549-020-05885-y
23. Liu D, Chen Y, Deng M, et al. Lymph node ratio and breast cancer prognosis: a meta-analysis. Breast Cancer. 2014;21(1):1–9. doi:10.1007/s12282-013-0497-8
24. Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nippon Geka Gakkai zasshi. 1984;85(9):1001–1005.
25. Ignacio de Ulíbarri J, González-Madroño A, de Villar NGP, et al. CONUT: a tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp. 2005;20(1):38–45.
26. Galizia G, Lieto E, Auricchio A, et al. Naples prognostic score, based on nutritional and inflammatory status, is an independent predictor of long-term outcome in patients undergoing surgery for colorectal cancer. Dis Colon Rectum. 2017;60(12):1273–1284. doi:10.1097/DCR.0000000000000961
27. Nakagawa N, Yamada S, Sonohara F, et al. Clinical implications of Naples prognostic score in patients with resected pancreatic cancer. Ann Surg Oncol. 2020;27(3):887–895. doi:10.1245/s10434-019-08047-7
28. Park SH, Woo HS, Hong IK, Park EJ. Impact of Postoperative Naples Prognostic Score to Predict Survival in Patients with Stage II-III Colorectal Cancer. Cancers. 2023;15(20):5098. doi:10.3390/cancers15205098
29. Feng JF, Zhao JM, Chen S, Chen QX. Naples prognostic score: a novel prognostic score in predicting cancer-specific survival in patients with resected esophageal squamous cell carcinoma. Front Oncol. 2021;11:652537. doi:10.3389/fonc.2021.652537
30. Wang H, Fang T, Yin X, et al. Prognostic importance of the preoperative New-Naples prognostic score for patients with gastric cancer. Cancer Med. 2023;12(2):1358–1375. doi:10.1002/cam4.5017
31. Li Q, Cong R, Wang Y, et al. Naples prognostic score is an independent prognostic factor in patients with operable endometrial cancer: results from a retrospective cohort study. Gynecol Oncol. 2021;160(1):91–98. doi:10.1016/j.ygyno.2020.10.013
32. A novel inflammatory-nutritional prognostic scoring system for patients with early-stage breast cancer - pubmed. Available from: https://PubMed.ncbi.nlm.nih.gov/35079223/.
33. Wang MD, Duan FF, Hua X, Cao L, Xia W, Chen JY. A novel albumin-related nutrition biomarker predicts breast cancer prognosis in neoadjuvant chemotherapy: a two-center cohort study. Nutrients. 2023;15(19):4292. doi:10.3390/nu15194292
34. Prognostic nutritional index (PNI) and controlling nutritional status (CONUT) score for predicting outcomes of breast cancer: a systematic review and meta-analysis - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/37680798/.
35. The role of nutrition-based index in predicting survival of breast cancer patients: a systematic review and meta-analysis - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/38169970/.
36. Salas S, Cottet V, Dossus L, et al. Nutritional factors during and after cancer: impacts on survival and quality of life. Nutrients. 2022;14(14):2958. doi:10.3390/nu14142958
37. Ozga AJ, Chow MT, Luster AD. Chemokines and the immune response to cancer. Immunity. 2021;54(5):859–874. doi:10.1016/j.immuni.2021.01.012
38. Kennel KB, Bozlar M, De Valk AF, Greten FR. Cancer-associated fibroblasts in inflammation and antitumor immunity. Clin Cancer Res. 2023;29(6):1009–1016. doi:10.1158/1078-0432.CCR-22-1031
39. Hou J, Karin M, Sun B. Targeting cancer-promoting inflammation - have anti-inflammatory therapies come of age? Nat Rev Clin Oncol. 2021;18(5):261–279. doi:10.1038/s41571-020-00459-9
40. Wang M, Chen S, He X, Yuan Y, Wei X. Targeting inflammation as cancer therapy. J Hematol Oncol. 2024;17(1):13. doi:10.1186/s13045-024-01528-7
41. Shi J, Liu T, Ge Y, et al. Cholesterol-modified prognostic nutritional index (CPNI) as an effective tool for assessing the nutrition status and predicting survival in patients with breast cancer. BMC Med. 2023;21(1):512. doi:10.1186/s12916-023-03225-7
42. Li Y, Zhang Y, Zhou Z, et al. Predictive value of controlling nutritional status score in postoperative recurrence and metastasis of breast cancer patients with HER2-low expression. Front Oncol. 2023;13:1116631. doi:10.3389/fonc.2023.1116631
43. Qu F, Luo Y, Peng Y, et al. Construction and validation of a prognostic nutritional index-based nomogram for predicting pathological complete response in breast cancer: a two-center study of 1170 patients. Front Immunol. 2023;14:1335546. doi:10.3389/fimmu.2023.1335546
44. Li W, Li M, Wang T, et al. Controlling Nutritional Status (CONUT) score is a prognostic factor in patients with resected breast cancer. Sci Rep. 2020;10(1):6633. doi:10.1038/s41598-020-63610-7
45. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
46. Propper DJ, Balkwill FR. Harnessing cytokines and chemokines for cancer therapy. Nat Rev Clin Oncol. 2022;19(4):237–253. doi:10.1038/s41571-021-00588-9
47. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–899. doi:10.1016/j.cell.2010.01.025
48. Altea-Manzano P, Cuadros AM, Broadfield LA, Fendt SM. Nutrient metabolism and cancer in the in vivo context: a metabolic game of give and take. EMBO Rep. 2020;21(10):e50635. doi:10.15252/embr.202050635
49. Baracos VE, Martin L, Korc M, Guttridge DC, Fearon KCH. Cancer-associated cachexia. Nat Rev Dis Primers. 2018;4(1):17105. doi:10.1038/nrdp.2017.105
50. Setiawan T, Sari IN, Wijaya YT, et al. Cancer cachexia: molecular mechanisms and treatment strategies. J Hematol Oncol. 2023;16(1):54. doi:10.1186/s13045-023-01454-0
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.