")
Back to Journals » Journal of Inflammation Research » Volume 17
Neutrophil-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio and Platelet-to-Lymphocyte Ratio as Predictors of Short- and Long-Term Outcomes in Ischemic Stroke Patients with Atrial Fibrillation
Authors Guo J, Wang D , Jia J, Zhang J, Liu Y, Lu J, Zhao X , Yan J
Received 29 May 2024
Accepted for publication 17 September 2024
Published 23 September 2024 Volume 2024:17 Pages 6661—6672
DOI https://doi.org/10.2147/JIR.S480513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Ning Quan
Jiahuan Guo,1 Dandan Wang,1 Jiaokun Jia,1 Jia Zhang,1 Yanfang Liu,1 Jingjing Lu,1,2 Xingquan Zhao,1– 4,* Jing Yan1,*
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Research Unit of Artificial Intelligence in Cerebrovascular Disease, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 4Center of Stroke, Beijing Institute for Brain Disorders, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xingquan Zhao; Jing Yan, Email [email protected]; [email protected]
Purpose: Inflammatory response plays essential roles in the pathophysiology of both ischemic stroke and atrial fibrillation (AF). We aimed to investigate whether composite inflammatory markers, including neutrophil to lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR) and platelet-to-lymphocyte ratio (PLR), can serve as early predictors of short- and long-term outcomes in ischemic stroke patients with AF.
Patients and Methods: Ischemic stroke patients with AF were enrolled in this cohort study. The primary outcome was 1-year functional dependence or death (modified Rankin scale (mRS) score 3– 6). Secondary outcomes included hemorrhagic transformation (HT) and early neurological deterioration (END, increase in the National Institutes of Health Stroke Scale (NIHSS) ≥ 4 within 7 days). Partial correlations were performed to assess the correlation between systemic inflammation markers and admission NIHSS scores. Univariate and multivariate logistic analyses were performed to investigate whether systemic inflammatory markers were independent predictors of adverse outcomes.
Results: A total of 408 patients were included. Partial correlation analysis revealed statistically significant but weak correlations between the NLR (r = 0.287; P < 0.001), PLR (r = 0.158; P = 0.001) and admission NIHSS score. Compared with patients without HT or END, patients who developed HT or END had higher NLR and PLR, and lower LMR. Patients in the functional dependence or death group had significantly higher NLR and PLR, and lower LMR than those in the functional independence group (all P < 0.001). Multivariate logistic analysis indicated that NLR, LMR and PLR were independent predictors of HT (OR = 1.069, 0.814 and 1.003, respectively), END (OR = 1.100, 0.768 and 1.006, respectively) and adverse 1-year functional outcome (OR = 1.139, 0.760 and 1.005, respectively).
Conclusion: NLR, LMR and PLR were independent predictors for in-hospital HT, END and long-term functional outcome in ischemic stroke patients with AF. Close monitoring of these inflammatory markers may help guide risk stratification and clinical treatment strategies.
Keywords: inflammation, ischemic stroke, atrial fibrillation, hemorrhagic transformation, early neurological deterioration, functional outcome
Introduction
Atrial fibrillation (AF) is the most common arrhythmia and is a significant contributor to ischemic stroke and mortality.1 Ischemic stroke patients with AF are often more severely ill and have a greater risk of a poor prognosis than those without AF.2 Moreover, treatment decision-making is usually more difficult in ischemic stroke patients with AF. The optimal antithrombotic strategy and timing to restart remain intractable problems since the relative benefit and hemorrhagic transformation (HT) should be considered. Identifying reliable biomarkers that can predict HT and functional outcomes is essential for risk stratification and determining possible means of controlling the risk factors at an early stage in ischemic stroke patients with AF.
Inflammatory response has been found to play essential roles in the pathogenesis and progression of both ischemic stroke and AF.3–7 Several studies have reported that inflammatory reactions are related to the triggering and maintenance of AF.8 Moreover, it has been suggested that inflammatory state in AF may promote the formation of left atrial thrombus and the detachment of an already formed thrombus and further contribute to an increased risk of thromboembolism and poor prognosis.9,10 Meanwhile, in patients with ischemic stroke, evidence has shown that neuronal cell death and disruption of the blood‒brain barrier caused by inflammation may result in hemorrhagic transformation and poor functional outcomes.11 This is particularly important for ischemic stroke patients with AF since the decision to prescribe therapeutic anticoagulation is challenging in clinical practice. Taken together, the role of inflammation in outcomes of ischemic stroke patients with AF may require extra attention, and may serve as an important predictor of HT and functional outcomes. However, there is limited evidence to support this.
Neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) represent novel systemic inflammation biomarkers that combine various inflammatory parameters. These composite inflammatory markers can be easily assessed at disease onset via routine blood tests, and may provide more information about immunological activity than traditional individual inflammatory markers.12 A previous study showed that NLR was an independent predictor of 90-day prognosis in acute ischemic stroke patients, and had a better predictive value than traditional individual inflammatory markers including C-reactive protein and white cell count.13 Another study demonstrated that NLR, PLR and LMR were associated with post-thrombolysis early neurological deterioration (END) in patients with acute ischemic stroke.14 Higher NLR levels has also been found to have predictive value for adverse functional outcomes in ischemic stroke patients after endovascular therapy or thrombolysis.15,16 However, whether NLR, LMR and PLR can be predictors of HT and functional outcomes in ischemic stroke patients with AF remains unclear.
In this study, we primarily aimed to investigate the associations of composite inflammatory markers, including NLR, LMR and PLR, with long-term functional outcome at 1 year in ischemic stroke patients with AF. Additionally, we explored the relationships between these inflammatory markers and stroke severity, in-hospital HT and END.
Material and Methods
Study Population
This retrospective cohort study was performed using prospectively collected data. Ischemic stroke patients with AF from all over the country admitted to Beijing Tiantan Hospital from February 2021 to January 2023 were screened. This study was approved by the ethics committee of Beijing Tiantan Hospital, Capital Medical University (No. KY2023-163-01). Written informed consent was obtained from all patients or their legal guardians. This study was conducted according to the Declaration of Helsinki and institutional guidelines.
The inclusion criteria included (1) age greater than or equal to 18 years, (2) a diagnosis of ischemic stroke according to the WHO criteria17 within 72 h of symptom onset, and (3) a documented history or in-hospital diagnosis of AF. The exclusion criteria were as follows: (1) had iatrogenic stroke, venous infarction or stroke due to head trauma; (2) had a prestroke modified Rankin scale (mRS) score ≥2; (3) had major comorbidities or late-stage disease with a life expectancy of <3 months; (4) had complications such as infectious diseases, inflammatory diseases, immune system disorders, or were receiving immunotherapy; (5) had comorbidities that may have increased inflammation indicators including tumors, myocardial infarction, trauma, recent surgery and anaphylaxis; (6) lacked neutrophil, lymphocyte, monocyte or platelet count data; and (7) lacked follow-up data.
Data Collection
Clinical data, including demographic variables, medical history, preonset medication and in-hospital treatment, were collected by a trained neurological physician. The severity of neurological impairment was assessed by the National Institute of Health Stroke Scale (NIHSS) score on the first three days and seventh day of admission. CT/MRI scans were performed on admission whenever neurologic worsening was detected and before discharge at the discretion of the treating physicians.
Neutrophil counts, lymphocyte counts, monocyte counts and platelet counts were assessed in the emergency room on admission with an autoanalyzer via standard procedures (BC-5390 CRP, Mindray, China). These counts were used to determine the systemic inflammatory markers listed below NLR was calculated as neutrophil count/lymphocyte count. PLR was calculated as platelet count/lymphocyte count. LMR was calculated as lymphocyte count/monocyte count.
Outcome Measurements
The primary outcome was 1-year functional dependence or death, which was defined as an mRS score of 2–6. Secondary outcomes included END (increase in NIHSS score ≥4 within 7 days) and HT (any hemorrhage found on the follow-up CT during hospitalization but not detected on initial head CT). The outcomes were collected through clinical interviews or telephone follow-up by trained investigators who were blinded to the baseline information.
Statistical Analysis
All statistical analyses were performed using SPSS software (version 25.0 for Windows, IBM). The χ2 test or Fisher’s exact test was used for comparisons of categorical variables, and Student’s t test and the Mann–Whitney U-test were used for comparisons of continuous variables. To assess the association between the composite inflammatory markers and the NIHSS score, partial correlation analyses were performed adjusted for age, sex, prior stroke or TIA, diabetes mellitus, hypertension, coronary heart disease, current smoking and AF type. Univariate and multivariate logistic regression model analyses were performed to assess the associations of the composite inflammatory markers with patient outcomes. Potential confounding factors for adjustments were selected based on their statistical significance in the univariate analysis and clinical importance. Model 1 was adjusted for age and sex. Model 2 was adjusted for Model 1 plus NIHSS score on admission, stroke etiology, prior hypertension, diabetes mellitus, stroke or TIA, coronary heart disease, current smoking status, use of antiplatelet agents, anticoagulant agents, and AF type. The composite inflammatory markers were analyzed as continuous variables and dichotomous variables, respectively. All the statistical analyses were two-tailed, and statistical significance was indicated if the P value was <0.05.
Results
Demographic and Clinical Characteristics
A total of 422 ischemic stroke patients with AF met the inclusion criteria. We excluded two patients with infectious disease and 12 patients without follow-up data. Ultimately, a total of 408 patients with a mean age of 70.5 years (257 males, 63.0%) were included in the analysis (Figure 1). During hospitalization, 79 (19.4%) patients developed END, and 158 (38.7%) patients developed HT. At the 1-year follow-up, the primary outcome (functional dependence or death) occurred in 215 (52.7%) patients. The baseline characteristics of the study participants are shown in Table 1. Compared to patients with favorable functional outcome, patients with functional dependence or death were older (67.0 vs 74.0, P < 0.001), a lower proportion were male (68.9% vs 57.7%, P = 0.019); had higher NIHSS score on admission (5.0 vs 13.0, P < 0.001); were more likely to have nonparoxysmal AF (39.4 vs 66.0, P < 0.001); had higher levels of white blood cell counts (7.9 vs 8.5, P = 0.018), neutrophil counts (5.8 vs 6.6, P < 0.001), C-reactive protein (2.1 vs 3.1, P < 0.001), NLR (3.9 vs 6.1, P < 0.001) and PLR (140.7 vs 184.4, P < 0.001); and had lower levels of lymphocyte counts (1.5 vs 1.0, P < 0.001), platelet counts (206.0 vs 184.0, P = 0.002) and LMR (3.4 vs 3.0, P < 0.001).
 |
Table 1 Baseline Characteristics of the Study Population According to Functional Outcome |
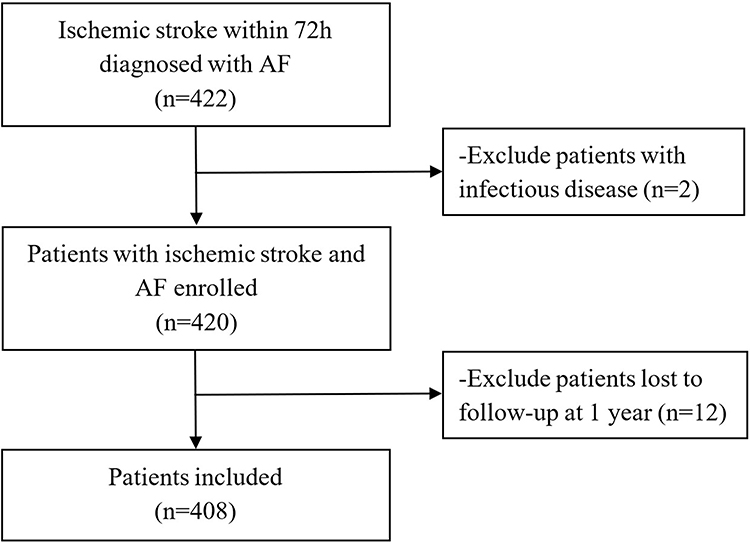 |
Figure 1 Study flow chart. |
Partial Correlation Analysis Between Systemic Inflammatory Markers and Admission NIHSS Score in Ischemic Stroke Patients with AF
As shown in Figure 2, partial correlation analysis revealed a weak but significant correlation between systemic inflammatory markers and stroke severity on admission. After adjusting for age, sex, prior stroke or TIA, diabetes, hypertension, coronary disease, smoking status and AF type, higher NLR (r = 0.287; P < 0.001) and PLR (r = 0.158; P = 0.001) were associated with higher NIHSS score on admission. LMR was not significantly associated with NIHSS score after adjusting for potential covariates (r = −0.085; P = 0.089).
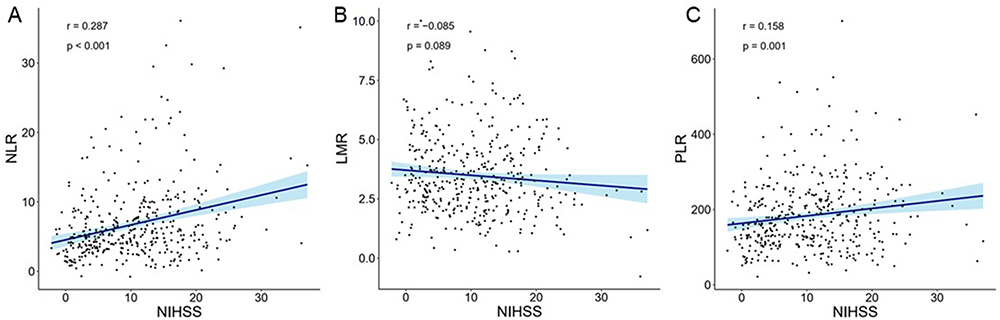 |
Figure 2 Relationships between composite systemic inflammatory markers and NIHSS score on admission after adjusting for potential covariates in ischemic stroke patients with atrial fibrillation. The blue line and shadow depict linear regressions with 95% confidence intervals, respectively. (A) NLR; (B) LMR; (C) PLR. |
Between-Group Differences in Levels of Systemic Inflammatory Markers
Figure 3 shows the violin plots of systemic inflammatory markers between patients with different outcomes. Patients in the functional dependence or death group had significantly higher levels of NLR (6.1 vs 3.9, P < 0.001), PLR (184.4 vs 140.7, P < 0.001) and lower levels of LMR (3.0 vs 3.4, P < 0.001) than patients in the functional independence group. Compared with those without HT, patients who developed the secondary outcome of HT had significantly higher levels of NLR (4.1 vs 6.6, P < 0.001), PLR (151.3 vs 187.8, P < 0.001) and lower levels of LMR (3.4 vs 2.8, P < 0.001). Patients with the secondary outcome of END had significantly higher levels of NLR (7.3 vs 4.6, P < 0.001), PLR (212.1 vs 151.7, P < 0.001) and lower levels of LMR (2.7 vs 3.3, P < 0.001) than those without END.
 |
Figure 3 Violin and box plots of composite systemic inflammatory markers among different prognosis groups. (A) NLR among functional Independence vs functional dependence or death at 1-year follow-up; (B) LMR among functional independence vs functional dependence or death at 1-year follow-up; (C) PLR among functional independence vs functional dependence or death at 1-year follow-up; (D) NLR among non-HT vs HT; (E) LMR among non-HT vs HT; (F) PLR among non-HT vs HT; (G) NLR among non-END vs END; (H) LMR among non-END vs END; (I) PLR among non-END vs END. ***p values indicate p< 0.001. |
Univariate and Multivariate Logistic Analyses of Systemic Inflammatory Markers and Adverse Clinical Outcomes
As shown in Table 2, according to the crude model of univariate logistic regression analysis, NLR (OR = 1.157, 95% CI: 1.097–1.221, P < 0.001), PLR (OR = 1.005, 95% CI: 1.002–1.007, P < 0.001) and LMR (OR = 0.763, 95% CI: 0.675–0.862, P < 0.001) were significant predictors of functional dependence or death at the 1-year follow-up. The associations between NLR (OR = 1.139, 95% CI: 1.067–1.216, P < 0.001), PLR (OR = 1.005, 95% CI: 1.002–1.008, P = 0.001) and LMR (OR = 0.760, 95% CI: 0.652–0.885, P < 0.001) and 1-year functional outcome remained significant even after adjustment for potential covariates.
 |
Table 2 Univariate and Multivariable-Adjusted Odds Ratios and 95% Confidence Intervals for Adverse Outcomes According to NLR, LMR and PLR as Continuous Variables |
The crude model of univariate logistic regression analysis showed that NLR (OR = 1.102, 95% CI: 1.058–1.149, P < 0.001), PLR (OR = 1.004, 95% CI: 1.002–1.006, P < 0.001) and LMR (OR = 0.791, 95% CI: 0.697–0.899, P < 0.001) were significant predictors of HT. After adjusting for all potential covariates, the NLR (OR = 1.069, 95% CI: 1.020–1.120, P = 0.006), PLR (OR = 1.003, 95% CI: 1.000–1.005, P = 0.023) and LMR (OR = 0.814, 95% CI: 0.703–0.944, P = 0.006) remained independent predictors of HT.
According to the crude model of univariate logistic regression analysis, NLR (OR = 1.100, 95% CI: 1.057–1.145, P < 0.001), PLR (OR = 1.006, 95% CI: 1.004–1.008, P < 0.001) and LMR (OR = 0.747, 95% CI: 0.629–0.886, P = 0.001) were significant predictors of END. Multivariate logistic analysis revealed that NLR (OR = 1.100, 95% CI: 1.051–1.151, P < 0.001), PLR (OR = 1.006, 95% CI: 1.003–1.008, P < 0.001) and LMR (OR = 0.768, 95% CI: 0.638–0.923, P = 0.005) were independent predictors of END.
When systemic inflammatory markers were analyzed as dichotomous variables, the associations between NLR, LMR and PLR remained unchanged (Table 3).
 |
Table 3 Univariate and Multivariable-Adjusted Odds Ratios and 95% Confidence Intervals for Adverse Outcomes According to the Median of NLR, LMR and PLR |
Receiver Operating Characteristic Curves of Systemic Inflammatory Markers
ROC curves were used to assess the efficiency of novel composite inflammatory markers and a traditional individual inflammatory marker (C-reactive protein) in predicting outcomes in ischemic stroke patients with AF (Supplementary Table 1 and Figures 1–3). The area under curve (AUC) of NLR, PLR and LMR in the prediction of 1-year functional outcome were 0.679 (95% CI: 0.625–0.733, P < 0.001), 0.625 (95% CI: 0.569–0.682, P < 0.001) and 0.625 (95% CI: 0.569–0.681, P < 0.001), respectively. Which were all greater than the AUC of C-reactive protein (0.603, 95% CI: 0.546–0.660, P = 0.001). The area under curve (AUC) of NLR, PLR and LMR for the prediction of HT were 0.673 (95% CI: 0.618–0.728, P < 0.001), 0.618 (95% CI: 0.561–0.675, P < 0.001) and 0.611 (95% CI: 0.552–0.670, P < 0.001), respectively. Which were all greater than the AUC of C-reactive protein (0.571, 95% CI: 0.512–0.631, P = 0.002). The area under curve (AUC) of NLR, PLR and LMR in the prediction of END were 0.687 (95% CI: 0.619–0.754, P < 0.001), 0.680 (95% CI: 0.613–0.746, P < 0.001) and 0.637 (95% CI: 0.566–0.707, P < 0.001), respectively. Which were all greater than the AUC of C-reactive protein (0.530, 95% CI: 0.456–0.605, P = 0.415).
Discussion
In this cohort study, we systematically assessed the associations between composite systemic inflammatory markers and short- and long-term outcomes in ischemic stroke with AF. Several major findings emerged. First, systemic inflammatory markers, including NLR and PLR, showed positive but weak correlations with stroke severity on admission in ischemic stroke patients with AF, whereas the correlation between LMR and stroke severity was not significant. Second, NLR, LMR and PLR were associated with long-term adverse outcomes (functional dependence or death at 1-year follow-up) in ischemic stroke patients with AF, independent of stroke severity and other potential covariates. Third, NLR, LMR and PLR may serve as biomarkers indicative of in-hospital short-term outcomes, including HT and END. Assessment of these systemic inflammatory markers is important for risk stratification and therapeutic strategy development in ischemic stroke patients with AF.
In recent years, accumulating evidence has revealed that inflammation is involved in the pathophysiology of cardiovascular and cerebrovascular diseases and has significant prognostic value.18–21 NLR, LMR and PLR are composite inflammatory markers of different combinations of inflammatory parameters and thus may provide more information about immunological activities. It has been reported that composite inflammatory markers are more stable and superior to traditional individual markers in the prediction of stroke prognosis.12 Additionally, these composite inflammatory markers can be easily calculated from blood cell counts, which are the most commonly used clinical tests and can be obtained via routine blood examination. Previous investigation of the relationship between composite inflammatory markers and outcomes of ischemic stroke demonstrated that inflammatory markers serve as independent prognostic indicators of functional outcome and mortality.13,22,23 A previous study reported that NLR, LMR and PLR were associated with END after thrombolysis in patients with ischemic stroke.14 Additionally, inflammation may also play an important role in the pathophysiology and prognostic outcomes of AF. Markers of systemic inflammation have been linked to atrial remodeling,24 incident AF25 and increased risk of stroke and all-cause mortality in patients with AF.26–28 Our study revealed similar results with the previous studies. And further provide evidence on the short- and long-term prognostic value of composite systemic inflammatory markers in ischemic stroke patients with AF, demonstrating that NLR, LMR and PLR were independent predictors of END and adverse functional outcome at 1-year follow-up.
The mechanisms underlying the relationship between systemic inflammation and adverse functional outcomes of ischemic stroke patients with AF may involve multiple pathways. First, damaged brain cells after ischemia triggers inflammatory response, leading to the release of inflammatory mediators.29 Conversely, peripheral leukocytes can induce the destruction of the blood‒brain barrier, cause secondary neuronal damage and aggravate neurological dysfunction.30,31 Second, inflammation and thrombosis are closely linked processes.32 In patients with AF, NLR and PLR have been found to be independent risk factors for the presence of left atrial thrombosis,22,33 which may contribute to an acute exacerbation of neurological impairment and a greater risk of stroke recurrence and further lead to adverse functional outcomes after ischemic stroke.
Hemorrhagic transformation can occur as a part of ischemic stroke progression and may be another reason for the increased risk of adverse functional outcomes.34 The optimal strategy and timing of resuming anticoagulation therapy after ischemic stroke with AF has always been an intractable clinical problem since resuming anticoagulation may contribute to HT in the acute phase of ischemic stroke.35 Therefore, early and rapid identification of patients at high risk of HT is essential in ischemic stroke patients, especially for those with AF. A previous study demonstrated that NLR is an independent biomarker for major bleeding events.36 Another study aimed at developing a model for predicting HT after ischemic stroke revealed that NLR was related to the risk of HT and enhanced the risk prediction for HT compared to the conventional risk model in real-world practice.37 Our study adds to the emerging body of evidence on the utility of the composite systemic inflammatory markers, including NLR, LMR and PLR, as independent predictors of HT after ischemic stroke in patients with AF. Disruption of the blood‒brain barrier by inflammatory mediators may be one of the reasons for the association between inflammatory markers and HT after stroke.11 In addition, it has been reported that peripheral monocytes and neutrophils can act as sources of matrix metalloproteinase-9, which can lead to HT.38,39 Regardless, the results of the current study indicate that markers of systemic inflammation may be reliable biomarkers for identifying patients at high risk of HT in the acute phase of ischemic stroke among patients with AF, which may facilitate risk stratification and clinical decision-making.
The main innovations of the present study are as follows: This study revealed several novel composite systemic inflammation biomarkers (NLR, PLR and LMR), which can easily be obtained from routine clinical practice, and may be used as predictive biomarkers for predicting HT, END, and long-term adverse functional outcomes in ischemic stroke patients with AF. These findings indicate that early measurement of inflammatory markers may improve the identification of ischemic stroke patients with AF at greatest risk of END or HT and adverse long-term functional outcomes. Incorporation of these markers into clinical decision-making may allow us to choose patients who will benefit the most from intensive monitoring, early anticoagulant therapy and avoid exposing other patients with substantial HT risk. Whether treatments targeting inflammatory pathways can prevent HT, END and improve functional outcomes deserves further investigation. Our study has some potential limitations. First, we analyzed data of inflammatory markers only on admission. The systemic inflammatory indices might be dynamic and change over time. Although the current study revealed the important role of early inflammatory markers in ischemic stroke patients with AF, future studies are needed to assess the dynamic changes in these markers after stroke and determine their prognostic value in ischemic stroke patients with AF. Second, due to the observational nature of this study, the causal relationship between higher levels of inflammatory markers and adverse outcomes cannot be determined. Future studies should determine whether the associations between these composite inflammatory markers and adverse outcomes in ischemic stroke patients with AF are only epiphenomenon or whether they reflect causal relationships. Third, HT after ischemic stroke was assessed only during hospitalization, and HT may occur in some patients after discharge. Therefore, HT events may have been underestimated. Finally, information on stroke recurrence and its etiology was not available in the current study, and the association between systemic inflammatory markers and stroke recurrence awaits further study.
Conclusion
In summary, our study revealed that composite inflammatory markers (including NLR, PLR and LMR) can serve as simple and universally available independent prognostic biomarkers for HT, END and adverse functional outcomes at 1-year follow-up in ischemic stroke patients with AF. Close monitoring of these inflammatory markers may be necessary for risk stratification and clinical decision-making. Whether treatments for inhibiting inflammatory response can improve short- and long-term outcomes in ischemic stroke patients with AF deserves further investigation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (Jing Yan) on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the ethics committee of Beijing Tiantan Hospital, Capital Medical University (No. KY2023-163-01). Written informed consent was obtained from all patients or their legal guardians. This study was conducted according to the Declaration of Helsinki and institutional guidelines.
Acknowledgments
We thank all the patients for participating in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors have read and approved the final submitted manuscript.
Funding
This study was supported by the National Science and Technology Major Project (2022ZD0118005), the Beijing Municipal Committee of Science and Technology (Z201100005620010), the Beijing Hospitals Authority Innovation Studio of Young Staff Funding Support (202112), the Beijing Tiantan Hospital Miaopu Project (2023MP05) and the Ministry of Finance of the People’s Republic of China [issued by Finance and Social Security [2015] Document No. 82; [2016] Document No. 50; [2017] Document No. 72; [2018] Document No. 48; [2019] Document No. 77; [2020] Document No. 75; [2021] Document No. 84, Ministry of Finance].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al-Khatib SM. Atrial Fibrillation. Ann Intern Med. 2023;176(7):ITC97–ITC112. doi:10.7326/AITC202307180
2. Vinding NE, Kristensen SL, Rorth R, et al. Ischemic Stroke Severity and Mortality in Patients With and Without Atrial Fibrillation. J Am Heart Assoc. 2022;11(4):e022638.
3. Scott L Jr, Li N, Dobrev D. Role of inflammatory signaling in atrial fibrillation. Int J Cardiol. 2019;287:195–200.
4. Cui J, Li H, Chen Z, et al. Thrombo-Inflammation and Immunological Response in Ischemic Stroke: focusing on Platelet-Tregs Interaction. Front Cell Neurosci. 2022;16:955385.
5. Iadecola C, Buckwalter MS, Anrather J. Immune responses to stroke: mechanisms, modulation, and therapeutic potential. J Clin Invest. 2020;130(6):2777–2788.
6. Qiu YM, Zhang CL, Chen AQ, et al. Immune Cells in the BBB Disruption After Acute Ischemic Stroke: targets for Immune Therapy? Front Immunol. 2021;12:678744.
7. Endres M, Moro MA, Nolte CH, et al. Immune Pathways in Etiology, Acute Phase, and Chronic Sequelae of Ischemic Stroke. Circ Res. 2022;130(8):1167–1186.
8. Engelmann MD, Svendsen JH. Inflammation in the genesis and perpetuation of atrial fibrillation. Eur Heart J. 2005;26(20):2083–2092.
9. Saliba W, Barnett-Griness O, Elias M, et al. Neutrophil to lymphocyte ratio and risk of a first episode of stroke in patients with atrial fibrillation: a cohort study. J Thromb Haemost. 2015;13(11):1971–1979.
10. Marin F, Corral J, Roldan V, et al. Factor XIII Val34Leu polymorphism modulates the prothrombotic and inflammatory state associated with atrial fibrillation. J Mol Cell Cardiol. 2004;37(3):699–704.
11. Wang R, Zhu Y, Liu Z, et al. Neutrophil extracellular traps promote tPA-induced brain hemorrhage via cGAS in mice with stroke. Blood. 2021;138(1):91–103.
12. Curbelo J, Luquero Bueno S, Galvan-Roman JM, et al. Inflammation biomarkers in blood as mortality predictors in community-acquired pneumonia admitted patients: importance of comparison with neutrophil count percentage or neutrophil-lymphocyte ratio. PLoS One. 2017;12(3):e0173947.
13. Chen L, Zhang L, Li Y, et al. Association of the Neutrophil-to-Lymphocyte Ratio with 90-Day Functional Outcomes in Patients with Acute Ischemic Stroke. Brain Sci. 2024;14(3).
14. Gong P, Liu Y, Gong Y, et al. The association of neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and lymphocyte to monocyte ratio with post-thrombolysis early neurological outcomes in patients with acute ischemic stroke. J Neuroinflammation. 2021;18(1):51.
15. Ruan Z, Wang D, He X, et al. Prognostic Value of Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio in Acute Ischemic Stroke Patients After Thrombolysis. Altern Ther Health Med. 2024.
16. Cong Y, Xia X, Liao J, et al. Association of Systemic Inflammatory Response Index and Neutrophil-to-lymphocyte Ratio on Unfavorable Functional Outcomes in Acute Ischemic Stroke Patients after Endovascular Therapy. World Neurosurg. 2024.
17. Stroke--1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke. 1989;20(10):1407–1431.
18. Libby P, Hansson GK. Inflammation and immunity in diseases of the arterial tree: players and layers. Circ Res. 2015;116(2):307–311.
19. Vinayak M, Cao D, Tanner R, et al. Impact of Bleeding Risk and Inflammation on Cardiovascular Outcomes After Percutaneous Coronary Intervention. JACC: Cardiovasc Interv. 2024;17(3):345–355.
20. Evans LE, Taylor JL, Smith CJ, et al. Cardiovascular comorbidities, inflammation, and cerebral small vessel disease. Cardiovasc Res. 2021;117(13):2575–2588.
21. Benz AP, Aeschbacher S, Krisai P, et al. Biomarkers of Inflammation and Risk of Hospitalization for Heart Failure in Patients With Atrial Fibrillation. J Am Heart Assoc. 2021;10(8):e019168.
22. Chen C, Gu L, Chen L, et al. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio as Potential Predictors of Prognosis in Acute Ischemic Stroke. Front Neurol. 2020;11:525621.
23. Lux D, Alakbarzade V, Bridge L, et al. The association of neutrophil-lymphocyte ratio and lymphocyte-monocyte ratio with 3-month clinical outcome after mechanical thrombectomy following stroke. J Neuroinflammation. 2020;17(1):60.
24. Lazzerini PE, Laghi-Pasini F, Acampa M, et al. Systemic Inflammation Rapidly Induces Reversible Atrial Electrical Remodeling: the Role of Interleukin-6-Mediated Changes in Connexin Expression. J Am Heart Assoc. 2019;8(16):e011006.
25. Conen D, Ridker PM, Everett BM, et al. A multimarker approach to assess the influence of inflammation on the incidence of atrial fibrillation in women. Eur Heart J. 2010;31(14):1730–1736.
26. Lu M, Zhang Y, Liu R, et al. Predictive value of neutrophil to lymphocyte ratio for ischemic stroke in patients with atrial fibrillation: a meta-analysis. Front Neurol. 2022;13:1029010.
27. Wu S, Yang YM, Zhu J, et al. Impact of Baseline Neutrophil-to-Lymphocyte Ratio on Long-Term Prognosis in Patients With Atrial Fibrillation. Angiology. 2021;72(9):819–828.
28. Fan Q, Gao L, Wang Z, et al. Prognostic Value of Platelet-to-Lymphocyte Ratio Combined with CHA(2)DS(2)-VAS(c) Score for Nonvalvular Atrial Fibrillation Induced Cardiogenic Cerebral Embolism. J Inflamm Res. 2023;16:5937–5947.
29. Macrez R, Ali C, Toutirais O, et al. Stroke and the immune system: from pathophysiology to new therapeutic strategies. Lancet Neurol. 2011;10(5):471–480.
30. Yang K, Zeng L, Ge A, et al. A systematic review of the research progress of non-coding RNA in neuroinflammation and immune regulation in cerebral infarction/ischemia-reperfusion injury. Front Immunol. 2022;13:930171.
31. Westendorp WF, Dames C, Nederkoorn PJ, et al. Immunodepression, Infections, and Functional Outcome in Ischemic Stroke. Stroke. 2022;53(5):1438–1448.
32. Abu-Fanne R, Stepanova V, Litvinov RI, et al. Neutrophil alpha-defensins promote thrombosis in vivo by altering fibrin formation, structure, and stability. Blood. 2019;133(5):481–493.
33. Yalcin M, Aparci M, Uz O, et al. Neutrophil-lymphocyte ratio may predict left atrial thrombus in patients with nonvalvular atrial fibrillation. Clin Appl Thromb Hemost. 2015;21(2):166–171.
34. van Kranendonk KR, Treurniet KM, Boers AMM, et al. Clinical and Imaging Markers Associated With Hemorrhagic Transformation in Patients With Acute Ischemic Stroke. Stroke. 2019;50(8):2037–2043.
35. Chang PY, Wang WT, Wu WL, et al. Oral Anticoagulation Timing in Patients with Acute Ischemic Stroke and Atrial Fibrillation. Thromb Haemost. 2022;122(6):939–950.
36. Fagundes A Jr, Ruff CT, Morrow DA, et al. Neutrophil-lymphocyte ratio and clinical outcomes in 19,697 patients with atrial fibrillation: analyses from ENGAGE AF- TIMI 48 trial. Int J Cardiol. 2023;386:118–124.
37. Liu J, Wang Y, Jin Y, et al. Prediction of Hemorrhagic Transformation After Ischemic Stroke: development and Validation Study of a Novel Multi-biomarker Model. Front Aging Neurosci. 2021;13:667934.
38. Duan Z, Wang H, Wang Z, et al. Neutrophil-Lymphocyte Ratio Predicts Functional and Safety Outcomes after Endovascular Treatment for Acute Ischemic Stroke. Cerebrovasc Dis. 2018;45(5–6):221.
39. Yamamoto Y, Osanai T, Nishizaki F, et al. Matrix metalloprotein-9 activation under cell-to-cell interaction between endothelial cells and monocytes: possible role of hypoxia and tumor necrosis factor-alpha. Heart Vessels. 2012;27(6):624–633.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Malnutrition and the Risk of Early Neurological Deterioration in Elderly Patients with Acute Ischemic Stroke
Bao Y, Zhang Y, Du C, Ji Y, Dai Y, Jiang W
Neuropsychiatric Disease and Treatment 2022, 18:1779-1787
Published Date: 20 August 2022
Predictors of Early Neurological Deterioration and Functional Outcome in Acute Ischemic Stroke: The Importance of Large Artery Disease, Hyperglycemia and Inflammatory Blood Biomarkers
Sabir Rashid A, Huang-Link Y, Johnsson M, Wetterhäll S, Gauffin H
Neuropsychiatric Disease and Treatment 2022, 18:1993-2002
Published Date: 6 September 2022
Dynamic Changes and Clinical Significance of Plasma Galectin-3 in Patients with Acute Ischemic Stroke Undergoing Endovascular Therapy
Yao M, Liang D, Zeng X, Xie X, Gao J, Huang L
Journal of Inflammation Research 2024, 17:1377-1387
Published Date: 1 March 2024
Exosomes as Vehicles for Noncoding RNA in Modulating Inflammation: A Promising Regulatory Approach for Ischemic Stroke and Myocardial Infarction
Lai Z, Ye T, Zhang M, Mu Y
Journal of Inflammation Research 2024, 17:7485-7501
Published Date: 21 October 2024
Predictive Value of Epicardial Adipose Tissue for Hemorrhagic Transformation and Functional Outcomes in Acute Ischemic Stroke Patients Undergoing Intravenous Thrombolysis Therapy
Liu L, Jia C, Xing C, Fu X, Liu Z, Ma A
Journal of Inflammation Research 2024, 17:11915-11929
Published Date: 31 December 2024