")
Back to Journals » Journal of Inflammation Research » Volume 18
Nomogram for Predicting Postoperative Cardiopulmonary Complications in Non-Small Cell Lung Cancer Based on Systemic Inflammatory Markers: A Retrospective Study
Authors He Z, Liu K, Wu L, Wei Q
Received 3 February 2025
Accepted for publication 2 July 2025
Published 10 July 2025 Volume 2025:18 Pages 8961—8976
DOI https://doi.org/10.2147/JIR.S519449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Felix Marsh-Wakefield
Zemin He,1 Keting Liu,2 Ling Wu,3 Qiang Wei1
1Department of Thoracic Surgery, The First People’s Hospital of Shuangliu District (West China Airport Hospital of Sichuan University), Chendu, Sichuan Province, 610200, People’s Republic of China; 2Department of Neurology, Chengdu Seventh People’s Hospital, Chendu, Sichuan Province, 610213, People’s Republic of China; 3Department of Respiratory Medicine, The First People’s Hospital of Shuangliu District (West China Airport Hospital of Sichuan University), Chendu, Sichuan Province, 610200, People’s Republic of China
Correspondence: Qiang Wei, Department of Thoracic Surgery, The First People’s Hospital of Shuangliu District (West China Airport Hospital of Sichuan University), Chendu, Sichuan Province, 610200, People’s Republic of China, Email [email protected]
Objective: The objective of this study is to investigate the association between systemic inflammatory markers and postoperative cardiopulmonary complications in patients with non-small cell lung cancer (NSCLC). Additionally, the study aims to develop a column chart tool to improve the accuracy of predicting the risk of postoperative cardiopulmonary complications in NSCLC patients.
Methods: This study analyzed data on patients with lung cancer who underwent surgery in our department from July 2022 to December 2024.Patients were divided into training and validation sets.Logistic regression analysis was used to construct a column chart and identify predictive factors for cardiopulmonary complications.The chart’s performance was evaluated using the C-index, the AUC, the calibration curve, and the decision curve analysis.The validation set was used for further model evaluation.
Results: Multivariate logistic regression analysis demonstrated that smoking history, postoperative neutrophil count, postoperative systemic immunoinflammatory index (SII), ΔSII (change in SII), ΔPLR (change in platelet-lymphocyte ratio), and ΔAISI (change in neutrophil * platelet * monocyte/lymphocyte ratio) were predictive factors for postoperative cardiopulmonary complications. In the training set, the C-index of the model is 0.86 (95% confidence interval: 0.82– 0.91), while in the validation set it is 0.81 (95% confidence interval: 0.73– 0.89). The calibration curve demonstrates a strong correlation between the column chart model and the observed data. The decision curve analysis indicates that the net profit of this model is considerably superior to that of other models.
Conclusion: The present study successfully developed and validated a predictive model based on systemic inflammatory markers to assess the risk of postoperative cardiopulmonary complications in patients with small cell lung cancer. This model assists clinicians in accurately assessing patients’ risk of postoperative cardiovascular and pulmonary complications, thereby promoting personalized patient management.
Keywords: systemic inflammatory markers, non small cell lung cancer, postoperative cardiopulmonary complications, prediction model
Introduction
Lung cancer is the most prevalent and deadly type of cancer worldwide, with a high incidence of mortality.1 According to the most recent cancer statistics published by the National Cancer Center in China, lung cancer is responsible for 20.03% of all malignant neoplasms and accounts for 26.99% of cancer-related deaths.2 Surgery remains the preferred and primary treatment for lung cancer.3 However, following lung cancer surgery, patients with advanced age, impaired respiratory function, pain, difficulty coughing and expectorating, local postoperative inflammatory reactions, direct stimulation of the heart and lungs after surgery, and changes in thoracic dynamics can lead to alterations in respiratory patterns and a temporary decline in cardiopulmonary function.4,5 The aforementioned factors have the potential to increase the risk of cardiovascular and pulmonary complications. Patients may experience various complications, with cardiovascular and pulmonary complications being particularly prevalent.
It has been reported that the incidence of pulmonary complications after thoracic surgery ranges from 19% to 59%, with pulmonary infection being one of the most common complications.6 Lai et al study found that among 421 stage I NSCLC patients, 15.2% experienced cardiopulmonary complications, with the most common being pulmonary infection (8.8%), atelectasis (5.9%), and pleural effusion (5.0%).7 These complications have been shown to prolong the hospital stay of patients, increase the financial burden on healthcare systems, and lead to an increased incidence of rehospitalization. Moreover, they have been associated with elevated long-term mortality rates.8
Presently, the predictive indicators for postoperative cardiopulmonary complications in lung cancer include pulmonary function tests, cardiac ultrasound, chest CT, and cardiopulmonary exercise testing. Nevertheless, these indicators are inadequate for predicting the occurrence of postoperative cardiopulmonary complications with sufficient accuracy.9 Recent studies have demonstrated that systemic inflammatory markers, including the neutrophil-to-lymphocyte ratio (NLR), the platelet-to-lymphocyte ratio (PLR), the lymphocyte-to-monocyte ratio (LMR), and the systemic immune-inflammatory index (SII), have a significant impact on the development of postoperative complications in patients undergoing cardiac, abdominal, and orthopedic surgery.9,10 Han11 et al demonstrated that NLR, MLR and PLR play a role in predicting survival in NSCLC patients. Ruan12 et al found that PLR and LMR can accurately predict pulmonary complications in surgical NSCLC patients. SII, by incorporating platelet dynamics, amplifies the thrombo-inflammatory cascade. Postoperative alterations (Δ) in these indicators are incorporated to capture real-time immune changes, as preoperative values lack sensitivity to intraoperative perturbations. In comparison to other indicators such as CRP or cytokines, these composite indicators offer a cost-effective and reproducible measure of systemic inflammation.
The objective of this study is to meticulously examine the systemic inflammatory indicators of lung cancer patients before and after surgery, with the aim of constructing a more precise prediction model for postoperative cardiopulmonary complications in lung cancer patients. This model will provide clinicians with a new tool for the accurate assessment of the risk of cardiopulmonary complications after surgery. It will also enable the timely identification and intervention of high-risk patients. Furthermore, it will provide a scientific basis for the comprehensive management of lung cancer patients.
Methods
Patients
The subjects of this retrospective study were patients who underwent lung resection surgery at our hospital between July 2022 and December 2024 and were diagnosed with non-small cell lung cancer after surgery. All patients were treated according to the clinical practice guidelines for thoracic surgery and perioperative management of lung cancer developed by the Chinese Society of Thoracic Surgery.This study was reviewed and approved by the hospital ethics committee, which waived the requirement for informed consent in accordance with the Declaration of Helsinki. All surgeries will be performed by our experienced surgical team according to standard procedures. Inclusion criteria for this study are: (1) patients who have completed lung resection; (2) the post-operative diagnosis was non-small cell lung cancer; (3) patients with complete clinical records. Exclusion criteria include: (1) age <18 years; (2) patients with pre-existing infectious diseases, haematological disorders, immune system disorders, or empyema prior to surgery; (3) patients undergoing total lung resection surgery; (4) individuals with poor medical compliance, automatic discharge, incomplete treatment processes, or missing data.
Study Protocol
The study was reviewed and endorsed by the institutional ethics committee. Its design and execution adhered to the Standards for Reporting Case-Control Studies (STROCSS).13 TThe research procedures were carried out in strict accordance with the Declaration of Helsinki (revised 2013).14 The sample size calculation method had already been employed before this study was conducted.15 The research flow chart is shown in Figure 1.
 |
Figure 1 Flow chart of this study. |
Definition of Postoperative Cardiopulmonary Complications
This study employed the diagnostic criteria for cardiovascular and pulmonary complications outlined in the extant literature, namely the STS/ESTS criteria.16 The researchers documented post-operative cardiovascular and pulmonary complications, including persistent lung leak, pulmonary infection, arrhythmia, acute myocardial infarction, pulmonary embolism, heart failure, empyema, bronchopleural fistula, secondary endotracheal intubation, and death, among others. The primary outcome measure is the occurrence of complications within 30 days following lung resection.
Data Collection and Potential Predictive Factors
In this study, based on relevant literature and clinical judgement, we retrospectively collected the medical records of patients who met the inclusion criteria through the hospital’s electronic medical record archiving system, quality control registration management system, and laboratory test report system. The information collected included: age, sex, smoking status, drinking status, body mass index (BMI), medical history (including chronic obstructive pulmonary disease, hypertension, diabetes, hyperlipidemia, cerebral infarction), operation plan (lobectomy and partial pneumonectomy), operation time, and laboratory test results (including routine blood test, liver function, kidney function, blood coagulation function, blood lipids) 1 week before and 1 day after operation. Based on the routine blood test results, we calculated the following inflammation indicators before and after surgery Systemic Immune Inflammatory Index (SII)=Neutrophil count (N) × Platelet count (P)/Lymphocyte count (L), Mononuclear Inflammatory Response Index (SIRI)=Neutrophil count (N) × Mononuclear cell count (M)/Lymphocyte count (L), Neutrophil to Lymphocyte Ratio (NLR)=Neutrophil Count (N)/Lymphocyte Count (L), Platelet to Lymphocyte Ratio (PLR).17 We subtract the preoperative value from the postoperative value to obtain the amount of change (Δ).
Development and Evaluation of Column Chart Models
A total of 693 patients were randomly assigned to the training and validation sets at a ratio of 7:3. To identify potential predictive factors, we performed logistic regression analysis on the training set and constructed a column chart model using multiple logistic regression. Column chart calibration was accompanied by the development of Hosmer-Lemeshow tests to determine the consistency between predicted and observed pollution events. The predictive accuracy and consistency of the model are assessed using the receiver operating characteristic (ROC) curve, the area under the ROC curve (AUC), the consistency index (C-index) and the calibration curve. In addition, Decision Curve Analysis (DCA) is used to reflect the net benefit of the model to patients. Identification and calibration are both performed by bootstrapping 1000 heavy samples.
Statistical Analysis
This study used Zstats software and R 4.4.0 software, combined with rms, pROC, ggplot2, and DCA software packages for data processing and analysis. For continuous data parameters, normal distribution is represented by mean ± standard deviation, while skewed distribution is represented by median (M) and quartile range (P25-P75); The count data is expressed as a ratio (%). All statistical tests were bilateral, and a P value<0.05 was considered statistically significant. By conducting binary logistic regression analysis, factors with P<0.05 were identified, and a column chart model was constructed using the RMS package in R software. The predictive performance and accuracy of the model are evaluated through the consistency index (C-index) and calibration chart method.
Results
Patient Characteristics
As shown in Table 1, a total of 693 eligible patients were included in this study. The entire cohort was randomly assigned to the training set (n=485) and the validation set (n=208). 102 patients experienced postoperative cardiopulmonary complications, 71 in the training set and 31 in the validation set. Statistical analysis showed no significant difference between the training and validation sets (P>0.05). Tables 1 and 2 shows the baseline characteristics of the patients.
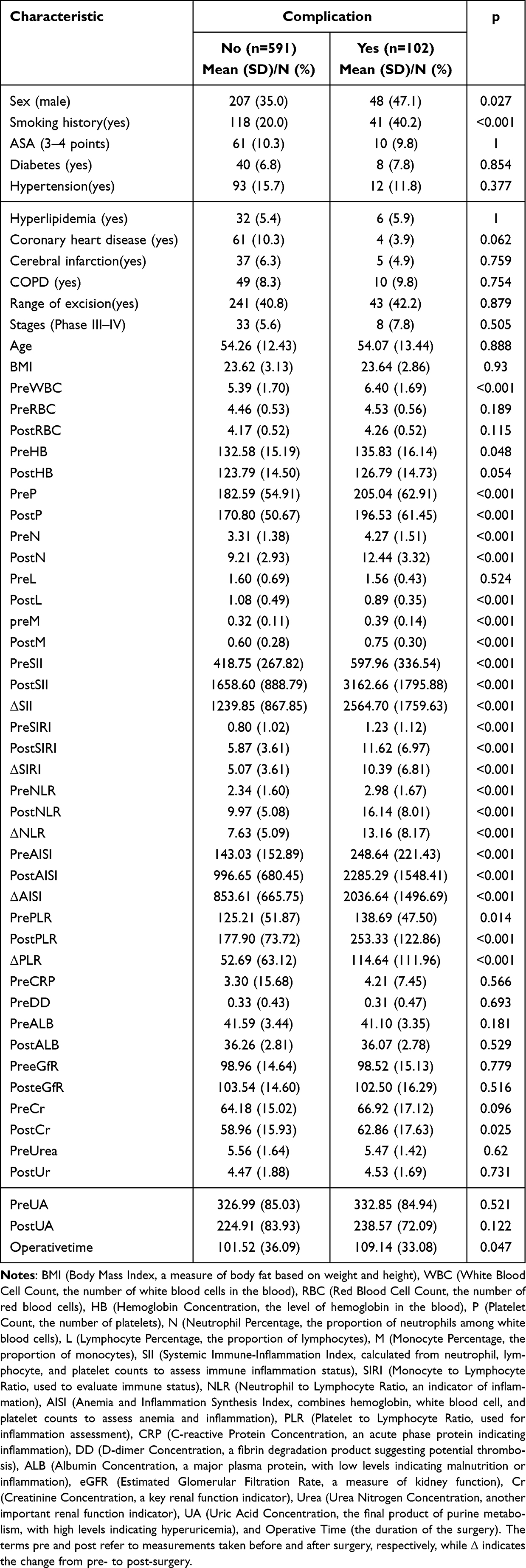 |
Table 1 Baseline Characteristics Between the Complication Group and the Non Complication Group |
 |
Table 2 Comparison of Training and Validation Sets |
Screening Predictive Factors
Using multivariate logistic regression analysis, we identified the following six factors as predictive of postoperative cardiopulmonary complications (p<0.05): smoking history (OR=1.97, 95% CI: 1.02–3. 81), postoperative neutrophil count (OR=1.31, 95% CI: 1.01–1.54), postoperative SII (OR=1.01, 95% CI: 1.01–1.01), Δ SII (OR=0.99, 95% CI: 0.99–0.99), Δ PLR (OR=1.01, 95% CI: 1.01–1.02) and Δ AISI (OR=1.01, 95% CI: 1.01–1.01) (Table 3).
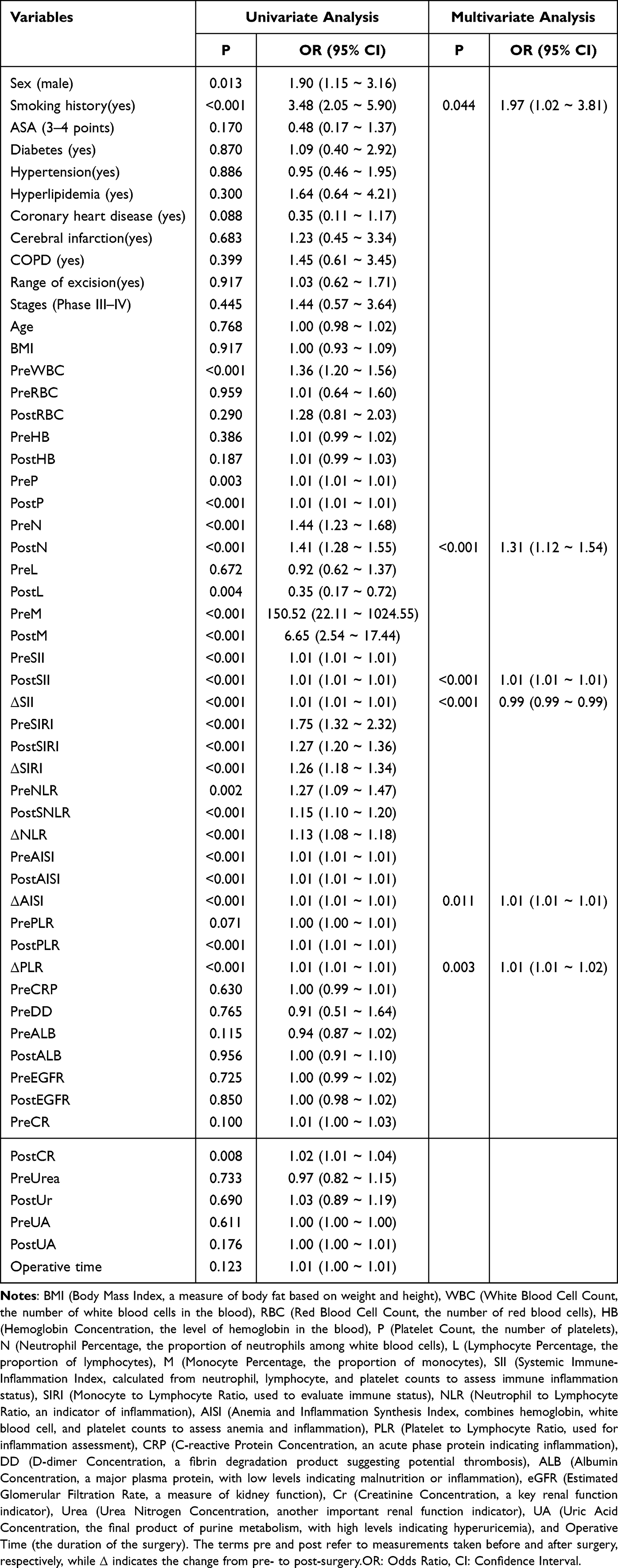 |
Table 3 Single Factor and Multiple Factor Logistic Regression Analyses Used for Screening Predictive Factors |
Develop Personalized Prediction Models
Based on multivariate logistic regression analysis, we created a column diagram to predict the risk of postoperative cardiopulmonary complications. This column chart includes six key clinical features: smoking history, postoperative neutrophil count, postoperative systemic immunoinflammatory index (SII), changes in postoperative systemic immunoinflammatory index (Δ SII), changes in platelet-lymphocyte ratio (Δ PLR), and changes in postoperative immunosuppression index (Δ AISI). Each feature is assigned a corresponding score based on its contribution to risk. For example, if the patient’s smoking history is 1 point, postN is 12 points, postSII is 3000 points, ASII is 2000 points, Δ AISI is −500 points, Δ PLR is 300 points, and the total score is 4813 points, the patient’s risk of postoperative complications can be predicted to be 50% based on the column chart. This prediction model helps doctors to identify high-risk patients in advance and take preventive measures to reduce the incidence of postoperative complications (Figure 2).
 |
Figure 2 Column chart for the research. |
Prediction Model Validation and Calibration
This study evaluated the stability and predictive performance of the prediction model on different datasets by analysing the ROC curves of the training and validation sets. The AUC value of the training set is 0.86, with a 95% confidence interval of 0.82 to 0.91, while the AUC value of the validation set is 0.81, with a 95% confidence interval of 0.73 to 0.89. This indicates that the model has good predictive ability on both independent datasets and the performance is consistent (Figures 3 and 4).
 |
Figure 3 ROC curve of the training set. |
 |
Figure 4 ROC curve of the validation set. |
Further decision curve analysis (DCA) revealed the value of the model under different high-risk thresholds. Compared to extreme strategies such as “do everything” or “do nothing”, this model can provide a higher net benefit for clinical decision making across a wide range of high-risk thresholds, particularly in the low-to-moderate risk threshold range where the net benefit of the model is more significant (Figures 5 and 6).
 |
Figure 5 Decision curve analysis [DCA] of the column chart of the training set. The green line signifies the assumption that no patients have dirt, while the red line indicates that all patients have dirt. The blue line corresponds to the risk column chart. |
 |
Figure 6 Decision curve analysis[DCA] of column chart of the validation set. The green line signifies the assumption that no patients have dirt, while the red line indicates that all patients have dirt. The blue line corresponds to the risk column chart. |
In addition, the Hosmer-Lemeshow test was used to assess the fit of the model. The P-values for the training and validation sets were 0.939 and 0.917 respectively, both greater than 0.05. This further confirms that there is no significant fit deviation between the model and the actual observed data, and that the model has a good fit. These data indicate that our column chart has enormous potential for clinical decision making (Figures 7 and 8).
 |
Figure 7 The calibration curve of the training set has a P-value >0.05 in the Hosmer Lemeshow test. |
 |
Figure 8 The calibration curve of the validation set, with a P value>0.05 in Hosmer Lemeshow test. |
This study evaluated the performance of the prediction model through system validation and calibration. The sensitivity of the model is 0.74 (95% confidence interval: 0.70–0.78), the specificity is 0.85 (95% confidence interval: 0.76–0.93), and the area under the receiver operating characteristic curve (AUC) is 0.86 (95% confidence interval: 0.82–0.91), confirming the excellent discriminative ability of the model. The optimal cut-off value determined by the Youden index is 4813 points, corresponding to a predicted risk probability of 50%. The positive predictive value (PPV) and negative predictive value (NPV) are 0.97 (95% confidence interval: 0.95–0.99) and 0.36 (95% confidence interval: 0.28–0.43), respectively. The calibration analysis shows that the predicted probability of the model is highly consistent with the actual observed results. The Hosmer-Lemeshow test P-values for the training and validation sets are 0.939 and 0.917, respectively, with a Brier score of 0.126 and a calibration slope of 0.98 (95% confidence interval: 0.92–1.04), indicating that the model has no significant overfitting and good calibration performance.
Discussion
Surgery, the classic treatment for lung cancer, still has a high incidence of postoperative cardiopulmonary complications. According to research reports, the incidence of cardiovascular and pulmonary complications after lung cancer surgery ranges from 16.4% to 31.7%,18 which has a significant impact on the postoperative recovery of patients. Currently, the methods for predicting postoperative cardiopulmonary complications in lung cancer mainly include traditional clinical indicators, scoring systems, lung ultrasound scores and other factors. Traditional clinical indicators include pulmonary function tests (PFTs), echocardiography, chest CT scans, and cardiopulmonary exercise testing (CPET). The scoring system includes APACHE II, ASA and POSSUM scores. In addition, age, open surgical approach, preoperative comorbidity with chronic obstructive pulmonary disease (COPD) and high preoperative white blood cell count have been confirmed as risk factors for postoperative cardiopulmonary complications.18–21
A recent study has demonstrated that the systemic immune-inflammatory index (SII) and forced expiratory volume in one second (FEV1) have the capacity to function as predictive factors for the occurrence of pulmonary complications subsequent to lung resection.22 Furthermore, the potential value of biomarkers of the systemic inflammatory response, such as albumin, neutrophil to lymphocyte ratio (NLR), mean platelet volume (MPV), lymphocyte to monocyte ratio (LMR), platelet to lymphocyte ratio (PLR), and systemic immune-inflammatory index (SII), in predicting postoperative complications has been demonstrated.23 A multicenter study further investigated the relationship between preoperative systemic inflammatory markers and long-term prognosis in patients with resectable non-small cell lung cancer (NSCLC). The study found that these preoperative inflammatory markers have significant predictive value for postoperative complications.24 This study also found that operating time is one of the most important factors influencing cardiovascular and pulmonary complications. Preliminary research has indicated that the likelihood of developing pneumonia, experiencing arrhythmias, and succumbing to mortality rises considerably when surgical duration exceeds 180 minutes.This phenomenon is primarily attributed to the exacerbation of tissue trauma, augmented fluid transfer, and subsequent activation of inflammatory responses during the surgical procedure.25 In light of these favorable outcomes, we have developed a pillar chart model based on systemic inflammatory factors to predict the occurrence of cardiovascular and pulmonary complications after lung cancer surgery. This model integrates key inflammatory markers such as neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), systemic immune inflammation index (SII) and other clinically relevant factors.The model’s objective is to provide clinicians with personalized risk assessment tools through visualisation.
The column chart has been widely used as a prediction model in clinical practice for both tumour and non-tumour diseases. It visually represents the possibility of clinical outcomes by integrating key factors.26 In this study, a column chart model was constructed to integrate the following factors: smoking history, postoperative neutrophil count, postoperative systemic immune inflammation index (SII), changes in postoperative SII (Δ SII), changes in platelet-lymphocyte ratio (Δ PLR), and changes in postoperative immune suppression index (Δ AISI). This particular column chart model is uncommon in contemporary research and offers a valuable enhancement to existing prediction methods. Several studies have provided evidence for the six aforementioned risk factors. It is well-documented that smoking constitutes a risk factor for postoperative complications in lung cancer. Research has demonstrated that a history of smoking constitutes a significant risk factor for the development of postoperative pneumonia in cancer patients.27 Furthermore, an elevated preoperative neutrophil count has been demonstrated to be associated with an augmented risk of postoperative infection, thereby suggesting a potential role for neutrophils in the development of postoperative complications. The systemic immune-inflammatory index (SII) has also been demonstrated to serve as a significant prognostic indicator. Despite the paucity of direct research on changes in postoperative SII (Δ SII) and platelet-lymphocyte ratio (Δ PLR), it is postulated that these indicators may serve as a reflection of the dynamic changes in the postoperative inflammatory response and immune status, which are closely related to the risk of postoperative complications.28 In addition, changes in the immunosuppression index (ΔAISI) may also be associated with changes in postoperative immune status and risk of complications.28
The present study constructed a columnar diagram of systemic inflammatory factors and their dynamic changes. In one study, known risk factors such as advanced age, previous pneumonia, and chronic lung disease were examined to investigate the role of postoperative changes in SII (Δ SII), changes in platelet-lymphocyte ratio (Δ PLR), and changes in immunosuppression index (Δ AISI) in predicting postoperative complications.29 Other studies30 were conducted to examine the impact of postoperative SII changes (ΔSII), platelet-lymphocyte ratio changes (ΔPLR), and immune suppression index changes (ΔAISI) on the prediction of postoperative complications. The study’s objective was to investigate the role of these changes in predicting postoperative complications, and the study’s participants included patients with known risk factors such as age, comorbidities of COPD, and duration of surgery. In comparison with existing research, our model not only validated these known risk factors but also systematically integrated the dynamic changes of inflammation and immune markers. This integration was especially notable in dynamic indicators such as Δ SII, Δ PLR, and Δ AISI, which demonstrated significant independent value in predicting postoperative complications. Furthermore, we have, for the first time, explored in detail the potential association between Δ PLR and Δ AISI and postoperative complications in the context of cancer surgery, thereby adding to our current understanding of changes in postoperative immune status and their impact. This column chart methodically examines postoperative dynamic alterations (Δ SII, Δ PLR, Δ AISI) in conjunction with clinical factors (eg, smoking history) and laboratory-related factors. In contrast to conventional models, our approach encompasses not only inflammation rates but also dynamic indicators and a more comprehensive analysis. Consequently, our study offers a more precise and personalized predictive instrument for risk assessment of postoperative complications. A comprehensive strategy to reduce the risk of postoperative complications in NSCLC resection has been identified through a column chart analysis. This strategy includes preoperative emphasis on smoking cessation intervention, control of pulmonary infections, strengthening pulmonary rehabilitation training, and improving FEV1 levels and exercise tolerance. During surgery, minimally invasive surgical techniques should be used and efforts should be made to shorten the operation time. After surgery, patients should be encouraged to engage in early activities and implement optimized pain management plans.
Limitations
This study has several limitations. Firstly, it is a retrospective study, which may suffer from selection bias and information bias, which may limit the completeness and accuracy of the data. Secondly, the sample size is relatively limited, and for some rare postoperative cardiopulmonary complications, it may not be possible to fully evaluate their relationship with systemic inflammatory indicators. The sample size limitation may also affect the extrapolation and universality of the model. In addition, the data in this study came from a single centre and may be influenced by specific medical environments and patient populations, which limits the generalisability of the research findings. Meanwhile, this study mainly focused on systemic inflammatory factors and their dynamic changes, but the occurrence of postoperative cardiopulmonary complications may be influenced by a combination of multiple factors, such as the patient’s psychological state, nutritional status, postoperative pain management, etc. Future research can widen the scope of the study to include more potential confounding factors. Although this study performed internal validation of the model through random assignment of training and validation sets, external validation is lacking. Future research can perform external validation in other independent patient cohorts to verify the universality of the model. Finally, this study can only demonstrate an association between systemic inflammatory factors and postoperative cardiopulmonary complications, but cannot establish causality. Future studies can use prospective cohort studies or randomised controlled trials to further investigate the causal relationship between these factors and complications.
Conclusion
This study provides a new perspective and scientific basis for predicting postoperative cardiopulmonary complications in lung cancer by constructing a column chart containing systemic inflammatory factors and their dynamic changes. We included six key factors: smoking history, postoperative neutrophil count, postoperative systemic immune inflammation index (SII), changes in postoperative SII (Δ SII), changes in platelet-lymphocyte ratio (Δ PLR), and changes in immune suppression index (Δ AISI) as evaluation factors to construct a more accurate and personalised prediction tool. We have confirmed the stability and reliability of the model through internal validation, and this predictive model has important value for post-operative patient identification and risk stratification to support clinicians’ treatment plans.
Ethical Approval
This study was approve by the Ethics Committee of the First People’s Hospital of Shuangliu District, Chengdu (2024-02-wen-01) and conducted under the tenets of the Declaration of Helsinki.The ethics committee waived informed consent for this retrospective study as it did not intervene in any way with the subjects, and all data collection was conducted in accordance with ethical standards.
Consent
The written informed consent is not related to this manuscript.
Funding
Chengdu Medical Research Project (2022103, 2021068).
Disclosure
The authors declare no conflicts of interest.
References
1. Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021;398(10299):535–554. doi:10.1016/S0140-6736(21)00312-3
2. Zheng RS, Chen R, Han BF. Cancer incidence and mortality in China, 2022. Zhonghua Zhong Liu Za Zhi. 2024;46(3):221–231. doi:10.3760/cma.j.cn112152-20240119-00035
3. Hoy H, Lynch T, Beck M. Surgical Treatment of Lung Cancer. Crit Care Nurs Clin North Am. 2019;31(3):303–313. doi:10.1016/j.cnc.2019.05.002
4. Nojiri T, Hamasaki T, Inoue M. Long-Term Impact of Postoperative Complications on Cancer Recurrence Following Lung Cancer Surgery. Ann Surg Oncol. 2017;24(4):1135–1142. doi:10.1245/s10434-016-5655-8
5. Salter KD, Burt BM. Necessity of the heart, for lung resection. J Thorac Dis. 2019;11(S9):S1132–S1134. doi:10.21037/jtd.2019.04.72
6. Stéphan F, Boucheseiche S, Hollande J. Pulmonary complications following lung resection: a comprehensive analysis of incidence and possible risk factors. Chest. 2000;118(5):1263–1270. doi:10.1378/chest.118.5.1263
7. Chughtai M, Gwam CU, Mohamed N. The Epidemiology and Risk Factors for Postoperative Pneumonia. J Clin Med Res. 2017;9(6):466–475. doi:10.14740/jocmr3002w
8. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
9. Piccioni F, Spagnesi L, Pelosi P. Postoperative pulmonary complications and mortality after major abdominal surgery. An observational multicenter prospective study. Minerva Anestesiol. 2023;89(11):964–976. doi:10.23736/S0375-9393.23.17382-2
10. Ali KA, He L, Deng X, Pan J, Huang H, Li W. Assessing the predictive value of pre- and post-operative inflammatory markers in patients undergoing total knee arthroplasty. J Orthop Surg Res. 2024;19(1):614. doi:10.1186/s13018-024-05104-0
11. Han R, Zhang F, Nlr HQ. NLR, MLR, and PLR are adverse prognostic variables for sleeve lobectomy within non-small cell lung cancer. Thorac Cancer. 2024;15(24):1792–1804. doi:10.1111/1759-7714.15405
12. Ruan Y, Cao W, Han J, Yang A, Xu J, Zhang T. Impact of preoperative inflammatory biomarkers on postoperative pneumonia and one-month pulmonary imaging changes after surgery for non-small cell lung cancer. Front Oncol. 2025;15:1489068. doi:10.3389/fonc.2025.1489068
13. Agha RA, Borrelli MR, Vella-Baldacchino M, Thavayogan R, Orgill DP. The STROCSS statement: strengthening the Reporting of Cohort Studies in Surgery. Int J Surg. 2017;46:198–202. doi:10.1016/j.ijsu.2017.08.586
14. World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
15. Latouche A, Porcher R, Chevret S. Sample size formula for proportional hazards modelling of competing risks. Stat Med. 2004;23(21):3263–3274. doi:10.1002/sim.1915
16. Brunelli A, Beretta E, Cassivi SD. Consensus definitions to promote an evidence-based approach to management of the pleural space. A collaborative proposal by ESTS, AATS, STS, and GTSC. Eur J Cardiothorac Surg. 2011;40(2):291–297. doi:10.1016/j.ejcts.2011.05.020
17. Yao W, Wang W, Tang W, Lv Q, Ding W. Neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and systemic immune inflammation index (SII) to predict postoperative pneumonia in elderly Hip fracture patients. J Orthop Surg Res. 2023;18(1):673. doi:10.1186/s13018-023-04157-x
18. Liu J, Yang X, Liu X, Xu Y, Huang H. Predictors of Readmission After Pulmonary Resection in Patients With Lung Cancer: a Systematic Review and Meta-analysis. Technol Cancer Res Treat. 2022;21:15330338221144512. doi:10.1177/15330338221144512
19. Brunelli A, Kim AW, Berger KI, Addrizzo-Harris DJ. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5):e166S–e190S. doi:10.1378/chest.12-2395
20. Watanabe Y, Hattori A, Fukui M. Postoperative complications and perioperative management in patients on hemodialysis undergoing lung resection. Gen Thorac Cardiovasc Surg. 2021;69(3):478–486. doi:10.1007/s11748-020-01489-x
21. He Z, Li H, Cao B. Predictive Value of Skeletal Muscle Function Test Combined with Climbing Test for Postoperative Cardiopulmonary Complications in Patients with COPD and Concurrent Lung Cancer. Int J Chron Obstruct Pulmon Dis. 2023;18:2699–2706. doi:10.2147/COPD.S438336
22. Mazzella A, Maiolino E, Maisonneuve P, Loi M, Alifano M. Systemic Inflammation and Lung Cancer: is It a Real Paradigm? Prognostic Value of Inflammatory Indexes in Patients with Resected Non-Small-Cell Lung Cancer. Cancers. 2023;15(6):1854. doi:10.3390/cancers15061854
23. Russo E, Guizzardi M, Canali L. Preoperative systemic inflammatory markers as prognostic factors in differentiated thyroid cancer: a systematic review and meta-analysis. Rev Endocr Metab Disord. 2023;24(6):1205–1216. doi:10.1007/s11154-023-09845-x
24. Zhang CL, Gao MQ, Jiang XC. Research progress and value of albumin-related inflammatory markers in the prognosis of non-small cell lung cancer: a review of clinical evidence. Ann Med. 2023;55(1):1294–1307. doi:10.1080/07853890.2023.2192047
25. Baar W, Semmelmann A, Anselm F, Loop T, Heinrich S. Registry FTWGOTGT. Risk Factors for Postoperative Pulmonary Complications in Patients Undergoing Thoracotomy for Indications Other than Primary Lung Cancer Resection: a Multicenter Retrospective Cohort Study from the German Thorax Registry. J Clin Med. 2025;14(5):1565. doi:10.3390/jcm14051565
26. Sghir N, Adadi A, Lahmer M. Recent advances in Predictive Learning Analytics: a decade systematic review (2012–2022). Educ Inf Technol. 2022;1–35. doi:10.1007/s10639-022-11536-0
27. Deng T, Song J, Tuo J. Incidence and risk factors of pulmonary complications after lung cancer surgery: a systematic review and meta-analysis. Heliyon. 2024;10(12):e32821. doi:10.1016/j.heliyon.2024.e32821
28. Furák J, Németh T, Lantos J. Perioperative Systemic Inflammation in Lung Cancer Surgery. Front Surg. 2022;9:883322. doi:10.3389/fsurg.2022.883322
29. Yao L, Luo J, Liu L. Risk factors for postoperative pneumonia and prognosis in lung cancer patients after surgery: a retrospective study. Medicine. 2021;100(13):e25295. doi:10.1097/MD.0000000000025295
30. Simonsen DF, Søgaard M, Bozi I, Horsburgh CR, Thomsen RW. Risk factors for postoperative pneumonia after lung cancer surgery and impact of pneumonia on survival. Respir Med. 2015;109(10):1340–1346. doi:10.1016/j.rmed.2015.07.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association of the Neutrophil-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio and Systemic Inflammation Response Index with Short-Term Functional Outcome in Patients with Acute Ischemic Stroke
Zhang YX, Shen ZY, Jia YC, Guo X, Guo XS, Xing Y, Tian SJ
Journal of Inflammation Research 2023, 16:3619-3630
Published Date: 23 August 2023
The Potential Value of Systemic Inflammation Response Index on Delirium After Hip Arthroplasty Surgery in Older Patients: A Retrospective Study
Lu W, Lin S, Wang C, Jin P, Bian J
International Journal of General Medicine 2023, 16:5355-5362
Published Date: 21 November 2023
Predictive Role of Blood Cell-Derived Inflammatory Markers for the Risk of Asymptomatic Cerebral Infarction in Essential Hypertension: A Population-Based Cross-Sectional Study in Central China
Zhang Q, Wang M, Du H, Qu H, Liu K, Dong W, Kong D, Tian D, Zhao X, Hao Y, Liu M
Journal of Inflammation Research 2025, 18:3523-3534
Published Date: 11 March 2025
A Nomogram for Diagnosing Ventilator-Associated Pneumonia Using Circulating Inflammation Indicators in ICU Patients
Yang J, Bao W, Wang H, Zhou J, Hu Q, Wang Y, Li Y
Journal of Inflammation Research 2025, 18:4615-4625
Published Date: 2 April 2025