")
Back to Journals » Clinical Ophthalmology » Volume 19
Nystagmus in Clinical Practice: From Diagnosis to Treatment—A Comprehensive Review
Authors Gurnani B , Kaur K, Chaudhary S , Gandhi AS, Balakrishnan H, Mishra C, Gosalia H, Dhiman S, Joshi S, Nagtode AH, Jain S, Aguiar M, Rustagi IM
Received 17 February 2025
Accepted for publication 8 May 2025
Published 17 May 2025 Volume 2025:19 Pages 1617—1657
DOI https://doi.org/10.2147/OPTH.S523224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Nystagmus in Clinical Practice – Video S3 [523224]
Views: 83
Bharat Gurnani,1 Kirandeep Kaur,2 Sameer Chaudhary,3 Adit Samir Gandhi,3 Harinikrishna Balakrishnan,3 Chitaranjan Mishra,4 Hirika Gosalia,5 Shweta Dhiman,6 Saloni Joshi,7 Apurva H Nagtode,8 Shreya Jain,3 Marushka Aguiar,9 Inder Mohan Rustagi10
1Department of Cataract, Cornea and Refractive Surgery, Gomabai Netralaya and Research Centre, Neemuch, MP, India; 2Department of Cataract, Pediatric Ophthalmology and Strabismus, Gomabai Netralaya and Research Centre, Neemuch, MP, India; 3Department of General Ophthalmology, Aravind Eye Hospital, Madurai, TN, India; 4Department of Vitreo-Retina, Trilochan Netralaya, Sambalpur, Odisha, India; 5Department of Cornea, LV Prasad Eye Institute, Hyderabad, AP, India; 6Department of Pediatric Ophthalmology and Squint, JPM Rotary Eye Hospital and Research Institute, Cuttack, Odisha, India; 7Department of Glaucoma, Aravind Eye Hospital, Pondicherry, India; 8Department of Cornea and Refractive Services, Aravind eye hospital, Pondicherry, India; 9Department of Pediatric Ophthalmology and Squint, KBH Bachooali Eye and ENT Hospital, Mumbai, Maharashtra, India; 10Department of Ophthalmology, Triveni Hospital Private Limited, Gurugram, Harayana, India
Correspondence: Bharat Gurnani, Department of Cataract, Cornea and Refractive Surgery, Gomabai Netralaya and Research Centre, Neemuch, MP, 458441, India, Tel +919080523059, Email [email protected]
Abstract: Nystagmus, a common yet intricate ocular movement disorder, significantly contributes to visual morbidity in the paediatric and adult populations. Defined by involuntary, rhythmic, to-and-fro eye movements, this condition may manifest as an isolated anomaly or harbour more serious ocular or systemic pathologies. Its presence often provides vital diagnostic clues, emphasizing the importance of thorough evaluation to uncover potentially hidden underlying conditions. These mechanisms may range from dysfunction in the neural pathways to genetic mutations that affect ocular motor control. Nystagmus can profoundly affect visual acuity, spatial perception, and overall quality of life, leading to challenges in education, employment, and daily activities for the affected individuals. The diverse classifications of nystagmus, spanning congenital, acquired, and spontaneous forms, have distinct aetiologies, clinical features, and therapeutic considerations. For clinicians, a structured and systematic approach is essential for an accurate diagnosis and management. Advances in diagnostic modalities, including high-resolution imaging, electrodiagnostic studies, and eye tracking technologies, have enhanced our ability to delineate the underlying pathology. Similarly, therapeutic innovations such as pharmacological interventions, surgical techniques such as tenotomy, and even gene therapy and neurostimulation are opening new avenues for managing this disorder. A robust literature search was conducted using PubMed, MEDLINE, Cochrane, and EMBASE. The search strategy incorporated MeSH terms including “nystagmus”, “classification”, “diagnosis”, and “treatment”, and included both English and non-English articles up to December 2024. Studies were selected based on relevance to clinical features, pathophysiology, and recent advances in the field. This review offers a comprehensive exploration of the epidemiology, classification, clinical presentation, diagnostic strategies, and treatment of nystagmus. It also sheds light on recent advancements and emerging research, including the integration of artificial intelligence in clinical diagnostics. Ultimately, this review aims to serve as a practical clinical reference that enhances diagnostic accuracy and optimizes patient care within the ophthalmic and neuro-ophthalmic communities.
Keywords: nystagmus, involuntary movements, Jerk Nystagmus, pendular nystagmus, ocular motor disorder
Introduction
Nystagmus is a disorder characterised by uncontrolled, repetitive to-and-fro movements of the eyes in a rhythmic pattern that may be physiological or pathological.1 It can occur as an isolated disorder but is most commonly part of an underlying ophthalmic or systemic disorder and is the most obvious or first presenting feature.2 It is common and affects both paediatric and adult age groups. The movements can be horizontal, vertical, torsional, or a combination of both. It usually starts as a slow movement of the eye away from the target, followed by a second movement to re-fixate back onto the target. If the second movement is fast, it is called jerk nystagmus, whereas a slow second movement is characterised by pendular nystagmus.2 However, with that said, the classification and waveforms of nystagmus remain highly intricate, and are based on aetiology, electronystagmography, and pathogenesis. The mechanisms underlying nystagmus remain unclear, and several hypotheses and models have been proposed to explain its pathogenesis. As nystagmus remains a multifaceted condition, the clinical and laboratory assessments of nystagmus in patients with neurological disorders can provide crucial information for differential diagnosis. This can provide insight into various systemic disorders and aid in their diagnosis.3 Moreover, these involuntary eye movements can negatively affect visual function and quality of life, making nystagmus an important complex ocular condition.4 Visual acuity may be limited, and patients may experience vertigo, oscillopsia, or adjusted head posture.3,5 This makes it imperative to understand the various types, underlying mechanisms, causes, assessment, and treatment of nystagmus. A diagnosis should be established using clinical assessment and confirmed by various investigations, including electrophysiological tests, optical coherence tomography, neuroimaging, and genetic workup.3 Once the diagnosis is confirmed, the underlying treatment is tailored to the diagnosis and aims to alleviate the visual symptoms and address the underlying aetiology. This review provides a comprehensive and structured description of the epidemiology, classification, clinical features, diagnostic workup, treatment, and recent advances in nystagmus. Moreover, this review uniquely integrates a comprehensive neuroanatomical and pathophysiological correlation for each subtype of nystagmus, offering readers a clearer clinical framework for differentiating among complex presentations. Unlike previous reviews, we have clubbed traditional classifications with newer diagnostic paradigms, incorporating nystagmoid movements, waveform analysis, and triggered nystagmus variants—areas which were either underrepresented or not structurally detailed in earlier works. Additionally, we have included updated neuro-ophthalmic diagnostic algorithms, realigned classifications by modern etiological groups (eg, vestibular, cerebellar, paraneoplastic), and introduced emerging diagnostic tools such as eye-tracking-based waveform analysis and AI-assisted vestibular testing, which reflect recent clinical advances. Importantly, we have also included a dedicated section outlining recent advances in treatment modalities and the evolving role of artificial intelligence (AI) in the diagnosis and monitoring of nystagmus, which further strengthens the clinical relevance of this work.
Methods of Literature Search
To comprehensively explore the broad spectrum of nystagmus, a systematic literature review was conducted using multiple biomedical databases, including PubMed, Cochrane Library, MEDLINE, EMBASE, PubMed Central, and Google Scholar. The search included studies published until December 2024. Medical Subject Headings (MeSH) such as “Nystagmus”, “Nystagmoid”, and “Involuntary Ocular Movements” were combined with keywords including “congenital”, “acquired”, “waveforms”, “classification”, “epidemiology”, “diagnosis”, “treatment”, “clinical evaluation”, and “rehabilitation”. Boolean operators “AND” and “OR” were applied to ensure a wide yet focused retrieval of relevant articles. The titles and abstracts were screened independently by two reviewers for relevance. Full-text articles were assessed for eligibility based on predefined inclusion criteria such as relevance to clinical, diagnostic, pathophysiological, or therapeutic aspects of nystagmus. Studies not in English were translated when feasible. Reference lists of included articles were scanned to identify additional literature. Duplicate records and unrelated articles were excluded. The final selection comprised peer-reviewed original studies, review articles, and clinical guidelines. This rigorous selection ensured a well-rounded understanding of current concepts and advances in the diagnosis and management of nystagmus (Figure 1).
 |
Figure 1 Depicts the flowchart for literature search strategy for Nystagmus. |
Epidemiology
The prevalence of pathologic nystagmus is estimated to be 24 per 10,000, with a slight predilection towards European ancestry. According to Sarvananthan et al.6 The prevalence is 16.6/10,000, with the most common form of nystagmus attributed to infantile nystagmus associated with albinism.6 Among adults, the prevalence was estimated to be 26.5 per 10,000, with the largest nystagmus group being associated with neurological diseases.6 According to a study by Hvid et al, the overall prevalence of infantile nystagmus in a large Danish population is 6.1 per 10,000 live births.7 It was higher in premature children (28.4/10,000 live births) than in children born at term (4.4/10,000) and was highest in children born extremely preterm (97.3/10,000).7 According to Nash et al, the annual age- and sex-adjusted incidence of all forms of paediatric nystagmus is 6.72 per 100,000 people.8 Among those with infantile nystagmus, the birth prevalence was one in 821 live births.8 In another study by Ehrt et al, acquired nystagmus was estimated to account for 17% of nystagmus cases in children and 40% in adults.9
Classification of Nystagmus
Categorisation of involuntary eye movements has led to a degree of ambiguity and uncertainty.10–16 The Classification of Eye Movement Abnormalities and Strabismus (CEMAS) system categorises nystagmus based on its oscillation type, direction, and amplitude. The Classification Committee of the Barany Society established different classifications of nystagmus for clinical and research purposes.
Based on Etiology
Nystagmus can be broadly classified as physiological or pathological (Figure 2).
 |
Figure 2 Depicts the etiological classification of nystagmus. It classifies nystagmus broadly into physiological and pathological types. |
Physiological Nystagmus
Physiologic End-Point Nystagmus
Nystagmus in the absence of any pathology due to normal variation in gaze-holding ability.17 Arises from the normal functioning of the neural integrator (gaze-holding mechanism), primarily involving the nucleus prepositus hypoglossi and medial vestibular nucleus (for horizontal gaze) and interstitial nucleus of Cajal (for vertical gaze). In healthy individuals, when the eyes are held at extreme eccentric gaze (usually beyond 30°), the integrator system cannot sustain tonic activity indefinitely, causing a drift back toward midline followed by corrective saccades. This results in a low-amplitude, horizontal jerk nystagmus with the fast phase directed toward the gaze. This is a benign phenomenon and differs from gaze-evoked nystagmus due to cerebellar or brainstem pathology by being symmetrical, non-progressive, and usually non-sustained.18
Per-Rotational Nystagmus
Horizontal jerk nystagmus due to sustained head rotations with fast phases ipsilateral to the rotation (Video S1).19 Mediated by the horizontal semicircular canals, vestibular nerve, vestibular nuclei, and the medial longitudinal fasciculus (MLF) projecting to ocular motor nuclei. During sustained head rotation, endolymph flow in the semicircular canals causes deflection of the cupula, stimulating the vestibulo-ocular reflex (VOR). This triggers slow eye movement opposite to head movement, followed by fast saccades in the direction of rotation to reset gaze. This nystagmus is horizontal, jerk, with fast phase in the direction of rotation. It is transient and stops when the head motion ceases.13
Post-Rotational Nystagmus
Horizontal nystagmus occurs when the body is rotated and after the rotation is stopped, with a contralateral fast phase and subjective rocking boat sensation.20 Same central pathways as per-rotational, involving vestibular labyrinth → vestibular nuclei → ocular motor nuclei via MLF. After rotation stops, the endolymph continues to move briefly due to inertia, producing the illusion of continued rotation. This causes eye movements with a fast phase opposite the direction of the prior spin. Often associated with vertigo and a subjective sense of motion (rocking or spinning). It is a testable component of vestibular function and adapts quickly.15
Optokinetic Nystagmus
Optokinetic nystagmus (OKN) is the physiological movement of the eyes in response to a large moving target in the visual field. It is characterised by a smooth pursuit movement, followed by a saccade back to the primary gaze.21 Involves a complex network: retina → pretectal nucleus → nucleus of the optic tract → vestibular nuclei and cerebellum → ocular motor nuclei. The OKN system complements the VOR by stabilizing images during slow movements of the visual field. The eyes pursue a moving target (slow phase), then make a quick reset saccade (fast phase) to acquire the next target. Symmetrical horizontal OKN is normal. Asymmetry or absence may suggest parietal lobe lesions, strabismus, or developmental abnormalities (eg, infantile nystagmus).15
Optokinetic After-Nystagmus
Ipsilateral optokinetic nystagmus persists even after the visual stimulus stops. It occurs for seconds, and then stops. Same as OKN, with more pronounced influence from the cerebellar flocculus and nodulus, which integrate velocity storage. After prolonged optokinetic stimulation, the velocity storage mechanism continues to discharge even after the stimulus stops, producing continued nystagmus in the same direction for several seconds. This is a normal transient response, more prominent in children or after long exposures. Prolongation beyond typical duration may suggest cerebellar dysfunction.15
Caloric Nystagmus
VOR reflex elicited by stimulation of the tympanic membrane and horizontal semi-circular canals with warm or cold water. Cold water stimulation causes nystagmus with a fast phase away from the side of the stimulus. Warm-water stimuli cause nystagmus with a fast phase toward the side of the stimulus. Absence of these markers may indicate brain death.22 Primarily stimulates the horizontal semicircular canals, with signal transmission via the superior vestibular nerve → vestibular nuclei → contralateral abducens and ipsilateral medial rectus nuclei. Pathophysiology: Irrigation with warm or cold water creates a temperature gradient in the horizontal canal, inducing endolymph movement and cupular deflection. Cold water → hyperpolarization → fast phase away. Warm water → depolarization → fast phase toward. Asymmetric or absent responses indicate vestibular hypofunction or brainstem death if bilaterally absent.23
Magnetic Vestibular Stimulation–Induced Nystagmus
Nystagmus that occurs while a patient is undergoing magnetic resonance imaging (MRI), depending on the strength and direction of the field.24 Involves the vestibular end organs, particularly the horizontal canals, responding to magnetic field-induced forces on endolymph or otoliths. High-strength MRI fields can induce ionic currents or pressure gradients in the labyrinth due to the Lorentz force, resulting in tonic stimulation of the horizontal canal and subsequent nystagmus. This may produce horizontal nystagmus in the scanner, which resolves after exiting the field. It is more prominent in supine positions and can be misinterpreted if not recognized.25
Recent studies have advanced our understanding of physiological nystagmus, particularly in the context of gaze-evoked nystagmus (GEN) and its characteristics in healthy individuals. Ritter et al investigated the occurrence of physiological GEN in healthy subjects during prolonged horizontal eccentric gaze at angles between 30° and 45°. The findings revealed that physiological GEN was elicited in all participants, with prevalence increasing at greater eccentricities: 71% at 30° and 100% at 40–45° The study also noted that eye drift velocities decreased during sustained eccentric gaze, indicating an increase in gaze stability over time. Additionally, physiological rebound nystagmus (RN) was observed in 21% of subjects after eccentric gaze at 30°, with higher prevalence at greater eccentricities. These findings provide quantitative benchmarks for eye drift velocities and the prevalence of physiological nystagmus in healthy individuals.26 Ozawa et al explored the stochastic properties of physiological GEN, also referred to as end-point nystagmus (EPN). The study suggested that healthy individuals commonly exhibit physiological GEN at wide horizontal gaze angles, ranging from −40° to 40°. This research highlights the variability and commonality of physiological GEN in the general population.27
Pathological Nystagmus
Abnormal nystagmus due to damage to vestibular-oculocephalic or cortical areas affecting oculomotor function.
Spontaneous Nystagmus
This subtype of nystagmus refers to involuntary rhythmic eye movements with alternating fast and slow components while the eyes are in the primary position without any provoking stimuli (Figure 3).
 |
Figure 3 Depicts the different types of spontaneous pathological nystagmus. |
Spontaneous Peripheral Vestibular Nystagmus
Spontaneous jerk nystagmus due to an imbalance in vestibular tone between the labyrinths or vestibular nerves, which usually follows a horizontal-torsional pattern.28, Arises from the peripheral vestibular apparatus, particularly the labyrinth (semicircular canals, utricle) or vestibular nerve. Input is transmitted to the vestibular nuclei in the brainstem, which then project via the medial longitudinal fasciculus (MLF) to ocular motor nuclei (III, IV, VI). Damage to one labyrinth (eg, vestibular neuritis) causes tonic imbalance between the left and right vestibular inputs. The intact side exerts a stronger influence, interpreted by the brain as continuous head movement. This activates the vestibulo-ocular reflex (VOR), producing a slow phase toward the lesioned side and a fast phase (corrective saccade) toward the intact side—resulting in jerk nystagmus.29
Features
- Direction-fixed (usually horizontal-torsional)
- Follows Alexander’s Law: increases in amplitude when gazing in direction of fast phase
- Inhibited by fixation (best seen in darkness or with Frenzel goggles)
- Often accompanied by vertigo, nausea, imbalance
- Fast phase is away from the lesion
Spontaneous Central Vestibular Nystagmus
Central forms of vestibular nystagmus arise from the dysfunction of the interconnections between the central vestibular structures and neural integrators.30 It can be horizontal or vertical. Originates in the brainstem or cerebellum, especially in areas like the vestibular nuclei, nucleus prepositus hypoglossi, interstitial nucleus of Cajal, flocculus, nodulus, and medullary reticular formation. Central vestibular nystagmus occurs due to lesions that impair the neural integrators for gaze-holding or disrupt the central vestibulo-ocular pathways. These include: brainstem strokes or demyelination, cerebellar infarcts or degeneration, tumors or neurodegenerative diseases. The direction be horizontal, vertical, or purely torsional. Direction-changing with gaze (unlike peripheral). Not suppressed by fixation. May not follow Alexander’s Law. Often associated with other neurological signs (eg, diplopia, ataxia, dysarthria) Fast phase may be toward or away from lesion, depending on location.13
Predominantly Horizontal Central Vestibular Nystagmus
Direction-Fixed Horizontal Central Vestibular Nystagmus
This is predominantly horizontal. It remains direction-fixed in the primary gaze position, which means that it beats either towards the normal or the pathological side in a fixed direction (Video S1). While direction-fixed nystagmus is more typical of peripheral lesions, certain brainstem pathologies, particularly involving vestibular nuclei or their commissural connections, may produce a direction-fixed horizontal nystagmus. Central lesions may cause tonic imbalance in vestibular output, mimicking peripheral vestibular tone asymmetry. However, the lack of suppression with fixation, absence of vertigo, and associated neurological signs help differentiate it from its peripheral counterpart. Though direction-fixed, if central, it may not follow Alexander’s law and is not inhibited by visual fixation. Often requires MRI to rule out brainstem infarcts or demyelinating lesions.4
Latent Nystagmus
Conjugate horizontal jerk nystagmus that manifests only on monocular occlusion.31 Arises due to disruption of binocular visual input control over the brainstem nuclei, especially involving the accessory optic system and vestibular integrators. In patients with congenital strabismus or infantile esotropia, latent nystagmus is a manifestation of impaired fusion. It is absent when both eyes are open, but when one eye is occluded, the uncovered eye exhibits a conjugate horizontal jerk nystagmus with fast phase toward the uncovered eye. Latent nystagmus is a hallmark of fusional disruption and is part of the “nystagmus compensation syndrome.” It may coexist with congenital motor nystagmus and improves with binocular fixation.31
Periodic Alternating Nystagmus (PAN)
Horizontal, conjugate, jerk nystagmus that periodically alternates direction in the fast phase. PAN commonly occurs in association with Chiari malformation, multiple sclerosis, cerebellar ataxia, and stroke. Originates in the nodulus and uvula of the cerebellum, regions that regulate the velocity storage mechanism of the vestibular system. PAN is characterized by cyclic reversal of nystagmus direction, typically every 90–120 seconds. The mechanism involves dysfunctional velocity storage integration, possibly due to lesions in the vestibulo-cerebellum or brainstem. Associated with Chiari malformation, multiple sclerosis, cerebellar degeneration, or brainstem stroke. Nystagmus may respond to baclofen, a GABA agonist that resets the velocity storage cycle. PAN is purely horizontal, and changes direction periodically, unlike most other nystagmus types.32
Bruns Nystagmus
This is a bidirectional nystagmus characterised by coarse, high-amplitude horizontal movements with low oscillatory frequency as the patient looks towards the side of the lesion, which transforms into a fine, low-amplitude, high-frequency primary-position nystagmus that increases as the patient looks to the side opposite to the lesion. It is most commonly observed in cerebellopontine angle tumours.33 Occurs due to involvement of both the cerebellar flocculus and brainstem, especially in cerebellopontine angle tumors such as vestibular schwannoma or meningioma. This type of nystagmus reflects two mechanisms: Gaze-evoked nystagmus due to floccular dysfunction on the side of the lesion (slow pursuit/gaze holding), And vestibular imbalance due to tumor compression of vestibular input, which produces spontaneous nystagmus in the primary gaze. Toward the lesion: coarse, slow-frequency, high-amplitude nystagmus (due to gaze-holding deficit). Away from lesion: finer, faster-frequency nystagmus from vestibular tone imbalance. Pathognomonic for cerebellopontine angle lesions and mandates urgent imaging. Bruns’ nystagmus, a classic sign of cerebellopontine angle tumors such as acoustic neuroma, differs distinctly from stroke-related nystagmus. It is characterized by a dual-component pattern: a coarse, high-amplitude, low-frequency nystagmus when looking toward the side of the lesion (due to vestibular hypofunction), and a fine, high-frequency, low-amplitude nystagmus when looking away (due to central gaze-holding failure). Unlike other central or stroke-related nystagmus, which is typically unidirectional or purely vertical/torsional depending on the lesion site, Bruns’ nystagmus reflects both peripheral vestibular and central cerebellar involvement, providing a unique diagnostic clue for mass lesions compressing both brainstem and cerebellar structures.34
Predominantly Vertical or Torsional Central Vestibular Nystagmus
Downbeat Nystagmus
Downbeat nystagmus (DBN) is characterised by a pathological upward drift of gaze, followed by a corrective downward saccade. It can be caused by lesions at the foramen magnum, such as Arnold– Chiari malformation and syringobulbia; drugs such as lithium and phenytoin; Wernicke’s encephalopathy; demyelination; and hydrocephalus.35 It is most commonly associated with lesions at the cervicomedullary junction, particularly involving the flocculus and paraflocculus of the cerebellum, which are responsible for stabilizing vertical gaze by inhibiting excessive activity from the anterior semicircular canals. When these inhibitory cerebellar structures are damaged—such as in Arnold–Chiari malformation, syringobulbia, or Wernicke’s encephalopathy—there is unopposed excitatory input to upward gaze pathways, producing DBN. Clinically, DBN is usually most pronounced in primary gaze and downgaze, may increase with convergence or lateral gaze, and is not suppressed by visual fixation, helping to distinguish it from peripheral causes.36
Upbeat Nystagmus
Upbeat nystagmus is characterised by downdrift of the eyes, corrected by a fast upward saccade. Lesions in the brainstem or the anterior cerebellar vermis can cause this type of nystagmus. It is typically linked to lesions in the pontine tegmentum, medial longitudinal fasciculus, or anterior cerebellar vermis, which affect vertical gaze-holding pathways and vestibular projections. Common causes of upbeat nystagmus include demyelinating disease, stroke, tumours, cerebellar degeneration, and tobacco use.37 UBN is generally present in primary gaze and can be gaze-enhanced on upgaze. Like DBN, it is not suppressed by fixation and may be associated with other brainstem signs, such as ataxia or dysarthria. Both types of vertical nystagmus are important localizing signs of central nervous system pathology and warrant prompt neuroimaging.38
Torsional Nystagmus
Nystagmus is predominantly torsional in the primary gaze and often occurs due to medullary and midbrain lesions. Primarily arises from lesions in the medulla (eg, vestibular nuclei) and midbrain (eg, interstitial nucleus of Cajal and rostral interstitial MLF), which are integral in controlling torsional gaze. Disruption of the otolithic–ocular pathways cause unbalanced torsional inputs to the ocular motor nuclei, leading to rotation of the eyes around the visual axis.Torsional nystagmus, especially if isolated, suggests brainstem or vestibular nucleus lesions and often coexists with vertical or gaze-evoked components.39
Infantile Nystagmus
Infantile idiopathic nystagmus develops within the first few months of life. It is usually bilateral, conjugate, horizontal, and of either a pendular waveform or jerk waveform with an accelerating slow phase; however, it can also occur as vertical or torsional nystagmus.5 Reflects dysfunction of the cortical–brainstem–ocular motor loop, particularly involving the accessory optic system, superior colliculus, and cerebellum. Defective development of foveal fixation and pursuit results in an oscillatory instability, typically manifesting as bilateral horizontal nystagmus with accelerating slow phases. Often conjugate, improves with convergence, and may show null point phenomenon; it may be idiopathic or associated with albinism, retinal dystrophies, or optic nerve hypoplasia.13
Acquired Pendular Nystagmus
The acquired pendular nystagmus involves slow-phase eye movements in the horizontal, vertical, and torsional planes, resulting in quasi-sinusoidal movement. MS is the most common cause of acquired pendular nystagmus (AN) {Video S2}.40 Involves instability in central gaze-holding structures, notably the nucleus prepositus hypoglossi, medial vestibular nuclei, and interstitial nucleus of Cajal. Impaired integration of eye position signals leads to smooth, sinusoidal oscillations in multiple planes without corrective saccades. Commonly associated with multiple sclerosis, brainstem stroke, or oculopalatal tremor; quasi-sinusoidal waveform differentiates it from jerk nystagmus.41
Oculopalatal Tremor
It is characterized by continuous and rhythmic movements of the soft palate, combined with pendular nystagmus. It occurs after injury to the brainstem or the cerebellar region.42 Results from lesions affecting the Guillain–Mollaret triangle (red nucleus, inferior olive, and dentate nucleus). Denervation hypersensitivity in the inferior olivary nucleus produces rhythmic impulses that are relayed to ocular motor and palatal muscles, causing pendular eye movements and palatal tremor. Occurs months after brainstem stroke, typically in the medullary region; low-frequency vertical or torsional nystagmus is characteristic.42
Oculomasticatory Myorhythmia
It is characterised by smooth, continuous, slow (1–3 hz), pendular, convergent-divergent nystagmus with concurrent contractions of the masticatory muscles and rhythmic movements of the limbs. It has also been observed in Whipple’s disease in the central nervous system. Localized to brainstem and thalamus, involving oculomotor nuclei, mesencephalic trigeminal nucleus, and limbic pathways. Whipple’s disease causes inflammatory infiltration leading to rhythmic central discharges manifesting as slow convergent-divergent eye movements, jaw contractions, and limb jerks. Pathognomonic of CNS Whipple’s disease; should prompt PCR or biopsy confirmation.43
Seesaw Nystagmus
Disconjugate nystagmus in which one half-cycle consists of slow-phase elevation and intorsion of one eye and synchronous depression and extorsion of the other eye.44 The next half-cycle consists of slow or fast phases in the opposite direction. Linked to lesions in the diencephalon, interstitial nucleus of Cajal, and parasellar region, disrupting vertical–torsional gaze integration. Imbalance in otolithic and interocular torsional circuits leads to one eye elevating and intorting while the other depresses and extorts. Often associated with chiasmal or midbrain lesions; may indicate parasellar tumors or craniopharyngioma.13
Epileptic Nystagmus
Nystagmus occurring during epileptic seizure activity is unilateral and horizontal, beating opposite the side of ictal discharge, and preceded by gaze deviation. Most of these occur as focal or generalised tonic-clonic seizures.45 Originates from the parieto-occipital cortex, spreading to frontal eye fields during ictal discharge. Seizure discharges drive contralateral saccadic commands, resulting in involuntary fast eye movements beating away from the epileptogenic focus. Always unilateral and horizontal, accompanied by gaze deviation; diagnosis is confirmed with EEG correlation.46
Pursuit-Paretic Nystagmus
Low-amplitude horizontal jerk nystagmus in response to slow ocular drift due to marked asymmetry of horizontal smooth pursuit resulting from large cerebral hemispheric lesions.47 Caused by large cerebral hemispheric lesions, particularly affecting the parieto-occipital cortex and MT/MST regions involved in smooth pursuit. Marked asymmetry in pursuit causes a slow drift toward the lesioned hemisphere and corrective saccade away, creating a jerk nystagmus.Often seen in unilateral cerebral infarcts, especially in the posterior cerebral artery territory.47
Gaze-Evoked Nystagmus
Jerk nystagmus occurs when the eyes are in an eccentric position and not in the primary gaze, with a fast phase towards the direction of gaze.48 It occurs when the neural integrator, which is normally responsible for gaze holding, is defective and the eye attempts to maintain an extreme gaze. Involves neural integrators like the nucleus prepositus hypoglossi (horizontal) and INC (vertical), which maintain eccentric gaze. If integrators are impaired, the eyes drift back to midline, triggering corrective saccades in the direction of gaze. The most common central nystagmus, often observed in cerebellar disorders, drug toxicity, and MS.49
Triggered Nystagmus
Nystagmus can be triggered by changes in head position, the Valsalva manoeuvre, headshaking, loud sounds, pressure changes, vibrations, or hyperventilation (Figure 3). 50–54 Origin varies based on stimulus type—eg, superior semicircular canal (sound-induced), vestibular nuclei (hyperventilation), or otolith organs (headshake). Stimuli such as Valsalva, sound, or position cause transient activation of hypersensitive vestibular pathways or reveal hidden canal dehiscence. Tullio phenomenon (sound-induced), pressure-triggered, and vibration-triggered forms suggest semicircular canal dehiscence, perilymph fistula, or vestibular paroxysmia. The hyperventilation-induced nystagmus test is used in conditions like vestibular paroxysmia and vestibular schwannoma. Hyperventilation for 30–60 seconds may provoke a burst of nystagmus due to transient changes in axonal excitability caused by alkalosis. In vestibular schwannoma, this test may unmask a latent vestibular imbalance by transiently increasing conduction in partially demyelinated vestibular nerve fibers. Head impulse testing, especially with video head impulse test (vHIT), is used to assess the vestibulo-ocular reflex and detect covert or overt saccades indicative of peripheral vestibular dysfunction. Similarly, vibration-induced nystagmus testing and pressure-induced tests (Valsalva maneuver) can reveal dehiscence syndromes or perilymphatic fistulae.55,56
Based on the nature of the stimulus, triggered nystagmus can be broadly categorized into positional, pressure-induced, sound-induced, vibration-induced, and respiratory-induced forms, each with distinct clinical implications and neuroanatomical localizations.
Positional Nystagmus
This occurs when a change in head or body position elicits the eye movement, typically observed in benign paroxysmal positional vertigo (BPPV). In BPPV, otoliths displaced into the semicircular canals, especially the posterior canal, result in abnormal endolymph flow when the head is moved into specific positions, producing transient torsional and vertical nystagmus. This form is highly position-dependent and usually brief, fatigable, and follows a latency period after the provocative maneuver. The Dix–Hallpike maneuver is a cornerstone for diagnosing benign paroxysmal positional vertigo (BPPV), particularly of the posterior semicircular canal. During this test, the patient is rapidly transitioned from sitting to a supine position with the head turned to one side and extended. A positive result is indicated by a brief latency followed by torsional upbeat nystagmus lasting less than 30 seconds, which fatigues with repetition—hallmarks of canalithiasis.15
Pressure-Induced Nystagmus
This type of nystagmus is seen in conditions where abnormal communication exists between intracranial, middle ear, or inner ear structures. For instance, patients with perilymph fistulas or semicircular canal dehiscence (SCD) may exhibit nystagmus triggered by barometric pressure changes, Valsalva maneuvers, or straining. This type typically presents with direction-fixed horizontal or vertical-torsional nystagmus, reflecting inappropriate activation of vestibular end organs.53
Sound-Induced Nystagmus
This nystagmus also known as the Tullio phenomenon, is another variant most often seen in superior semicircular canal dehiscence. In this condition, high-amplitude sounds stimulate the dehiscent canal, activating the vestibulo-ocular reflex (VOR) and resulting in nystagmus that is direction-specific based on the involved canal. This nystagmus is usually vertical or torsional and may be accompanied by vertigo, oscillopsia, or autophony.53
Vibration-Induced Nystagmus
This is most commonly observed in unilateral vestibular loss. When a vibratory stimulus is applied to the mastoid or sternocleidomastoid, it activates the intact side’s vestibular system asymmetrically, resulting in nystagmus toward the healthy ear. It is used diagnostically to reveal covert vestibular hypofunction in clinical settings.53
Respiratory-Induced Nystagmus,
Although rare, this type of nystagmus can occur during hyperventilation in conditions like vestibular schwannoma or demyelinating disease, where nerve excitability is altered. In such cases, nystagmus may be transient and accompanied by auditory or neurological symptoms.50
By differentiating triggered nystagmus into these well-defined subtypes, clinicians can localize pathology more precisely, guide appropriate imaging, and determine the underlying etiology. Careful history-taking, provocative testing, and observation of the waveform and directionality of nystagmus in relation to the triggering factor are essential for accurate diagnosis and effective management.
Recent studies have provided critical understanding into pathological nystagmus, enhancing our understanding of its diagnostic and therapeutic aspects. Below is a review of notable recent research: A 2021 study by Mantokoudis et al revisited Bruns’ nystagmus as an indicator of stroke in patients presenting with acute vestibular syndrome (AVS). The research utilized video-oculography to assess gaze-evoked nystagmus (GEN) in 47 AVS patients, comprising 35 with vestibular neuritis and 12 with stroke. Findings revealed that one-third of the stroke patients exhibited spontaneous nystagmus in a straight-ahead gaze and pathological GEN, manifesting as Bruns’ nystagmus. The study concluded that automated quantification of GEN could effectively identify stroke-related AVS in emergency settings.57 Gottlieb et al conducted a systematic review in 2023 to evaluate the diagnostic accuracy of the Head Impulse, Nystagmus, Test of Skew (HINTS) examination in identifying central causes of AVS. Analyzing data from 16 studies with 2,024 participants, the review found that the clinical HINTS examination demonstrated a sensitivity of 94.0% and specificity of 86.9% for diagnosing central etiologies. The authors emphasized the importance of clinician training in performing the HINTS examination and called for further research to assess its reliability across different providers and settings.58 The HINTS (Head-Impulse–Nystagmus–Test-of-Skew) exam has emerged as a valuable bedside tool to distinguish between central (often stroke-related) and peripheral causes of acute vestibular syndrome (AVS). When performed correctly by expert clinicians, especially neuro-ophthalmologists or neurotologists, the HINTS battery has demonstrated greater sensitivity than early MRI in detecting posterior circulation strokes. However, despite its utility, the HINTS exam has important limitations that merit clarification—particularly when applied across diverse clinical settings. A key limitation lies in the high degree of examiner skill required for accurate interpretation. The head impulse test (HIT), for instance, demands precise technique and careful observation to detect covert saccades. Inexperienced clinicians may misinterpret normal or subtle findings, reducing the diagnostic accuracy of the test. Similarly, interpreting direction-changing nystagmus or a subtle skew deviation without appropriate training or equipment (like Frenzel goggles or video-oculography) may result in false conclusions. Additionally, the HINTS exam assumes an isolated AVS presentation and may be confounded in patients with baseline nystagmus, poor fixation, or pre-existing neurological deficits. In real-world emergency settings, variable lighting, patient cooperation, and lack of specialized equipment may further compromise test reliability. Moreover, many primary care or emergency physicians are not adequately trained in advanced eye movement assessments, leading to inconsistent test applications and potential diagnostic errors. Therefore, while the HINTS exam is powerful in skilled hands, its routine use should be paired with clinician training, clinical context awareness, and, when possible, adjunctive imaging or tele-neuro-ophthalmology consultation to improve diagnostic accuracy across healthcare settings.57,58
A review by Strupp in 2011 explored current pharmacological treatments for various forms of nystagmus. The study highlighted that baclofen has shown efficacy in improving periodic alternating nystagmus, while gabapentin and memantine have been beneficial for pendular nystagmus. Despite these advancements, the authors noted that many eye movement disorders, such as ocular flutter and see-saw nystagmus, remain challenging to treat, underscoring the need for further research in this area.59 Wagner et al conducted a study in 1990 focusing on the incidence and characteristics of nystagmus in individuals with Down syndrome. Among 188 consecutive patients, 56 exhibited nystagmus, with the majority lacking clinically recognizable ocular pathology to account for it. The study identified various forms of nystagmus, including fine rapid horizontal and dissociated pendular types, suggesting that nystagmus occurs frequently in patients with Down syndrome.60
Nystagmoid Movements
Nystagmoid movements, described as “sheep in wolves’ clothing”, are involuntary movements or saccades that disrupt fixation or have a fast phase followed by a slow phase. In contrast, true nystagmus is initiated during the slow phase.61 They consist of the following types (Figure 4).
 |
Figure 4 Depicts the different types of nystagmoid movements. |
Saccadic Intrusions And Oscillations
They involuntary conjugate saccades that disrupt fixation as compared to the slow drift in true nystagmus.62 Saccadic intrusions can be idiopathic or secondary to neurological conditions such as Parkinson’s disease, multiple sclerosis, and metabolic or toxic aetiologies.
Square-Wave Jerks
They are horizontal conjugate saccades (typically <2°) that interrupt the fixation. It consists of an initial saccade that moves the fovea away from the intended position of fixation, followed by a second saccade in the opposite direction that refoveates the fixation position. Associated with dysfunction of superior colliculus, brainstem omnipause neurons, or cerebellar fastigial nucleus.: Inappropriate release of saccadic commands leads to small horizontal saccades away from and back to fixation. Common in elderly and patients with Parkinson’s disease, multiple sclerosis, or progressive supranuclear palsy. Easily mistaken for nystagmus but lacks rhythmicity and slow-phase drift.63
Macro-Saccadic Oscillations
Oscillations that straddle around a fixation point due to saccadic hypermetria. Typically, due to lesions in the cerebellar fastigial nucleus or cerebellar outflow pathways. Saccadic hypermetria results in overshooting saccades oscillating around a fixation point.Often seen in cerebellar disease, they retain intersaccadic intervals and mimic ocular tremors; however, they are nonrhythmic and not triggered by gaze.62
Saccadic Pulses
These consist of a brief saccade away from the fixation position followed by an immediate recorrecting saccade, and can be differentiated from square-wave jerks by the intersaccadic interval seen in the latter.64 Linked to dysfunction of the neural integrator system, especially the nucleus prepositus hypoglossi and medial vestibular nucleus. Consist of small saccades that fail to hold eccentric gaze, immediately corrected by a return saccade without a pause. This results from instability in gaze-holding circuitry. They differ from square-wave jerks by their lack of intersaccadic interval and are often subtle. May occur in cerebellar degeneration and brainstem disorders affecting gaze stability.64
Ocular Flutter
This consists of intermittent bursts of conjugate horizontal saccades without an intersaccadic interval and is induced by blinking or voluntary eye movements. Reflects dysfunction in saccade-generating brainstem circuits, especially the pontine paramedian reticular formation (PPRF) and cerebellar fastigial nucleus. Characterized by bursts of horizontal, conjugate saccades in rapid succession without an intersaccadic pause, often triggered by blinking or attempted fixation.Seen in paraneoplastic syndromes, viral encephalitis, and toxic/metabolic states. It is pathologic and often coexists with cerebellar signs. Unlike opsoclonus, flutter is limited to the horizontal plane.65
Opsoclonus
Combined conjugate multidirectional saccadic oscillations without an intersaccadic interval that can disrupt steady fixation. Involves widespread dysfunction in brainstem omnipause neurons, PPRF, and cerebellum, leading to loss of saccadic inhibition. Presents as spontaneous, chaotic, high-frequency multidirectional saccades without an intersaccadic interval, disrupting fixation in all planes. A hallmark of paraneoplastic opsoclonus-myoclonus syndrome (OMS) (eg, neuroblastoma in children), but also occurs in viral encephalitis and toxic encephalopathy. Often associated with ataxia and myoclonus, it requires neuroimaging and CSF evaluation.66
Voluntary Saccadic Oscillations
Normal subjects can voluntarily induce conjugate high-frequency saccadic oscillations, which are usually horizontal and have characteristics similar to opsoclonus and ocular flutter. Originate in cortical eye fields under voluntary control.Some individuals can voluntarily produce high-frequency saccadic oscillations, typically horizontal, mimicking ocular flutter or opsoclonus. Distinguished by patient awareness and volitional control; no associated neurological deficits. Often seen in young individuals with high visual attention or as a trick response during examination.64
Tailor et al in their study investigated how involuntary eye movements in individuals with idiopathic infantile nystagmus syndrome (IINS) affect visual crowding—a phenomenon where objects that are easily recognized in isolation become difficult to identify when surrounded by other stimuli. The researchers found that the horizontal oscillations characteristic of IINS exacerbate crowding effects, leading to decreased visual acuity and function. The study suggests that these visual impairments are primarily driven by the eye movements themselves rather than long-term neural changes.67 Lalanne et al introduced a novel method for analyzing nystagmus waveforms using eye-tracking data. The proposed approach employs convolutional sparse coding to automatically identify and separate pathological eye movements from natural ones. The method aims to improve the accuracy of nystagmus analysis, which is crucial for clinical interpretation and diagnosis.68 The literature review by Musat et al, focused on the evaluation of ocular movements, particularly nystagmus, in the context of peripheral vestibular disorders. The authors discuss various types of nystagmus associated with conditions such as benign paroxysmal positional vertigo (BPPV), vestibular neuritis, and Meniere’s disease. The review underscores the diagnostic value of detailed ocular examinations and proposes an algorithm to aid clinicians in distinguishing between peripheral and central causes of vertigo and imbalance.69 These studies contribute to the evolving understanding of nystagmoid movements, offering insights into their impact on visual function, advancements in diagnostic methodologies, and the importance of thorough clinical evaluations.
Other Nystagmoid Movements
Brainstem-Related Movements
Convergence-Retraction Nystagmus
It is characterised by irregular oscillatory movements of the eyes, particularly with gaze and saccades in the upward direction. Involuntary convergence and globe retraction were observed during upgaze (Video S3). It is commonly associated with dorsal midbrain lesions and is a component of Parinaud syndrome.70,71 Man and Fu (2014) reported on a 49-year-old woman who presented with sudden onset of binocular diplopia and unsteady gait. Clinical examination demonstrated convergence-retraction nystagmus on upgaze, see-saw nystagmus on left gaze, and ocular tilt reaction with skew deviation. MRI revealed a right thalamo mesencephalic infarct. The authors discussed that CRN in such patients might result from damage to supranuclear fibers that inhibit convergence neurons or ischemia affecting divergence neurons in the midbrain, leading to sustained medial rectus muscle activity.72
Ocular Bobbing
Abrupt, spontaneous downward jerks of the eyes with a slow return to the mid-position, is associated with paralysis of spontaneous and reflex horizontal eye movements.73 Ocular bobbing is a vertical nystagmoid movement characterized by rapid downward eye jerks followed by slow upward drifts and is typically associated with lesions in the ventral pons. Damage to pontine structures such as the paramedian pontine reticular formation (PPRF) and omnipause neurons disrupts saccadic inhibition, allowing uncontrolled vertical saccades. The interconnections between the pons and midbrain vertical gaze centers—like the rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF)—are also affected, impairing vertical gaze control. Additionally, dysfunction in cerebellar modulation, particularly from the fastigial nucleus, may contribute to the imbalance between the fast and slow eye movements, resulting in the classic ocular bobbing pattern.73 A notable study by Chang et al, provided detailed insights into this phenomenon. The authors reported on a patient who developed ocular bobbing following a pontine hemorrhage. Detailed eye movement analyses revealed pendular oscillations accompanying the ocular bobbing, suggesting a complex interplay between different neural mechanisms in the brainstem. The study emphasizes the importance of comprehensive eye movement recordings in understanding the pathophysiology of ocular bobbing and its variants.74 Ocular bobbing is a vertical eye movement disorder often observed in comatose patients, but it manifests in different variants with distinct clinical implications. Classic ocular bobbing consists of a rapid downward jerk followed by a slow upward drift and is typically associated with structural lesions in the pons, such as infarctions or hemorrhages, reflecting damage to vertical saccadic pathways and gaze-holding centers. In contrast, inverse ocular bobbing features a rapid upward jerk followed by a slow downward drift and is more commonly seen in metabolic encephalopathies like hepatic or uremic encephalopathy, indicating diffuse cortical dysfunction rather than a focal brainstem lesion. Another related phenomenon, ocular dipping, shows a slow downward movement followed by a brisk upward correction and is frequently associated with hypoxic-ischemic brain injury, suggesting depressed cortical function with relatively preserved brainstem reflexes. Rarely, reverse ocular dipping, characterized by slow upward drift followed by a fast downward jerk, may occur in severe metabolic or cerebellar disorders. While classic ocular bobbing points toward irreversible brainstem pathology, the other variants, particularly in metabolic encephalopathies, may be transient and reversible, highlighting the importance of clinical context and neurological localization in patient management.73
Ping-Pong Gaze (PPG)
Conjugate smooth rhythmic horizontal deviations of the eyes between the two extreme positions, seen most commonly in comatose patients with severe bilateral hemispheric dysfunction.75,76 Yang et al reviewed valuable insights into PPG. The study analyzed 14 consecutive patients diagnosed with PPG at Shanghai General Hospital between February 2016 and March 2018. The median age of the patients was 60 years, with a predominance of males (12 out of 14). The cycle duration of PPG ranged from 1.5 to 6.5 seconds. The leading etiologies identified were acute ischemic stroke (5 patients), post-seizure state (3 patients), and hypoxic-ischemic encephalopathy (2 patients). Notably, 88.9% of patients exhibiting consistent whole-field PPG had similar bilateral hemispheric damage, whereas 80% of those with hemifield PPG had unilateral or markedly asymmetric bilateral hemispheric damage. The study concluded that PPG is indicative of hemispheric damage and that asymmetric PPG may assist in predicting the lateralization of lesions. The clinical outcomes varied, with seven patients achieving neurological remission, one entering a vegetative state, and six succumbing to their conditions.77
Myokymia and Tremor-Like Movements
Superior Oblique Myokymia
Monocular, high-frequency, low-amplitude, torsional, involuntary contractions of the superior oblique muscle that result in oscillopsia and diplopia.73 It has been reported in cases of brainstem tumours, head trauma, cerebellopontine angle lesions, and multiple sclerosis (MS).78 Noro et al, provided insights into the surgical management of SOM. The authors reported on two patients who underwent microvascular decompression (MVD) via the lateral supracerebellar infratentorial approach. Both patients experienced immediate and complete resolution of symptoms postoperatively, with no recurrence observed during follow-ups at 24 and 17 months, respectively. The study underscores the importance of considering MVD as a definitive treatment for SOM, especially when conservative therapies are ineffective.79
Pendular Pseudo-Nystagmus
Pendular ocular oscillations arising from a combination of head tremors and vestibular hypofunction.77 Bronstein et al described three patients with pendular pseudo-nystagmus characterized by oscillopsia, head tremor, and absent vestibulo-ocular reflex (VOR). Symptoms worsened with reading, concentration, and head movements, but rigid head immobilization abolished retinal oscillations. Eye movement recordings showed compensatory motion to head tremor but with phase error, unlike normal VOR. The findings suggest that head tremor-induced oscillopsia in the absence of VOR can mimic brainstem disease, highlighting the importance of recognizing this condition.80
Reflex Disorders
Vestibulo-Ocular Reflex (VOR)
Reflex movement of the eye that keeps the visual image stable on the retina during brief high-frequency head rotation.18 Morrow and Young studied the importance of the vestibulo-ocular reflex (VOR) in assessing brainstem function in comatose patients. The authors reviewed three cases where VOR was initially absent due to sedative use (opioids, benzodiazepines) but later recovered within 24 hours after discontinuation of sedation. Despite absent OCR and OVR responses, other brainstem functions remained intact, suggesting a transient drug-induced effect. Clinicians should consider sedative medications as a reversible cause of absent VOR during neurological evaluations.81
Based on Electronystagmography
It measures corneal-retinal potential variation during ocular movements via electrodes placed above and below the eye to record electrical activity. This is discussed in detail in the following sections.
There are four different types of waveforms of nystagmus80
- Pendular nystagmus was characterised by sinusoidal oscillation without a fast phase (Figure 5A)

Figure 5 Depicts the different waveforms of nystagmus on electronystagmography. (A) Pendular nystagmus. (B) Sawtooth nystagmus. (C) Accelerating velocity exponential slow phase nystagmus. (D) Decelerating velocity exponential slow phase nystagmus.
- Sawtooth nystagmus, with linear velocity slow phase (Figure 5B)
- Accelerating velocity exponential slow phase nystagmus (Figure 5C)
- Decelerating velocity exponential slow phase nystagmus (Figure 5D)

The classification of nystagmus waveforms can be expanded beyond traditional linear and pendular types to include elliptical, circular, and oblique waveforms, particularly in complex cases seen with acquired or central nystagmus. Elliptical waveforms feature rotational movements in an elliptical path, often observed in conditions like oculopalatal tremor, where combined torsional and vertical oscillations occur. Circular waveforms describe continuous eye movements in a full circular trajectory, typically noted in patients with severe brainstem or cerebellar involvement. Oblique waveforms, which combine horizontal and vertical components at non-orthogonal angles, are often seen in central vestibular disorders and can suggest disrupted vertical-torsional gaze integration pathways. Recognizing these atypical patterns is critical for localizing pathology and refining diagnostic accuracy in neuro-ophthalmologic practice.80
Clinical significance of each nystagmus waveform in diagnosing specific conditions:
Pendular Waveform
Characterized by sinusoidal, smooth oscillations without a distinct fast or slow phase. Seen in infantile nystagmus syndrome, multiple sclerosis, or oculopalatal tremor. Suggests central pathology, particularly involving the paramedian tracts or Guillain-Mollaret triangle.40
Jerk Waveform
Features a slow drift followed by a corrective fast phase. It is typical of vestibular nystagmus, and the direction of the fast phase helps localize the lesion. For example, peripheral vestibular lesions (labyrinthine or vestibular nerve) produce unidirectional horizontal jerk nystagmus, suppressed by fixation and enhanced with gaze in the direction of the fast phase (Alexander’s law).63
Accelerating Slow Phase (Jerk Nystagmus)
This waveform is characteristic of infantile idiopathic nystagmus, often associated with sensory visual deficits or foveal hypoplasia. Its presence may suggest early-onset, benign conditions.15
Decelerating Slow Phase
Typically seen in vestibular nystagmus. A sudden deceleration before the corrective fast phase indicates acute vestibular imbalance, helping to distinguish from congenital patterns.15
Elliptical Waveform
Suggests complex torsional and vertical involvement, often seen in oculopalatal tremor or seesaw nystagmus, and helps localize lesions to the interstitial nucleus of Cajal or midbrain tegmentum.45
Circular Waveform
Indicates severe central integration dysfunction, often in advanced brainstem pathology. It suggests disinhibition of omnipause neurons or aberrant vestibulo-ocular reflex loop activity.13
Oblique Waveform
Common in central disorders where both horizontal and vertical pathways are involved, such as in stroke, tumors, or multiple sclerosis. It aids in identifying brainstem-cerebellar axis involvement.15
Recognizing these waveform types and their associated neuroanatomical correlates is essential for accurate localization and etiology identification in patients with nystagmus, guiding both imaging and treatment strategies.
Based on Pathogenesis
Based on the underlying pathogenetic mechanism, nystagmus can be classified as:-
- Physiological
- Infantile or congenital
- Acquired nystagmus.
Physiological Nystagmus
Involuntary oscillations of the eyes that occur due to self-rotation to maintain steady images of the retina and enable clear vision are known as physiological nystagmus.82 These are of two types: optokinetic and vestibular nystagmus.83,84 Rucker discussed recent advancements in nystagmus and saccadic intrusions, emphasizing their diagnostic differentiation and treatment. Key findings include improved understanding of underlying mechanisms, recognition of provocative maneuvers that unmask nystagmus, and differences in acquired pendular nystagmus between demyelinating disease and oculopalatal myoclonus. The study also highlights new pharmacologic treatments, such as memantine for acquired pendular nystagmus and 4-aminopyridine for downbeat nystagmus. Accurate diagnosis through detailed examination techniques is essential for effective management of visual impairment.85
Optokinetic nystagmus is an involuntary, conjugate, and jerky movement of the eye with a moving target in the visual field. They are primarily of amplitude–3-4° and frequency–2-3 hz (Video S1). Knapp et al delved into the symmetry of OKN, particularly focusing on vertical OKN. The study found that while horizontal OKN is generally symmetrical in healthy adults, vertical OKN exhibits asymmetry, with a preference for upward motion. The authors emphasized that factors such as target size, shape, contrast, and velocity can influence OKN gains. This review enhances the understanding of OKN’s underlying mechanisms and its clinical implications.86
Vestibular nystagmus is observed when self-rotation is present even in darkness because of the motion detectors present in the inner ear labyrinth. They are unilateral conjugate, horizontal, oblique, or torsional movements of the eyes observed upon irrigating the ears with cold or warm water. Musat et al reviewed nystagmus in peripheral vestibular disorders to improve diagnostic accuracy by distinguishing peripheral from central causes of vertigo and imbalance. A PubMed search identified 52 relevant articles, discussing nystagmus classifications, diagnostic techniques like video/electro-oculography, and their relevance in BPPV, vestibular neuritis, and Meniere’s disease. The study proposes an algorithm for better clinical diagnosis and highlights the importance of ocular movement evaluation in vestibular disorders. It emphasizes the need for continued research to enhance understanding and patient outcomes in vestibular medicine.69
Childhood Nystagmus
Childhood nystagmus can be caused by ocular pathologies, primary neurological abnormalities, or isolated oculomotor disorders. Table 1 summarises various types of childhood nystagmus and their salient features. The exact pathogenesis of infantile nystagmus is not yet fully understood. Many theories have been proposed, but none have been able to explain its development in a system with intact saccades, pursuits, and VOR.87 Table 2 enlist the differences between true Nystagmus and Nystagmoid movements.
 |
Table 1 Classification of Different Types of Childhood Nystagmus |
 |
Table 2 Depicts the Comparison of Nystagmoid Movements with True Nystagmus |
Acquired Nystagmus83
Three major mechanisms act together to maintain a stable gaze position - Visual fixation VOR. Mechanism that holds the eyes at an eccentric eye position90. Any disturbance in this mechanism results in acquired nystagmus (Table 3).
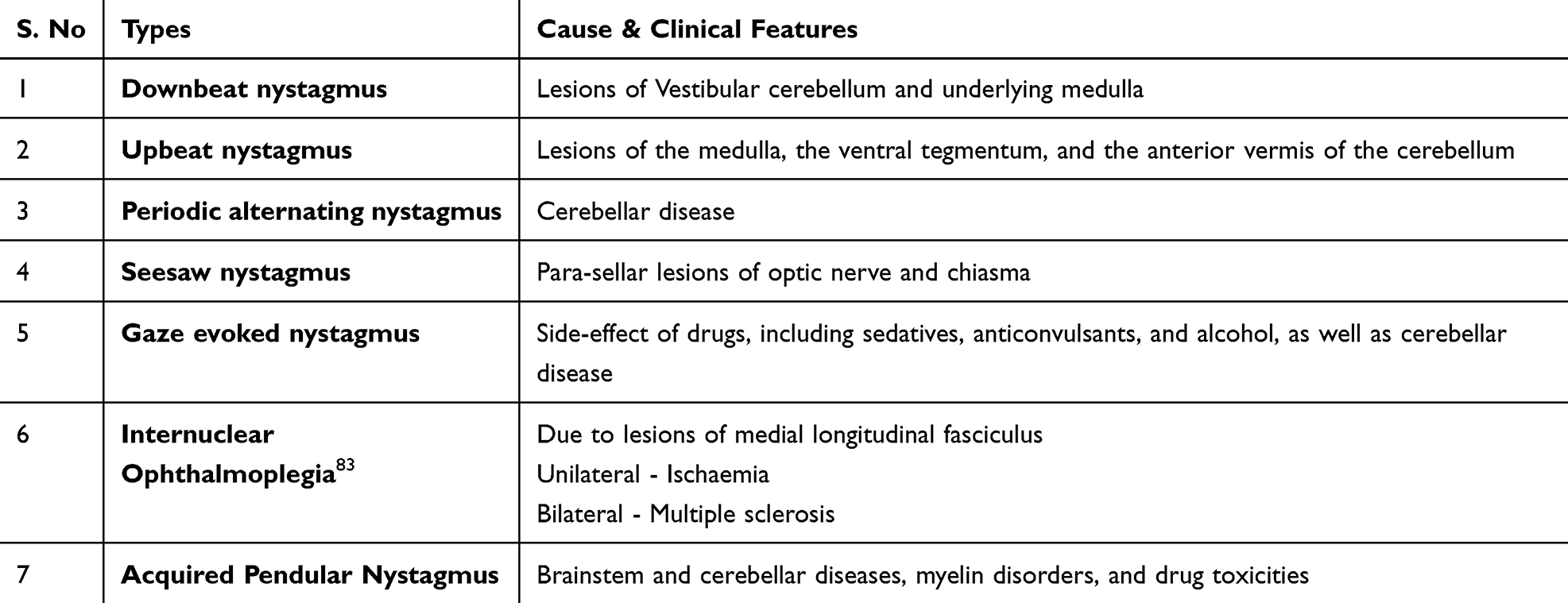 |
Table 3 Different Types of Acquired Nystagmus |
Clinical Assessment and Diagnostic Workflow
Efforts to classify nystagmus may fall short in clinical practice as one condition can result in various types of nystagmus. Comprehensive and targeted evaluation is essential for accurate diagnosis of the underlying cause. The single best and most important step in diagnosis is the clinical examination
A patient with nystagmus must first be examined in the primary gaze, followed by the observation of eye movements in cardinal gazes. The following characteristics should be assessed:17
- Binocularity: can be monocular or binocular
- Conjugacy: Can be conjugate (both eyes rotate simultaneously in the same direction by the same amount) or disconjugate (they do not rotate in the same direction). Disconjugate may be further dissociated if the velocity or amplitude of the movements is different in the two eyes, or disjunctive if the two eyes simultaneously rotate in different directions.
- Direction of movement: horizontal, vertical, torsional or mixed.
- Velocity: Quantitative measurement of the slow-phase movement in degrees per second.
- Waveform: oscillatory appearance of nystagmus on an oculographic trace. Jerky (constant, decreasing, or increasing velocity waveform) or pendular (horizontal, vertical, diagonal, elliptical, circular, convergent, divergent, or seesaw).
- Frequency: Measuring beats per second or Hz (hertz)
- Amplitude: Magnitude in degrees of each beat, that is, the amount of excursion of the globe with each phase.
- Intensity: Qualitative measurement of the product of amplitude and frequency
- Temporal profile: Continuous, intermittent or changing
- Presence of null point: The direction of gaze or distance of fixation at which nystagmus is minimal or nil
- Age at presentation: congenital or infantile if present from birth until six months or acquired if it develops after six months or later.
- Gaze positions: Contributes to nystagmus, including trajectory
- Vergence: may have convergence – divergence component.
- Effect of provocative manoeuvres: changes in position, sound, Valsalva, headshaking, vibration, and hyperventilation.
The following approaches are used to categorise nystagmus into various types and streamline the diagnostic process based on clinical findings and patient history:
Neurologic Causes (Neurologic Group):3
Assess the patient’s birth and family history as well as their growth and development. If no relevant family history or signs of neurological issues were present, brain magnetic resonance imaging (MRI) as the initial test.
Vision/Ocular Related Causes (Ocular Group)3
In the absence of relevant family history and no neurological signs, a complete paediatric ocular examination was conducted. The findings of the eye examination were used to guide further testing, prioritizing the most likely tests. If vision is severely impaired with high hyperopia, molecular genetic testing for Leber congenital amaurosis (LCA) is the first step. The presence of iris transillumination defects may warrant macular optical coherence tomography (OCT) or molecular genetic testing for albinism, especially if there is a history of easy bruising and bleeding or if the family seeks information for family planning. Handheld OCT is a valuable tool, especially for young infants who can be tested while awake or for toddlers under anaesthesia.91 Evaluate pupil shape and consider PAX6 testing if the pupil appears ectopic or oval. If no specific findings guide testing, consider initiating an electroretinogram (ERG) as the initial test, which can help differentiate between genetic retinal dystrophies and other causes (neurological, anatomical, and motor). This group is also called the “Sensory group”.92
Oculomotor/ Eye Movement Disorder Causes (Motor Group)3
Examine eye movement patterns and nystagmus characteristics. Identify any unusual eye movements, including saccadic intrusions or oscillations. Diagnoses were based on specific characteristics and patterns observed, and further evaluation was considered necessary. Primarily a diagnosis of exclusion.93
Diagnostic Workup
Table 4 presents a comprehensive approach towards the basic assessment and investigative workup of suspected nystagmus cases.
 |
Table 4 Diagnostic Work up of Nystagmus. It Summarizes the Various Steps and the Actions That Should Be Taken by the Examiner |
Clinical Evaluation and Investigations
Infantile Nystagmus Syndrome
It is essential to broaden the differential diagnosis to include ocular, neurological, and syndromic causes when evaluating infants or young children with nystagmus. Thorough clinical examination, including age of onset, direction, frequency, amplitude, conjugation, and eye movement recordings, is essential. It is important to rule out potential causes such as corneal dystrophies, cataracts, aniridia, or congenital glaucoma. Important findings, such as anomalous head posture (AHP), head nodding, and general physical examination findings, including skin pigmentation and adnexa, are necessary to rule out syndromic causes. A paradoxical pupillary reaction suggests retinal pathology. Infantile nystagmus syndrome (INS) presents with characteristic clinical features such as oscillation (can be pendular or jerk) occurring in the horizontal plane and remaining horizontal in the up-gaze. Vertical and rotatory oscillations were less common. The INS worsens distance fixation and dampens convergence. The null zone is a common finding in which the patient adopts AHP if it is out of the primary position.3,5,92,93 Lee et al, discussed the advancements in handheld spectral-domain OCT (HH-SDOCT) for pediatric ophthalmology, enabling detailed retinal and optic nerve imaging previously unavailable for children. HH-SDOCT aids in diagnosing infantile nystagmus syndrome, retinal dystrophies, and optic nerve disorders, as well as monitoring retinopathy of prematurity, intraocular tumors, and glaucoma. The study emphasizes that pediatric OCT imaging requires adjustments for shorter axial lengths and ongoing retinal development. Importantly, early OCT-based findings in achromatopsia and albinism suggest potential benefits of early treatment intervention to optimize visual outcomes.94
Acquired Nystagmus
It is important to assess neurological symptoms, such as oscillopsia, along with the clinical history. Movement of the eyes in neurological nystagmus is essential to suspect a diagnosis and proceed with appropriate investigation. Imaging is essential, and further referral to a neurologist, neurosurgeon, or neuro oncology may be necessary.
Spasmus Nutans Syndrome
It typically presents as acquired nystagmus during infancy. Nystagmus associated with SNS is intermittent, with a small amplitude, high frequency, and variable or dissociated patterns. Patients may exhibit variable torticollis (head tilt), head shaking, or bobbing movements. Fundus examination often reveals a normal appearance. Generally, affected individuals have good vision, and over time, nystagmus tends to improve or resolve. In cases, SNS are diagnosed clinically based on observed symptoms. There is a need for caution regarding the potential association with infantile brain tumours; therefore, MRI is usually recommended to rule out such lesions. The nystagmus pattern seen on SNS, while common in this condition, is not exclusive to it and can also occur in more serious conditions such as diencephalic or optic chiasm tumours. If MRI does not reveal any abnormalities, further ophthalmic assessment is recommended.95 Notably, in some cases, patients initially diagnosed with SNS may have negative electroretinography (ERG) results, leading to alternative diagnoses, such as Congenital Stationary Night Blindness (CSNB).96 CSNB, which can mimic SNS, may not always present with night blindness and may have diverse genetic manifestations. Given the potential overlap between SNS and retinal diseases,97,98 it is essential to rule out retinal conditions before confirming SNS diagnosis.
Fusion Maldevelopment Syndrome (FMS)
Latent Nystagmus (LN) / manifest latent nystagmus (LMN) is currently categorised as Fusion Maldevelopment Syndrome (FMS). These are two distinct forms of nystagmus with unique characteristics. LN typically remains concealed when both eyes are open and becomes evident only when one eye is covered and the uncovered eye fixates on an object. It often manifests as predominantly horizontal jerk-type nystagmus, with the fast phase beating away from the covered eye. In contrast, the MLN is observable even when both eyes are open, although it may be of lower intensity and potentially subclinical. The MLN also presents as horizontal jerk nystagmus, but the direction of the fast phase is towards the fixing or open eye. MLN are often associated with various conditions including congenital squint syndrome, Down syndrome, cataracts, optic nerve hypoplasia, and complex nystagmus waveforms, setting them apart from LN in terms of their broader clinical associations.92,99,100
Cerebellar Nystagmus
Cerebellar causes often produce downbeat, upbeat, gaze-evoked, seesaw, or periodic alternating nystagmus (PAN), reflecting involvement of the flocculus, nodulus, or anterior vermis. These types of nystagmus may be vertical, horizontal, or torsional and often lack suppression with visual fixation. Downbeat nystagmus is particularly linked to lesions near the foramen magnum, such as in Arnold–Chiari malformation, and can also occur with phenytoin toxicity or Wernicke’s encephalopathy. PAN is classically seen in cerebellar ataxias and multiple sclerosis. These nystagmus types often coexist with truncal ataxia, dysmetria, and impaired smooth pursuit, helping localize the lesion to cerebellar circuits.50
Brainstem Nystagmus
Brainstem-related nystagmus is generally associated with pathology affecting central gaze-holding and vestibular integration centers. A classic example is Bruns nystagmus, seen in cerebellopontine angle tumors, which shows coarse horizontal movements when gazing toward the lesion and fine fast-frequency nystagmus in primary or contralateral gaze. Other brainstem signs such as cranial nerve palsies or hemiparesis often accompany these nystagmus types. Oculopalatal tremor and oculomasticatory myorhythmia also fall under this category and typically follow delayed degeneration in the Guillain-Mollaret triangle due to brainstem infarcts or neoplasms.1
Drug-Induced or Toxic Nystagmus
Drug-induced nystagmus is most commonly due to central nervous system depressants, anticonvulsants, and lithium. Downbeat nystagmus is frequently observed with chronic phenytoin use, while opsoclonus and ocular flutter may result from intoxication with sedatives or illicit drugs. These involuntary eye movements are typically bilateral and may present acutely or chronically depending on the duration and dosage of exposure. Careful drug history and correlation with serum levels can be critical in diagnosis. Prompt discontinuation or dose adjustment is often effective in managing the symptoms.8
Paraneoplastic Nystagmus
In paraneoplastic syndromes, nystagmus may present as part of opsoclonus-myoclonus or chaotic flutter-like movements. These are typically rapid, multidirectional saccadic intrusions without intersaccadic intervals and are associated with ataxia, tremor, and encephalopathy. Common malignancies include neuroblastoma in children and small-cell lung carcinoma (SCLC) in adults. Serological tests for paraneoplastic antibodies (eg, anti-Ri, anti-Hu) and neuroimaging help confirm the diagnosis. Management involves treatment of the underlying malignancy and immunotherapy to limit immune-mediated neuronal injury.5
Metabolic and Nutritional Nystagmus
Metabolic derangements such as Wernicke’s encephalopathy, hepatic encephalopathy, and electrolyte imbalances can present with pendular or vertical nystagmus. Downbeat nystagmus is particularly linked to thiamine deficiency and should raise suspicion for Wernicke’s encephalopathy in at-risk populations, including chronic alcoholics and patients with malnutrition. Correction of the metabolic derangement often leads to improvement, although nystagmus may persist in chronic cases. Prompt recognition and treatment are essential to prevent irreversible neurological damage.11
Seizure-Related (Epileptic) Nystagmus
Epileptic nystagmus is a rare but important entity characterized by unilateral, horizontal eye movements that occur during focal cortical seizures. These are typically fast and directed away from the epileptogenic focus, often preceded by sustained gaze deviation. Ictal nystagmus is best confirmed with video EEG, and neuroimaging may be needed to identify structural lesions. Antiepileptic therapy remains the mainstay of treatment, with resolution of nystagmus following seizure control.13
Multiple Sclerosis Associated Nystagmus
Patients with multiple sclerosis (MS) frequently exhibit nystagmus due to demyelination of the medial longitudinal fasciculus (MLF), leading to internuclear ophthalmoplegia. Acquired pendular nystagmus is also a common manifestation and may involve horizontal, vertical, and torsional components. These involuntary oscillations are often resistant to fixation suppression and can significantly impair vision. Management may involve gabapentin, memantine, or botulinum toxin in refractory cases.15
Gaze-Evoked Nystagmus (GEN)
It is characterized by involuntary eye movements when looking in specific directions. During the clinical assessment, patients’ eye movements are evaluated by instructing them to fixate on stationary and moving targets and assessing smooth pursuits and saccades. It is typically observed when the gaze shifts towards the direction of nystagmus. This suggests an underlying neurological or vestibular disorder. Differential diagnosis should consider neurological, vestibular, or drug-related causes. Depending on the clinical context, further investigations such as neuroimaging or vestibular testing may be necessary. The GEN assessment is a diagnostic tool that reveals specific anatomical issues. (a) GEN indicates cerebellar disorders, neurodegenerative diseases, or medication-induced effects in all directions (b) Purely horizontal GEN indicates brainstem lesions that affect horizontal gaze-holding. (c) Purely vertical GEN points to midbrain lesions that affect vertical gaze. (d) Dissociated horizontal GEN with adduction deficit indicates internuclear ophthalmoplegia (INO) due to a medial longitudinal fascicle (MLF) defect. (e) GEN with rebound nystagmus is suggestive of cerebellar or flocculus/paraflocculus pathway impairment.101
Vestibular Nystagmus
Assessment of vestibular nystagmus involves clinical history to identify symptoms and triggers, observation of eye movements for direction and intensity, positional testing such as the Dix-Hallpike manoeuvre, evaluation of spontaneous nystagmus, gaze testing in different positions, caloric testing for vestibular function, and video-oculography to precisely record and distinguish between central and peripheral nystagmus patterns. Table 5 highlights the differences between peripheral and central vestibular nystagmus. Various studies have suggested that spontaneous nystagmus with an upward component can manifest as both central and peripheral vestibular disorders. Nevertheless, exclusively upward nystagmus is considered to be a distinctive marker of central vestibular dysfunction.102 Table 6 summarizes the assessment of acquired nystagmus during childhood. Table 7 show the Neurological Associations of Nystagmoid Movements.
 |
Table 5 Differences Between Peripheral and Central Vestibular Nystagmus102 |
 |
Table 6 Summary of Assessment of Acquired Nystagmus in Childhood |
 |
Table 7 Depicts the Neurological Associations of Nystagmoid Movements |
Investigations
The first and foremost step is clinical assessment to establish a diagnosis, followed by paraclinical testing to confirm the diagnosis. The investigations available to aid in diagnosis include electrophysiology, neuroimaging, OCT, and genetic workup.3
Electrophysiology
The ERG is the investigation of choice for suspected retinal dystrophy. Hemispheric VEP, which is less frequently performed, is useful for establishing chiasmal misrouting in albinism, in which iris transillumination defects and typical fundus characteristics are absent.107
Optical Coherence Tomography (OCT)
Optical Coherence Tomography (OCT) is useful for evaluating other causes of foveal hypoplasia and nystagmus, including achromatopsia, PAX-6 mutations, isolated foveal hypoplasia, and FRMD7 mutations. It also helps assess visual prognosis.108
Neuroimaging
The use of Medical Resonance Imaging (MRI) is widespread, particularly for avoiding missing neurological diseases. A few indications for neuroimaging, as summarized by Brodsky,84 include the presence of optic nerve hypoplasia (to exclude septo-optic dysplasia, migration abnormalities, and rarely compressive chiasmal lesions), optic atrophy to rule out hydrocephalus and compressive suprasellar lesions), associated spasmus nutans (to rule out chiasmal gliomas), seesaw nystagmus (to rule out achiasmia), and the presence of neurological signs and symptoms.
Genetic Testing
Genetic workup can detect retinal dystrophies, FRMD7 mutations, and isolated or secondary foveal hypoplasia. The next generation sequencing (NGS) is the most exciting recent advance with the use of nystagmus gene panels. Rim et al showed a 58.3% diagnostic yield for infantile nystagmus using an NGS panel in a South Korean study.109 Another study conducted in the UK reported a molecular detection rate of 80%.110 GNS is likely to be widely available and is the next best investigation to replace the existing tools.
Electronystagmography
Electronystagmography (ENG) is a simple, noninvasive, and commonly used method for recording eye movements. It uses the corneal-retinal potential variation principle to record and interpret the functional properties of the vestibular system, along with the saccadic, pursuit, optokinetic, and fixation visual systems.69 It serves as an important objective tool for the evaluation of nystagmus.87 ENG is an essential adjunct tool to differentiate between the vestibular and ocular causes of nystagmus and hence plays an important role in diagnosis.29 ENG can be very useful for pre- and post-surgical evaluations and can aid in differential diagnosis; however, it is not commonly available in all centres. The ENG does not measure torsional eye movements and is not reliable for eye movements of < 5 °. The vector-ENG is another variant of the ENG which uses three channels to record eye movements and identify horizontal, vertical, and oblique eye movements.111
Videonystagmography
In recent years, videonystagmography (VNG) has slowly replaced ENG, which records eye movements with the help of invisible infrared sensors instead of electrodes in specially made spectacles or masks attached to a computerised system to analyse and display eye movements.112,113 It is possible to record horizontal, vertical, and torsional nystagmus. A few advantages over ENG are that it records the exact direction of eye movements, has no artefacts of muscular origin, and assesses positional nystagmus in cases of benign paroxysmal positional vertigo. VNG readings are more accurate, easier, and faster to perform, although they are more costly. VNG is difficult to perform in children less than five years, in those with ptosis and claustrophobia.111 Both ENG and VNG can be used for treatment strategies, monitoring progression, and planning surgery for vestibular schwannomas and ablations.114 Table 8 depicts the comparison of Diagnostic Modalities for Nystagmus and Eye Movement Disorders.
 |
Table 8 Depicts the Comparison of Diagnostic Modalities for Nystagmus and Eye Movement Disorders |
Bedside Examination (Primary Screening Tools)
Alexander’s Law
Assessed during spontaneous nystagmus. It helps differentiate peripheral from central vestibular lesions by observing that the nystagmus intensity increases when gazing in the direction of the fast phase and decreases when looking in the opposite direction. This is a simple, non-invasive clinical tool best used in bedside evaluation.13,29
Head Impulse Test (HIT)
Evaluates vestibulo-ocular reflex (VOR) integrity. A catch-up saccade after rapid passive head rotation indicates peripheral vestibular hypofunction. It is one of the cornerstones of the HINTS protocol in acute vestibular syndrome and highly useful at the bedside.57,58
Fixation Suppression Testing
Observation of whether spontaneous nystagmus reduces with visual fixation. Peripheral nystagmus is typically suppressed by fixation, whereas central nystagmus persists. This can be evaluated using Frenzel goggles or infrared video goggles if available.17
Observation of Gaze-Evoked Nystagmus
Easily performed at bedside by asking the patient to hold eccentric gaze. Central nystagmus (gaze-evoked) typically lacks a crescendo-decrescendo pattern and may reverse direction with gaze.17
Alternate Cover Test
To check for latent nystagmus in cases of suspected congenital origin.17
Advanced Neuro-Ophthalmic Evaluation (Specialized Testing)
Video-Oculography (VOG)
Allows precise quantification of nystagmus waveform, directionality, and frequency. It helps differentiate between jerk, pendular, and disconjugate eye movements and is critical for evaluating complex presentations like opsoclonus or acquired pendular nystagmus.112
Caloric Testing
Stimulates the horizontal semicircular canals by irrigating the external auditory canal with warm or cold water/air to induce nystagmus. Used in vestibular lab settings to quantify canal paresis.102
Rotational Chair Testing
For evaluating VOR responses at various frequencies, particularly in children or bilateral vestibulopathy cases where caloric responses may be equivocal.1.7
Optokinetic Testing
Assesses smooth pursuit and saccadic responses to moving stimuli. Helps uncover central visual pathway dysfunction.52
Electronystagmography (ENG) / Infrared Videonystagmography (VNG)
Comprehensive vestibular test battery to identify spontaneous, positional, and gaze-evoked nystagmus in objective terms.113
MRI Brain with Contrast
Essential when central signs are suspected, especially in cases with Bruns’ nystagmus, vertical nystagmus, or lack of fixation suppression.39
At the bedside, tools like HIT, Alexander’s Law, fixation suppression, and gaze-holding tests are invaluable in distinguishing peripheral from central causes of nystagmus. Advanced evaluations like video-oculography, caloric testing, and neuroimaging offer detailed insights in complex or inconclusive cases, enabling accurate diagnosis and management.
Treatment
The main goal of treatment is to alleviate the visual symptoms by reducing the speed of the nystagmus slow phase.115 In addition to this, the other aim is to negate the visual consequences of the nystagmus. In addition to visual disturbances, psychological, social, and cosmetic concerns are other reasons why patients with nystagmus seek treatment.4 Various medical, surgical, and optical options are available for treatment. Generally, those that abolish abnormal ocular oscillations while preserving physiological eye movements (saccades, vergence, and vestibulo-ocular reflex) are preferred.116,117 The cause of nystagmus, presence of visual complaints, and the type of nystagmus play a major role in determining the treatment modality.
Medical Treatment
Medical therapy is the mainstay of treatment for the acquired forms of nystagmus. However, long-term therapy is limited by drug-related side effects. Several trials have been conducted to determine the optimal treatment approach for specific types of nystagmus. Table 1 summarizes drug treatments for different forms of nystagmus.
Downbeat Nystagmus
GABAergic Purkinje cells located in the cerebellum regulate vertical smooth-pursuit movements (downward movements more vigorously than upward movements), and damage to these potassium-laden cells is hypothesised to cause downbeat nystagmus (DBN).118,119 GABA receptor agonists have been extensively studied in nystagmus, and Clonazepam, a GABAA receptor agonist, has proven to be useful in suppressing DBN.120,121 However, GABAB receptor agonists, such as Baclofen, have demonstrated inconsistent results, with some studies indicating an increase in the DBN.122,123 Aminopyridines (3,4-diaminopyridine [3,4AP] and 4-aminopyridone [4AP]) are non-selective K+ channel blockers and are considered first-line agents for the treatment of DBN.124 Acting via K+ channels, these drugs stabilise the axonal membranes, increase Purkinje cell excitability, and normalize the irregular firing rate so that the inhibitory influence of the cerebellar cortex on the vestibular and deep cerebellar nuclei is restored, thereby reducing the DBN.125 4AP crosses the blood-brain barrier more effectively than 3,4AP, making it more effective.126,127 However, it is contraindicated in patients with previous seizures and may rarely prolong the QT interval.93 4-AP at a dosage of 5 mg two–four times per day is recommended for the treatment of DBN; the requirement of electrocardiogram both at baseline and about 45 min after taking the drug to exclude QT prolongation is necessary. A sustained-release form of the same drug approved for gait disorders in multiple sclerosis can also be used at a dosage of 10 mg once or twice per day.102 Other drugs evaluated included scopolamine, chlorzoxazone, memantine, and gabapentin.59,128,129
Upbeat Nystagmus
Upbeat nystagmus (UBN) tends to be short-lasting, and treatment is indicated only in persistent cases.116 The pathophysiological hypothesis described here is an imbalance in the vertical vestibulo-ocular reflex tone, as suggested for the DBN. The treatment options include baclofen, memantine and 4AP.122,130,131 However, only moderate success was shown for GABAergic substances, such as baclofen (5–10 mg/3 times a day).122 Glasauer et al showed a reduction in UBN with 10 mg of 4-AP by improving the function of cerebellar pathways.132
Periodic Alternating Nystagmus
Periodic alternating nystagmus (PAN) is a horizontal jerk nystagmus characterised by a reversal in direction every 60–120 seconds and is caused by damage to cerebellar nodules and uvula.133 Baclofen is the first-line drug for the treatment of PAN,134–136 and memantine is used in refractory cases.137
See-Saw Nystagmus
Seesaw nystagmus is a rare form characterised by half-cycles, in which one eye elevates and intorts while the other eye simultaneously depresses and extorts. They can present either pendular or jerk waveforms. The pendular form is observed in patients with pituitary lesions and can be treated with clonazepam,138–140 whereas the jerk form occurs in patients with brainstem lesions and is treated with gabapentin or memantine.112 Benzodiazepines such as diazepam and lorazepam also provide modest benefits.114
Torsional Nystagmus
Torsional nystagmus is a spontaneous jerk-waveform nystagmus in which the eye rotates around the line of sight (LOS). It can persist and cause disabling oscillopathies. Because of its rare nature, very few clinical trials have been conducted to evaluate treatment options. However, one trial reported the suppression of torsional nystagmus with gabapentin.131
Gaze-Evoked Nystagmus
Gaze-evoked nystagmus (GEN) is a jerk-waveform nystagmus that is only evident with attempted eccentric fixation.133 It occurs due to lesions of the cerebellar flocculus, medial vestibular nucleus, and interstitial nucleus of Cajal,114 which results in an inability to hold the eyes in a position of eccentric fixation. Causes include drug intoxication (eg carbamazepine, phenytoin, and alcohol), inherited and acquired cerebellar degeneration, hindbrain anomalies, and Multiple Sclerosis (MS). Most cases of GEN do not produce visual disturbances and hence do not require treatment, although gabapentin has been noted to improve GEN associated with MS.141
Acquired Pendular Nystagmus
This peculiar type of spontaneous pendular waveform nystagmus can have various combinations of horizontal, vertical, and torsional components.116 Most patients with acquired pendular nystagmus (APN) seek treatment for debilitating oscillopsia. Approximately 90% of the APN cases are associated with MS or oculopalatal tremor (OPT).142 As the pathology of the neural integrator is suspected to cause APN due to MS, early studies focused on GABAergic drugs such as clonazepam, isoniazid, and valproate, and found them to be effective in a few patients.143,144 Gabapentin reduces APN by its GABAergic action as well as by binding to calcium channel subunits, and is currently considered the first-choice drug.124,145 For MS patients refractory to gabapentin, memantine 40 mg/day is an effective alternative.131,146,147 Trials comparing baclofen and vigabatrin with gabapentin have confirmed the superiority of gabapentin.124,141 APN due to OPT is generally refractive, although occasionally, patients may respond to gabapentin and memantine.124,141 The pathology of APN caused by OPT involves increased AChE activity in the inferior olivary nucleus.148 Hence, anticholinergic agents, such as trihexyphenidyl149,150 and scopolamine139 have been studied, but they produce only modest effects. Other drugs that demonstrated benefits in selected patients with OPT included isoniazid, clonazepam, and baclofen.142
Infantile Nystagmus Syndrome
It is typically more prominent when the patient fixates on a distant visual target and less prominent when converging on a near target. In many cases, nystagmus is minimised in the null position/null zone. A randomised controlled trial compared the effects of gabapentin and memantine on infantile nystagmus syndrome (INS) and demonstrated an improvement in visual acuity and a decrease in nystagmus intensity with both drugs.151 Oral and topical carbonic anhydrase inhibitors, such as acetazolamide and brinzolamide, have also been reported to be beneficial.152–154
Optical Treatment
The incidence of refractive error in childhood nystagmus is 85%.155 Improvement in visual acuity often suppress infantile and acquired forms of nystagmus; hence, the correction of refractive error is often the first step in the management protocol.156,157 Children should be prescribed full cycloplegic correction and adults should tolerate the highest correction.137 Contact lenses have the advantages of reduced prismatic effects and optical aberrations, and they provide proprioceptive feedback via the trigeminal nerve.158,159 Spectacles with 5–7 prism-diopter base-out prisms can reduce nystagmus in patients with good fusion, by stimulating convergence.160,161 Base-out prisms can also be used for downbeat nystagmus,162 and for patients with nystagmus that worsens during near vision, base-in prisms may prove beneficial.163 Another strategy involves the use of high-convex spectacle lenses combined with high-negative contact lenses.164 The high-plus lenses form a defocused image close to the centre of rotation of the eye, whereas high-minus lenses focus the image back on the retina, thus improving its clarity.107 Employing this optical modality, up to 90% of the visual effects of nystagmus can be negated.165 Pendular nystagmus can be managed using electro-optical devices that measure oscillations of the eye, and motor-driven prisms oscillate the image in step with the nystagmus, thus reducing visual disturbance.166
Surgical Treatment
The goals of nystagmus surgery include shifting the null zone to the primary position, eliminating accommodative head posture (AHP), and improving vision. Based on the two principles of ‘immobilisation’ and ‘relocalisation’ of eyes, these are achieved by either recession, resection, transposition of extraocular muscles or a combination of these procedures. Immobilisation surgery decreases muscle efficiency and dampens nystagmus, whereas relocalization procedures shift the null position to the primary position. Studies have shown that after nystagmus surgery, the null zone broadens, resulting in an improvement in visual acuity.167,168 The earliest surgeries involved treatment of horizontal AHPs to improve nystagmus. Anderson169 proposed recession of the two horizontal muscles that rotated the eyes towards the preferred horizontal gaze. Gotto proposed resection of the two antagonistic muscles and Kestenbaum170 proposed a combined recession of 5 mm on the horizontal muscles in both eyes. Parks171 modified the amount of surgery performed on the medial rectus to 5 mm and 6 mm and on the lateral rectus to 7 mm and 8 mm for recession and resection, respectively (Park’s 5-6-7-8 rule). Pratt-Johnson172 further increased the number of surgeries to 10 mm for all four horizontal muscles. Another surgery, namely the augmented Anderson procedure, involves large recessions on yoke muscles and is useful in most cases with small AHPs,173 whereas for larger AHPs, the Kestenbaum procedure is preferred.
The correction of vertical AHPs and vertical nystagmus involves surgery of the vertical recti and obliques. For chin-up AHPs, recession of the inferior recti and superior obliques in both eyes was advocated by Pierse.174 Later modifications involved recession-resection of the vertical recti of both eyes with sparing of the obliques and horizontal transposition of the vertical recti to correct the A or V patterns.161 For chin-down AHPs, anterior transposition of the inferior obliques175 or recession-resection of the vertical recti of both eyes176 have yielded good results. Torsional nystagmus causes head tilt, and treatment involves rotating the eyes in the direction of the head tilt, which can be achieved by strengthening and weakening the appropriate obliques177 or by horizontal transposition of the vertical recti.178 For AHP in multiple planes, the correction of the most significant results resulted in good improvement.161 Artificial divergence surgery, which involves bi-medial recession, can be performed in patients with strong fusion whose nystagmus dampens with convergence.179 This procedure can be combined with the Anderson-Kestenbaum operation to produce better visual outcomes.180,181 Tenotomy and reattachment involve detachment of the muscles, dissection of the perimuscular fascia, and reattachment of muscles to the same site. This procedure broadens the null zone and has shown mixed results in the treatment of INS,182–185 although one of the major drawbacks is the disruption of extraocular proprioceptive feedback signals.186 Retrobulbar injection of botulinum toxin weakens the extraocular muscles and reduces the intensity of the nystagmus. However, drawbacks include a temporary duration of action and side effects such as loss of physiological eye movements, diplopia, and ptosis. Figure 6 depicts the diagnostic and treatment flowchart of Nystagmus.131
 |
Figure 6 Depicts the diagnostic and treatment flowchart of Nystagmus. |
Recent Advances
As mentioned earlier, nystagmus can occur as an isolated disorder or as a part of an ophthalmic or systemic disorder. This entity has many causes; however, many conditions have overlapping phenotypes. Hence, a proper understanding of genetic causes enables accurate diagnosis and novel targeted therapeutic options. Hypomorphic phenotypes require a structured and methodical investigation pathway, which requires access to equipment and expertise which might not be available in all clinical centres.167 Over recent years, there has been improvement in the understanding of specific conditions which cause nystagmus as part of their phenotype, including oculocutaneous albinism (OCA), aniridia, achromatopsia, and Leber congenital amaurosis (LCA). Gene therapies targeting these underlying conditions may potentially treat the genetic forms of nystagmus associated with these syndromes.187 Tyrosinase enzyme is responsible for the normal retinal pigmentation and development. Nitisinone188 increases ocular melanin by inhibiting 4-hydroxyphenyl pyruvate dioxygenase, and has been approved by the US FDA (Food and Drug Administration) for the treatment of tyrosinemia. Levodopa189 was evaluated for OCA treatment. Levodopa increases postnatal retinal development and visual function. Adeno-associated virus vector (AAV)-mediated gene therapy for RPE65-associated LCA106 is proven to improve functional vision. Subretinal injection of the Voretigene neparvovec-rzyl (Luxturna; Spark Therapeutics) was the first gene therapy approved for the treatment of inherited retinal diseases.187 The central dogma of molecular biology states that protein synthesis occurs in two steps: transcription (in the nucleus of eukaryotes) and translation and production of the polypeptide chain (in the cytoplasm of eukaryotes). Mutations in this pathway lead to disruption and hindrance of protein synthesis. Among all classes of mutations, the nonsense mutation is considered the most dangerous point mutation, with the premature occurrence of stop codons UAG, UGA, and UAA in the mRNA sequence, interpreted as a premature termination codon (PTC), leading to truncated and non-functional proteins. Recently, a breakthrough has materialised in the form of translational readthrough-inducing drugs (TRIDs) to suppress the nonsense codon (NonSups) and allow the nascent peptide chain to elongate, resulting in a full-length protein.190 They basically fool ribosomes during the recognition of PTC as a stop signal, thus avoiding premature termination of protein synthesis.191 TRIDS can affect various targets, resulting in various readthroughs. The various classes of TRIDs are as follows.
- Aminoglycosides192 – gentamicin, tobramycin, ELX-02193
- Oxadiazoles – Fluorinated 1, 2, 4- oxadiazole known as Ataluren or PTC 124194
- Miscallenous - Amlexanox,195 clitosine196
Other strategies explored to suppress nonsense codons include the administration of CRISPR-Cas9 nuclease, which cuts DNA in a sequence-based manner, and the use of anticodon-engineered transfer RNAs (ACE-tRNAs). However, these have not been proven to have significant benefits.197 Another drug, antimalarial quinine, can be used to treat APN by blocking connexin-36.198 A pilot study demonstrated the benefit of real-time computer-based visual feedback in reducing slow-phase movements in a DBN.199 In 2017, Tse et al, reported a case wherein for a patient with nystagmus without a null zone, a titanium T-plate was anchored to the lateral orbital rim and inferior rectus tendon with a suture. The patient had a significant decrease in the amplitude of her nystagmus and oscillopsia, which was sustained after seven years of follow-up.200 In 2022, Chen Y and colleagues, reported two patients who underwent bilateral T-plate placement, which was objectively measured using videonystagmography. Immediate and sustained improvement in nystagmus was observed.201 Recently, implantable magnetic rare-earth prostheses were developed to dampen nystagmus in intractable cases.202 Table 9 depict the treatment guidelines for different types of nystagmus. Recent research on nystagmus has significantly impacted clinical management by refining diagnostic accuracy and guiding targeted interventions. Studies have highlighted the utility of video-oculography and machine learning–based eye movement analysis in distinguishing between central and peripheral causes of nystagmus, improving early detection of conditions such as brainstem infarcts and demyelinating lesions.203 Advances in neuroimaging have correlated specific nystagmus waveforms with anatomical loci, such as upward drift in upbeat nystagmus with anterior vermis lesions. Moreover, research on pharmacologic therapies has identified agents like gabapentin and memantine as effective in treating acquired pendular nystagmus, particularly in multiple sclerosis.204 Rehabilitation-focused studies underscore the role of vision therapy and sensory substitution techniques in managing functional deficits, especially in oscillopsia. These findings collectively enhance diagnostic precision, inform treatment choices, and personalize rehabilitation strategies, ultimately improving visual outcomes and patient quality of life.205
 |
Table 9 Treatment Guidelines for Different Types of Nystagmus |
Recent advances in the understanding and management of various types of nystagmus have significantly enhanced diagnostic precision and therapeutic strategies. For upbeat and downbeat nystagmus, MRI tractography and the use of aminopyridines like 4-AP have improved lesion localization and symptomatic relief by targeting cerebellar and brainstem dysfunction.37,122 Gaze-evoked nystagmus now benefits from high-resolution video-oculography to assess neural integrator integrity, while acquired pendular nystagmus, commonly seen in multiple sclerosis, shows symptomatic improvement with gabapentin and memantine. In infantile nystagmus, ocular motor recordings and emerging gene therapy for FRMD7 mutations hold promise for targeted interventions.26 Seesaw nystagmus has been linked to parasellar lesions via functional imaging, and Bruns nystagmus is increasingly recognized as a diagnostic clue for cerebellopontine tumors. Latent nystagmus and periodic alternating nystagmus are better characterized using infrared oculography and managed with baclofen, respectively. Advances in 3D eye-tracking have improved torsional nystagmus analysis, especially in medullary lesions.44
In rare and complex cases, breakthroughs in neuroimmunology and imaging have elucidated disorders like opsoclonus, ocular flutter, and oculopalatal tremor, often linked with autoimmune or paraneoplastic conditions.66 Triggered nystagmus subtypes—positional (as in BPPV), pressure-induced (Valsalva-related), and sound-induced (Tullio phenomenon)—are now more accurately identified using video-oculography, CT imaging, and canalith repositioning maneuvers. Tools like EEG-fMRI fusion aid in diagnosing epileptic nystagmus, while advanced caloric testing and optokinetic nystagmus platforms enhance vestibular and visual assessments. The use of portable digital devices, serum pharmacokinetics for drug-induced nystagmus, and detailed pursuit testing for pursuit-paretic nystagmus contribute to a more comprehensive, mechanistically-driven classification and management approach across the spectrum of nystagmus disorders.206
Conclusion
Nystagmus represents a complex and multifaceted ocular motor disorder that spans physiological variations, congenital conditions, and a spectrum of acquired neurological pathologies. This comprehensive review underscores the importance of a systematic clinical approach, including detailed history, waveform analysis, and neuroanatomical correlation, to aid accurate diagnosis. The integration of bedside tests—such as the HINTS exam—with advanced technologies like video-oculography, OCT, and MRI enables clinicians to delineate between central and peripheral causes more precisely. Moreover, differentiating true nystagmus from nystagmoid intrusions enhances diagnostic specificity. While some forms of nystagmus remain benign or self-limiting, others signal serious systemic or neurological diseases that require prompt intervention. Emerging advances such as gene therapy, targeted pharmacologic agents (eg, memantine, gabapentin, 4-aminopyridine), and refined electrophysiological techniques are gradually transforming management paradigms. Ultimately, the goal is to not only address the underlying etiology but also improve visual function and quality of life for affected individuals. Ongoing interdisciplinary collaboration, coupled with innovations in neuro-ophthalmic diagnostics and therapeutics, will be crucial in translating evolving research insights into better clinical outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
No external support (public or private) was received for this study.
Disclosure
The authors declare that they have no competing financial interests or personal relationships that could influence the work reported in this study.
References
1. Strupp M, Hüfner K, Sandmann R, et al. Central oculomotor disturbances and nystagmus: a window into the brainstem and cerebellum. Dtsch Arztebl Int. 2011;108(12):197–204.
2. Panthagani J, Virdee J, MacDonald T, Bruynseels A, Batra R. Acquired nystagmus. Br J Hosp Med. 2020;81(11):1–8.
3. Bertsch M, Floyd M, Kehoe T, Pfeifer W, Drack AV. The clinical evaluation of infantile nystagmus: what to do first and why. Ophthalmic Genet. 2017;38(1):22–33.
4. McLean RJ, Windridge KC, Gottlob I. Living with nystagmus: a qualitative study. Br J Ophthalmol. 2012;96(7):981–986.
5. Papageorgiou E, McLean RJ, Gottlob I. Nystagmus in Childhood. Pediatr Neonatol. 2014;55(5):341–351.
6. Sarvananthan N, Surendran M, Roberts EO, et al. The prevalence of nystagmus: the Leicestershire nystagmus survey. Invest Ophthalmol Vis Sci. 2009;50(11):5201–5206.
7. Hvid K, Nissen KR, Bayat A, Roos L, Grønskov K, Kessel L. Prevalence and causes of infantile nystagmus in a large population-based Danish cohort. Acta Ophthalmol. 2020;98(5):506–513.
8. Nash DL, Diehl NN, Mohney BG. Incidence and types of pediatric nystagmus. Am J Ophthalmol. 2017;182:31–34.
9. Ehrt O. Infantile and acquired nystagmus in childhood. Eur J Paediatr Neurol. 2012;16(6):567–572.
10. Abadi RV, Dickinson CM. Monochromatic fundus photography of human albinos. Arch Ophthalmol. 1983;101(11):1706–1711. doi:10.1001/archopht.1983.01040020708008
11. Cogan DG, Chu FC, Reingold D, Barranger J. Ocular motor signs in some metabolic diseases. Arch Ophthalmol. 1981;99(10):1802–1808. doi:10.1001/archopht.1981.03930020676010
12. Dell’Osso LF, Daroff RB. Congenital nystagmus waveforms and foveation strategy. Doc Ophthalmol. 1975;39(1):155–182. doi:10.1007/BF00578761
13. Hoyt CS. Nystagmus and other abnormal ocular movements in children. Pediatr Clin North Am. 1987;34(6):1415–1423.
14. Baloh RW. Pathologic nystagmus: a classification based on electro-oculographic recordings. Bull Los Angeles Neurol Soc. 1976;41(3):120–141.
15. Troost BT. Nystagmus: a clinical review. Rev Neurol. 1989;145(6–7):417–428.
16. Yee RD, Wong EK, Baloh RW, Honrubia V. A study of congenital nystagmus: waveforms. Neurology. 1976;26(4):326–333.
17. Eggers SDZ. Approach to the examination and classification of nystagmus. J Neurol Phys Ther. 2019;43(Suppl 2):S20–S26.
18. Fetter M. Vestibulo-ocular reflex. Dev Ophthalmol. 2007;40:35–51. doi:10.1159/000100348
19. Ichijo H. Three-dimensional analysis of per-rotational nystagmus. Am J Otolaryngol. 2023;44(5):103947.
20. Howard IP, Zacher JE, Allison RS. Post-rotatory nystagmus and turning sensations after active and passive turning. J Vestib Res. 1998;8(4):299–312.
21. Büttner U, Kremmyda O. Smooth pursuit eye movements and optokinetic nystagmus. Dev Ophthalmol. 2007;40:76–89.
22. Munakomi S, Lui F. Caloric reflex test. In: StatPearls. StatPearls Publishing; 2023.
23. Shepard NT, Jacobson GP. The caloric irrigation test. Handb Clin Neurol. 2016;137:119–131.
24. Ward BK, Roberts DC, Della Santina CC, Carey JP, Zee DS. Vestibular stimulation by magnetic fields. Ann NY Acad Sci. 2015;1343(1):69–79.
25. Roberts DC, Marcelli V, Gillen JS, Carey JP, Della Santina CC, Zee DS. MRI magnetic field stimulates rotational sensors of the brain. Curr Biol. 2011;21(19):1635–1640.
26. Ritter MS, Bertolini G, Straumann D, Bögli SY. Prevalence and characteristics of physiological gaze-evoked and rebound nystagmus: implications for testing their pathological counterparts. Front Neurol. 2020;11:547015. doi:10.3389/fneur.2020.547015
27. Ozawa M, Suzuki Y, Nomura T. Stochastic physiological gaze-evoked nystagmus with slow centripetal drift during fixational eye movements at small gaze eccentricities. Front Hum Neurosci. 2022;16:842883. doi:10.3389/fnhum.2022.842883
28. Hotson JR, Baloh RW. Acute vestibular syndrome. N Engl J Med. 1998;339(10):680–685.
29. Baloh RW. Clinical practice. Vestibular neuritis. N Engl J Med. 2003;348(11):1027–1032.
30. Brodsky MC. Visuo-vestibular eye movements: infantile strabismus in 3 dimensions. Arch Ophthalmol. 2005;123(6):837–842.
31. Gresty MA, Metcalfe T, Timms C, Elston J, Lee J, Liu C. Neurology of latent nystagmus. Brain. 1992;115(Pt 5):1303–1321.
32. DiBartolomeo JR, Yee RD. Periodic alternating nystagmus. Otolaryngol Head Neck Surg. 1988;99(6):552–557.
33. Biswas SN, Ray S, Ball S, Chakraborty PP. Bruns nystagmus: an important clinical clue for cerebellopontine angle tumours. BMJ Case Rep. 2018;2018:bcr2017223378,bcr–2017–223378.
34. Venkateswaran R, Gupta R, Swaminathan RP. Bruns nystagmus in cerebellopontine angle tumor. JAMA Neurol. 2013;70(5):646–647.
35. Wagner JN, Glaser M, Brandt T, Strupp M. Downbeat nystagmus: aetiology and comorbidity in 117 patients. J Neurol Neurosurg Psychiatry. 2008;79(6):672–677.
36. Halmagyi GM, Rudge P, Gresty MA, Sanders MD. Downbeating nystagmus. A review of 62 cases. Arch Neurol. 1983;40(13):777–784.
37. Kim JS, Yoon B, Choi KD, Oh SY, Park SH, Kim BK. Upbeat nystagmus: clinicoanatomical correlations in 15 patients. J Clin Neurol. 2006;2(1):58–65.
38. Hirose G, Kawada J, Tsukada K, Yoshioka A, Sharpe JA. Upbeat nystagmus: clinicopathological and pathophysiological considerations. J Neurol Sci. 1991;105(2):159–167.
39. Lopez L, Bronstein AM, Gresty MA, Rudge P, du Boulay EP. Torsional nystagmus. A neuro-otological and MRI study of thirty-five cases. Brain. 1992;115(Pt 4):1107–1124.
40. Kang S, Shaikh AG. Acquired pendular nystagmus. J Neurol Sci. 2017;375:8–17.
41. Gresty MA, Ell JJ, Findley LJ. Acquired pendular nystagmus: its characteristics, localising value and pathophysiology. J Neurol Neurosurg Psychiatry. 1982;45(5):431–439.
42. Borruat FX. Oculopalatal tremor: current concepts and new observations. Curr Opin Neurol. 2013;26(1):67–73. doi:10.1097/WCO.0b013e32835c60e6
43. Schwartz MA, Selhorst JB, Ochs AL, et al. Oculomasticatory myorhythmia: a unique movement disorder occurring in Whipple’s disease. Ann Neurol. 1986;20(6):677–683. doi:10.1002/ana.410200605
44. Nakada T, Kwee IL. Seesaw nystagmus role of visuovestibular interaction in its pathogenesis. J Clin Neuroophthalmol. 1988;8(3):171–177.
45. Kaplan PW, Tusa RJ. Neurophysiologic and clinical correlations of epileptic nystagmus. Neurology. 1993;43(12):2508–2514. doi:10.1212/wnl.43.12.2508
46. Lee SU, Suh HI, Choi JY, Huh K, Kim HJ, Kim JS. Epileptic nystagmus: a case report and systematic review. Epilepsy Behav Case Rep. 2014;2:156–160. doi:10.1016/j.ebcr.2014.08.004
47. Sharpe JA. Neurophysiology and neuroanatomy of smooth pursuit: lesion studies. Brain Cogn. 2008;68(3):241–254. doi:10.1016/j.bandc.2008.08.015
48. Baier B, Dieterich M. Incidence and anatomy of gaze-evoked nystagmus in patients with cerebellar lesions. Neurology. 2011;76(4):361–365. doi:10.1212/WNL.0b013e318208f4c3
49. Lee H, Kim HA. Anatomical structure responsible for direction changing bilateral gaze-evoked nystagmus in patients with unilateral cerebellar infarction. Medicine. 2020;99(17):e19866. doi:10.1097/MD.0000000000019866
50. Cherchi M, Hain TC. Provocative maneuvers for vestibular disorders. Handbook of Clinical Neurophysiology 2010;9(C):111–134. doi:10.1016/S1567-4231(10)09009-X
51. Huh YE, Kim JS. Patterns of spontaneous and head-shaking nystagmus in cerebellar infarction: imaging correlations. Brain. 2011;134(Pt 12):3662–3671. doi:10.1093/brain/awr269
52. Walker MF, Zee DS. Directional abnormalities of vestibular and optokinetic responses in cerebellar disease. Ann NY Acad Sci. 1999;871:205–220. doi:10.1111/j.1749-6632.1999.tb09186.x
53. Minor LB, Solomon D, Zinreich JS, Zee DS. Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg. 1998;124(3):249–258. doi:10.1001/archotol.124.3.249
54. Dumas G, Karkas A, Perrin P, Chahine K, Schmerber S. High-frequency skull vibration-induced nystagmus test in partial vestibular lesions. Otol Neurotol. 2011;32(8):1291–1301. doi:10.1097/MAO.0b013e31822f0b6b
55. Choi KD, Kim JS, Kim HJ, et al. Hyperventilation-induced nystagmus in peripheral vestibulopathy and cerebellopontine angle tumor. Neurology. 2007;69(10):1050–1059. doi:10.1212/01.wnl.0000271378.54381.6a
56. Walker MF, Zee DS. The effect of hyperventilation on downbeat nystagmus in cerebellar disorders. Neurology. 1999;53(7):1576–1579. doi:10.1212/wnl.53.7.1576
57. Mantokoudis G, Korda A, Zee DS, et al. Bruns’ nystagmus revisited: a sign of stroke in patients with the acute vestibular syndrome. Eur J Neurol. 2021;28(9):2971–2979. doi:10.1111/ene.14997
58. Gottlieb M, Peksa GD, Carlson JN. Head impulse, nystagmus, and test of skew examination for diagnosing central causes of acute vestibular syndrome. Cochrane Database Syst Rev. 2023;11(11):CD015089. doi:10.1002/14651858.CD015089.pub2
59. Strupp M, Thurtell MJ, Shaikh AG, Brandt T, Zee DS, Leigh RJ. Pharmacotherapy of vestibular and ocular motor disorders, including nystagmus. J Neurol. 2011;258(7):1207–1222. doi:10.1007/s00415-011-5999-8
60. Wagner RS, Caputo AR, Reynolds RD. Nystagmus in Down’s syndrome. Ophthalmology. 1990;97(11):1439–1444. doi:10.1016/s0161-6420(90)32399-0
61. Lambert J. A Sheep in Wolves’ Clothing? Nystagmoid Eye Movements. Am Orthopt J. 2017;67(1):27–30. doi:10.1080/0065955X.2017.12023628
62. Lemos J, Eggenberger E. Saccadic intrusions: review and update. Curr Opin Neurol. 2013;26(1):59–66. doi:10.1097/WCO.0b013e32835c5e1d
63. Salman MS, Sharpe JA, Lillakas L, Steinbach MJ. Square wave jerks in children and adolescents. Pediatr Neurol. 2008;38(1):16–19. doi:10.1016/j.pediatrneurol.2007.08.011
64. Oh EH, Choi SY, Choi KD, Choi JH. Monocular single saccadic pulses. J Neuroophthalmol. 2019;39(2):237–239. doi:10.1097/WNO.0000000000000740
65. Verhaeghe S, Diallo R, Nyffeler T, Rivaud-Péchoux S, Gaymard B. Unidirectional ocular flutter. J Neurol Neurosurg Psychiatry. 2007;78(7):764–766. doi:10.1136/jnnp.2006.107797
66. Bhatia P, Heim J, Cornejo P, Kane L, Santiago J, Kruer MC. Opsoclonus-myoclonus-ataxia syndrome in children. J Neurol. 2022;269(2):750–757. doi:10.1007/s00415-021-10536-3
67. Tailor VK, Theodorou M, Dahlmann-Noor AH, Dekker TM, Greenwood JA. Eye movements elevate crowding in idiopathic infantile nystagmus syndrome [published correction appears in J Vis. 2022 Jun 1;22(7):2. doi: 10.1167/jov.22.7.2]. J Vis. 2021;21(13):9. doi:10.1167/jov.21.13.9
68. Lalanne C, Rateaux M, Oudre L, Robert MP, Moreau T. Extraction of nystagmus patterns from eye-tracker data with convolutional sparse coding. Annu Int Conf IEEE Eng Med Biol Soc. 2020;2020:928–931. doi:10.1109/EMBC44109.2020.9175621
69. Musat GC, Tataru CP, Musat O, et al. Ocular movement examination in peripheral vestibular disorders as a tool to improve diagnosis: a literature review. Medicina. 2024;60(10):1665. doi:10.3390/medicina60101665
70. Ortiz JF, Eissa-Garces A, Ruxmohan S, et al. Understanding Parinaud’s Syndrome. Brain Sci. 2021;11(11):1469. doi:10.3390/brainsci11111469
71. Rambold H, Kömpf D, Helmchen C. Convergence retraction nystagmus: a disorder of vergence? Ann Neurol. 2001;50(5):677–681. doi:10.1002/ana.1263
72. Man BL, Fu YP. See-saw nystagmus, convergence-retraction nystagmus and contraversive ocular tilt reaction from a paramedian thalamo mesencephalic infarct. BMJ Case Rep. 2014;2014:bcr2014206851. doi:10.1136/bcr-2014-206851
73. Bosch EP, Kennedy SS, Aschenbrener CA. Ocular bobbing: the myth of its localizing value. Neurology. 1975;25(10):949–953. doi:10.1212/wnl.25.10.94
74. Chang TP, Gold DR, Otero-Millan J, Huang BR, Zee DS. Pendular oscillation and ocular bobbing after pontine hemorrhage. Cerebellum. 2021;20(5):734–743. doi:10.1007/s12311-019-01086-6
75. Patel BC, Malhotra R. Superior oblique myokymia. StatPearls. StatPearls Publishing; 2023. Available from: http://www.ncbi.nlm.nih.gov/books/NBK580560/.
76. Ishikawa H, Ishikawa S, Mukuno K. Short-cycle periodic alternating (ping-pong) gaze. Neurology. 1993;43(6):1067–1070. doi:10.1212/wnl.43.6.1067
77. Yang SL, Han X, Guo CN, Zhu XY, Dong Q, Wang Y. A closer look at ping-pong gaze: an observational study and literature review. J Neurol. 2018;265(12):2825–2833. doi:10.1007/s00415-018-9062-x
78. Tandon A, Oliveira C. Superior oblique myokymia, a review. Curr Opin Ophthalmol. 2019;30(6):472–475. doi:10.1097/ICU.0000000000000619
79. Noro S, Seo Y, Honjo K, et al. Lateral supracerebellar infratentorial approach for superior oblique myokymia: a case series. Oper Neurosurg. 2022;22(3):101–105. doi:10.1227/ONS.0000000000000015
80. Bronstein AM, Gresty MA, Mossman SS. Pendular pseudonystagmus arising as a combination of head tremor and vestibular failure. Neurology. 1992;42(8):1527–1531. doi:10.1212/wnl.42.8.1527
81. Morrow SA, Young GB. Selective abolition of the vestibular-ocular reflex by sedative drugs. Neurocrit Care. 2007;6(1):45–48. doi:10.1385/NCC:6:1:45
82. Abadi RV, Bjerre A. Motor and sensory characteristics of infantile nystagmus. Br J Ophthalmol. 2002;86(10):1152–1160. doi:10.1136/bjo.86.10.1152
83. Abadi RV. Mechanisms underlying nystagmus. J R Soc Med. 2002;95(5):231–234. doi:10.1177/014107680209500504
84. Brodsky MC. Nystagmus in Children. In: Brodsky MC editor. Pediatric Neuro-Ophthalmology. Springer; 2010:383–441. doi:10.1007/978-0-387-69069-8_8.
85. Rucker JC. Nystagmus and Saccadic Intrusions. Continuum. 2019;25(5):1376–1400. doi:10.1212/CON.0000000000000772
86. Knapp CM, Proudlock FA, Gottlob I. OKN asymmetry in human subjects: a literature review. Strabismus. 2013;21(1):37–49. doi:10.3109/09273972.2012.762532
87. Dell’Osso LF, van der Steen J, Steinman RM, Collewijn H. Foveation dynamics in congenital nystagmus. II: smooth pursuit. Doc Ophthalmol. 1992;79(1):25–49. doi:10.1007/BF00160131
88. Weissman BM, Dell’Osso LF, Abel LA, Leigh RJ. Spasmus nutans. A quantitative prospective study. Arch Ophthalmol. 1987;105(4):525–528. doi:10.1001/archopht.1987.01060040095041
89. von Noorden GK, Wong SY. Surgical results in nystagmus blockage syndrome. Ophthalmology. 1986;93(8):1028–1031. doi:10.1016/s0161-6420(86)33626-1
90. Dell’Osso LF. Neural integration in ocular motility. Bull Soc Belge Ophtalmol. 1989;237:19–33.
91. Lee H, Sheth V, Bibi M, et al. Potential of handheld optical coherence tomography to determine cause of infantile nystagmus in children by using foveal morphology. Ophthalmology. 2013;120(12):2714–2724. doi:10.1016/j.ophtha.2013.07.018
92. Hertle RW, Maldanado VK, Maybodi M, Yang D. Clinical and ocular motor analysis of the infantile nystagmus syndrome in the first 6 months of life. Br J Ophthalmol. 2002;86(6):670–675. doi:10.1136/bjo.86.6.670
93. Richards MD, Wong A. Infantile nystagmus syndrome: clinical characteristics, current theories of pathogenesis, diagnosis, and management. Can J Ophthalmol. 2015;50(6):400–408. doi:10.1016/j.jcjo.2015.07.010
94. Lee H, Proudlock FA, Gottlob I. pediatric optical coherence tomography in clinical practice-recent progress. Invest Ophthalmol Vis Sci. 2016;57(9):OCT69–OCT79. doi:10.1167/iovs.15-18825
95. Khan AO. Magnetic resonance imaging findings in children with spasmus nutans. J AAPOS. 2017;21(4):345. doi:10.1016/j.jaapos.2017.06.004
96. Smith DE, Fitzgerald K, Stass-Isern M, Cibis GW. Electroretinography is necessary for spasmus nutans diagnosis. Pediatr Neurol. 2000;23(1):33–36. doi:10.1016/s0887-8994(00)00134-x
97. Gottlob I, Helbling A. Nystagmus mimicking spasmus nutans as the presenting sign of Bardet-Biedl syndrome. Am J Ophthalmol. 1999;128(6):770–772. doi:10.1016/s0002-9394(99)00293-7
98. Kiblinger GD, Wallace BS, Hines M, Siatkowski RM. Spasmus nutans-like nystagmus is often associated with underlying ocular, intracranial, or systemic abnormalities. J Neuroophthalmol. 2007;27(2):118–122. doi:10.1097/WNO.0b013e318067b59f
99. Dell’Osso LF, Schmidt D, Daroff RB. Latent, manifest latent, and congenital nystagmus. Arch Ophthalmol. 1979;97(10):1877–1885. doi:10.1001/archopht.1979.01020020325008
100. Zahidi AA, Woodhouse JM, Erichsen JT, Dunn MJ. Infantile nystagmus: an optometrist’s perspective. Clin Optom. 2017;9:123–131. doi:10.2147/OPTO.S126214
101. Strupp M, Kremmyda O, Adamczyk C, et al. Central ocular motor disorders, including gaze palsy and nystagmus. J Neurol. 2014;261(Suppl S2):S542–558. doi:10.1007/s00415-014-7385-9
102. Ling X, Wu Y-X, Feng Y-F, et al. Spontaneous nystagmus with an upbeat component: central or peripheral vestibular disorders? Front Neurol. 2023;14:1106084. doi:10.3389/fneur.2023.1106084
103. Guyton DL, Cheeseman EW, Ellis FJ, Straumann D, Zee DS. Dissociated vertical deviation: an exaggerated normal eye movement used to damp cyclovertical latent nystagmus. Trans Am Ophthalmol Soc. 1998;96:389–424;discussion424–429.
104. Shallo-Hoffmann J, Schwarze H, Simonsz HJ, Mühlendyck H. A reexamination of end-point and rebound nystagmus in normals. Invest Ophthalmol Vis Sci. 1990;31(2):388–392.
105. Luis L, Lehnen N, Muñoz E, et al. Anticompensatory quick eye movements after head impulses: a peripheral vestibular sign in spontaneous nystagmus. J Vestib Res. 2016;25(5–6):267–271. doi:10.3233/VES-160566
106. Nagel-Wolfrum K, Möller F, Penner I, Baasov T, Wolfrum U. Targeting nonsense mutations in diseases with translational read-through-inducing drugs (TRIDs). BioDrugs. 2016;30(2):49–74. doi:10.1007/s40259-016-0157-6
107. Dorey SE. The clinical features of albinism and their correlation with visual evoked potentials. Br J Ophthalmol. 2003;87(6):767–772. doi:10.1136/bjo.87.6.767
108. Thomas MG, Gottlob I. Optical coherence tomography studies provides new insights into diagnosis and prognosis of infantile nystagmus: a review. Strabismus. 2012;20(4):175–180. doi:10.3109/09273972.2012.735336
109. Rim JH, Lee S-T, Gee HY, et al. Accuracy of next-generation sequencing for molecular diagnosis in patients with infantile nystagmus syndrome. JAMA Ophthalmology. 2017;135(12):1376–1385. doi:10.1001/jamaophthalmol.2017.4859
110. Thomas MG, Maconachie GD, Sheth V, McLean RJ, Gottlob I. Development and clinical utility of a novel diagnostic nystagmus gene panel using targeted next-generation sequencing. Eur J Hum Genet. 2017;25(6):725–734. doi:10.1038/ejhg.2017.44
111. Ganança MM, Caovilla HH, Ganança FF. Eletronistagmografia versus videonistagmografia. Braz J Otorhinolaryngol. 2010;76(3):399–403. doi:10.1590/S1808-86942010000300021
112. Claussen C-F, von Schlachta I. Butterfly chart for caloric nystagmus evaluation. Archives of Otolaryngology - Head and Neck Surgery. 1972;96(4):371–375. doi:10.1001/archotol.1972.00770090547015
113. Caovilla HH, Ganança MM, Munhoz MSL, Silva MLG, Ganança FF, Ganança CF. O registro dos movimentos oculares. In: Caovilla HH, Ganança MM, Munhoz MSL, Silva MLG, editors. Equilibriometria Clínica. São Paulo: Atheneu; 1999:31–40.
114. Barin K. Laboratory Vestibular Testing. In:
115. Ehrhardt D, Eggenberger E. Medical treatment of acquired nystagmus. Current Opinion in Ophthalmology. 2012;23(6):510. doi:10.1097/ICU.0b013e328358ba6e
116. Thurtell MJ. Treatment of nystagmus. Semin Neurol. 2015;35(5):522–526. doi:10.1055/s-0035-1563575
117. Thurtell MJ, Leigh RJ. Therapy for nystagmus. J Neuroophthalmol. 2010;30(4):361. doi:10.1097/WNO.0b013e3181e7518f
118. Stone LS, Lisberger SG. Visual responses of Purkinje cells in the cerebellar flocculus during smooth-pursuit eye movements in monkeys. I. Simple spikes. J Neurophysiol. 1990;63(5):1241–1261. doi:10.1152/jn.1990.63.5.1241
119. Pierrot-Deseilligny C, Milea D. Vertical nystagmus: clinical facts and hypotheses. Brain. 2005;128(6):1237–1246. doi:10.1093/brain/awh532
120. Young Y-H, Huang T-W. Role of clonazepam in the treatment of idiopathic downbeat nystagmus. Laryngoscope. 2001;111(8):1490–1493. doi:10.1097/00005537-200108000-00029
121. Currie JN, Matsuo V. The use of clonazepam in the treatment of nystagmus-induced oscillopsia. Ophthalmology. 1986;93(7):924–932. doi:10.1016/s0161-6420(86)33640-6
122. Dieterich M, Straube A, Brandt T, Paulus W, Büttner U. The effects of baclofen and cholinergic drugs on upbeat and downbeat nystagmus. J Neurol Neurosurg Psychiatry. 1991;54(7):627–632. doi:10.1136/jnnp.54.7.627
123. Averbuch‐Heller L, Tusa RJ, Fuhry L, et al. A double-blind controlled study of gabapentin and baclofen as treatment for acquired nystagmus. Ann Neurol. 1997;41(6):818–825. doi:10.1002/ana.410410620
124. Tran TM, Lee MS, McClelland CM. Downbeat nystagmus: a clinical review of diagnosis and management. Curr Opin Ophthalmol. 2021;32(6):504–514. doi:10.1097/ICU.0000000000000802
125. Kalla R, Strupp M. Aminopyridines and acetyl-DL-leucine: new therapies in cerebellar disorders. Curr Neuropharmacol. 2019;17(1):7–13. doi:10.2174/1570159X16666180905093535
126. Claassen J, Spiegel R, Kalla R, et al. A randomised double-blind, cross-over trial of 4-aminopyridine for downbeat nystagmus--effects on slowphase eye velocity, postural stability, locomotion and symptoms. J Neurol Neurosurg Psychiatry. 2013;84(12):1392–1399. doi:10.1136/jnnp-2012-304736
127. Kalla R, Spiegel R, Claassen J, et al. Comparison of 10-mg doses of 4-aminopyridine and 3,4-diaminopyridine for the treatment of downbeat nystagmus. J Neuroophthalmol. 2011;31(4):320–325. doi:10.1097/WNO.0b013e3182258086
128. Feil K, Claaßen J, Bardins S, et al. Effect of chlorzoxazone in patients with downbeat nystagmus: a pilot trial. Neurology. 2013;81(13):1152–1158. doi:10.1212/WNL.0b013e3182a55f6d
129. Barton JJ, Huaman AG, Sharpe JA. Muscarinic antagonists in the treatment of acquired pendular and downbeat nystagmus: a double-blind, randomized trial of three intravenous drugs. Ann Neurol. 1994;35(3):319–325. doi:10.1002/ana.410350312
130. Thurtell MJ, Joshi AC, Leone AC, et al. Crossover trial of gabapentin and memantine as treatment for acquired nystagmus. Ann Neurol. 2010;67(5):676–680. doi:10.1002/ana.21991
131. Glasauer S, Kalla R, Büttner U, Strupp M, Brandt T. 4-aminopyridine restores visual ocular motor function in upbeat nystagmus. J Neurol Neurosurg Psychiatry. 2005;76(3):451–453. doi:10.1136/jnnp.2004.045716
132. Thurtell MJ, Leigh RJ. Nystagmus and saccadic intrusions. Handb Clin Neurol. 2011;102:333–378. doi:10.1016/B978-0-444-52903-9.00019-4
133. Halmagyi GM, Rudge P, Gresty MA, Leigh RJ, Zee DS. Treatment of periodic alternating nystagmus. Ann Neurol. 1980;8(6):609–611. doi:10.1002/ana.410080611
134. Furman JM, Wall C, Pang DL. Vestibular function in periodic alternating nystagmus. Brain. 1990;113(Pt 5):1425–1439. doi:10.1093/brain/113.5.1425
135. Straube A, Leigh RJ, Bronstein A, et al. EFNS task force--therapy of nystagmus and oscillopsia. Eur J Neurol. 2004;11(2):83–89. doi:10.1046/j.1468-1331.2003.00754.x
136. Kumar A, Thomas S, McLean R, et al. Treatment of acquired periodic alternating nystagmus with memantine: a case report. Clin Neuropharmacol. 2009;32(2):109–110. doi:10.1097/WNF.0b013e3181873697
137. Frisén L, Wikkelsø C. Posttraumatic seesaw nystagmus abolished by ethanol ingestion. Neurology. 1986;36(6):841–844. doi:10.1212/wnl.36.6.841
138. Lepore FE. Ethanol-induced resolution of pathologic nystagmus. Neurology. 1987;37(5):887. doi:10.1212/wnl.37.5.887
139. Cochin JP, Hannequin D, Do Marcolino C, Didier T, Augustin P. Intermittent sea-saw nystagmus successfully treated with clonazepam. Rev Neurol. 1995;151(1):60–62.
140. Bandini F, Castello E, Mazzella L, Mancardi GL, Solaro C. Gabapentin but not vigabatrin is effective in the treatment of acquired nystagmus in multiple sclerosis: how valid is the GABAergic hypothesis? J Neurol Neurosurg Psychiatry. 2001;71(1):107–110. doi:10.1136/jnnp.71.1.107
141. Tilikete C, Jasse L, Pelisson D, et al. Acquired pendular nystagmus in multiple sclerosis and oculopalatal tremor. Neurology. 2011;76(19):1650–1657. doi:10.1212/WNL.0b013e318219fa9c
142. Traccis S, Rosati G, Monaco MF, Aiello I, Agnetti V. Successful treatment of acquired pendular elliptical nystagmus in multiple sclerosis with isoniazid and base-out prisms. Neurology. 1990;40(3 Pt 1):492–494. doi:10.1212/wnl.40.3_part_1.492
143. Lefkowitz D, Harpold G. Treatment of ocular myoclonus with valproic acid. Ann Neurol. 1985;17(1):103–104. doi:10.1002/ana.410170123
144. Bauer CS, Nieto-Rostro M, Rahman W, et al. The increased trafficking of the calcium channel subunit alpha2delta-1 to presynaptic terminals in neuropathic pain is inhibited by the alpha2delta ligand pregabalin. J Neurosci. 2009;29(13):4076–4088. doi:10.1523/JNEUROSCI.0356-09.2009
145. Shery T, Proudlock FA, Sarvananthan N, McLean RJ, Gottlob I. The effects of gabapentin and memantine in acquired and congenital nystagmus: a retrospective study. Br J Ophthalmol. 2006;90(7):839–843. doi:10.1136/bjo.2005.086322
146. Starck M, Albrecht H, Pöllmann W, Dieterich M, Straube A. Acquired pendular nystagmus in multiple sclerosis: an examiner-blind cross-over treatment study of memantine and gabapentin. J Neurol. 2010;257(3):322–327. doi:10.1007/s00415-009-5309-x
147. Koeppen AH, Barron KD, Dentinger MP. Olivary hypertrophy: histochemical demonstration of hydrolytic enzymes. Neurology. 1980;30(5):471–480. doi:10.1212/wnl.30.5.471
148. Herishanu Y, Louzoun Z. Trihexyphenidyl treatment of vertical pendular nystagmus. Neurology. 1986;36(1):82–84. doi:10.1212/wnl.36.1.82
149. Jabbari B, Rosenberg M, Scherokman B, Gunderson CH, McBurney JW, McClintock W. Effectiveness of trihexyphenidyl against pendular nystagmus and palatal myoclonus: evidence of cholinergic dysfunction. Mov Disord. 1987;2(2):93–98.
150. McLean R, Proudlock F, Thomas S, Degg C, Gottlob I. Congenital nystagmus: randomized, controlled, double-masked trial of memantine/gabapentin. Ann Neurol. 2007;61(2):130–138. doi:10.1002/ana.21065
151. Hertle RW, Yang D, Adkinson T, Reed M. Topical brinzolamide (Azopt) versus placebo in the treatment of infantile nystagmus syndrome (INS). Br J Ophthalmol. 2015;99(4):471–476. doi:10.1136/bjophthalmol-2014-305915
152. Dell’osso LF, Hertle RW, Leigh RJ, Jacobs JB, King S, Yaniglos S. Effects of topical brinzolamide on infantile nystagmus syndrome waveforms: eyedrops for nystagmus. J Neuroophthalmol. 2011;31(3):228–233. doi:10.1097/WNO.0b013e318223d0a9
153. Thurtell MJ, Dell’osso LF, Leigh RJ, Matta M, Jacobs JB, Tomsak RL. Effects of Acetazolamide on infantile nystagmus syndrome waveforms: comparisons to contact lenses and convergence in a well-studied subject. Open Ophthalmol J. 2010;4:42–51.
154. Hertle RW, Dell’Osso LF. Clinical and ocular motor analysis of congenital nystagmus in infancy. J AAPOS. 1999;3(2):70–79.
155. Anderson J, Lavoie J, Merrill K, King RA, Summers CG. Efficacy of spectacles in persons with albinism. J AAPOS. 2004;8(6):515–520.
156. Hertle RW. Examination and refractive management of patients with nystagmus. Surv Ophthalmol. 2000;45(3):215–222. doi:10.1016/s0039-6257(00)00153-3
157. Allen ED, Davies PD. Role of contact lenses in the management of congenital nystagmus. Br J Ophthalmol. 1983;67(12):834–836. doi:10.1136/bjo.67.12.834
158. Taibbi G, Wang ZI, Dell’Osso LF. Infantile nystagmus syndrome: broadening the high-foveation-quality field with contact lenses. Clin Ophthalmol. 2008;2(3):585–589. doi:10.2147/opth.s2744
159. Serra A, Dell’Osso LF, Jacobs JB, Burnstine RA. Combined gaze-angle and vergence variation in infantile nystagmus: two therapies that improve the high-visual-acuity field and methods to measure it. Invest Ophthalmol Vis Sci. 2006;47(6):2451–2460.
160. Ospina LH. Dealing with Nystagmus. J Binocul Vis Ocul Motil. 2018;68(4):99–109. doi:10.1080/2576117X.2018.1493311
161. Lavin PJ, Traccis S, Dell’Osso LF, Abel LA, Ellenberger C Jr. Downbeat nystagmus with a pseudocycloid waveform: improvement with base-out prisms. Ann Neurol. 1983;13(6):621–624.
162. Averbuch-Heller L, Leigh RJ. Medical treatments for abnormal eye movements: pharmacological, optical and immunological strategies. Aust N Z J Ophthalmol. 1997;25(1):7–13.
163. Rushton D, Cox N. A new optical treatment for oscillopsia. J Neurol Neurosurg Psychiatry. 1987;50(4):411–415. doi:10.1136/jnnp.50.4.411
164. Leigh RJ, Rushton DN, Thurston SE, Hertle RW, Yaniglos SS. Effects of retinal image stabilization in acquired nystagmus due to neurologic disease. Neurology. 1988;38(1):122–127. doi:10.1212/wnl.38.1.122
165. Stahl JS, Lehmkuhle M, Wu K, Burke B, Saghafi D, Pesh-Imam S. Prospects for treating acquired pendular nystagmus with servo-controlled optics. Invest Ophthalmol Vis Sci. 2000;41(5):1084–1090.
166. Dell’Osso LF, Flynn JT. Congenital nystagmus surgery. A quantitative evaluation of the effects. Arch Ophthalmol. 1979;97(3):462–469. doi:10.1001/archopht.1979.01020010212004
167. Flynn JT, Dell’Osso LF. The effects of congenital nystagmus surgery. Ophthalmology. 1979;86(8):1414–1427. doi:10.1016/s0161-6420(79)35379-9
168. Anderson JR. Causes and treatment of congenital eccentric nystagmus. Br J Ophthalmol. 1953;37(5):267–281. doi:10.1136/bjo.37.5.267
169. Kestenbaum A. New operation for nystagmus. Bull Soc Ophtalmol Fr. 1953;6:599–602.
170. Parks MM. Symposium: nystagmus. Congenital nystagmus surgery. Am Orthopt J. 1973;23:35–39.
171. Pratt-Johnson JA. The surgery of congenital nystagmus. Can J Ophthalmol. 1971;6(4):268–272.
172. de Decker W. Kestenbaum transposition in nystagmus therapy. Transposition in horizontal and torsional plane. Bull Soc Belge Ophtalmol. 1987;221-222:107–120.
173. Pierse D. Operation on the vertical muscles in cases of nystagmus. Br J Ophthalmol. 1959;43(4):230–233. doi:10.1136/bjo.43.4.230
174. Roberts EL, Saunders RA, Wilson ME. Surgery for vertical head position in null point nystagmus. J Pediatr Ophthalmol Strabismus. 1996;33(4):219–224. doi:10.3928/0191-3913-19960701-04
175. Lee J. Surgical management of nystagmus. J R Soc Med. 2002;95(5):238–241. doi:10.1177/014107680209500506
176. Fricke J, Neugebauer A, Nobis H, Bartz-Schmidt KU, Rüssmann W. Counterrotation of the globe in macular translocation. Graefes Arch Clin Exp Ophthalmol. 2000;238(8):664–668. doi:10.1007/s004170000170
177. von Noorden GK, Jenkins RH, Rosenbaum AL. Horizontal transposition of the vertical rectus muscles for treatment of ocular torticollis. J Pediatr Ophthalmol Strabismus. 1993;30(1):8–14. doi:10.3928/0191-3913-19930101-04
178. Gräf M, Hausmann A, Lorenz B. High-dose Anderson operation for nystagmus-related anomalous head turn. Graefes Arch Clin Exp Ophthalmol. 2019;257(9):2033–2041. doi:10.1007/s00417-019-04369-0
179. Zubcov AA, Stärk N, Weber A, Wizov SS, Reinecke RD. Improvement of visual acuity after surgery for nystagmus. Ophthalmology. 1993;100(10):1488–1497. doi:10.1016/s0161-6420(13)31453-5
180. Sendler S, Shallo-Hoffmann J, Mühlendyck H. Artificial divergence surgery in congenital nystagmus. Fortschr Ophthalmol. 1990;87(1):85–89.
181. Hertle RW, Dell’Osso LF, FitzGibbon EJ, Yang D, Mellow SD. Horizontal rectus muscle tenotomy in children with infantile nystagmus syndrome: a pilot study. J AAPOS. 2004;8(6):539–548. doi:10.1016/j.jaapos.2004.08.005
182. Hertle RW, Dell’Osso LF, FitzGibbon EJ, Thompson D, Yang D, Mellow SD. Horizontal rectus tenotomy in patients with congenital nystagmus: results in 10 adults. Ophthalmology. 2003;110(11):2097–2105. doi:10.1016/S0161-6420(03)00802-9
183. Wang ZI, Dell’Osso LF. Tenotomy procedure alleviates the “slow to see” phenomenon in infantile nystagmus syndrome: model prediction and patient data. Vision Res. 2008;48(12):1409–1419. doi:10.1016/j.visres.2008.03.007
184. Boyle NJ, Dawson ELM, Lee JP. Benefits of retroequatorial four horizontal muscle recession surgery in congenital idiopathic nystagmus in adults. J AAPOS. 2006;10(5):404–408. doi:10.1016/j.jaapos.2006.03.013
185. Dell’Osso LF, Wang ZI. Chapter 1.10 - extraocular proprioception and new treatments for infantile nystagmus syndrome. In: Kennard C, Leigh RJ editors. Progress in Brain Research. Vol 171. Using Eye Movements as an Experimental Probe of Brain Function. Elsevier; 2008:67–75. doi:10.1016/S0079-6123(08)00610-9.
186. Self JE, Lee H. Novel therapeutics in nystagmus: what has the genetics taught us so far? Ther Adv Rare Dis. 2021;2:2633004021998714. doi:10.1177/2633004021998714
187. Adams DR, Menezes S, Jauregui R, et al. One-year pilot study on the effects of nitisinone on melanin in patients with OCA-1B. JCI Insight. 2019;4(2):e124387. doi:10.1172/jci.insight.124387
188. Leguire LE, Rogers GL, Bremer DL, Walson P, Hadjiconstantinou-Neff M, Flynn JT. Levodopa and childhood amblyopia. J Pediatr Ophthalmol Strabismus. 1992;29(5):290–299. doi:10.3928/0191-3913-19920901-08
189. Russell S, Bennett J, Wellman JA, et al. Efficacy and safety of voretigene neparvovec (AAV2-hRPE65v2) in patients with RPE65-mediated inherited retinal dystrophy: a randomised, controlled, open-label, Phase 3 trial. Lancet. 2017;390(10097):849–860. doi:10.1016/S0140-6736(17)31868-8
190. Campofelice A, Lentini L, Di Leonardo A, et al. Strategies against nonsense: oxadiazoles as translational readthrough-inducing drugs (TRIDs). Int J Mol Sci. 2019;20(13):3329. doi:10.3390/ijms20133329
191. Manuvakhova M, Keeling K, Bedwell DM. Aminoglycoside antibiotics mediate context-dependent suppression of termination codons in a mammalian translation system. RNA. 2000;6(7):1044–1055. doi:10.1017/s1355838200000716
192. Leubitz A, Frydman-Marom A, Sharpe N, van Duzer J, Campbell KCM, Vanhoutte F. Safety, tolerability, and pharmacokinetics of single ascending doses of ELX-02, a potential treatment for genetic disorders caused by nonsense mutations, in healthy volunteers. Clin Pharmacol Drug Dev. 2019;8(8):984–994. doi:10.1002/cpdd.647
193. Welch EM, Barton ER, Zhuo J, et al. PTC124 targets genetic disorders caused by nonsense mutations. Nature. 2007;447:7140):87–91. doi:10.1038/nature05756
194. Meng W, Dong Y, Liu J, et al. A clinical evaluation of amlexanox oral adhesive pellicles in the treatment of recurrent aphthous stomatitis and comparison with amlexanox oral tablets: a randomized, placebo controlled, blinded, multicenter clinical trial. Trials. 2009;10:30. doi:10.1186/1745-6215-10-30
195. Friesen WJ, Trotta CR, Tomizawa Y, et al. The nucleoside analog clitocine is a potent and efficacious readthrough agent. RNA. 2017;23(4):567–577. doi:10.1261/rna.060236.116
196. Lueck JD, Yoon JS, Perales-Puchalt A, et al. Engineered transfer RNAs for suppression of premature termination codons. Nat Commun. 2019;10(1):822. doi:10.1038/s41467-019-08329-4
197. Mehta AR, Kennard C. The pharmacological treatment of acquired nystagmus. Pract Neurol. 2012;12(3):147–153. doi:10.1136/practneurol-2011-000181
198. Teufel J, Bardins S, Spiegel R, et al. Real-time computer-based visual feedback improves visual acuity in downbeat nystagmus - a pilot study. J Neuroeng Rehabil. 2016;13:1. doi:10.1186/s12984-015-0109-2
199. Tse BC, McKeown CA, Tse DT. Titanium T-plate as a platform for globe stabilization in acquired nystagmus and oscillopsia without a null zone. Ophthalmic Plast Reconstr Surg. 2017;33(3):e61–e63. doi:10.1097/IOP.0000000000000750
200. Chen Y, Stevens S, Topilow N, Capo H, Tse D. Titanium T-plate as a stabilizing platform in the management of acquired nystagmus and oscillopsia without a null zone. Ophthalmic Plast Reconstr Surg. 2022;38(3):e89–e92. doi:10.1097/IOP.0000000000002123
201. Nachev P, Rose GE, Verity DH, et al. Magnetic oculomotor prosthetics for acquired nystagmus. Ophthalmology. 2017;124(10):1556–1564. doi:10.1016/j.ophtha.2017.05.028
202. Tychsen L, Richards M, Wong A, Foeller P, Bradley D, Burkhalter A. The neural mechanism for latent (fusion maldevelopment) nystagmus. J Neuroophthalmol. 2010;30(3):276–283. doi:10.1097/WNO.0b013e3181dfa9ca
203. Cho C, Park S, Ma S, Lee HJ, Lim EC, Hong SK. Feasibility of video-based real-time nystagmus tracking: a lightweight deep learning model approach using ocular object segmentation. Front Neurol. 2024;15:1342108. doi:10.3389/fneur.2024.1342108
204. Kalla R, Teufel J, Feil K, Muth C, Strupp M. Update on the pharmacotherapy of cerebellar and central vestibular disorders. J Neurol. 2016;263(Suppl 1):S24–S29. doi:10.1007/s00415-015-7987-x
205. Duesing SL, Lane-Karnas K, Duesing SJA, et al. Sensory substitution and augmentation techniques in cerebral visual impairment: a discussion of lived experiences. Front Hum Neurosci. 2025;19:1510771. doi:10.3389/fnhum.2025.1510771
206. Jeong SH, Kim JS. Update on nystagmus and other ocular oscillations. J Clin Neurol. 2021;17(3):337–343. doi:10.3988/jcn.2021.17.3.337
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.