")
Back to Journals » Clinical Ophthalmology » Volume 18
Ocular Surface Disease and Dry Eye Severity in Glaucoma Patients at Urban Private Eye Care Centres in Malaysia
Authors Gan EH, Woo WW, Seng KF, Singh P, Lee MY, Kong VY, Khoo SP, Lee MW, Liang LK
Received 6 May 2024
Accepted for publication 21 October 2024
Published 14 November 2024 Volume 2024:18 Pages 3249—3262
DOI https://doi.org/10.2147/OPTH.S476779
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Eng Hui Gan,1 Wen Wei Woo,1 Kheong Fang Seng,1 Pall Singh,2 Ming Yueh Lee,3 Vui Yin Kong,4 Say Peng Khoo,4 Mun Wai Lee,5 Liau Kok Liang6
1International Specialist Eye Centre, Kuala Lumpur, Selangor, Malaysia; 2Tun Hussein Onn National Eye Hospital, Petaling Jaya, Selangor, Malaysia; 3Parkcity Medical Centre, Kuala Lumpur, Selangor, Malaysia; 4Synergy Specialist Eye Centre, Kota Kinabalu, Sabah, Malaysia; 5LEC Eye Centre, Ipoh, Perak, Malaysia; 6Mahkota Medical Centre, Melaka, Malaysia
Correspondence: Eng Hui Gan, International Specialist Eye Centre (ISEC) Kuala Lumpur, Level 8 Centrepoint South MidValley City, Kuala Lumpur, 59200, Malaysia, Tel +603 2284 8989, Fax +603 2284 4330, Email [email protected]
Background: Ocular surface disease (OSD) severity varies among glaucoma patients and is exacerbated by intraocular pressure (IOP)-lowering medications.
Purpose: To determine OSD prevalence and dry eye severity among glaucoma patients at nine private clinics in Malaysia.
Methods: This multicentre, cross-sectional observational study recruited glaucoma patients undergoing routine eye examinations, with IOP ≤ 21mmHg receiving anti-glaucoma eye drops. OSD was assessed through National Eye Institute (NEI) scoring, tear film break-up time (TBUT), hyperaemia grading, Schirmer’s tests and questionnaires on symptom evaluation, OSD index and quality of life (QoL).
Results: Our cohort (n = 406, mostly male, ethnically Chinese, mean 63.5 ± 11.5 years, mean IOP 15.34 ± 2.95mmHg) frequently used prostaglandin analogues or PGA/beta-blockers and had cornea total NEI scores of 3.64 ± 2.76, mostly with minimal (51.2%) or mild (40.4%) epitheliopathy. Mean TBUT was 6.59 ± 3.08s (25.0%) in patients with severe lipid deficiency dry eye (DE). Bulbar conjunctiva hyperemia (70.4%) and palpebral conjunctiva hyperemia (68.0%) were mild. Schirmer’s test showed that most had tear deficiency (70.2%) with severe DE (38.9%). Questionnaires reported ocular symptoms in few patients, but 69.2% had DE symptoms (13.1% moderate/severe). While QoL was good, several patients had QoL and OSD index scores suggesting some adaptation to ocular symptoms and discomfort, with most patients being unconcerned (43– 60%) by the occurrence of eye drop side effects (75.4%).
Conclusion: Normal-mild DE or OSD can be asymptomatic, and the symptoms are unlikely to bother most patients. However, as OSD severity varies in patients with glaucoma, it should be evaluated using questionnaires and clinical tests to ensure that subjectively asymptomatic individuals are not missed.
Keywords: glaucoma, ocular surface disease, prevalence, questionnaires, clinical tests
Introduction
Glaucoma is a multifactorial disease with increased risks of ocular surface disease (OSD),1 while OSD is a multifactorial disorder of the tear film, eyelids, cornea and conjunctiva.2 Approximately 60% of patients have comorbid glaucoma and OSD,3 with older individuals frequently affected.3,4 OSD can develop in glaucoma patients as a pre-existing condition exacerbated by topical therapy or a new condition after initiating topical glaucoma medication.2
Ocular surface conditions are affected by environmental and social factors. The former includes climate-associated factors such as allergens, wind speed, temperature and humidity; pollution including those that are airborne or particulates.5 The latter include residential and working conditions, access to health services and digital information.6 OSD presents as dry eye resulting from inadequate or deficient tear production but can involve tear film degradation and ocular surface damage causing ocular discomfort and decreased visual clarity.7,8 Clinically meaningful signs of OSD include short tear film break-up time (TBUT), high tear osmolarity, increased ocular surface staining, and hyperaemia.8
Stopping glaucoma progression and maintaining the visual field is achieved by reducing intraocular pressure (IOP),1,9 as proven in several case studies.10,11 First-line therapy in ocular hypertension, primary open-angle glaucoma (POAG) and primary angle-closure glaucoma include IOP-lowering prostaglandin analogue (PGA)-based eye drops,12,13 which can delay disease progression and prevent further optic nerve damage.14 PGAs facilitate a hypotensive effect via the prostaglandin FP receptors, located in the ciliary muscle and in the trabecular meshwork that provide increased uveoscleral and trabecular meshwork outflow.3 However, the long-term or chronic use of such topical anti-glaucoma treatments changes the ocular surface and tear film function,15–18 and can lead to conjunctival squamous metaplasia, goblet cell loss, corneal epithelial toxicity, tear film disruption and ocular surface inflammation,19 thus aggravating OSD, such as dry eyes, punctate keratitis or hyperaemia.16,20,21 Despite their efficacy, 49–59% of patients on IOP-lowering eye drops present with OSD.2 Persisting OSD symptoms can reduce medication adherence in patients with glaucoma and adverse surgical outcomes.2,22,23
OSD must be managed well in patients with glaucoma to reduce ocular morbidity and improve the success of glaucoma therapy.2 Recent Malaysian data on OSD prevalence in glaucoma patients is lacking, with most hospital-based and population-based studies that report specific causes of OSD, like dry eye disease, preceding 2018.24–27 Our primary objective was thus to determine the OSD prevalence among patients, with glaucoma presenting at nine private eye care centres in Malaysia, for whom such data does not currently exist. Our secondary objective was to evaluate the severity of dry eye symptoms in this cohort.
Methods
Study Design
Our multicentre, cross-sectional observational study was conducted at nine participating private eye care centres across Malaysia between 4 December 2020 and 13 September 2021. Study sites were selected across different regions to capture sufficient patients for an assessment of OSD prevalence in glaucoma patients attending these private eye clinics. The study was conducted in compliance with the Malaysian Good Clinical Practice, Declaration of Helsinki, and Questra Clinical Research tenets. The study protocol was approved by the National Medical Research Ethics Committee and the independent ethics committee of Ramsay Sime Darby Health Care. All patients provided informed consent before screening for eligibility and data collection.
Study Population
Patients were enrolled during their routine eye examination if they had a clinical diagnosis of glaucoma (POAG, primary angle-closure glaucoma, pseudoexfoliation glaucoma, pigment dispersion glaucoma or ocular hypertension) requiring IOP-lowering ocular medications. Demographic information, medical history and concomitant medication were recorded. Eligible patients were those aged ≥21 years, on anti-glaucoma medications for >6 months; IOP ≤21 mmHg (based on the Goldman Applanation Tonometer) in the study eye while on treatment; and minimum best-corrected visual acuity score of 6/36 on the Snellen Chart in each eye. Excluded patients were those with secondary ocular hypertension of glaucoma; severe visual field disorder (mean deviation of 20 dB or worse); a history of ocular surgery in the last 6 months (intraocular surgery, including laser treatment affecting ocular surface condition); a history of glaucoma or corneal refractive surgery; severe dry eye associated with systemic disorders requiring treatment; ocular allergy, inflammation or infection; use of eye drops for other ocular comorbidities and/or systemic or ophthalmic steroids; pregnant, nursing or lactating status; contact lens use; corneal abnormalities or comorbid conditions preventing reliable applanation tonometry; and use of oral antihistamine, antipsychotics or antidepressants. Patients were eligible for primary analysis if at least one eye met all inclusion criteria and no exclusion criteria. Study endpoints were based on changes to the first visit OSD assessments recorded by 9 examiners (study authors).
OSD Assessments
Fluorescein Staining Score
The conjunctival sac was stained with fluorescein, and patients were instructed to blink to distribute the dye. The stained area was measured using the National Eye Institute (NEI) system, which divided the cornea and conjunctiva into five and six areas, respectively. Each area was assigned a staining intensity score between 0 and 3 (0: no staining, 1: scarce, 2: dense, 3: coalesced; see https://www.aao.org/image/neiindustry-grading-system),28 to a total score of 15 for the cornea and 18 for the conjunctiva. Fluorescein staining and scoring were conducted on the eye(s) that fulfilled the inclusion and exclusion criteria. The eye with a higher NEI score served as the “study eye” if both were eligible. Total NEI score for the cornea was indicative of corneal epitheliopathy and graded as minimal (0–3), mild (4–7), moderate (8–11) or severe (12–15).29 Grading for total NEI score for the conjunctiva and conjunctiva plus cornea were not captured in this study owing to the lack of supporting literature.
Tear film Break-Up Time (TBUT)
Following fluorescein staining, TBUT was measured as the time between the last complete blink and the appearance of a dark spot (indicating an exposed corneal surface caused by a tear film break) using a slit-lamp microscope with a timer. The mean value was calculated from three consecutive measurements. A TBUT under 10 seconds indicated an abnormal tear film, with values of 5 to 10 seconds indicating mild-to-moderate dry eye and <5 seconds indicating severe dry eye.30
Hyperaemia Grading
Bulbar and palpebral conjunctival blood vessel dilation was categorised as follows: grade 0 (no vasodilation), grade 1 (some vessel vasodilation), grade 2 (extensive vessel vasodilation) and grade 3 (overall vasodilation).31 Reference photographs depicting the severity of conjunctival hyperaemia have been previously published.29
Schirmer’s Test
To assess tear production under anaesthesia, a Schirmer test strip was inserted in the lower fornix of the eye, and the eye was allowed to open and blink as usual; after 5 minutes, the strip was removed, and the tear edge marked. A wetting score of 0 to <5mm indicated severe tear deficiency and severe dry eyes, 5–10mm indicated moderate dry eyes, and ≥10 mm was normal (under anaesthesia, 10–15mm of wetting indicated mild dry eye, while >15mm of wetting indicated normal tear function).32,33
Questionnaire Evaluations
The secondary endpoint of dry eye symptom severity in glaucoma patients was evaluated using symptom evaluation questionnaires, two validated questionnaires [Ocular Surface Disease Index (“OSDI”) and Glaucoma quality of life (QoL)(gQoL-15)], and one unvalidated Patient Experience Questionnaire (PEQ; adapted from Bourne RRA, et al34). Irritation, burning or stinging sensation, foreign body sensation, tearing, itching, and dry eye were assessed, categorised into None, Trace, Mild, Moderate and Severe and evaluated on a 20-point scale. Using the OSDI questionnaire, OSD symptoms, functional limitations and environmental factors associated with dry eye were assessed35 on a 5-point scale (0–4, 0: none of the time, 1: some of the time, 2: half of the time, 3: most of the time, and 4: all the time). Using the gQoL-15 to evaluate QoL, the patients were followed-up to provide a Glaucoma Total Score (range for all visual tasks: 15 – no visual disability, to 75 – severe disability).36 Finally, the PEQ was used to collect data on our patients’ experience with treatment and its side effects. The results from all questionnaires were recorded in each patient’s case report form.
Statistical Analysis
All endpoint measures were summarised descriptively. Continuous variables were reported as the number of observations and mean ± standard deviation (SD), while categorical variables were presented as frequencies and percentages. The target sample size was calculated to be 400 patients based on a 3.54% prevalence of glaucoma in Asian patients,7 an estimated population of 29 million in Malaysia and a 20% dropout rate.37 All patients were included in the analysis. Missing data was reported as-is and excluded from final analyses.
The validated gQoL-15 and OSDI questionnaires were analysed using Pearson’s correlation for linear correlation between these scores for all patients. Scaled linear scores (QoL total score range of 0–60, with six scales 0–6; OSDI total score range of 0–48, with five scales 0–5) were used. Relatedness of the symptom evaluation questionnaire and the above questionnaires was not assessed as the former was unvalidated with a different total scoring (0–20). Pearson’s correlation coefficient is shown in r values [range: +1 (total positive linear correlation), 0 (no correlation) to −1 (total negative correlation)].
Results
Patient Characteristics and Demographics
Of 411 patients from nine study sites across Malaysia screened for eligibility, 406 participated (Figure 1). Most of the cohort were aged >50 years (84.5%; Table 1) with a mean age of 63.5 ± 11.5 years, ethnically Chinese (85.2%) and male (53.9%). POAG accounted for 82.8% of cases. The mean IOP of the cohort was 15.34 ± 2.95 mmHg, with most patients (53.7%) recruited based on the eligibility of their right eye (IOP ≤ 21mmHg). PGA was the most common IOP-reducing agent (34.0%), followed by a combination treatment with a PGA plus a beta-blocker (21.0%).
 |
Table 1 Patient Demographic and Disease Status |
 |
Figure 1 Study profile. |
Disease Evaluation
The mean total NEI score of the cornea was 3.64 ± 2.76 and 3.80 ± 2.78 for the conjunctiva, giving a combined (cornea and conjunctiva) total of 7.44 ± 5.17. Minimal corneal epitheliopathy was detected in 51.2% of patients, while 40.4% had mild epitheliopathy (Table 2). One patient had severe epitheliopathy, indicating severe OSD.
 |
Table 2 Clinical Scores for NEI, TBUT and Schirmer’s Tests (n = 406) |
Mean TBUT was 6.59 ± 3.08 seconds. Most patients (90.4%) had abnormal TBUT. TBUT was >10 seconds in 39 patients (9.6%), 5–10 seconds in 266 patients (65.5%), and <5 seconds in 101 patients (24.9%) (data not shown).
Bulbar conjunctiva and palpebral conjunctiva hyperaemia were reported in 70.4% and 68.0% of patients but most were mild (Figure 2).
 |
Figure 2 Hyperaemia grading. Patients with hyperaemia of various grades (n=406). |
Two-thirds (n = 285; 70.2%) of patients showed tear deficiency (Schirmer’s test ≤ 10mm; data not shown), with 38.9% (n = 158) recording scores <5mm, indicating severe dry eye.
Questionnaire Evaluations
In symptom evaluation questionnaires (Table 3), over 50% of patients felt no irritation, burning, stinging, tearing or itching sensation, while 70% reported no foreign body sensation. Yet, 69.2% of patients experienced dry eye symptoms at trace (35.7%), mild (22.2%), moderate (7.9%), and severe (3.4%) levels. Based on the OSDI questionnaires and severity scores (Table 4) in the overall cohort, OSDI was normal in 67% of patients, mild in 19.9% (collectively, n = 353 or 86.9%), moderate in 7.4% or severe in 5.7% (data not shown). Thus, any ocular discomfort or symptom was either unlikely to be noticed or experienced, or was noticed but unlikely to be considered noteworthy or bothersome.
 |
Table 3 Patient Symptom Evaluation |
 |
Table 4 OSDI Questionnaire Scoring According to Severity |
The gQoL-15 questionnaire showed a mean Glaucoma Total Score (n = 406) of 18.45 [SD: 5.84; median: 17 (Interquartile range, IQR: 15, 20); min, max: 2.54] (Figure 3), indicating a relatively good gQoL in our patients with most experiencing no or a little glaucoma-associated discomfort. A scatterplot to visually represent our study cohort (Figure 4) showed a positive correlation between gQoL-15 and OSDI (r = 0.473, p = 0.000), with most patients having low gQoL-15 (little to no difficulty with tasks) also having low OSDI scores. Several patients also had low QoL scores but high OSDI (perhaps due to the ocular discomfort), while others had high QoL but high OSDI (perhaps due to them being accustomed to ocular discomfort). These outliers were included in our scatterplot as no subgroup analyses was conducted, but their exclusion would likely have improved the correlation between the metrics.
 |
Figure 3 Glaucoma QoL-15 questionnaire. |
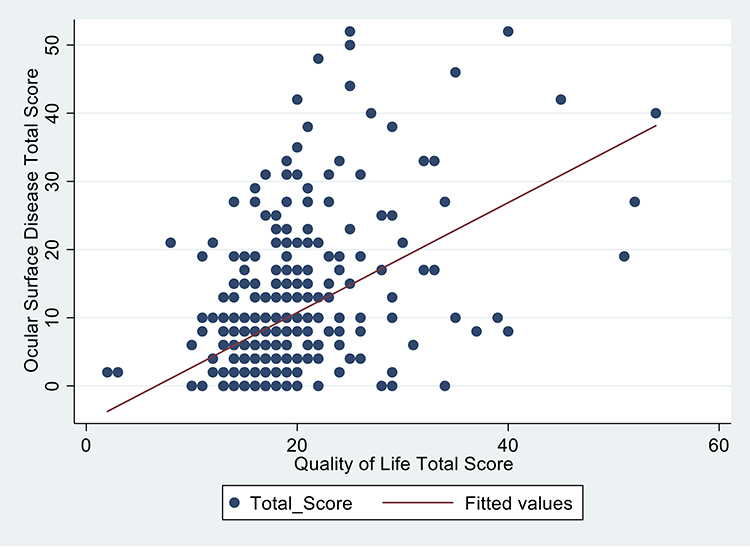 |
Figure 4 Scatterplot of correlation between gQoL-15 and OSDI with a best fit line (r=0.473). |
Finally, the PEQ showed that while 75.4% (n = 306) of patients experienced some side effects after eye drop instillation, 26.4% (n = 100) experienced none (Figure 5). Among the former, 43–60% of patients were unconcerned about side effects. Although side effects were evident, no patient consulted with a doctor, whereas 49% consulted nurses, pharmacists, or non-medical personnel, and 4.3% did not consult with anyone. Some level of ignorance of the discomfort caused by the IOP-reducing eye drop was evident, given that 109 subjects (35.6%) could not remember if they had received a consultation.
 |
Figure 5 Patient Experience Questionnaire (PEQ). |
Discussion
OSD is common among Malaysian patients with glaucoma. NEI score, TBUT, hyperaemia score and Schirmer’s test revealed that our patients experienced various degrees of OSD. Most patients showed signs of mild dry eye, possibly because only patients with mild-to-moderate glaucoma were enrolled. Punctate epithelial erosion was moderate/severe in 8.4% of patients but mild (Grade 1 or 2 NEI) in 91.6%; tear film instability was severe in 24.9% of patients but mild (5–10 seconds TBUT) in 75.1%; tear deficiency was severe in 38.9% of patients but moderate in 31.3% and normal in 29.8%; palpebral hyperaemia was severe in 2.0% but mild/moderate in 68%; and bulbar hyperaemia was mild/moderate in 68.9% of patients and severe in just 1.5%. Symptom evaluation questionnaires noted that most patients experienced no OSD-associated discomfort, while the OSDI and Glaucoma QoL-15 questionnaires found little impairment of QoL.
Our findings corroborate the studies correlating glaucoma with OSD.38 However, ocular signs are prevalent in Malaysian patients. Other countries or international studies reported decreased tear production and abnormal tear quality in 61.0% and 78.0% of patients, respectively (versus 70.2% and 90.4% in Malaysia),3 and conjunctival hyperaemia in 32.0% of participants (versus 70.4% [bulbar] and 68.0% [palpebral] in Malaysia).39 OSD prevalence may rise to 50.0% in the general population with glaucoma on medical treatment.40 OSD was more common in patients on IOP-lowering drugs for more than 6 months, than controls (72.4% vs 44.6%).41 Longer treatment durations were also statistically-significantly correlated with a deterioration in OSD symptoms, while high topical medication burdens increased OSD severity and impacted treatment adherence, outcomes, and QoL.41 A similar prevalence was also reported42 with 75.0% of glaucoma-treated patients exhibiting OSD versus 30.0% in glaucoma-free patients. Moreover, the additive effects of multiple medications increased ocular surface damage,42 dry eye prevalence and severity.13,43 This is relevant to glaucoma and ocular hypertension, which require multiple topical IOP-lowering agents and longer treatment durations.38,40,42,44–46
Recent local publications on OSD prevalence in glaucoma47,48 are sparse. In Turkey,49 at least 25% of patients with glaucoma may have OSD, with redness (91.9%) and conjunctival hyperaemia (75.6%) being the most commonly observed symptoms. In Finnish private clinics,50 glaucoma-affected patients had worse OSD symptoms and signs (excluding Schirmer’s test), and dry eye sensations than glaucoma-free individuals, indicating that medications must be chosen carefully. In Greece, over 93.1% of patients with glaucoma15 showed OSD signs including conjunctival hyperaemia, eyelid redness, conjunctival and corneal fluorescein staining, and abnormal TBUT. A Brazilian study51 uncovered high rates of OSD with glaucoma, and worse keratitis and conjunctival hyperaemia compared to patients with cataracts. Tear meniscus heights, bulbar redness, meibography grades, TBUT and QoL were worse in patients with glaucoma than cataract. Thus, these patients should be objectively assessed for changes in ocular surface integrity to address potential dry eye early, since long-term treatment is needed. A Thai study52 found OSD in 38.5% of glaucoma patients, who used a mean of 3.2–2.4 IOP-lowering drops daily, and 99.1% had abnormal tear quality, 32.1% had positive fluorescein staining, 38.6% had positive rose Bengal staining, and 73.4% had decreased tear production. Tests associated an increased number of IOP-lowering drops with increased abnormal corneal fluorescein and rose Bengal staining. High OSD rates required IOP-lowering eye drops to mitigate ocular surface toxicity, but in POAG patients with uncontrolled glaucoma and multiple topical medications, less toxic topical treatments are required to improve ocular surface health and IOP control.
Our questionnaire results contradicted, underscoring the importance of objective evaluations in identifying patients needing treatment. In public healthcare, questionnaires are a principal data collection tool but may be inaccurate,53 biased due to communication barriers,53 and subjective. Additionally, questionnaires detect fewer dry eye symptoms than clinical testing. In one report of OSD prevalence during cataract surgery assessments,54 63.3% of patients had abnormal tear tests, 39.2% had positive corneal staining, 7.5% had epithelial basement membrane dystrophy, and 1.6% had Salzmann nodules. In contrast, questionnaires detected OSD in just 54.0% of patients, with 85% of asymptomatic patients showing at least 1 abnormal tear test and 48% showing abnormalities in both tests. Ultimately, OSD was suspected in most (80%) patients with at least 1 abnormal tear test, and in 40% of those with 2 abnormal tests. An observational study55 of dry eye incidence and severity similarly found no foreign body sensations in nearly 60% of patients, with it occurring half or most of the time in 13% of those with sensations. Yet, TBUT was ≤5 seconds in 62.9% of patients, corneal staining was positive in 77% of eyes with positive central corneal staining seen in 50% of eyes, and Schirmer’s score was ≤5 mm in 21.3% of eyes. Thus, many patients remain undiagnosed with questionnaires, and subjective symptom assessments disagree with objective clinical evaluations. Both assessments are needed to prevent missing glaucoma patients with OSD and mitigate disease progression. Using questionnaires, ophthalmologists in settings with fewer objective tools (eg, rural clinics) can proactively offer treatments or escalate patients for specialist evaluations. At least two tests may also be needed to identify patients with undiagnosed dry eye.
Our outcomes may differ from those published, due to non-patient (eg, climate, urban locations) and patient-specific factors (eg, age, comorbidities). As glaucoma and OSD prevalence increase with age and become comorbid,41 one-sixth of patients with glaucoma require treatment for severe OSD. Age may have influenced outcomes within our cohort, 85% of whom were over 51 years. Older individuals have a higher Adversity Quotient (AQ)56 – an ability to cope with difficulties in life57 – and may consider the issues raised in the questionnaire (eg, eye discomfort) as insignificant and not warranting intervention or not associated with glaucoma or OSD nor feel any reduction in QoL. Over half of our patients were unconcerned or tolerated side effects from IOP-reducing medication (ie, had a high tolerance to discomfort).
Our large cohort (n = 411) comprised mainly ethnically Chinese patients (85.2%), in contrast to a 2021 survey of the general Malaysian population (22.4% ethnically Chinese and 69.8% ethnically Malay).58 This demographic is representative of private outpatient care in Malaysia and is reflected in two local studies on health insurance, where one found that 56.6% of participants were uninsured.59 Lack of insurance is high in the major ethnic group (Malays and other Bumiputra), who generally have lower incomes than ethnic Chinese.60 Ethnic Chinese also had a higher private health insurance and private healthcare uptake and usage59 due to their urban residency where these services are accessible.61 Thus, our patients reflect the urban, Chinese-dominant locations where our study sites/clinics are located. Furthermore, private hospitals in Malaysia are clustered in urban locations – a disincentive for Malays/Bumiputras who reside mainly in rural locations. There, government or public healthcare services are more highly available and utilized. Malays/Bumiputras also dominate the civil service, which provides them and their dependants with payment exemptions for public healthcare.61 The Malaysian government recently increased its reliance on private healthcare services to relieve public service burdens; thus, private medical centres have significant numbers of glaucoma patients and were those that agreed to join our study. Malaysian government clinics lack the time or resources to participate in such studies.
One small-cohort publication from an urban eye specialist hospital, which was also part of our study, found that 85.7% (n = 24) of patients were ethnically Chinese,1 with few ethnic Malays (3.6%, n = 1) or Indians (10.7%, n = 3). Our patients had early clinical eye care support due to increased private healthcare access, resources, and provision (eg, regular screening programmes). A 2016 study24 found dry eye in 33.8% of patients at a secondary referral hospital in Malaysia, of whom 47.2% may have had ocular surface changes. Ethnicity was statistically-significantly associated (p = 0.019) with dry eye, with the highest incidence in ethnic Malays (40.3%), Chinese (35.1%) and Indians (8.7%). The relationship between dry eye and ethnicity in Malaysia requires further study, as does the incidence, prevalence and severity of glaucoma with comorbid OSD, and the usage of different formulations of IOP-lowering drugs.
Our estimation of OSD prevalence at private eye care clinics across Malaysia and the association between OSD and glaucoma underscore a need to proactively prevent OSD when considering medication options for patients with glaucoma. We completed all assessments in one visit to reduce the risk of loss to follow-up and ensure adherence to the study protocol. Nevertheless, our study was limited by its cross-sectional, explorative nature and variable topical medication usage durations. A longitudinal analysis would have allowed us to capture changes within a patient cohort over time, to determine if such changes are likely attributable to the various medication formulations that may contribute to OSD or its progression.2,62 To better understand OSD prevalence, glaucoma patients over 50 years of age should be excluded to allow analysis of those without age-related dry eyes. Future studies should exclude those patients, but include a baseline period with a control group and a washout period to facilitate comparisons of the effects on OSD with different medication formulations. While the initial diagnosis of glaucoma and the duration of medication use impact OSD, our goal was to assess the prevalence and severity of OSD in our cohort of glaucoma patients. Nevertheless, future investigations should include the relationship between OSD severity and duration of medication use, the specific correlations between commonly used IOP-lowering medications and OSD, a comparative control group that had not used the study drugs, and patients from other regions for greater regional and ethnic coverage.
Our private clinics, primarily serving Chinese patients, may not represent Malaysia’s diverse population. A district hospital study47 found different visual impairment prevalence between districts due to demographic (age), socio-economic health service access and eye disease awareness factors. Our private clinics may also be similarly affected, highlighting a need for more public healthcare data to understand comorbid OSD and glaucoma rates, prevent missed diagnoses and mitigate disease progression. Future studies comparing OSD prevalence in glaucoma (including severe glaucoma) versus a normal cohort may confirm the high prevalence of coexisting OSD and glaucoma in Malaysia.
Conclusion
Malaysian patients with glaucoma experience various degrees of OSD. The coexistence of glaucoma, glaucoma therapy and OSD is an important consideration for patients and physicians. Prescriptions should account for a patient’s potential symptoms, risk factors for OSD, and their response to different medication formulations, to improve treatment compliance and outcomes.62 As our results show, glaucoma patients also have dry eyes, which should be considered in glaucoma management through the inclusion of treatment with preservative-free eye drops. Physicians can also incorporate the evaluation of OSD signs and symptoms into routine glaucoma assessments for early detection and treatment of both diseases.23
Acknowledgments
Santen Pharmaceutical funded the study but played no role in conducting the study, analysing the data or developing the contents of this manuscript. All investigators received investigator fees for their contribution to the study. Medical Writers Asia received funding from Santen Pharmaceuticals for independent statistical analyses by Lakmini Bulathsinhala and manuscript editing by Shawna Tan. The authors thank the contribution of all study investigators, patients and healthcare professionals involved in the study. Data analysis was conducted by Questra Clinical Research Sdn. Bhd. Medical writing assistance was provided by Veronica Yap and Lin Jia Lee of MIMS (Malaysia) while manuscript rewriting was provided by Dr Shawna Tan of Medical Writers Asia (Singapore) in accordance with the Good Publication Practice 3 guidelines.63
Disclosure
The authors report no conflicts of interest in this work.
References
1. L HH, S T. Ocular surface conditions in Asian glaucoma patients with existing corneal disorders switching from preserved prostaglandin analogue monotherapy to preservative-free tafluprost. Malays J Ophthalmol. 2021;3(3):109–122. doi:10.35119/myjo.v3i3.185
2. Zhang X, Vadoothker S, Munir WM, Saeedi O. Ocular Surface Disease and Glaucoma Medications: a Clinical Approach. Eye Contact Lens. 2019;45(1):11–18. doi:10.1097/icl.0000000000000544
3. Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma. 2008;17(5):350–355. doi:10.1097/IJG.0b013e31815c5f4f
4. Trask W, Muzychuk A. Strategies for the Management of Ocular Surface Disease in Glaucoma. Canadian Eye Care Today. 2023;2023:10–14.
5. Alves M, Asbell P, Dogru M, et al. TFOS Lifestyle Report: impact of environmental conditions on the ocular surface. The Ocular Surface. 2023;29:1–52. doi:10.1016/j.jtos.2023.04.007
6. Stapleton F, Abad JC, Barabino S, et al. TFOS lifestyle: impact of societal challenges on the ocular surface. Ocul Surf. 2023;28:165–199. doi:10.1016/j.jtos.2023.04.006
7. Chan EW, Li X, Tham YC, et al. Glaucoma in Asia: regional prevalence variations and future projections. Br J Ophthalmol. 2016;100(1):78–85. doi:10.1136/bjophthalmol-2014-306102
8. MA Lemp, GN Foulks. The Definition and Classification of Dry Eye Disease: report of the Definition and Classification Subcommittee of the International Dry Eye Workshop (2007). Ocul Surf. 2007;5(2):75–92. doi:10.1016/S1542-0124(12)70081-2
9. Society APG Asia Pacific Glaucoma Guidelines. 2016, Available from: https://pdf4pro.com/download/asia-pacific-glaucoma-guide-lines-1f2de5.html.
10. Luo LJ, Nguyen DD, Lai JY. Harnessing the tunable cavity of nanoceria for enhancing Y-27632-mediated alleviation of ocular hypertension. Theranostics. 2021;11(11):5447–5463. doi:10.7150/thno.54525
11. Luo LJ, Nguyen DD, Lai JY. Benzoic acid derivative-modified chitosan-g-poly(N-isopropylacrylamide): methoxylation effects and pharmacological treatments of Glaucoma-related neurodegeneration. J Control Release. 2020;317:246–258. doi:10.1016/j.jconrel.2019.11.038
12. Inoue K. Managing adverse effects of glaucoma medications. Clin Ophthalmol. 2014;8:903–913. doi:10.2147/opth.S44708
13. Baudouin C, Labbé A, Liang H, et al. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–334. doi:10.1016/j.preteyeres.2010.03.001
14. Harasymowycz P, Birt C, Gooi P, et al. Medical Management of Glaucoma in the 21st Century from a Canadian Perspective. J Ophthalmol. 2016;2016:6509809. doi:10.1155/2016/6509809
15. Dermenoudi M, Matsou A, Keskini C, Anastasopoulos E. Ocular Surface Disease Signs and Symptoms in Patients with Pseudoexfoliative Glaucoma: a Case-Control Study. Vision (Basel). 2022;6:20220208. doi:10.3390/vision6010011
16. Pisella PJ, Pouliquen P, Baudouin C. Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br J Ophthalmol. 2002;86(4):418–423. doi:10.1136/bjo.86.4.418
17. Wong ABC, Wang MTM, Liu K, et al. Exploring topical anti-glaucoma medication effects on the ocular surface in the context of the current understanding of dry eye. Ocul Surf. 2018;16(3):289–293. doi:10.1016/j.jtos.2018.03.002
18. Arita R, Itoh K, Maeda S, et al. Comparison of the long-term effects of various topical antiglaucoma medications on meibomian glands. Cornea. 2012;31(11):1229–1234. doi:10.1097/ICO.0b013e31823f8e7d
19. Roberti G, Agnifili L, Berardo F, et al. Prospective, Randomized, Single Masked, Parallel Study Exploring the Effects of a Preservative-Free Ophthalmic Solution Containing Hyaluronic Acid 0.4% and Taurine 0.5% on the Ocular Surface of Glaucoma Patients Under Multiple Long-Term Topical Hypotensive Therapy. Adv Ther. 2018;35(5):686–696. doi:10.1007/s12325-018-0699-8
20. Jaenen N, Baudouin C, Pouliquen P, et al. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur J Ophthalmol. 2007;17(3):341–349. doi:10.1177/112067210701700311
21. Kuppens EV, de Jong CA, Stolwijk TR, et al. Effect of timolol with and without preservative on the basal tear turnover in glaucoma. Br J Ophthalmol. 1995;79(4):339–342. doi:10.1136/bjo.79.4.339
22. Boimer C, Birt CM. Preservative exposure and surgical outcomes in glaucoma patients: the PESO study. J Glaucoma. 2013;22(9):730–735. doi:10.1097/IJG.0b013e31825af67d
23. Kaštelan S, Tomić M, Metež SK, Salopek-Rabatić J. How ocular surface disease impacts the glaucoma treatment outcome. Biomed Res Int. 2013;2013:696328. doi:10.1155/2013/696328
24. Muna’aim MA, Tey Y, Mohamad Zafarullah A, et al. Dry eye among patients at the eye clinic of a secondary referral hospital. Malays J Med Sci. 2016;12:30–37.
25. Mohd-Ali B, Fee LS, Abdul-Mutalib H, Mohidin N. Incidence of dry eye in a sample population in Kuala Lumpur. International Journal of Collaborative Research on Internal Medicine & Public Health. 2011;3:839–845.
26. Md Din N, Sa’aid S, Shen L, et al. Hormone Replacement Therapy and Dry Eye in Post Menopausal Women: study in a Tertiary Centre in Malaysia. International Journal of Medical Students. 2013;1(1):12–15. doi:10.5195/ijms.2013.14
27. Ling TE, Othman K, Yan OP, et al. Evaluation of Ocular Surface Disease in Asian Patients with Primary Angle Closure. Open Ophthalmol J. 2017;11(1):31–39. doi:10.2174/1874364101711010031
28. AAoO. NEI/Industry Grading System, Availble from: https://www.aao.org/image/neiindustry-grading-system.
29. Amparo F, Wang H, Yin J, et al. Evaluating Corneal Fluorescein Staining Using a Novel Automated Method. Invest Ophthalmol Vis Sci. 2017;58(6):Bio168–bio173. doi:10.1167/iovs.17-21831
30. Vidas Pauk S, Petriček I, Jukić T, et al. NONINVASIVE TEAR FILM BREAK-UP TIME ASSESSMENT USING HANDHELD LIPID LAYER EXAMINATION INSTRUMENT. Acta Clin Croat. 2019;58(1):63–71. doi:10.20471/acc.2019.58.01.09
31. Masumoto H, Tabuchi H, Yoneda T, et al. Severity Classification of Conjunctival Hyperaemia by Deep Neural Network Ensembles. J Ophthalmol. 2019;2019:7820971. doi:10.1155/2019/7820971
32. Miyake H, Kawano Y, Tanaka H, et al. Tear volume estimation using a modified Schirmer test: a randomized, multicenter, double-blind trial comparing 3% diquafosol ophthalmic solution and artificial tears in dry eye patients. Clin Ophthalmol. 2016;10:879–886. doi:10.2147/opth.S105275
33. Holly FJ, Lamberts DW, Esquivel ED. Kinetics of capillary tear flow in the Schirmer strip. Curr Eye Res. 1982;2(1):57–70. doi:10.3109/02713688208998380
34. Bourne RRA, Kaarniranta K, Lorenz K, et al. Changes in ocular signs and symptoms in patients switching from bimatoprost-timolol to tafluprost-timolol eye drops: an open-label Phase IV study. BMJ Open. 2019;9(4):e024129. doi:10.1136/bmjopen-2018-024129
35. Dougherty BE, Nichols JJ, Nichols KK. Rasch Analysis of the Ocular Surface Disease Index (OSDI). Investigative Ophthalmology & Visual Science. 2011;52(12):8630–8635. doi:10.1167/iovs.11-8027
36. Goldberg I, Clement CI, Chiang TH, et al. Assessing Quality of Life in Glaucoma Patients Using the Glaucoma Quality of Life – 15 (GQL–15) Questionnaire. Investigative Ophthalmology & Visual Science. 2005;46:1902.
37. D WW, C CL. Biostatistics a Foundation for Analysis in the Health Sciences.
38. Asiedu K, Abu SL. The impact of topical intraocular pressure lowering medications on the ocular surface of glaucoma patients: a review. J Curr Ophthalmol. 2019;31(1):8–15. doi:10.1016/j.joco.2018.07.003
39. Stalmans I, Lemij H, Clarke J, Baudouin C. Signs and Symptoms of Ocular Surface Disease: the Reasons for Patient Dissatisfaction with Glaucoma Treatments. Clin Ophthalmol. 2020;14:3675–3680. doi:10.2147/opth.S269586
40. Mylla Boso AL, Gasperi E, Fernandes L, et al. Impact of Ocular Surface Disease Treatment in Patients with Glaucoma. Clin Ophthalmol. 2020;14:103–111. doi:10.2147/opth.S229815
41. Pai V, Reddy LSH. Prevalence of ocular surface disease in patients with glaucoma on topical medications. Asian Journal of Ophthalmology. 2018;16(2):101–109. doi:10.35119/asjoo.v16i2.382
42. Barisic F, Krolo I, Popovic-Suic S, et al. Prevalence of ocular surface disease in patients with glaucoma using topical antiglaucoma medications. J Clin Exp Ophthalmol. 2014;5(02):2. doi:10.4172/2155-9570.1000334
43. Garcia-Feijoo J, Sampaolesi JR. A multicenter evaluation of ocular surface disease prevalence in patients with glaucoma. Clin Ophthalmol. 2012;6:441–446. doi:10.2147/opth.S29158
44. Seen S, Tong L. Dry eye disease and oxidative stress. Acta Ophthalmol. 2018;96(4):e412–e420. doi:10.1111/aos.13526
45. S DIS, Agnifili L, Ciancaglini M, et al. In Vivo Scanning Laser Confocal Microscopy of Conjunctival Goblet Cells in Medically-controlled Glaucoma. In Vivo. 2018;32(2):437–443. doi:10.21873/invivo.11259
46. Thygesen J. Glaucoma therapy: preservative-free for all? Clin Ophthalmol. 2018;12:707–717. doi:10.2147/opth.S150816
47. Thevi T, Basri M, Reddy S. Prevalence of eye diseases and visual impairment among the rural population–a case study of Temerloh hospital. Malaysian Family Physician: the Official Journal of the Academy of Family Physicians of Malaysia. 2012;7(1):6.
48. Ramli N, Supramaniam G, Samsudin A, et al. Ocular Surface Disease in Glaucoma: effect of Polypharmacy and Preservatives. Optom Vis Sci. 2015;92(9):e222–226. doi:10.1097/OPX.0000000000000542
49. Yıldırım N, Bozkurt B, Yüksel N, et al. Prevalence of Ocular Surface Disease and Associated Risk Factors in Glaucoma Patients: a Survey Study of Ophthalmologists. Turk J Ophthalmol. 2022;52(5):302–308. doi:10.4274/tjo.galenos.2021.20726
50. Parkkari M, Purola P, Uusitalo H. Ocular surface disease signs and symptoms of glaucoma patients and their relation to glaucoma medication in Finland. Eur J Ophthalmol. 2022;33:20221213. doi:10.1177/11206721221144339
51. Portela RC, Fares NT, Machado LF, et al. Evaluation of Ocular Surface Disease in Patients With Glaucoma: clinical Parameters, Self-report Assessment, and Keratograph Analysis. J Glaucoma. 2018;27(9):794–801. doi:10.1097/ijg.0000000000001007
52. Ruangvaravate N, Prabhasawat P, Vachirasakchai V, Tantimala R. High Prevalence of Ocular Surface Disease Among Glaucoma Patients in Thailand. J Ocul Pharmacol Ther. 2018;34(5):387–394. doi:10.1089/jop.2017.0104
53. Choi BC, Pak AW. A catalog of biases in questionnaires. Prev Chronic Dis. 2005;2(1):A13.
54. Gupta PK, Drinkwater OJ, VanDusen KW, et al. Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg. 2018;44(9):1090–1096. doi:10.1016/j.jcrs.2018.06.026
55. Trattler WB, Majmudar PA, Donnenfeld ED, et al. The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423–1430. doi:10.2147/OPTH.S120159
56. Somaratne C, Jayawardena LNAC, Perera B. Role of Adversity Quotient (AQ) on Perceived Stress of Managers: with specific reference to AQ Dimensions. Kelaniya Journal of Management. 2020;8(2):40. doi:10.4038/kjm.v8i2.7603
57. Singh S, Sharma T. Affect of Adversity Quotient on the Occupational Stress of IT Managers in India. Procedia Computer Science. 2017;122:86–93. doi:10.1016/j.procs.2017.11.345
58. Malaysia DoS. Availble from: https://www.dosm.gov.my/portal-main/release-content/current-population-estimates-malaysia-2021.
59. Balqis-Ali NZ, Anis-Syakira J, Fun WH, Sararaks S. Private Health Insurance in Malaysia: who Is Left Behind? Asia Pac J Public Health. 2021;33(8):861–869. doi:10.1177/10105395211000913
60. Malaysia DoS. Household Income & Basic Amenities Survey Report 2019. 2020. Availble from: https://www.dosm.gov.my/portal-main/release-content/household-income-&-basic-amenities-survey-report-2019.
61. Anis-Syakira J, Jawahir S, Abu Bakar NS, et al. Factors Affecting the Use of Private Outpatient Services among the Adult Population in Malaysia. Int J Environ Res Public Health. 2022;19(20):20221021. doi:10.3390/ijerph192013663
62. Costa VP, Marcon IM, Galvão Filho RP, Malta RFS. The prevalence of ocular surface complaints in Brazilian patients with glaucoma or ocular hypertension. Arquivos Brasileiros de Oftalmologia. 2013;76(4):221–225. doi:10.1590/S0004-27492013000400006
63. Battisti WP, Wager E, Baltzer L, et al. Good Publication Practice for Communicating Company-Sponsored Medical Research: GPP3. Ann Intern Med. 2015;163(6):461–464. doi:10.7326/M15-0288
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Pooled Assessment of Ocular Surface Disease After Switching from Preserved Prostaglandins to Tafluprost Across Six Countries in Asia
Tumbocon JA, Wong TT, Sangapillai T, Yen YC, Park SW, Lim HH, Ruangvaravate N
Clinical Ophthalmology 2022, 16:2669-2676
Published Date: 17 August 2022