")
Back to Journals » Nature and Science of Sleep » Volume 17
Optimizing Obstructive Sleep Apnea Risk Assessment in Hypertension: Development of a Predictive Nomogram in China
Authors Yang Y , Sun X, Liang J, Liao WF, Ye W, Zheng Z, Du L, Chen M, Zhang Y , Lin W, Huang J, Yao W, Chen R
Received 7 August 2024
Accepted for publication 26 January 2025
Published 11 February 2025 Volume 2025:17 Pages 285—295
DOI https://doi.org/10.2147/NSS.S486186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Yitian Yang,1,* Xishi Sun,2,* Jinhua Liang,1,* Wei Feng Liao,1,* Weilong Ye,1 Zhenzhen Zheng,1 Lianfang Du,1 Mingdi Chen,1 Yuan Zhang,3 Wenjia Lin,2 Jinyu Huang,2 Weimin Yao,1 Riken Chen1,4
1The Second Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524003, People’s Republic of China; 2Emergency Medicine Center, Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524001, People’s Republic of China; 3The First Clinical School of Medicine, Guangdong Medical University, Zhanjiang, Guangdong, 524003, People’s Republic of China; 4State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, 510120, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Riken Chen; Weimin Yao, The Second Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524003, People’s Republic of China, Tel +13560244631 ; +13822521722, Email [email protected]; [email protected]
Purpose: Obstructive sleep apnea (OSA) is common in patients with hypertension. Our study aims to construct and validate an objective nomogram that can accurately predict the risk of OSA in patients with hypertension.
Patients and Methods: Retrospective data were collected from patients with hypertension who underwent polysomnography (PSG) at the Sleep Medicine Center of the First Affiliated Hospital of Guangzhou Medical University, China. All participants were assigned to the training group (used to develop the predictive model). Similarly, data from patients with hypertension who underwent PSG at the Sleep Medicine Center of the Second Affiliated Hospital of Guangdong Medical University, China, were collected, and these participants were assigned to the validation group (used to test the model’s performance). Logistic and LASSO regression analyses were used to identify factors and construct the nomogram. C-index, calibration curve, decision curve analysis (DCA) and clinical impact curve analysis (CICA) were used to assess the model. Finally, nomogram validation was performed in the validation group.
Results: This study included a training group of 303 patients and a validation group of 217 patients. Based on LASSO and Logistic regression analyses and clinical practicality, we identified gender, age, BMI (body mass index), NC (neck circumference) and ESS (Epworth Sleepiness Scale) as predictors for the nomogram. The C-index is 0.840 in the training group and 0.808 in the validation group. The area under the curve (AUC) of the predictive model and STOP-Bang at the three diagnostic cut-off points of the Apnea-Hypopnea Index (AHI) ≥ 5, AHI ≥ 15 and AHI ≥ 30 were 0.840 vs 0.778, 0.754 vs 0.740, and 0.765 vs 0.751 respectively. The AUC at each intercept point was higher than that of STOP-Bang. DCA and CICA showed that the nomogram is clinically useful.
Conclusion: The nomogram predictive model consisting of the five indicators (gender, age, BMI, NC and ESS) can be useful in determining OSA risk in patients with hypertension.
Keywords: obstructive sleep apnea, nomogram, predictors, STOP-Bang
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Pan has been published for this article.
Graphical Abstract:

Introduction
Obstructive sleep apnea (OSA) is a common and potentially fatal disease in clinical practice, with an adult prevalence of 2%-7% and a higher prevalence in the elderly.1 In recent years, the global rise in obesity has been accompanied by a significant increase in the prevalence of OSA, with a recent study by Cunningham et al reporting that 57.7% of males and 41.7% of females had any OSA, while 20.2% of males and 10.0% of females had moderate to severe OSA.2 The American Heart Association’s scientific statement on OSA and cardiovascular disease highlights that the risk of OSA is closely linked to BMI, with obesity being the primary modifiable risk factor for the condition.3 A recent meta-analysis demonstrated that a reduction in weight or BMI by 10%, 20%, and 30% corresponds to a 36%, 57%, and 69% decrease in AHI, respectively, regardless of the intervention applied.4 It is even more frightening that many cases of OSA in the population remain undiagnosed. According to the 2012 AASM interpretation guidelines, patients with AHI ≥ 5 times/h and obstructive apnea as the main type of respiratory event were judged as OSA patients, and the severity of the disease was classified into the normal group (AHI < 5 times/h), mild OSA group (5 ≤ AHI < 15 times/h), moderate OSA group (15 ≤ AHI < 30 times/h) and severe OSA group (≥30 times/h).5 Using AHI ≥5 as the diagnostic criterion, the prevalence of undiagnosed OSA could reach as high as 64.0% of participants, compared to 29.3% of participants when AHI ≥ 15 is applied.1,6 OSA is often accompanied by intermittent hypoxemia, nocturnal awakenings, daytime sleepiness, etc., which trigger neuroendocrine disorders, endothelial dysfunction and inflammatory response, leading to an increased risk of cardiovascular events. OSA is currently considered the most important factor in hypertension,1,7 and both are chronic diseases that significantly increase the risk of cardiovascular events. The Sleep Heart Health Study results show that the prevalence rates of hypertension in patients with mild, moderate and severe OSA are 59%, 62% and 67% respectively.8 A total of 30% to 50% of patients with hypertension have OSA, and the prevalence is even higher among patients with refractory hypertension: roughly 77% in women and as high as 90% in men.9 The two diseases exhibit common mechanisms, including increased sympathetic activity, activated systemic inflammation and oxidative stress.10,11 At present, there are few studies on the screening of OSA in patients with hypertension, and the treatment of OSA-related hypertension is very different from that of ordinary patients with hypertension. First, the problems of sleep apnea and nocturnal hypoxia must be solved. Therefore, in patients with hypertension, the diagnosis of OSA is very important. Chiu et al found that the Berlin Questionnaire (BQ), STOP-Bang, STOP and ESS had low specificity in detecting different severities of OSA.12 Therefore, the search for simple screening tools to identify OSA in patients with hypertension has become increasingly important. The nomogram is a simple and practical risk prediction tool that combines important predictors for judging clinical events and outcomes. It has been widely used to predict the risk and prognosis of various diseases.13–16 In the early stages, we established a nomogram composed of five factors including BMI and NC to predict OSA in the general population, and achieved good predictive performance.17 However, a nomogram model combining multiple objective clinical indicators with good ability to diagnose OSA in patients with hypertension has not yet been developed. Our study aims to develop and validate a nomogram for the accurate screening and prediction of OSA risk in patients with hypertension. By exploring a straightforward screening method, we intend to establish a predictive model that assists clinicians and community doctors in the early detection of OSA, facilitating timely intervention for refractory hypertension.
Material and Methods
Subjects
This study collected retrospective data of patients with confirmed hypertension who underwent polysomnography (PSG) at the Sleep Medicine Center of the First Affiliated Hospital of Guangzhou Medical University from April 2012 to September 2016, and at the Second Affiliated Hospital of Guangdong Medical University from June 2017 to June 2024. Eligible patients were selected according to inclusion and exclusion criteria. Inclusion criteria: (1) Patients with hypertension who received PSG at the Center for the first time due to symptoms related to sleep-disordered breathing (patients with a history of definite hypertension or taking antihypertensive drugs); (2) Patients with complete demographic information, anthropometric indicators and PSG data; (3) Total sleep time of > 4 hours. Exclusion criteria: (1) Patients with various psychiatric and psychological diseases; (2) Abuse of alcohol or sedatives/sleeping drugs; (3) History of brain tumor or epilepsy; (4) Pregnant women; (5) Previous diagnosis of obstructive sleep apnea hypoventilation syndrome (OSA). This retrospective study was approved by the Ethics Committees of the First Affiliated Hospital of Guangzhou Medical University (201705) and the Second Affiliated Hospital of Guangdong Medical University (PJKT2024-050). We adhered to the principles of the Declaration of Helsinki, ensuring patient data confidentiality and the protection of patient privacy.
Basic Data Collection
In this retrospective analysis study, we collected patient demographic data such as height, weight, age, gender, waist circumference (WC), Neck circumference (NC) and BMI. The ESS questionnaires were jointly filled out by the patients and their families. The ESS questionnaire consists of eight questions, allowing subjects to assess their degree of sleepiness in specific scenarios during the day, with 0 being no sleepiness and 1, 2 and 3 being light, moderate and severe sleepiness respectively, for a total score of 24 points. An ESS score of ≥ 10 points indicates the presence of some degree of daytime sleepiness.18
Polysomnography
PSG monitoring is mainly used to diagnose sleep-disordered breathing and assess patients’ sleep quality. Participants were asked not to drink alcohol or coffee or take sedatives or hypnotics on the day of monitoring. At the Center, a Philips Respironics ALICE 5 PSG was used for continuous and synchronous recording for at least seven hours, and the output was interpreted and analyzed by two trained sleep professionals. The recorded indicators included blood oxygen saturation, oral airflow, electrooculogram, chest and abdomen breathing, electrocardiogram, sleep posture and other parameters. AHI refers to the number of apnea events plus hypopnea per hour of sleep. According to the 2012 AASM (American Academy of Sleep Medicine) interpretation guidelines, patients with AHI ≥ 5 times/h and obstructive apnea as the main type of respiratory event were judged as OSA patients, and the severity of the disease was classified into the normal group (AHI < 5 times/h), mild OSA group (5 ≤ AHI < 15 times/h), moderate OSA group (15 ≤ AHI < 30 times/h) and severe OSA group (AHI ≥ 30 times/h).5
Establishment and Validation of the Nomogram
We performed Least Absolute Shrinkage and Selection Operator (LASSO) and logistic regression analyses to identify the best predictive features. A calibration curve was drawn to evaluate the calibration of the model, and the nomogram was bootstrapped to calculate the relative corrected C-index. The receiver operating characteristic (ROC) curve was drawn using MedCalc software, and the area under the curve (AUC) was determined to assess the discriminative power of the nomogram. Sensitivity, specificity, positive likelihood ratio (LRP) and negative likelihood ratio (LRN) were recorded at cut-off points of 5, 15, and 30 for AHI, respectively, and reported with their respective 95% CIs. Decision curve analysis (DCA) and clinical impact curve analysis (CICA) were used to assess the clinical benefits of the nomogram based on its net benefits at different threshold probabilities.
Statistical Analysis
SPSS 26.0 statistical software, R software 4.0.5 and MedCalc software were used for analysis. Measurement data were expressed as mean ± standard deviation, and count data were expressed as frequency. Measurement data were analyzed by the t test, and count data were analyzed by the chi-square test. P < 0.05 was defined as statistically significant.
Results
Baseline Characteristics
In the training group, 303 patients with hypertension and suspected OSA were collected from the Sleep Medicine Center of the First Affiliated Hospital of Guangzhou Medical University, while 217 patients from the Second Affiliated Hospital of Guangdong Medical University were included in the validation group. There were more males in the OSA group than in the non-OSA group, both in the training group and validation group. Compared to patients without OSA, patients with OSA had a higher BMI, NC, WC, total sleep time, AHI, ESS and STOP-Bang, while age was lower (P < 0.05, Table 1), but there were no significant differences in blood pressure and total recording time (TIB) (P > 0.05, Table 1). The statistically significant factors in the Table 1 were analyzed by univariate logistic regression to further identify risk factors. The results of univariate logistic regression analysis indicate that gender, age, BMI, NC, WC, ESS and STOP-Bang are potential risk factors for OSA (P < 0.05, Table 2).
 |
Table 1 Clinical Characteristics of the Study Participants with or Without OSA in Different Group |
 |
Table 2 Risk Factors for OSA Patients in the Training Group According to the Univariate Logistic Regression Model |
Factor Selection for Predictive Models
LASSO regression obtains compression coefficients by constructing a penalty function, and sets certain compression coefficients to zero so that the most important predictors can be extracted from the main dataset.19 In this study, each subject’s risk score was calculated by a linear combination of factors weighted by the subject’s coefficient, resulting in a coefficient distribution curve (Figure 1A). The error plot for the cross-validation of the LASSO regression model is shown in Figure 1B.
 |
Figure 1 Least Absolute Shrinkage and Selection Operator (LASSO) logistic regression model to select risk factors. (A). Optimal parameter (λ) selection in LASSO regression using 10-fold cross-validation (pass minimum criteria). Black vertical lines are drawn at the best values by using the smallest criterion and one standard error of the smallest criterion (1-SE criterion). (B). Profile of LASSO coefficients for 10 features plotted against logarithmic (λ) series. |
Nomogram Validation
Based on the results of univariate logistic regression analysis, combined with clinical practicality and significance, five risk predictors (gender, age, BMI, NC and ESS) were finally selected to develop an easy-to-use nomogram (Figure 2) Each factor was assigned a corresponding score, and the total score was the sum of the scores for each factor. The higher the total score, the higher the probability of bronchiectasis patients developing OSA. In terms of predicting OSA in patients with hypertension, the C-index of the nomogram in the training group and validation group were 0.840 and 0.808 respectively. The calibration plots showed good correlation between observed and predicted OSA in the training group (Figure 3A) and validation group (Figure 3B). In the training group, we used ROC curve to evaluate the model for predicting AHI diagnostic cut-offs at 5 events/hour, 15 events/hour and 30 events/hour. When the AUC of the nomogram was at the best cut-off point, the AUC was 0.840, 0.754 and 0.765, and the curve area of each of their intercept points was higher than the STOP-Bang (AUC = 0.778, 0.740 and 0.751) (Table 3, Figure 4A–C). It can be seen that the nomogram has a better diagnostic performance in predicting mild, moderate, and severe OSA in patients with hypertension.
 |
Table 3 The Efficiency of Nomogram and STOP-Bang for Detecting OSA (95% CI) |
 |
Figure 2 Construction of a nomogram for predicting OSA. Each variable is listed on the left side of the image. Each category for the variables is associated with a certain number of points. These points are found by drawing a vertical line up to the “Points” scale at the top of the nomogram. After calculating the points for each variable based on the patient’s characteristics, you sum up the total points. The total points can be located along the “Total Points” scale at the bottom of the chart. After identifying the total points, you draw a vertical line from the “Total Points” row down to the “Risk of OSA” scale. This will give you the predicted probability of developing OSA based on the given characteristics. Abbreviation: BMI: Body mass index; ESS: Epworth Sleepiness Scale; NC: Neck circumference; OSA: Obstructive sleep apnea. |
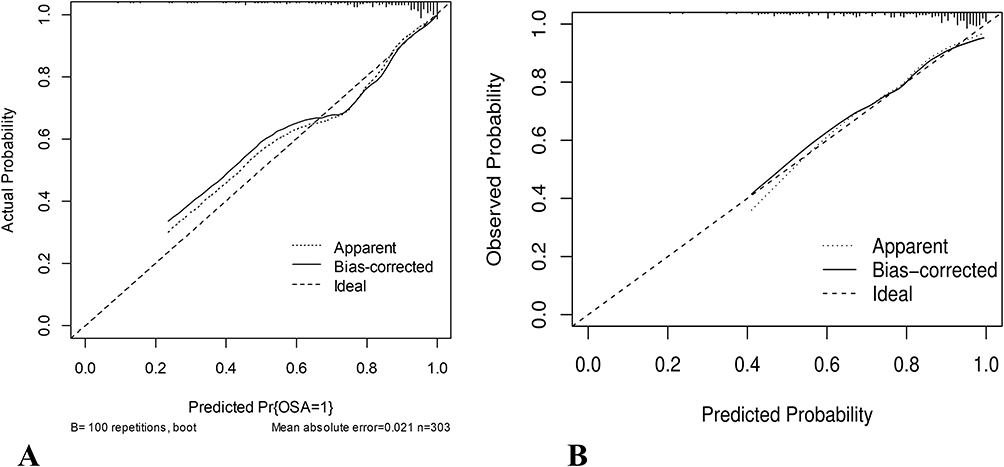 |
Figure 3 Calibration curves of the nomogram. The solid line represents the performance of the nomogram, with closer proximity to the diagonal dashed line indicating better predictive accuracy. (A). In the training group. (B). In the validation group. |
 |
Figure 4 ROC curves comparing the performance of the nomogram model and the STOP-Bang model. (A). At the cut-off points of the AHI ≥ 5. (B). At the cut-off points of the AHI ≥ 15. (C). At the cut-off points of the AHI ≥ 30. |
Clinical Application Value
Like other nomogram predictive models, this study evaluated the clinical utility of the nomogram clinical predictive model and STOP-Bang for predicting OSA in patients with hypertension using DCA and CICA (Figure 5A–F). Both in the training and validation groups, DCA and CICA showed better results visually, and the nomogram had superior overall net benefits over a wide and realistic threshold probability range, and impacted clinical outcomes in patients with hypertension.
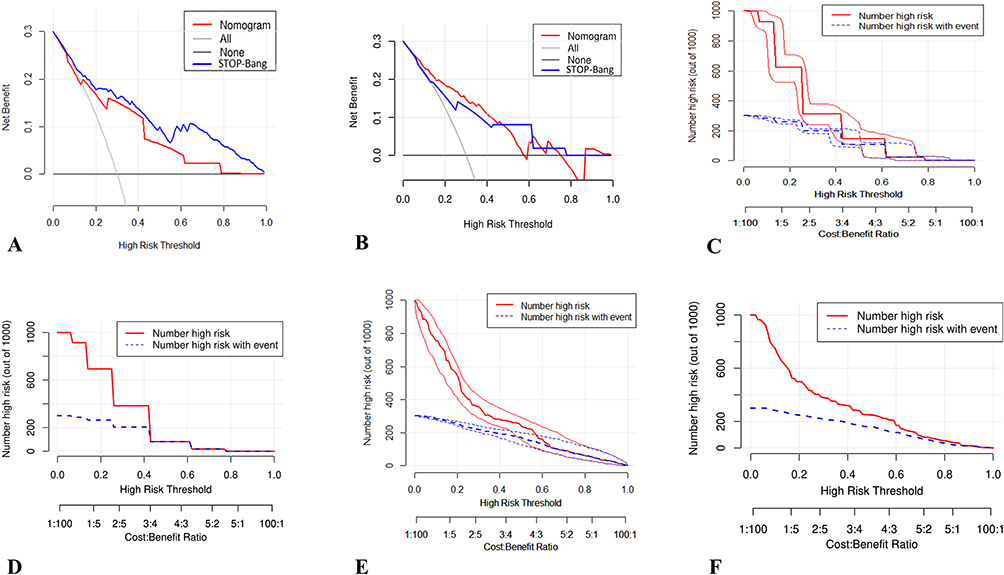 |
Figure 5 DCA and CICA for the STOP-Bang and the Nomogram model in the training and validation cohorts for predicting OSA. (A). DCA comparing the performance of the Nomogram model (blue line) and the STOP-Bang model (red line) in the training group. The y-axis represents the net benefit, and the x-axis represents the threshold probability. The black line assumes no intervention for any patient, while the grey line assumes intervention for all patients. (B). DCA for the validation group, comparing the Nomogram model (blue line) and the STOP-Bang model (red line). The results are consistent with the training group, indicating the robustness of the Nomogram model in external validation. (C). CICA for the STOP-Bang model in the training group. The red curve shows the number of patients classified as high risk for OSA at each threshold, while the blue curve shows the actual number of true positives. (D). CICA for the STOP-Bang model in the validation group, showing similar patterns to the training group. (E). CICA for the Nomogram model in the training group. The gap between the curves reflects the model’s ability to accurately predict high-risk patients. (F). CICA for the Nomogram model in the validation group. Similar to the training group. |
Discussion
Studies have found that OSA is very common in patients with hypertension, of whom 30% to 50% will have OSA, and for drug-resistant hypertension, up to 80% of patients may have OSA.3,20 In this retrospective study, we developed and validated a simple-to-use nomogram to predict the likelihood of OSA in the hypertensive population. The nomogram, which was developed using data from the training group, included five items: gender, age, BMI, NC and ESS. Many studies have found that men are more likely to develop more severe OSA.21 The higher prevalence of OSA in men may be related to characteristics of the upper airway tissue.22 Loss of fat and muscle mass in older adults due to weight loss often results in the impairment of the strength and effectiveness of the pharyngeal muscles, collapse of easily folded upper airways and increased risk of OSA.23 NC is an important independent predictor of OSA severity.21 Obesity will cause fat deposition in the tissues around the upper airway, resulting in sleep apnea or hypoventilation due to lumen shrinkage and upper airway collapse. Obesity and OSA are mutually causal, and obesity is an independent risk factor for OSA.24 BMI is associated with sleepiness in men, but in women with OSA, the ESS score is not associated with BMI.25 Moreover, a study reported that the prevalence of excessive daytime sleepiness (EDS), as defined by ESS, was 16.0% in the general population in Finland.26 Another study found that over one-fifth of American adults reported experiencing EDS.27 These findings indicate that EDS is relatively prevalent in non-clinical populations. Additionally, ESS has been shown to have a strong correlation with OSA.28 Therefore, the inclusion of sleepiness as a variable in our nomogram enhances its applicability, not only in clinical populations but also in non-clinical populations. We will further investigate the potential applications of this model in community populations in future studies. Therefore, the predictors of gender, age, DBP, BMI, NC and ESS are all associated with OSA, making them reasonable for model construction. These variables are readily available in clinical and community outpatient clinics, and the established nomogram shows good predictive performance, so it can be considered a primary screening tool to facilitate the assessment of hypertension patients at risk of developing OSA in outpatient clinics or remote areas with underdeveloped medical resources. This can help in the selection of high-risk patients for diagnostic PSG monitoring, thereby reducing the burden on both doctors and patients, and saving medical resources.
The nomogram is a graphical computing tool that has long been used in the clinic to facilitate clinical decision analysis at the bedside.29 A nomogram including disease duration, smoking status, sleep difficulty, lack of energy and WC was created by an ordinal logistic regression procedure, and was found to be more than 80% accurate in identifying non-OSA, moderate-to-severe OSA and severe OSA.30 The validation of the nomogram is important for avoiding overfitting and determining generality.13 In our study, the calibration curves of the training group and validation group showed that the actual probability of occurrence was close to the predicted probability, and there was good agreement between the two.Furthermore, the C-index of the nomogram for both the training and validation groups was 0.840, indicating that our nomogram, like the STOP-Bang questionnaire, has excellent discrimination and stability. STOP-Bang is a current method used for the widespread screening of OSA.31–33 In comparison with other questionnaires, we found that the diagnostic performance of STOP-Bang is very good, and it is applicable to both medical and surgical inpatients.31,34 In this study, it was found that the ROC curve of the nomogram composed of five indicators (gender, age, BMI, NC and ESS) showed that the curve area was better than STOP-Bang at each cut-off point. This suggests that our predictive model has better predictive value for these conditions compared to STOP-Bang. The indicators used in the modified model included objective indicators and the subjective ESS, which are highly relevant factors for OSA.28 This also contributed to the better predictive performance of the nomogram model than the STOP-Bang questionnaire. Our predictive model relies on demographic and anthropometric measurements, requires no additional effort and is low cost, thus it easily aids clinical decision-making. Current research suggests that OSA and hypertension are co-morbidities.1,35,36 To the best of our knowledge, this is the first study to develop a predictive OSA model using common demographic parameters in a hypertensive population, and may provide a great tool for the early diagnosis and treatment of OSA in patients with hypertension, especially patients with refractory hypertension. In other words, the nomogram holds significant potential for enhancing early diagnosis and improving treatment outcomes for patients with hypertension and OSA.
In this new study, we developed a nomogram predictive model incorporating five predictors: gender, age, BMI, neck circumference, and ESS, by incorporating multicenter data and advanced statistical methods. Compared to our previous single-center data and conventional statistical approaches,37 this new model demonstrates higher predictive accuracy (higher AUC values) at various diagnostic cut points (AHI ≥ 5, AHI ≥ 15, and AHI ≥ 30). Additionally, decision curve analysis (DCA) and clinical impact curve analysis (CICA) have proven its practical value in diverse clinical settings. This model significantly enhances the accuracy and reliability of OSA risk assessment in hypertensive patients, outperforming single tools such as STOP-Bang.
Advantages of this study: First, the sample size of patients with hypertension was relatively large, they had all undergone PSG testing and the anthropometric data was relatively complete. Second, we used the well-known STOP-Bang questionnaire as a reference, which is more persuasive. Limitations: Our nomogram was developed and validated based on inclusion and exclusion criteria specific to hypertensive patients in a retrospective study, with the model established in one hospital and validated in another. As a result, it is currently applicable to most clinical patients. In the future, we aim to conduct multicenter, prospective studies across a broader, unselected population, allowing the nomogram to benefit a wider, more general population.
Conclusion
This study developed a nomogram predictive model with good accuracy and clinical applicability that consists of five indicators: gender, age, BMI, NC and ESS. It may have value in determining OSA risk in patients with hypertension and may have important implications for patients with refractory hypertension.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University (Ethics Number: 201705). As this is a retrospective study, the requirement for consent was waived by an ethics committee.
Acknowledgments
We would also like to thank everyone who has helped with our research.
Authors’ Contributors
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
All authors have seen and approved the manuscript. The authors have no conflicts of interest.
Funding
This study was funded by the Guangdong Medical Research Fund Project (No. A2024728, No. A2024723), the Natural Science Foundation of Basic and Applied Basic Research Fund of Guangdong Province (No.2022A1515012375), the Science and Technology Development Special Fund Competitive Allocation Project of Zhanjiang City (2021A05086, 2021A05088) and the Science and Technology Development Special Project of Zhanjiang City (No.2022A01142, No. 2022A01110).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Torres G, Sanchez-de-la-Torre M, Barbe F. Relationship between OSA and hypertension. Chest. 2015;148(3):824–832. doi:10.1378/chest.15-0136
2. Cunningham J, Hunter M, Budgeon C, et al. The prevalence and comorbidities of obstructive sleep apnea in middle-aged men and women: the Busselton Healthy Ageing Study. J Clin Sleep Med. 2021;17(10):2029–2039. doi:10.5664/jcsm.9378
3. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a Scientific statement from the American Heart Association. Circulation. 2021;144(3):e56–e67. doi:10.1161/CIR.0000000000000988
4. Malhotra A, Heilmann CR, Banerjee KK, Dunn JP, Bunck MC, Bednarik J. Weight reduction and the impact on apnea-hypopnea index: a systematic meta-analysis. Sleep Med. 2024;121:26–31. doi:10.1016/j.sleep.2024.06.014
5. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
6. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504. doi:10.5664/jcsm.6506
7. Hou H, Zhao Y, Yu W, et al. Association of obstructive sleep apnea with hypertension: a systematic review and meta-analysis. J Glob Health. 2018;8(1):010405. doi:10.7189/jogh.08.010405
8. Gottlieb DJ. The sleep heart health study: a progress report. Curr Opin Pulm Med. 2008;14(6):537–542. doi:10.1097/MCP.0b013e328312ed61
9. Oscullo G, Torres G, Campos-Rodriguez F, et al. Resistant/refractory hypertension and sleep apnoea: current knowledge and future challenges. J Clin Med. 2019;8(11):1872. doi:10.3390/jcm8111872
10. Schwarz EI. Cardiovascular consequences of obstructive sleep apnea in different study models and novel perspectives. Curr Opin Pulm Med. 2019;25(6):614–622. doi:10.1097/MCP.0000000000000618
11. Garvey JF, Taylor CT, McNicholas WT. Cardiovascular disease in obstructive sleep apnoea syndrome: the role of intermittent hypoxia and inflammation. Eur Respir J. 2009;33(5):1195–1205. doi:10.1183/09031936.00111208
12. Chiu HY, Chen PY, Chuang LP, et al. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP, and Epworth sleepiness scale in detecting obstructive sleep apnea: a bivariate meta-analysis. Sleep Med Rev. 2017;36:57–70. doi:10.1016/j.smrv.2016.10.004
13. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–1370. doi:10.1200/JCO.2007.12.9791
14. Xue M, Liu L, Wang S, et al. A simple nomogram score for screening patients with type 2 diabetes to detect those with hypertension: a cross-sectional study based on a large community survey in China. PLoS One. 2020;15(8):e0236957. doi:10.1371/journal.pone.0236957
15. Wang W, Cai D. Complement components sC5b-9 and CH50 predict prognosis in heart failure patients combined with hypertension. Am J Hypertens. 2020;33(1):53–60. doi:10.1093/ajh/hpz140
16. Zhang J, Gong Z, Gong Y, Guo W. Development and validation of nomograms for prediction of overall survival and cancer-specific survival of patients with stage IV colorectal cancer. Jpn J Clin Oncol. 2019;49(5):438–446. doi:10.1093/jjco/hyz035
17. Sun X, Zheng Z, Liang J, et al. Development and validation of a simple clinical nomogram for predicting obstructive sleep apnea. J Sleep Res. 2022;31(5):e13546. doi:10.1111/jsr.13546
18. Veugen C, Teunissen EM, den Otter LAS, Kos MP, Stokroos RJ, Copper MP. Prediction of obstructive sleep apnea: comparative performance of three screening instruments on the apnea-hypopnea index and the oxygen desaturation index. Sleep Breath. 2021;25(3):1267–1275. doi:10.1007/s11325-020-02219-6
19. Friedman J, Hastie T, Tibshirani R. Regularization paths for generalized linear models via coordinate descent. J Stat Softw. 2010;33(1):1–22. doi:10.18637/jss.v033.i01
20. Pedrosa RP, Barros IML, Drager LF, et al. OSA is common and independently associated with hypertension and increased arterial stiffness in consecutive perimenopausal women. Chest. 2014;146(1):66–72. doi:10.1378/chest.14-0097
21. Subramanian S, Jayaraman G, Majid H, Aguilar R, Surani S. Influence of gender and anthropometric measures on severity of obstructive sleep apnea. Sleep Breath. 2012;16(4):1091–1095. doi:10.1007/s11325-011-0607-9
22. Mohsenin V. Gender differences in the expression of sleep-disordered breathing: role of upper airway dimensions. Chest. 2001;120(5):1442–1447. doi:10.1378/chest.120.5.1442
23. Liu Y, Zou J, Qian Y, et al. The association between obesity indices and obstructive sleep apnea is modified by age in a sex-specific manner. Sleep Breath. 2021;25(1):189–197. doi:10.1007/s11325-020-02083-4
24. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006–1014. doi:10.1093/aje/kws342
25. Honig E, Green A, Dagan Y. Gender differences in the sleep variables contributing to excessive daytime sleepiness among patients with obstructive sleep apnea. Sleep Breath. 2021;25(4):1837–1842. doi:10.1007/s11325-020-02276-x
26. Huang CJ, Hsu NW, Chen HC. Prevalence, dimensions, and correlates of excessive daytime sleepiness in community-dwelling older adults: the Yilan study, Taiwan. Ann Med. 2024;56(1):2352028. doi:10.1080/07853890.2024.2352028
27. Kolla BP, He JP, Mansukhani MP, Frye MA, Merikangas K. Excessive sleepiness and associated symptoms in the U.S. adult population: prevalence, correlates, and comorbidity. Sleep Health. 2020;6(1):79–87. doi:10.1016/j.sleh.2019.09.004
28. Thomas SJ, Booth JN 3rd, Jaeger BC, et al. Association of sleep characteristics with nocturnal hypertension and nondipping blood pressure in the CARDIA study. J Am Heart Assoc. 2020;9(7):e015062. doi:10.1161/JAHA.119.015062
29. Song GQ, Wang DL, Wu HM, et al. Two effective clinical prediction models to screen for obstructive sleep apnoea based on body mass index and other parameters. Sleep Breath. 2022;26(2):923–932. doi:10.1007/s11325-021-02347-7
30. Luo M, Zheng HY, Zhang Y, et al. A nomogram for predicting the likelihood of obstructive sleep apnea to reduce the unnecessary polysomnography examinations. Chin Med J. 2015;128(16):2134–2140. doi:10.4103/0366-6999.162514
31. Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812–821. doi:10.1097/ALN.0b013e31816d83e4
32. Chen R, Liu W, Cheng J, et al. The No-apnea score vs. the other five questionnaires in screening for obstructive sleep apnea-hypopnea syndrome in patients with cerebral infarction. J Thorac Dis. 2019;11(10):4179–4187. doi:10.21037/jtd.2019.09.75
33. Duarte RLM, Magalhaes-da-silveira FJ, Oliveira ESTS, Rabahi MF, Mello FCQ, Gozal D. Predicting obstructive sleep apnea in patients with insomnia: a comparative study with four screening instruments. Lung. 2019;197(4):451–458. doi:10.1007/s00408-019-00232-5
34. Hong C, Chen R, Qing S, et al. Validation of the NoSAS score for the screening of sleep-disordered breathing: a hospital-based retrospective study in China. J Clin Sleep Med. 2018;14(2):191–197. doi:10.5664/jcsm.6930
35. Natsios G, Pastaka C, Vavougios G, et al. Age, body mass index, and daytime and nocturnal hypoxia as predictors of hypertension in patients with obstructive sleep apnea. J Clin Hypertens. 2016;18(2):146–152. doi:10.1111/jch.12645
36. Appleton SL, Vakulin A, Martin SA, et al. Hypertension is associated with undiagnosed osa during rapid eye movement sleep. Chest. 2016;150(3):495–505. doi:10.1016/j.chest.2016.03.010
37. Zheng Z, Sun X, Chen R, et al. Comparison of six assessment tools to screen for obstructive sleep apnea in patients with hypertension. Clin Cardiol. 2021;44(11):1526–1534. doi:10.1002/clc.23714
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.