")
Back to Journals » Clinical Ophthalmology » Volume 18
Oral Azithromycin versus Oral Doxycycline in the Treatment of Meibomian Gland Dysfunction: A Systematic Review and Meta-Analysis
Authors Bukhari ZM, Alsudais AS, Bshnaq AG , Alshabri M, Alqurashi AR, Alghamdi AM, Alshehri OA, Bashrahil B, Alghamdi S
Received 18 July 2024
Accepted for publication 7 November 2024
Published 21 November 2024 Volume 2024:18 Pages 3353—3363
DOI https://doi.org/10.2147/OPTH.S480719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ziad M Bukhari,1,2 Ali S Alsudais,2,3 Abdullatif Ghazi Bshnaq,2,3 Meshari Alshabri,4 Ahmed Ruwaybih Alqurashi,4 Amer M Alghamdi,5 Omar A Alshehri,6,7 Bader Bashrahil,2,3 Saeed Alghamdi1– 3
1Department of Ophthalmology, Ministry of the National Guard-Health Affairs, Jeddah, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia; 3College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 4Department of Ophthalmology, King Abdullah Medical City, Makkah, Saudi Arabia; 5Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 6Jeddah Eye Hospital, Ministry of Health, Jeddah, Saudi Arabia; 7King Khalid Eye Specialist Hospital, Riyadh, Saudi Arabia
Correspondence: Ziad M Bukhari, Email [email protected]
Purpose: The first-line treatment approach of Meibomian gland dysfunction (MGD) comprises conservative management, but antibiotics with anti-inflammatory properties are recommended in severe or persistent cases. Oral doxycycline and oral azithromycin are commonly used antibiotics for managing MGD. However, a systematic review and meta-analysis comparing their efficacy and safety is needed.
Patients and Methods: This study adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and included randomized controlled trials (RCTs) focusing on patients with MGD. The primary outcomes assessed were symptom score, sign score, and overall clinical response. Adverse events were also evaluated. Multiple databases were comprehensively searched, and data extraction and quality assessment were performed by two independent authors.
Results: Four trials and a quasi-experimental study involving 612 participants/eyes were included. Meta-analysis showed a statistically significantly lower mean sign score in the oral azithromycin group than in the doxycycline group. However, one RCT reported a lower mean symptom score in the doxycycline group. No significant differences were found in the means of total scores between the two groups. Systemic adverse events such as nausea, abdominal cramps, decrease in appetite, and diarrhea were more prevalent in the doxycycline group.
Conclusion: The systematic review and meta-analysis suggest that oral azithromycin may be more effective in reducing signs of MGD than oral doxycycline. However, the results regarding symptom scores and total scores were inconclusive. Azithromycin also demonstrated a better safety profile with fewer gastrointestinal adverse events. Further research is needed to determine the optimal antibiotic treatment for MGD.
Keywords: Meibomian gland dysfunction, azithromycin, doxycycline
A Letter to the Editor has been published for this article.
Introduction
Ocular surface disease (OSD) is defined by an insufficiency of tears, an unsteady tear film caused by inferior tear quality, damage to the surface of the eye, and/or symptoms such as discomfort, stinging, the feeling of a foreign object in the eye, and dryness. It is one of the most common reasons for visiting an ophthalmologist according to the American Academy of Ophthalmology (AAO).1 The meibomian gland plays a vital role in maintaining the health of the ocular surface, preventing the evaporation of the tear film by secreting a lipid and protein mixture.2,3 Meibomian gland dysfunction (MGD) is one of the most common causes of OSD. It is characterized by obstruction of the terminal duct and/or quantitative/qualitative changes in the secretions of the meibomian glands.4 The subsequent accumulation of meibum is responsible for inflammation and increased bacterial colonization of the lid margins, resulting in both signs and symptoms of OSD.1
The first-line therapy in most MGD cases is conservative management, including the use of warm compresses to promote adequate meibum secretion, mechanical eyelid massage, cleansing with shampoo and cotton buds to remove excess debris, and the use of artificial tears to lubricate the ocular surface.5,6 However, in severe and refractory cases, antibiotics (topical and systemic) with anti-inflammatory properties are recommended as second-line therapy.7 Doxycycline, which is a longer-acting variant of tetracycline, is often recommended for its ability to reduce inflammation and suppress matrix metalloproteinases. However, poor adherence due to its longer duration of use and frequent gastrointestinal adverse effects are considered significant limitations.8 Azithromycin, on the other hand, works by inhibiting pro-inflammatory cytokines and is potent against gram-negative microorganisms. It has anti-inflammatory properties and has been reported to have a longer tissue half-life and lower frequency of gastrointestinal adverse events than doxycycline making it an excellent alternative to doxycycline for treating MGD.9
Although previous studies have compared the efficacy of oral doxycycline and oral azithromycin in managing MGD, to the best of our knowledge, the topic has not been systematically reviewed thus far. Therefore, this article aimed to systematically review and perform a meta-analysis of the available evidence comparing the efficacy and safety of oral doxycycline and oral azithromycin in managing MGD.
Materials and Methods
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines throughout its planning, conduct, and reporting (as shown in Supplementary file).10 Additionally, the study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the identifier 447891.
Eligibility Criteria
The study selection process involved a comprehensive systematic review of relevant randomized controlled trials (RCTs) focusing on patients with MGD. The inclusion criteria encompassed RCTs that specifically investigated the use of oral azithromycin as an intervention in comparison to oral doxycycline in managing patients with MGD with no improvement on conservative or topical management. Conversely, studies employing topical azithromycin as the main intervention were excluded from consideration. The primary outcomes of interest in this review included symptom score, sign score, and total score of MGD. Participants in the studies answered a questioner to assess symptom score, subjective score, based on categorical scale from 0 to 3. The questioner evaluated the symptoms of itchiness, burning sensation, foreign body sensation, dryness, and swelling of eyelid. Sign score was evaluated objectively also on a 4-points categorical scale by the examiner. Seven signs were evaluated that include meibomian secretion, plugged gland orifices, injection of conjunctiva, redness of lid margin, debris of lid margin, tear break up time, and staining of corneal surface by fluorescein. The sum of the sign and symptom scores calculated to for the total score. These outcomes were evaluated to assess the efficacy of oral azithromycin versus oral doxycycline in managing MGD. Additionally, gastrointestinal adverse events were appraised as a secondary outcome of interest.
Search Strategy
A systematic search of relevant literature was performed using the following databases: PubMed, the Cochrane Library (including clinical trials in CENTRAL), Scopus, the Directory of Open Access Journals, and ClinicalTrials.gov. The search included the period from the inception of each database to 4 July 2023. The search terms used included “meibomian gland dysfunction”, “meibomian gland disease”, “blepharitis”, “meibomianitis”, “meibomitis”, “ocular rosacea”, “azithromycin”, “macrolides”, “doxycycline”, and “tetracyclines” to identify studies that met the inclusion criteria. In addition, the reference lists of included studies were manually checked to identify any additional relevant articles.
Study Selection and Data Extraction
Two authors independently reviewed the identified articles for eligibility based on the predefined inclusion and exclusion criteria. Any disagreements were resolved through discussion and consensus. Following the study selection process, the two authors independently performed data extraction from the included studies. A standardized data extraction form was used to capture relevant information. The extracted data included study characteristics (author, year), participant demographics (sample size, age, gender), intervention details (dose, duration, frequency), outcomes measured (efficacy measures), and any reported adverse events. Any discrepancies in data extraction were resolved through discussion and consensus between the two authors.
Quality Assessment and Certainty of Evidence
The assessment of potential bias within the included studies was conducted using the Cochrane Risk of Bias 2 (RoB2) tool for RCTs and the Joanna Briggs Institute (JBI) tool for quasi-experimental studies.11,12 Two independent authors, namely A.B. and Z.B., undertook the responsibility of assessing the risk of bias for each study. The process of evaluation of the quality of evidence for each outcome was based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria.13 The utilization of the GRADE instrument, a method endorsed by the Cochrane Collaboration, facilitated a comprehensive assessment of evidence quality and the grading of recommendation strength within the studies included in the meta-analysis.14 This systematic evaluation encompassed various crucial features, including research design, consistency, indirectness, heterogeneity, imprecision, publication bias, and other relevant characteristics of the papers incorporated into this systematic review. Subsequently, the quality of evidence was categorized into distinct levels, namely high, moderate, low, or very low, based on the overall assessment conducted in accordance with the GRADE framework.13,14
Meta-Analysis
The treatment effect was computed utilizing the Review Manager 5 (RevMan 5, version 5.3, Cochrane Collaboration) software. Statistical significance was set at a 95% confidence level, with a threshold P-value of 0.05. To evaluate the presence of statistical heterogeneity within the included studies, the I2 statistic was employed, which quantifies the proportion of total variation attributable to heterogeneity. Risk ratios were employed to express the effect of the intervention on dichotomous outcomes, while standardized mean difference was utilized to calculate the intervention effect for continuous outcomes. To account for potential variability across the included studies, a random effects model was employed.
Results
After conducting an extensive and systematic search, we identified a total of 2,209 reports from five different databases. Out of this initial pool, 2,199 reports were excluded as they did not meet the predetermined eligibility criteria. Subsequently, an additional five reports were excluded due to issues such as limited accessibility or variations in the route of administration. Eventually, our selection process led us to include five reports that were derived from four distinct trials and a quasi-experimental study, as visually depicted in Figure 1.9,15–18
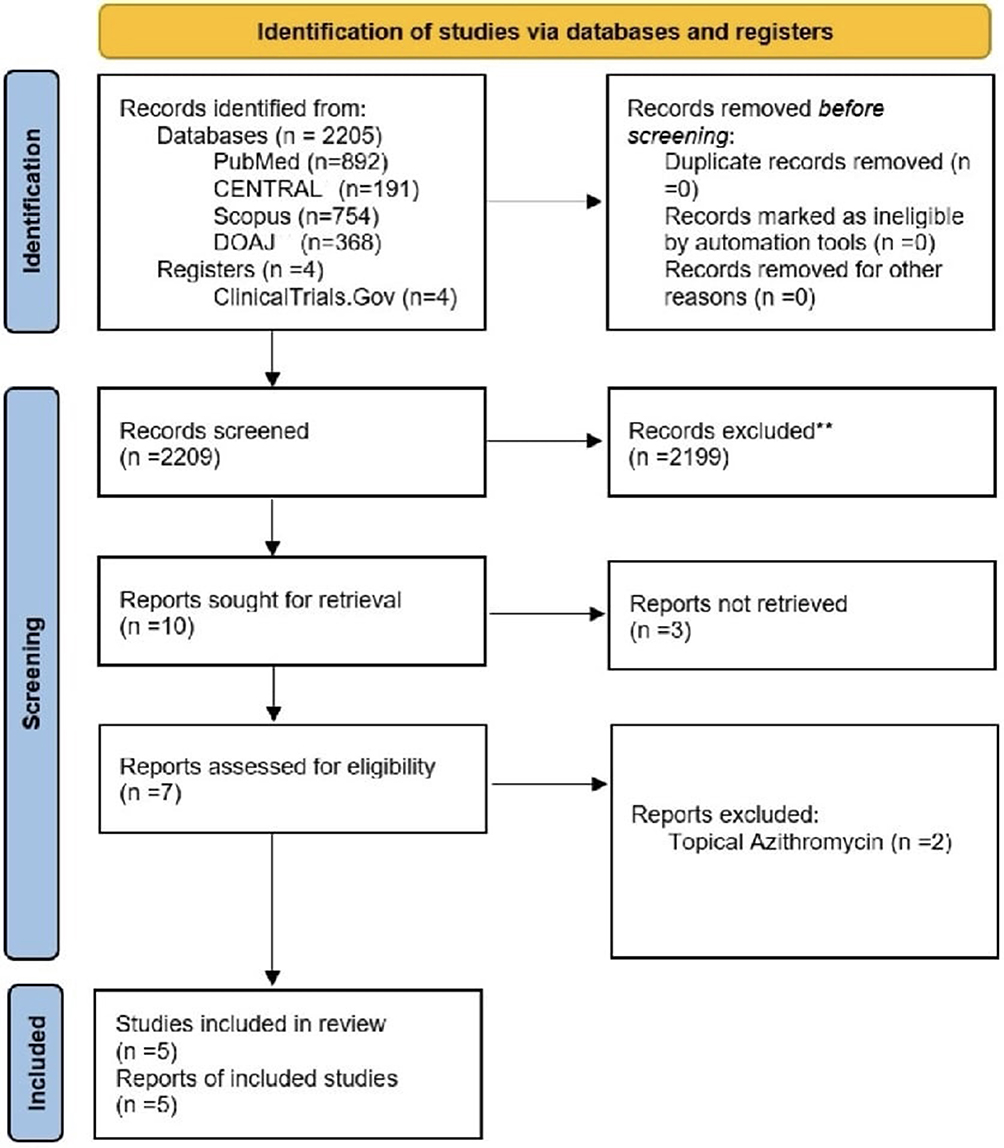 |
Figure 1 Study flow diagram. CENTRAL, Cochrane Central Register of Controlled Trial; DOAJ, Directory of Open Access Journals. |
Study Characteristics
The study encompassed a total of four trials and a quasi-experimental study, involving a cohort of 612 participants corresponding to 612 eyes.9,15–18 The mean age of the trial participants varied across the trials, spanning 40.25 years to 61.45 years. A total of 297 participants were male, accounting for 48.52% of the entire participant pool. The treatment regimen for the oral azithromycin and doxycycline varied slightly among the included studies.9,15–18 For more comprehensive information on the attributes and particulars of the included studies, as shown in Table 1.
 |
Table 1 Detailed Characteristics of the Included Studies |
Risk of Bias Assessment
Two independent reviewers, namely A.B. and Z.B, systematically employed the RoB 2 tool11 and the JBI criteria12 to individually appraise the potential sources of bias in the eligible RCTs and quasi-experimental study.9,15–18 Any discrepancies were solved by discussion till an agreement between reviewers was reached. Three of the four trials in this investigation exhibited a discernibly high risk of bias, and one trial had low risk as visually depicted in Figures 2 and 3. Additionally, the quasi-experimental study assessed with the JBI criteria12 indicated a low risk of bias.
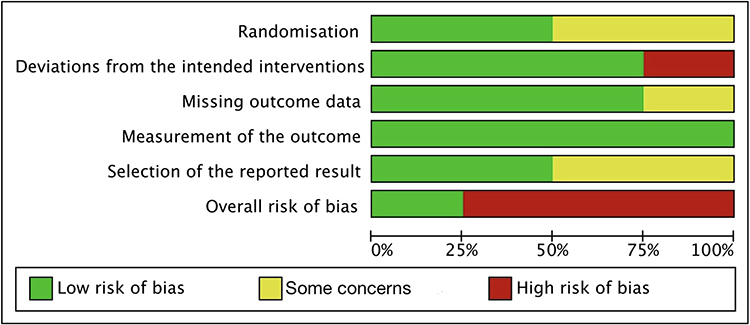 |
Figure 2 Risk of bias graph. |
 |
Figure 3 Risk of bias summary. |
Efficacy Based on Sign Score
In terms of evaluating the efficacy outcomes, four studies incorporated sign scores as a measured parameter.15–18 Among these studies, two RCTs provided compelling evidence of a lower mean sign score within the oral azithromycin group.15,17 This finding yielded a statistically significant pooled estimate favoring the azithromycin group over the doxycycline group (standardized mean difference [SMD] = −0.47, 95% confidence interval [CI] −0.66 to −0.29, p < 0.000001, I2 = 92%); see Figure 4. (Very low certainty of evidence; see Table 2).
 |
Table 2 Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Evidence Profile |
 |
Figure 4 Forest plot of sign scores. Cl, confidence interval; SD, standard deviation. |
To address the considerable heterogeneity observed, a sensitivity analysis was conducted, excluding the influence of the study by Benedetti & Vaiano. This resulted in a reduced but still statistically significant level of heterogeneity (I2 = 77%), as visually depicted in (Figure S1). Further efforts were made to investigate the underlying cause of the notable heterogeneity, leading to a subgroup analysis based on the duration of follow-up. The results of this analysis are presented in (Figure S2), revealing that at the 6-month follow-up, there was no significant difference (p = 0.59) in sign scores between the administration of doxycycline and azithromycin. However, when considering patients with a follow-up duration of less than 6 months, azithromycin demonstrated a statistically significant (p < 0.00001) advantage over doxycycline in terms of sign scores. The overall analysis showed a statistically significant (p < 0.0001) difference favoring azithromycin over doxycycline (Figure S2).
Efficacy Based on Symptom Score
Four articles were included in the analysis, with symptom score serving as one of the primary efficacy outcomes.15–18 Of particular interest, one of the RCTs17 reported a notably lower mean symptom score in the doxycycline group compared to the symptom scores observed in the remaining three studies. This discrepancy yielded a statistically significant pooled estimate that favored the doxycycline group (SMD = 0.24, 95% CI 0.05 to 0.42, p = 0.01, I2 = 91%) as evidenced by the data presented in Figure 5. (Very low certainty of evidence; see Table 1).
 |
Figure 5 Forest plot of symptom scores. Cl, confidence interval; SD, standard deviation. |
To address the observed heterogeneity, a sensitivity analysis was conducted, excluding the influence of the Benedetti & Vaiano study. Following the exclusion of this study and the subsequent sensitivity analysis, no significant difference in symptoms between the doxycycline and azithromycin groups was observed. However, it is important to note that a moderate level of heterogeneity (I2 = 69%) persisted in the results (Figure S3).
Efficacy Based on Total Score
The meta-analysis incorporated four RCTs that computed the total scores of MGD.9,15–17 The findings revealed no significant differences in the mean total scores between the two groups at the final follow-up assessment (SMD = −0.07, 95% CI −0.26 to 0.12, p = 0.50, I2 = 73%); see (Figure S4). (Low certainty of evidence; see Table 1).
Adverse Events
In the present study, gastrointestinal adverse events were carefully monitored across the four studies throughout all follow-up periods.15–18 The most frequently reported gastrointestinal adverse event was nausea, which exhibited a higher incidence in the doxycycline groups. The pooled estimates consistently favored the azithromycin groups, with a statistically significant difference observed (SMD = 0.61, 95% CI 0.45 to 0.84, p = 0.002, I2 = 0%) as seen in Figure 6. Similarly, abdominal cramps (SMD = 0.51, 95% CI 0.36 to 0.72, p = 0.0001, I2 = 0%), decrease in appetite (SMD = 0.43, 95% CI 0.28 to 0.68, p = 0.0003, I2 = 0%), and diarrhea (SMD = 0.56, 95% CI 0.36 to 0.86, p = 0.008, I2 = 0%) were also found to be more favorable towards the azithromycin groups (Figure 6). Overall, the pooled estimates demonstrated a consistent preference for the azithromycin group in terms of all gastrointestinal adverse events (SMD = 0.54, 95% CI 0.45 to 0.65, p < 0.00001, I2 = 0%); see (Figure 6).
 |
Figure 6 Forest plot of adverse events. Cl, confidence interval; SD, standard deviation. |
Discussion
MGD is a prevalent condition that contributes to OSD via obstruction and alterations in the meibomian gland secretions.19 While conservative management is the primary approach for MGD treatment, antibiotics with anti-inflammatory properties are recommended for severe cases.5 Oral doxycycline and oral azithromycin are commonly prescribed antibiotics for managing MGD.8,20 In this systematic review and meta-analysis, we aimed to compare the efficacy of these two antibiotics in the treatment of MGD. Our findings suggest that oral azithromycin may be more effective in reducing signs of MGD compared to oral doxycycline. However, the results regarding symptom scores and total scores were inconclusive. Furthermore, azithromycin demonstrated a better safety profile, with fewer gastrointestinal adverse events. These results highlight the potential of azithromycin as a treatment option for MGD, but further research is needed to establish the optimal antibiotic therapy for this condition.
Our findings suggest that the use of azithromycin results in greater overall improvement in the signs of MGD compared to doxycycline, according to the sign scores presented in Figure 3. Specifically, studies by Kashkouli et al and Benedetti & Vaiano demonstrated that azithromycin led to greater improvement in conjunctival redness and corneal staining, in addition to MG secretion in the work by Benedetti & Vaiano. However, it is important to note the high heterogeneity in the results (I2 = 92%), indicating substantial variability among the studies. To address this heterogeneity, a sensitivity analysis was conducted by excluding the effect of the study by Benedetti & Vaiano, resulting in a lower but still significant level of heterogeneity (I2 = 77%) as shown in (Figure S1). Further efforts were made to explore the source of high heterogeneity, leading to a subgroup analysis based on the duration of follow-up. (Figure S2) depicts the results of this analysis, showing that at the 6-month follow-up, there was no significant difference in sign scores between doxycycline and azithromycin. However, when evaluating patients with a follow-up duration of less than 6 months, azithromycin demonstrated a statistically significant superiority over doxycycline in terms of sign scores (Figure S2). This early efficacy of azithromycin (< 6 months) was observed only by Benedetti & Vaiano (who assessed patients after 3 months of treatment) and Kashkouli et al (who assessed patients after 2 months). These findings suggest that azithromycin has an early and potentially more potent anti-inflammatory effect on the signs of MGD. Furthermore, this early effect appears to be maintained, and azithromycin remains as effective as doxycycline after 6 months of treatment.
In contrast, when examining the symptom score, our findings indicate a statistically significant preference for the doxycycline group. This result may be attributed to the influence of Benedetti & Vaiano’s RCT on the overall analysis. However, upon removing the effect of this RCT and conducting a sensitivity analysis (Figure S3), no significant difference between the doxycycline and azithromycin groups in terms of symptoms was observed. Nevertheless, a high level of heterogeneity remained in the results (I2 = 69%). This heterogeneity can be explained by variations in the mean symptom scores reported in the Kashkouli et al and Benedetti & Vaiano studies. Specifically, the symptom score for MGD was better in the azithromycin group in the Kashkouli study, while in the Benedetti & Vaiano study, doxycycline demonstrated superior symptom scores. However, it is important to note that these differences were not statistically significant in the original articles.
When considering the total score, which combines both the signs and symptoms of MGD, azithromycin and doxycycline were found to exhibit comparable effectiveness. However, it is important to note the high degree of heterogeneity in the results (I2 = 91%), which is likely due to the variations in the sign scores observed in the azithromycin group during the early follow-up periods.
Previous systematic reviews have also examined the efficacy of both oral and topical forms of azithromycin in the treatment of MGD.21,22 Specifically, topical azithromycin has been reported to potentially yield superior effects compared to oral azithromycin in improving tear break-up time and corneal staining. However, when considering the overall effects on MGD signs and symptoms, both oral and topical forms exhibit comparable efficacy and that topical azithromycin is not widely available in all health care institutions in comparison to the oral form.22,23 It should be noted, however, that oral doxycycline may require a longer therapeutic course to achieve a similar level of effectiveness.8,22 The treatment regimen for the oral azithromycin varied between 5 to 21 days among the included studies with a slightly different doses.9,15–18 However, the doxycycline groups were treated for longer duration compared to the azithromycin groups in all the included studies.9,15–18
Oral doxycycline has been documented to elicit systemic adverse events when administered for the treatment of MGD, including gastrointestinal, dermatological, and allergic events.23 Conversely, oral azithromycin has been reported as a well-tolerated medication with a lower incidence of systemic side effects.24 Consequently, it comes as no surprise that our study revealed a reduced occurrence of systemic adverse events in the azithromycin group compared to the doxycycline group, with consistent findings across the study population. Additionally, the subgroup analysis focusing on gastrointestinal side effects demonstrated a similarly diminished occurrence in the azithromycin group.
Despite the high heterogeneity observed in this meta-analysis, it is important to note that all the studies included in the analysis exhibited comparable baseline characteristics and low risk of bias and employed similar assessment tools and scores for measuring the impact of the intervention on MGD. The underlying causes of this observed heterogeneity in the assessment scores remain incompletely understood; however, it is plausible that variations in therapeutic dosage, frequency, and duration across the included studies may have contributed to the pooled results being influenced. Furthermore, another factor that could have potentially influenced the results of our analysis is the early effect of azithromycin on the sign score in the initial 2–3 months, as demonstrated in studies by Kashkouli et al and Bendeti et al. These studies provide evidence of a potential temporal variation in the efficacy of azithromycin treatment for MGD.
As mentioned before, MGD is a chronic disease that is usually managed with conservative treatment such as lid hygiene, lubrication, or warm compressors as first line therapy.5 There are multiple treatment options that can be used as an adjunctive treatment if the oral administration of antibiotics is contraindicated such as intraductal meibomian gland probing, topical N-acetyl-cysteine, omega-3 essential fatty acids, or topical cyclosporine A.25 A new treatment approach that worth mentioning is the intense pulsed light (IPL), which work as adjunctive treatment to improve the signs and symptoms of MGD, and can be used if oral antibiotics are contraindicated.26 IPL can also be combined with the oral doxycycline to decrease the recurrence of chalazion and improve the MGD.27 However, no studies have mentioned the use of oral azithromycin with IPL treatment.
Several limitations of our study should be acknowledged. First, the inclusion of a limited number of studies is a notable constraint. This arises from the fact that antibiotic use is not considered a first-line treatment in the management of MGD and is not widely adopted in clinical practice. Consequently, the availability of eligible studies meeting our inclusion criteria was limited, potentially limiting the generalizability of our findings. Furthermore, a significant limitation is the high level of heterogeneity observed among the included studies. This heterogeneity may be attributed to methodological disparities and variations in the study design, intervention protocols, and outcome measures employed across the studies. The resulting inconsistency in the pooled results necessitates caution when interpreting and extrapolating the findings. However, it is important to note that we conducted a thorough investigation to identify potential sources of heterogeneity and explore their underlying causes. Despite these limitations, our study provides valuable insights into the efficacy of antibiotics in the management of MGD. Nevertheless, future research endeavors should aim to address these limitations by conducting larger-scale studies with a more diverse range of participants, standardized protocols, and consistent outcome measures. Such efforts would contribute to the robustness and generalizability of the findings, thereby enhancing our understanding of the role of antibiotics in the treatment of MGD.
Conclusion
This systematic review and meta-analysis sought to evaluate the efficacy and safety of oral azithromycin in comparison to those of oral doxycycline for the treatment of MGD. The findings of this study indicate that oral azithromycin exhibits promise in managing the signs and symptoms associated with MGD. While no statistically significant difference was observed in final efficacy between the two treatments, oral azithromycin demonstrated a shorter duration of treatment and a more favorable adverse effects profile, which could improve patient compliance. However, it is imperative to conduct further investigations with larger sample sizes to obtain a more comprehensive understanding of the long-term outcomes pertaining to the use of oral azithromycin in MGD. In conclusion, this study contributes valuable evidence to the existing literature, providing insights that help optimize the treatment approach for MGD patients.
Approval Date of Registry and the Registration No. of the Study/Trial
Protocol registration: PROSPERO- CRD42023447891, Date: 31/07/2023.
Abbreviations
OSD, Ocular surface disease, MGD, Meibomian gland dysfunction, PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses, RCTs, randomized controlled trials.
Ethical Approval and Consent to Participate
The present investigation represents a systematic review and meta-analysis, in which the original articles have adhered to the ethical principle of obtaining informed consent. No new data or patient information was collected during our review. Additionally, both King Abdulaziz Medical City (KAMC) and King Saud bin Abdulaziz University for Health Sciences (KASUHS) adhere to the guidelines set forth by the King Abdullah International Medical Research Center (KAIMRC), which does not mandate IRB approval for literature reviews, systematic reviews, or meta-analyses. Hence, no ethical approval was required.
Disclosure
The authors declare no competing interests.
References
1. Wladis EJ, Bradley EA, Bilyk JR, Yen MT, Mawn LA. Oral antibiotics for meibomian gland-related ocular surface disease. Ophthalmology. 2016;123(3):492–496. doi:10.1016/j.ophtha.2015.10.062
2. Arita R, Suehiro J, Haraguchi T, et al. Topical diquafosol for patients with obstructive meibomian gland dysfunction. Br J Ophthalmol. 2013;97(6):725–729. doi:10.1136/bjophthalmol-2012-302668
3. Ding J, Kam WR, Dieckow J, Sullivan DA. The influence of 13- cis retinoic acid on human meibomian gland epithelial cells. Invest Ophthalmol Vis Sci. 2013;54(6):4341. doi:10.1167/iovs.13-11863
4. Bron AJ, Tiffany JM. The contribution of meibomian disease to dry eye. The Ocular Surface. 2004;2(2):149–164. doi:10.1016/S1542-0124(12)70150-7
5. Romero JM, Biser SA, Perry HD, et al. Conservative treatment of meibomian gland dysfunction. Eye Contact Lens. 2004;30(1):14–19. doi:10.1097/01.ICL.0000095229.01957.89
6. Guillon M, Maissa C, Wong S. Eyelid margin modification associated with eyelid hygiene in anterior blepharitis and meibomian gland dysfunction. Eye Contact Lens. 2012;38(5):319–325. doi:10.1097/ICL.0b013e318268305a
7. Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2011;52(4):2050. doi:10.1167/iovs.10-6997g
8. Foulks GN, Borchman D, Yappert M, Kakar S. Topical azithromycin and oral doxycycline therapy of meibomian gland dysfunction: a comparative clinical and spectroscopic pilot study. Cornea. 2013;32(1):44–53. doi:10.1097/ICO.0b013e318254205f
9. Upaphong P, Tangmonkongvoragul C, Phinyo P. Pulsed oral azithromycin vs 6-week oral doxycycline for moderate to severe meibomian gland dysfunction: a randomized clinical trial. JAMA Ophthalmol. 2023;141(5):423. doi:10.1001/jamaophthalmol.2023.0302
10. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372. doi:10.1136/BMJ.N71
11. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ;2019. l4898. doi:10.1136/bmj.l4898
12. Barker TH, Stone JC, Sears K, et al. Revising the JBI quantitative critical appraisal tools to improve their applicability: an overview of methods and the development process. JBI Evidence Synth. 2023;21(3):478–493. doi:10.11124/JBIES-22-00125
13. Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–406. doi:10.1016/j.jclinepi.2010.07.015
14. Cochrane Training. Chapter 14: completing ‘Summary of findings’ tables and grading the certainty of the evidence. Available from: https://training.cochrane.org/handbook/current/chapter-14.
15. Kashkouli MB, Fazel AJ, Kiavash V, Nojomi M, Ghiasian L. Oral azithromycin versus doxycycline in meibomian gland dysfunction: a randomised double-masked open-label clinical trial. Br J Ophthalmol. 2015;99(2):199–204. doi:10.1136/bjophthalmol-2014-305410
16. Singh H, Nagpal H, Sidhu T, Goyal M. A comparative study between the efficacy of oral azithromycin versus the efficacy of oral doxycycline over 6 months in patients of meibomian gland dysfunction. Int J Med Res Prof. 2022;8:86–92.
17. De Benedetti G, Vaiano A. Oral azithromycin and oral doxycycline for the treatment of Meibomian gland dysfunction: a 9-month comparative case series. Indian J Ophthalmol. 2019;67(4):464. doi:10.4103/ijo.IJO_1244_17
18. Yousuf W, Humayun F, Janjua TA, Khan TA, Sarfraz MH, Mehboob MA. Comparison between efficacy and safety of oral azithromycin (250mg) vs oral doxycycline (100mg) in treatment of meibomian gland dysfunction(Mgd). PAFMJ. 2023;73(SUPPL–2):S312–315. doi:10.51253/pafmj.v73i3.8815
19. Foulks GN, Bron AJ. Meibomian gland dysfunction: a clinical scheme for description, diagnosis, classification, and grading. The Ocular Surface. 2003;1(3):107–126. doi:10.1016/S1542-0124(12)70139-8
20. Igami TZ, Holzchuh R, Osaki TH, Santo RM, Kara-Jose N, Hida RY. Oral azithromycin for treatment of posterior blepharitis. Cornea. 2011;30(10):1145–1149. doi:10.1097/ICO.0b013e318207fc42
21. Ahmad A, Rehman M. Comparative study evaluating the efficacy of topical azithromycin versus oral doxycycline in the treatment of meibomian gland dysfunction. J Pak Med Assoc. 2023;73(05):995–999. doi:10.47391/JPMA.6732
22. Tao T, Tao L. Systematic review and meta-analysis of treating meibomian gland dysfunction with azithromycin. Eye. 2020;34(10):1797–1808. doi:10.1038/s41433-020-0876-2
23. Aly Zaky M, Galal Zaky A, Fayez Elsawy M, Fatehy Shehata K, Samy Abd Elaziz M. Efficacy of topical azithromycin versus systemic doxycycline in treatment of meibomian gland dysfunction. Journal of Ophthalmology. 2023; 2023:1–7.
24. Bakar Ö, Demirçay Z, Gürbüz O. Therapeutic potential of azithromycin in rosacea. Int J Dermatol. 2004;43(2):151–154. doi:10.1111/j.1365-4632.2004.01958.x
25. Qiao J, Yan X. Emerging treatment options for meibomian gland dysfunction. Clin Ophthalmol. 2013;7:1797–1803. doi:10.2147/OPTH.S33182
26. Smith J, Doe A. Efficacy of intense pulsed light therapy on signs and symptoms of dry eye disease: a meta-analysis and systematic review. J Ophthalmol. 2023;45(3):123–134.
27. Yoon H-J, Moon JY, Yoon KC. Efficacy of combined doxycycline and intense pulsed light therapy for the management of intractable recurrent chalazion. Front Med. 2024;11:1454049. doi:10.3389/fmed.2024.1454049
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.