")
Back to Journals » Clinical Ophthalmology » Volume 18
Outcomes of Micropulse Laser Trabeculoplasty Compared to Selective Laser Trabeculoplasty: A Systematic Review and Meta-Analysis
Authors Zhu D, Shah PP , Zhang C, Wong A, Bouaziz M, Barmas-Alamdari D, Mootz J, Yu A, Tirsi A , Tello C
Received 24 May 2024
Accepted for publication 26 July 2024
Published 6 August 2024 Volume 2024:18 Pages 2205—2215
DOI https://doi.org/10.2147/OPTH.S476257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Daniel Zhu,1,2,* Paras P Shah,1,2,* Charles Zhang,3 Amanda Wong,4 Michael Bouaziz,1,2 Daniel Barmas-Alamdari,1,2 Joseph Mootz,1,2 Austin Yu,5 Andrew Tirsi,1,2 Celso Tello1,2
1Department of Ophthalmology, Northwell Health Eye Institute, Great Neck, New York, 11021, USA; 2Manhattan Eye, Ear, & Throat Hospital, New York, New York, 10065, USA; 3Department of Ophthalmology, Ross Eye Institute, Jacobs School of Medicine and Biomedical Sciences, State University of New York, University at Buffalo, Buffalo, NY, 14203, USA; 4Department of Ophthalmology, New York Eye and Ear Infirmary, New York, New York, 10003, USA; 5Department of Ophthalmology, Drexel University College of Medicine, Philadelphia, PA, 19129, USA
*These authors contributed equally to this work
Correspondence: Daniel Zhu, Department of Ophthalmology, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, 600 Northern Blvd., Suite 214, Great Neck, NY, 11021, USA, Email [email protected]
Purpose: To perform a meta-analysis and systematic review to compare the efficacy and complications of micropulse laser trabeculoplasty (MLT) and selective laser trabeculoplasty (SLT) in adult patients with open-angle glaucoma (OAG) and ocular hypertension (OHT).
Methods: We performed a systematic review utilizing PubMed, Embase, and Scopus, on April 8, 2024. Meta-analyses were performed for the mean change in intraocular pressure (IOP) at one-month, six-month, and one-year follow-up visits, rate of IOP spikes (> 5 mmHg increase from the pre-procedure baseline IOP), rate of treatment failure (< 20% or < 3 mmHg reduction in IOP or requiring additional medications or procedures), and mean change in number of medications.
Results: Six studies, with a total of 593 eyes, were included: 283 underwent MLT, while 310 underwent SLT. A statistically significant difference in the efficacy of MLT versus SLT at one-month and six-month follow-ups was present, with SLT reducing IOP by 0.83 mmHg (95% CI: 0.20, 1.47; P = 0.01) more and 0.55 mmHg (95% CI: 0.02, 1.08; P = 0.04) more than MLT, respectively. At the one-year follow-up, there was no significant disparity in IOP reduction between SLT and MLT (WMD = 0.16; 95% CI: − 0.40, 0.71; P = 0.58). There was a significantly lower rate of IOP spikes in the MLT treatment group (RR = 0.37; 95% CI: 0.16, 0.89; P = 0.03). There was no statistically significant difference in the rate of treatment failures (RR = 1.05; 95% CI: 0.68, 1.62; P = 0.84) or number of topical medications reduced (WMD = 0.06; 95% CI: − 0.13, 0.26; P = 0.53).
Conclusion: While SLT may offer greater short-term reductions in IOP, it may be associated with more postoperative IOP spikes when compared to MLT. At one-year follow-up, there were no significant differences in IOP reduction or failure rates between the MLT and SLT groups.
Keywords: trabeculoplasty, micropulse, SLT, selective laser trabeculoplasty, glaucoma
Introduction
Glaucoma is a leading cause of irreversible vision loss globally, with the primary goal of intervention being to reduce intraocular pressure (IOP).1 The most common methods to achieve IOP reduction include topical medication drops and laser trabeculoplasty (LTP).2 In the 1970s, the first laser treatment introduced for open-angle glaucoma (OAG) and ocular hypertension (OHT) was argon laser trabeculoplasty (ALT). ALT involved inducing thermal damage to the trabecular meshwork (TM) to enhance the drainage of aqueous humor, thereby reducing IOP.3 In the 1990s, selective laser trabeculoplasty (SLT) was introduced, which preferentially targeted pigmented TM cells, thereby sparing adjacent tissues from thermal damage as in the case of ALT.4,5 Laser trabeculoplasty is increasingly being accepted as the standard of care for the initial management of OAG and OHT, with the Laser in Glaucoma and Ocular Hypertension (LiGHT) trial demonstrating that initial SLT, rather than medication therapy, has better long-term outcomes.6 More recently, a new method of LTP, micropulse laser trabeculoplasty (MLT), has emerged.7,8
Initially reported in 2005, MLT induces neither thermal nor cellular damage, as in the cases with ALT and SLT.7,8 It achieves this by fractionating a continuous laser beam into shorter pulses, allowing for the pigmented cells to cool during the interpulse periods, thereby preventing cellular and morphologic alterations to the TM.8 Studies comparing outcomes of MLT and SLT have shown that MLT can produce fewer IOP spikes and less pain than SLT.9–13 Studies have also reported on the efficacy of MLT at lowering IOP and reducing the number of drops compared to SLT, with conflicting results.9–11,13–16 While there are multiple studies on the topic, there is currently a lack of higher-level evidence directly comparing the efficacy and complications of MLT with those of SLT.17 To the best of our knowledge, no prior meta-analysis has pooled data from studies that directly compared MLT and SLT in patients with OAG and OHT, in order to compare their reductions in IOP and topical medications, IOP spikes, and failure rates.
Materials and Methods
Design
A systematic literature review was conducted utilizing the guidelines set forth by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Cochrane Handbook of Systematic Reviews of Interventions.18,19 We prospectively registered the study protocol in the international prospective register of systematic reviews (PROSPERO, CRD42024535238). This study only used previously published and publicly available data, so institutional review board approval was not required.
Search Strategy
A search was performed using the Pubmed, Scopus, and Embase databases, on April 8, 2024, for all articles to that date. Variations of the following terms were used in the search strategy: “trabeculoplasty”, “micropulse”, “glaucoma”, and “MLT.” Supplemental eTable 1 contains the detailed search strategy.
Article Selection
Articles were screened independently by authors DZ and PPS in two different phases: (1) screening of titles and abstracts and (2) screening of full texts. During first phase, articles were retained if they reported the outcomes of MLT and SLT in either the title or the abstract. If the focus of the article was ambiguous from just the title and abstract, the study was included for additional review in full-text screening.
During this second phase, specific inclusion and exclusion criteria were independently utilized by the authors to screen full-text articles. These criteria were: (1) the study compared outcomes of MLT and SLT in adult OAG or OHT patients; (2) the article reported on outcomes or complications including change in IOP, change in number of topical medications, rate of IOP spikes, and failure rates (3) the published language was English; (4) the study was a clinical trial, cohort study, or case-control study. The study was excluded if it: was a case report, review, meta-analysis, or conference abstract, contained non-human subjects, or was a duplicate.
Quality Assessment
Authors DZ and PPS utilized the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool and the revised Cochrane risk-of-bias tool for randomized trials (RoB 2) tool for nonrandomized comparative studies and randomized comparative studies, respectively, to determine the risk of bias.20,21 There are seven independent domains in the ROBINS-I risk of bias tool with each carrying anywhere from low-high risk that is assessed using set preset questions. The results of these questions together provide an overall assessment of risk. There are five domains in the RoB 2 tool, and similar to ROBINS-I, each domain carries anywhere from low-high risk, followed by an overall risk assessment. The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) framework was utilized to perform quality assessment.22
Data Extraction
Data from six studies was extracted by two authors (DZ, PS), with disagreements being solved through discussion. The following data were extracted: first author’s name, publication year, nation in which the study was conducted, sample size, duration of follow-up, MLT parameters, IOP change in MLT and SLT treatment groups, failure rates, IOP spike rates, and change in the number of topical medications. Failure was defined as a <20% or <3 mmHg reduction in IOP or requiring additional medications or procedures for IOP control.23 An IOP spike was defined as a >5 mmHg increase from the pre-intervention baseline IOP. PlotDigitizer was utilized to deduce data along with measures of variance if studies only reported outcomes in a graphical format (https://plotdigitizer.com/). For articles that solely reported pre- and post-treatment IOPs and corresponding standard deviations (SD), a mean difference was computed, and the SD was estimated as per the Cochrane Handbook.24,25
Statistical Analysis
The RevMan 5.4.1 software was utilized to perform meta-analyses of weighted mean differences (WMD) to compare change in IOP and number of topical medications between MLT and SLT.26 The six-week follow-up visit was used in one study which did not report data at one-month.9 For studies that compared the failure rates of MLT and SLT or the proportion of eyes with IOP spikes, a meta-analysis of risk ratios (RR) was performed. Due to expected heterogeneity from the differences in study protocols, follow-up durations, and differences in patient populations, random-effects models were utilized. Forest plots were used to visually represent the summary effect measure and confidence intervals (CI). Cochran’s Q and Higgins’ I2 were used to assess for heterogeneity. Cochran’s Q P of less than 0.1 and I2 greater than 40% were used as thresholds of significant heterogeneity. All statistical tests were conducted using a two-tailed approach, and a P-value of less than 0.05 was deemed statistically significant.
Publication Bias
RevMan 5.4.1 software was utilized to create a Begg’s funnel plot for each meta-analysis. However, regression tests for funnel plot asymmetry were not carried out in this meta-analysis, as it included only six studies. According to the Cochrane Handbook, these tests lack sufficient power when the number of studies is fewer than ten.24
Results
Search Results
A PRISMA chart for this analysis can be found in Figure 1.27 The complete search string (Supplemental eTable 1) resulted in 310 studies that were exported into Covidence, and one additional reference was identified through hand-searching of bibliographies. After 88 duplicates were removed, 223 studies remained. Following the title and abstract screening phase, 15 studies were left. In final step involving screening of full-texts, nine studies were further excluded (Supplemental eTable 2), resulting in a final total of six studies that remained.
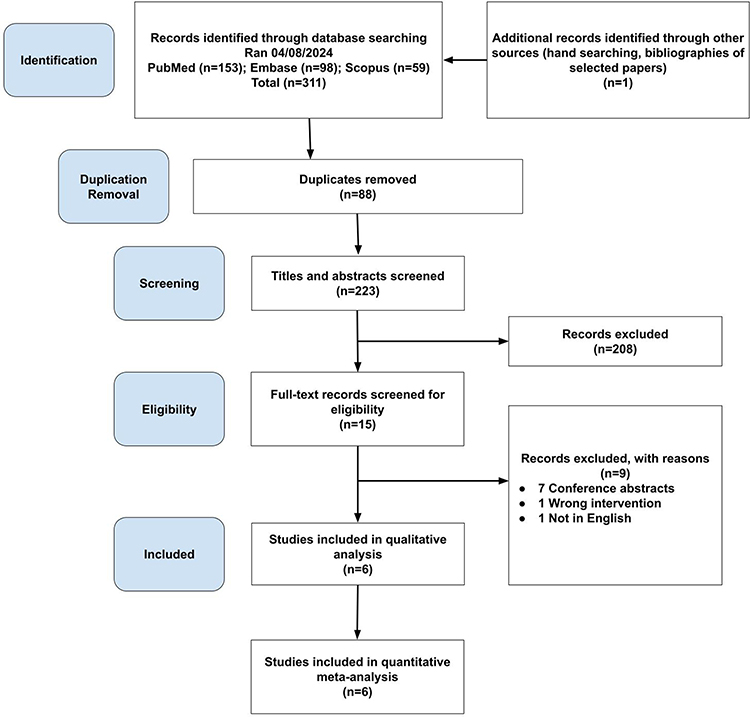 |
Figure 1 PRISMA flowchart for this meta-analysis. Abbreviation: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. |
Study Characteristics
Our final analysis included six studies, with the year of publication ranging from 2017–2023. Overall, 593 eyes were included: 283 underwent MLT and 310 underwent SLT. The studies were carried out in these nations: United States (4), Mexico (1), and Brazil (1). Four studies were retrospective, one was a nonrandomized prospective study, and one was an RCT. Studies included patients with OHT and several forms of OAG, including primary open angle (POAG), pseudoexfoliative (PXG), and pigmentary (PG). Two studies used MLT with a wavelength 577nm, while four studies used a wavelength of 532nm. In regard to other MLT parameters, all studies had a spot size of 300μm, duration of 300ms, 15% duty cycle, and lasered 360° of the angle. For SLT parameters, four studies performed 360° SLT, one performed 180° SLT, and one performed >180° SLT. The energy used for SLT ranged from 0.3mJ to 2.0mJ with five studies titrating to the level of visible bubble formation and one study titrating to the level just below visible bubbles. Table 1 provides detailed characteristics of all included studies. Supplemental eTable 3 shows the parameters for SLT that were used in each study.
 |
Table 1 Summary of Included Studies |
Quality Assessment
Five of the six studies were non-randomized, whereas one was a RCT. Three of the non-randomized studies were determined to have a “moderate” risk of bias. De León et al and Robin et al were both assessed a moderate risk of bias due to missing data.12,16 The former study lost over 40% of the patients in the MLT group and nearly 20% of the patients in the SLT group by three-month follow up, and the study excluded all such patients from the analysis completely. The latter study lost 30% of the eyes in the SLT group by merely one-week follow up. Hirabayashi et al was determined to have a moderate confounding bias risk due to a significant difference in the number of shots between the MLT and SLT groups (mean 130.2 versus 84.6 shots, respectively).10 Additionally, in all five included nonrandomized studies, the measurement of outcomes presented a moderate risk of bias. This was due to outcome assessors being aware of the interventions received by participants, a common issue in non-RCTs. Finally, there were “some concerns” of intervention deviations in Abramowitz et al, because although randomization was performed, neither the participant nor the examiners were blinded during the study period.10 The criteria and subdomains for each study are shown in Supplemental eTable 4 and Supplemental eTable 5. Using the GRADE guidelines, the overall quality of evidence was determined to be very low, as shown in Supplemental eTable 6.
IOP Differences at One Month
Figure 2a shows the mean reduction in IOP at one month following treatment with MLT and SLT, along with the corresponding forest plot. Four studies with 345 eyes were analyzed. Compared to MLT, SLT reduced the IOP significantly more by 0.83 mmHg (WMD = 0.83; 95% CI: 0.20, 1.47; P = 0.01). Heterogeneity was not present (I2 = 22%; P = 0.28). The corresponding Begg’s funnel plot can be found in Supplemental eFigure 1.
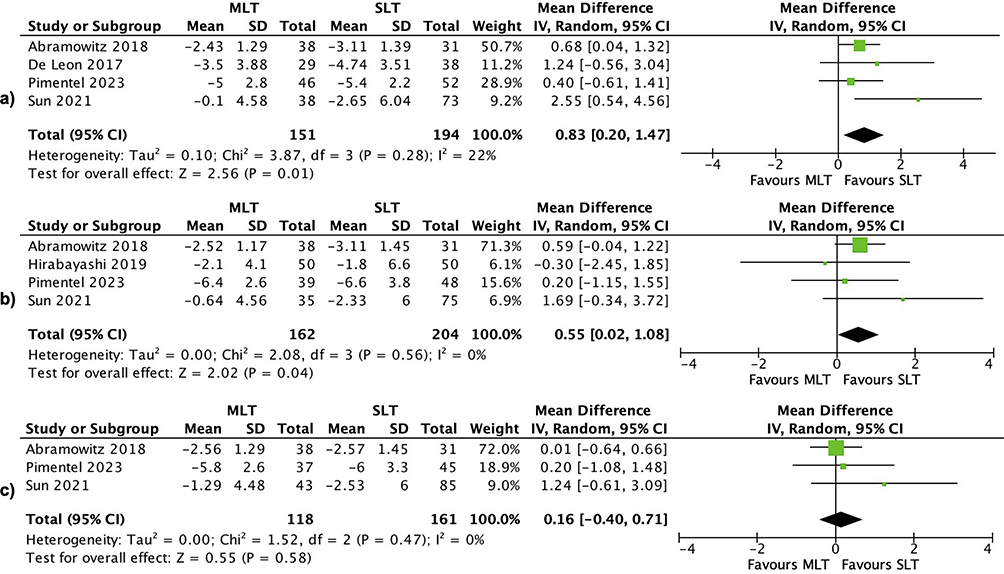 |
Figure 2 This forest plot displays the meta-analysis comparing the mean reduction in intraocular pressure (IOP) between micropulse laser trabeculoplasty (MLT) and selective laser trabeculoplasty (SLT) at three different time points: (a) 1 month, (b) 6 months, and (c) 1 year. Each study is represented by the first author’s last name along with the mean difference (MD) and the 95% confidence interval (CI). The overall mean difference and 95% CI, calculated using random-effect estimations, are also depicted. The green squares indicate the effect sizes of the individual studies with their 95% confidence intervals, while the diamonds represent the pooled effect sizes with their 95% confidence intervals. Abbreviation: IV, inverse variance; SD, standard deviation. |
A subgroup analysis was performed at the one-month follow-up for studies that used 577nm MLT compared to those that used 532nm since differences in wavelength can affect tissue penetration and energy absorption.11 In studies using 532nm MLT, the difference in IOP reduction between SLT and MLT was no longer statistically significant (WMD = 1.29; 95% CI: −0.78, 3.37; P = 0.22). The difference in IOP reduction between SLT and MLT remained significant in the studies that performed 577nm MLT (WMD = 0.74; 95% CI: 0.14, 1.34; P = 0.02). The forest plot for this subgroup analysis is shown in Supplemental eFigure 2.
IOP Differences at Six Months
Figure 2b displays the mean reduction in IOP at six months after treatment with MLT and SLT, along with the corresponding forest plot. Four studies with 366 eyes were analyzed. Compared to MLT, SLT reduced the IOP significantly more by 0.55 mmHg (WMD = 0.55; 95% CI: 0.02, 1.08; P = 0.04). Heterogeneity was not present (I2 = 0%; P = 0.56). The corresponding Begg’s funnel plot can be found in Supplemental eFigure 1.
IOP Differences at One-Year
Figure 2c presents the mean reduction in IOP at one year following treatment with MLT and SLT, along with the corresponding forest plot. Three studies with 279 eyes were analyzed. Compared to MLT, SLT reduced the IOP more by 0.16 mmHg (WMD = 0.16; 95% CI: −0.40, 0.71; P = 0.58); however, the difference was not statistically significant. Heterogeneity was not present (I2 = 0%; P = 0.47). The corresponding Begg’s funnel plot can be found in Supplemental eFigure 1.
Rate of IOP Spikes
Figure 3 illustrates the rate of IOP spikes, defined as an increase of more than 5 mmHg from the pre-procedure baseline IOP, along with the corresponding forest plot. Five studies with 526 eyes were analyzed. All the included studies in this meta-analysis except Hirabayashi et al stated that a topical alpha-2 agonist was administered prior to the procedure to reduce the risk of IOP spikes.10 There was a statistically significant lower rate of IOP spikes in the MLT treatment group compared to the SLT treatment group (RR = 0.37; 95% CI: 0.16, 0.89; P = 0.03). Heterogeneity was not present in the studies (I2 = 13%; P = 0.33). The corresponding Begg’s funnel plot can be found in Supplemental eFigure 1.
 |
Figure 3 This forest plot illustrates the meta-analysis of the risk ratio (RR) comparing the incidence of IOP spikes (defined as an increase of more than 5 mmHg following laser treatment) between micropulse laser trabeculoplasty and selective laser trabeculoplasty. Each study is identified by the first author’s last name and shows the odds ratio (OR) with the 95% confidence interval (CI). The combined effect and 95% CI, derived from random-effect estimations, are also shown. The blue squares reflect the effect sizes of individual studies with their 95% confidence intervals, and the diamonds represent the pooled effect sizes with their 95% confidence intervals. Abbreviation: MH, Mantel-Haenszel. |
Rate of Treatment Failures
Figure 4 depicts the rate of treatment failures, defined as a decrease in IOP of less than 20% or less than 3 mmHg, or the need for additional medications or procedures for IOP control, along with the corresponding forest plot. Four studies with 359 eyes were analyzed. There was no statistically significant difference in the rate of treatment failures between MLT and SLT (RR = 1.05; 95% CI: 0.68, 1.62; P = 0.84). Heterogeneity was not present in the studies (I2 = 0%; P = 0.68). The corresponding Begg’s funnel plot can be found in Supplemental eFigure 1
 |
Figure 4 This forest plot presents the meta-analysis of the risk ratio (RR) comparing failure rates between micropulse laser trabeculoplasty and selective laser trabeculoplasty. Failure is defined as a less than 20% or less than 3 mmHg reduction in IOP, or the need for additional medications or procedures to control IOP. Each study is shown with the first author’s last name and the odds ratio (OR) with 95% confidence interval (CI). The combined effect and 95% CI, calculated using random-effect estimations, are also presented. The blue squares represent the effect sizes of individual studies with their 95% confidence intervals, and the diamonds depict the pooled effect sizes with their 95% confidence intervals. Abbreviation: MH, Mantel-Haenszel. |
Reduction in Topical Medications
Figure 5 shows the mean reduction in topical medications at one year after treatment with MLT and SLT, along with the corresponding forest plot. Three studies with 310 eyes were analyzed. Two studies reported the average number of baseline medications in each group. In the Sun et al study, MLT and SLT patients were on an average of 1.8 and 2.0 medications, respectively, and in the Pimentel et al study, MLT and SLT patients were on an average of 1.52 and 1.42 medications, respectively.11,13 There was no statistically significant difference in the number of medications SLT reduced compared to MLT (WMD = 0.06; 95% CI: −0.13, 0.26; P = 0.53). Heterogeneity was not present (I2 = 0%; P = 0.42). The corresponding Begg’s funnel plot can be found in Supplemental eFigure 1
 |
Figure 5 This forest plot shows the meta-analysis comparing the mean reduction in the use of topical medications between micropulse laser trabeculoplasty and selective laser trabeculoplasty. Each study is identified by the first author’s last name along with the mean difference (MD) and 95% confidence interval (CI). The overall mean difference and 95% CI, derived from random-effect estimations, are also displayed. The green squares indicate the effect sizes of the individual studies with their 95% confidence intervals, while the diamonds represent the pooled effect sizes with their 95% confidence intervals. Abbreviation: IV, inverse variance; SD, standard deviation. |
Discussion
In this meta-analysis, we pooled data from six studies to compare various outcomes between MLT and SLT, including degree of IOP reduction, rates of IOP spikes, failure rates, and number of topical medications reduced. Patients treated with MLT were found to have significantly lower rates of IOP spikes compared to those treated with SLT. However, SLT-treated patients had significantly greater IOP reductions at one and six-months of follow-up. Interestingly, at the one-year time point, the reduction in IOP was no longer statistically significant. There was also no significant difference in failure rates or topical medication reduction between the two treatment groups.
As IOP spikes in patients with glaucoma can lead to further damage of the optic nerve, it is important to reduce the incidence of this complication after LTP.28 In a prior review of the literature on postoperative IOP spikes, the authors recommended rigorous control of moderate IOP spikes in eyes that are at higher risk of damage associated with these spikes, such as patients with advanced glaucoma.28,29 In addition to treating IOP spikes with IOP lowering medications, when necessary, it is also important to investigate methods to reduce the rate of this complication following LTP. One method is to preoperatively treat with a topical alpha-2 agonist, which has been shown to prevent IOP increases after LTP through reduction of ciliary blood flow and aqueous formation.30 All included studies in this meta-analysis, except Hirabayashi et al, explicitly stated they gave a drop of an alpha-2 agonist prior to the procedure to reduce the risk of IOP spikes.10
It has also been hypothesized that the cellular damage to the TM and the excessive early pigment dispersion can result in elevated levels of inflammation, which may contribute to SLT’s complications.31 In this study, we found that there was a significantly lower risk of having an IOP spike following MLT compared to SLT. This is likely related to the fact that, compared to other forms of LTP, MLT is less likely to result in structural damage to the TM due to its ability to minimize the thermal spread and coagulative effects of the laser.32 However, the degree of IOP spike is also important to consider. Although every included study used a definition of >5 mmHg increase in IOP from baseline as their definition of an IOP spike, most studies did not specify the average IOP spike beyond this definition. However, in Robin et al, the authors mentioned that the average IOP spike increase in the SLT group was 7.57 mmHg compared to a 5 mmHg IOP spike in the MLT group.12 Another factor to consider is that the majority of included studies used an SLT energy level that produced visible cavitation bubbles, as opposed to using a level just below bubble formation. The literature has not shown a significant energy dose-response benefit of increased energy on SLT efficacy and increased levels could contribute to increased rates of IOP spikes.33 MLT, on the other hand, does not induce any visible tissue reaction which makes energy titration more difficult.34 Therefore, it is possible that undertreatment of laser energy, relative to SLT, may explain the lower likelihood of adverse events. Although the findings in this meta-analysis suggest that MLT may offer an alternative to SLT with fewer post-laser complications, further research is necessary to determine if MLT still produces fewer IOP spikes compared to SLT when the target energy levels are titrated to be below a visible bubble response.
In terms of efficacy between MLT and SLT, this meta-analysis found that at shorter follow-ups of one and six months, SLT lowered IOP slightly more in a statistically significant manner, however at one year, there was no significant difference in efficacy. The rates of treatment failures were comparable between MLT and SLT. Although the difference in IOP was statistically significant at one and six months, the difference was small, less than 1 mmHg at both time points, and this statistical significance was lost by one year. Therefore, it is important to raise the question if the difference is clinically significant. Moreover, since there are natural IOP fluctuations during the day, it is difficult to discern whether such a small difference in IOP is the effect of natural fluctuation or a treatment effect.35,36 Since the majority of the included studies were retrospective, it is unclear if an average of multiple IOP measurements was consistently taken or if just a single measurement was used. It has been reported that a single measure of IOP does not adequately estimate the average of multiple measurements.37 Further, RCTs with more standardized protocols are necessary to determine if there is any clinically significant difference in the IOP-lowering effects of MLT compared to SLT.
An important factor to consider in the use of MLT is the lack of standardization, with significant variations between studies on the wavelength, spot size, power, and spot duration used, and the lack of a clear endpoint during application of the laser.8 Unlike in SLT where the target energy is either typically titrated to be at or just below visible cavitation bubble formation, MLT does not produce any visible reaction.31,33 Factors such as TM pigmentation and media opacity can impact the amount of energy delivered to the TM during LTP.38 In the case of MLT where there is a lack of a visible endpoint during treatment, it can be difficult to titrate the level of energy needed to produce an effective response to treatment. Additional research is required to establish a standardized MLT protocol.
The wavelength of the laser used in MLT can influence the degree of tissue penetration and energy absorption. In this meta-analysis, two studies used 577nm MLT, while four studies used 532nm MLT.11 Only the one-month follow-up for change in IOP meta-analysis had both studies that used 577nm MLT, so a subgroup analysis was performed and found that when stratified by wavelength, the difference in IOP between SLT and MLT was no longer statistically significant in the 532nm MLT subgroup. However, this result should be taken with caution due to the limited number of studies in each subgroup, and there was also significant heterogeneity in the 532nm MLT subgroup. There is currently a lack of a standardized MLT protocol, as seen by the studies in this meta-analysis, which poses a challenge to widespread use of the technology.8 Further research is needed to establish guidelines for MLT and assess if variations in wavelengths lead to significant differences in outcomes of the procedure.
While this meta-analysis provides valuable insights into outcomes of MLT compared to SLT, it is important to consider the limitations of this study. The majority of included studies were retrospective which inherently increases the risk of selection bias. There were also variations in whether patients were treatment naive to LTP between the included studies. Some included first time only SLT,12,13 whereas another included only those who did not have laser in the prior 6 months,11 and the remainder did not specify. Although it has been reported that repeat SLT has similar efficacy as the initial treatment, it is something important to consider as a potential source of heterogeneity.39 Additionally, two studies12,16 did not perform 360° SLT on some or all of their patients to match the 360° MLT performed. Since the two treatment groups in these studies received varying degrees of laser, this complicates the direct comparison between them because 360° SLT has been shown to be more effective than 180° SLT at reducing IOP.40–42 Another point to consider is that depending on the type of OAG, there can be differences in responsiveness to LTP.43 However, due to a lack of stratification by the individual studies on MLT and SLT efficacy in various types of glaucoma, separate meta-analyses of subgroups could not be conducted.
Although the study has limitations, this meta-analysis offers valuable perspectives into the effectiveness and complications of MLT in comparison to SLT. Strengths of the study include a larger sample size to allow for greater power to detect differences between treatments. There were also multiple countries included with diverse patient populations, which can improve the generalizability of the findings. In light of reports that LTP is the preferred first-line treatment option for OAG and OHT, it is crucial to have further studies investigating MLT to determine the optimal laser parameters to achieve successful control of IOP while also minimizing unwanted complications.6
Data Sharing Statement
Data extracted from included studies and analysis are available from the authors upon reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Distelhorst JS, Hughes GM. Open-angle glaucoma. Am Fam Physician. 2003;67(9):1937–1944.
3. Wise JB, Witter SL. Argon laser therapy for open-angle glaucoma. A pilot study. Arch Ophthalmol. 1979;97(2):319–322. doi:10.1001/archopht.1979.01020010165017
4. Zgryźniak A, Przeździecka-Dołyk J, Szaliński M, Turno-Kręcicka A. Selective Laser Trabeculoplasty in the Treatment of Ocular Hypertension and Open-Angle Glaucoma: clinical Review. J Clin Med. 2021;10(15):3307. doi:10.3390/jcm10153307
5. Latina MA, Park C. Selective targeting of trabecular meshwork cells: in vitro studies of pulsed and CW laser interactions. Exp Eye Res. 1995;60(4):359–371. doi:10.1016/s0014-4835(05)80093-4
6. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial: six-Year Results of Primary Selective Laser Trabeculoplasty versus Eye Drops for the Treatment of Glaucoma and Ocular Hypertension. Ophthalmology. 2023;130(2):139–151. doi:10.1016/j.ophtha.2022.09.009
7. Ingvoldstad DD, Krishna R, Willoughby L. MicroPulse Diode Laser Trabeculoplasty versus Argon Laser Trabeculoplasty in the Treatment of Open Angle Glaucoma. Invest Ophthalmol Visual Sci. 2005;46(13):123.
8. Ma A, Yu SWY, Wong JKW. Micropulse laser for the treatment of glaucoma: a literature review. Surv Ophthalmol. 2019;64(4):486–497. doi:10.1016/j.survophthal.2019.01.001
9. Abramowitz B, Chadha N, Kouchouk A, Alhabshan R, Belyea DA, Lamba T. Selective laser trabeculoplasty vs micropulse laser trabeculoplasty in open-angle glaucoma. Clin Ophthalmol. 2018;12:1599–1604. doi:10.2147/opth.S167102
10. Hirabayashi MT, Rosenlof TL, An JA. Comparison of successful outcome predictors for MicroPulse(®) laser trabeculoplasty and selective laser trabeculoplasty at 6 months. Clin Ophthalmol. 2019;13:1001–1009. doi:10.2147/opth.S205977
11. Pimentel RL, Alves Júnior RR, Lima W, Dantas LOR, Costa VP. Selective laser trabeculoplasty versus micropulse laser trabeculoplasty for intraocular pressure control in patients with primary open angle glaucoma: a 12-month retrospective comparative study. Lasers Med Sci. 2023;38(1):102. doi:10.1007/s10103-023-03771-9
12. Robin AZ, Syar P, Darwish D, et al. Comparison of success rate and intraocular pressure spikes between selective laser trabeculoplasty and micropulse laser trabeculoplasty in African American and Hispanic patients. Int J Ophthalmol. 2023;16(1):75–80. doi:10.18240/ijo.2023.01.11
13. Sun CQ, Chen TA, Deiner MS, Ou Y. Clinical Outcomes of Micropulse Laser Trabeculoplasty Compared to Selective Laser Trabeculoplasty at One Year in Open-Angle Glaucoma. Clin Ophthalmol. 2021;15:243–251. doi:10.2147/opth.S285136
14. Gapsis BC, Bickford M, Sharpe RA, Das S, Kammerdeiner L, Nutaitis MJ. Analysis of the Relative Efficacy of Micropulse Laser Trabeculoplasty and Selective Laser Trabeculoplasty. Invest Ophthalmol Visual Sci. 2018;59(9):6090.
15. Coombs P, Radcliffe NM. Outcomes of Micropulse Laser Trabeculoplasty vs. Selective Laser Trabeculoplasty. Invest Ophthalmol Visual Sci. 2014;55(13):6155.
16. DMIDL DE, LEÓN D, López DAG. Selective laser trabeculoplasty vs micropulse laser trabeculoplasty for the treatment of open angle glaucoma and ocular hypertension. Intern J Res. 2017;14(1):2307.
17. Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg. 2011;128(1):305–310. doi:10.1097/PRS.0b013e318219c171
18. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:372:n71. 10.1136/bmj.n71.
19. Lefebvre C, Briscoe S, Featherstone R, et al., Chapter 4: searching for and selecting studies, Higgins JPT, Thomas J, Chandler J, et al. editors. Cochrane Handbook for Systematic Reviews of Interventions Version 64 updated October 2023). 2023
20. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016:
21. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019:
22. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
23. Latina MA, Sibayan SA, Shin DH, Noecker RJ, Marcellino G. Q-switched 532-nm Nd:YAG laser trabeculoplasty (selective laser trabeculoplasty): a multicenter, pilot, clinical study. Ophthalmology. 1998;105(11):2082–2088. doi:10.1016/s0161-6420(98)91129-0.
24. Higgins JPT TJ, Chandler J, Cumpston M, Li T, Page MJ, (Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane, 2023. Available from.www.training.cochrane.org/handbook.
25. You EL, Hébert M, Jin TS, et al. Comparing interventions for chronic central serous chorioretinopathy: a network meta-analysis. Surv Ophthalmol. 2023;68(4):601–614. doi:10.1016/j.survophthal.2023.03.001
26. Macaskill P GC, Deeks JJ, Harbord RM, Takwoingi Y. Chapter 10: analysing and Presenting Results. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy Version 10 the Coch Colla. 2010;1:1.
27. Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA Statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
28. McMonnies CW. Intraocular pressure spikes in keratectasia, axial myopia, and glaucoma. Optom Vis Sci. 2008;85(10):1018–1026. doi:10.1097/OPX.0b013e3181890e91
29. Tranos P, Bhar G, Little B. Postoperative intraocular pressure spikes: the need to treat. Eye (Lond). 2004;18(7):673–679. doi:10.1038/sj.eye.6701319
30. Zhang L, Weizer JS, Musch DC. Perioperative medications for preventing temporarily increased intraocular pressure after laser trabeculoplasty. Cochrane Database Syst Rev. 2017;2(2):Cd010746. doi:10.1002/14651858.CD010746.pub2
31. Gambini G, Carlà MM, Caporossi T, et al. Spotlight on MicroPulse Laser Trabeculoplasty in Open-Angle Glaucoma: what’s on? A Review of the Literature. Vision (Basel). 2022. 61. 10.3390/vision6010008
32. Fudemberg SJ, Myers JS, Katz LJ. Trabecular Meshwork Tissue Examination With Scanning Electron Microscopy: a Comparison of Micropulse Diode Laser (MLT), Selective Laser (SLT), and Argon Laser (ALT) Trabeculoplasty in Human Cadaver Tissue. Invest Ophthalmol Visual Sci. 2008;49(13):1236.
33. Radcliffe N, Gazzard G, Samuelson T, et al. Energy Dose-Response in Selective Laser Trabeculoplasty: a Review. J Glaucoma. 2022;31(8):e49–e68. doi:10.1097/ijg.0000000000002062
34. Lee JWY, Yau GSK, Yick DWF, Yuen CYF. MicroPulse Laser Trabeculoplasty for the Treatment of Open-Angle Glaucoma. Medicine. 2015;94(49):e2075. doi:10.1097/md.0000000000002075 Medicine (Baltimore).
35. Saccà SC, Rolando M, Marletta A, Macrí A, Cerqueti P, Ciurlo G. Fluctuations of intraocular pressure during the day in open-angle glaucoma, normal-tension glaucoma and normal subjects. Ophthalmologica. 1998;212(2):115–119. doi:10.1159/000027290
36. Yaoeda K, Fukushima A, Shirakashi M, Miki A, Fukuchi T. Factors associated with fluctuations in repeated measurements of intraocular pressure using the Goldmann applanation tonometer in Japanese patients with primary open-angle glaucoma. Clin Ophthalmol. 2018;12:1473–1478. doi:10.2147/opth.S174277
37. Zhang ML, Chon BH, Wang J, et al. Single vs multiple intraocular pressure measurements in glaucoma surgical trials. JAMA Ophthalmol. 2014;132(8):956–962. doi:10.1001/jamaophthalmol.2014.867
38. Leahy KE, White AJ. Selective laser trabeculoplasty: current perspectives. Clin Ophthalmol. 2015;9:833–841. doi:10.2147/opth.S53490
39. Garg A, Vickerstaff V, Nathwani N, et al. Efficacy of Repeat Selective Laser Trabeculoplasty in Medication-Naive Open-Angle Glaucoma and Ocular Hypertension during the LiGHT Trial. Ophthalmology. 2020;127(4):467–476. doi:10.1016/j.ophtha.2019.10.023
40. Dahlgren T, Ayala M, Zetterberg M. Optimal Performance of Selective Laser Trabeculoplasty: results from the Swedish Optimal SLT Multicenter Randomized Controlled Trial. Ophthalmol Glaucoma. 2023;7(2):105–115. doi:10.1016/j.ogla.2023.10.004
41. Michaelov E, Sachdeva R, Raniga A, Lin T. A Randomized, Controlled Comparison of 180 Versus 360 Degrees Selective Laser Trabeculoplasty in Open Angle Glaucoma and Glaucoma Suspects. J Glaucoma. 2023;32(4):252–256. doi:10.1097/ijg.0000000000002184
42. Zhu D, Shah P, Wong A, et al. 180° versus 360° Selective Laser Trabeculoplasty in Open Angle Glaucoma and Ocular Hypertension: a Systematic Review and Meta-Analysis. J Glaucoma. 9900:
43. Sarenac T, Turkanović A B, Ferme P, Gračner T. A Review of Selective Laser Trabeculoplasty: ”The Hype Is Real”. J Clin Med. 2022;11(13):3879. doi:10.3390/jcm1113387
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.