")
Back to Journals » Clinical Ophthalmology » Volume 19
Outcomes of Repeat Deep Anterior Lamellar Keratoplasty in Keratoconus: Case Series
Authors Kirat O, Fairaq R , AlMutlak M, AlQahtani RS, AlHussein GA, AlHilali S
Received 29 March 2025
Accepted for publication 16 June 2025
Published 10 July 2025 Volume 2025:19 Pages 2203—2209
DOI https://doi.org/10.2147/OPTH.S528658
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Omar Kirat,1 Rafah Fairaq,1 Mohammed AlMutlak,1 Raneem S AlQahtani,2 Ghadah A AlHussein,2 Sara AlHilali1
1Anterior Segment Division, King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia; 2Surgery Department, Aldiriyah Hospital - Riyadh Third Health Cluster, Riyadh, Saudi Arabia
Correspondence: Sara AlHilali, Anterior Segment Division, King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia, Tel +966544017155, Email [email protected]
Purpose: To report the incidence, indications, and clinical outcomes of repeat deep anterior lamellar keratoplasty (DALK) in keratoconus patients.
Methods: Case series.
Results: This retrospective study included all repeat DALK procedures for keratoconus performed at King Khaled Eye Specialist Hospital (KKESH) between 2016 and 2024. Patient demographics, surgical techniques, complications, and outcomes were analyzed. Among 2136 primary DALK procedures, only 0.66% (14 eyes) required repeat keratoplasty. The mean age at the time of repeat DALK was 32 and the mean follow-up duration was 30 months. Indications included lipid keratopathy (28.6%), persistent epithelial defect with severe immune reaction (14.3%), high irregular astigmatism (14.3%), and stromal scarring (7.1%). Graft exchange alone was sufficient in most cases (64%), while larger trephination and further dissection (22%) were performed for stromal scars or host rim ectasia. Postoperative complications (43%) included loose sutures (36%), elevated intraocular pressure (7%), and cataract formation (7%). The overall graft survival rate was 93%, with one failure due to poor compliance with postoperative steroids and follow-ups. Visual recovery was favorable, with 57% achieving 20/40 or better.
Conclusion: Repeat DALK is a safe and effective alternative to penetrating keratoplasty (PK) for failed primary DALK, offering high graft survival and favorable visual outcomes while minimizing immune-related complications. Postoperative adherence and timely steroid management are critical for optimizing success. Further studies comparing repeat DALK and repeat PK are needed to assess long-term endothelial health and visual stability.
Keywords: deep anterior lamellar keratoplasty, (DALK), keratoconus, repeat keratoplasty
Introduction
Over the last decade, deep anterior lamellar keratoplasty (DALK) have gained popularity and been accepted as the preferred treatment modality for patients with keratoconus. Although the refractive and visual outcomes of DALK and penetrating keratoplasty (PK) for the treatment of keratoconus are reported to be similar,1 compared to PK, DALK has the advantage of maintaining the structural integrity of the eye, lowering the risk of wound dehiscence in the occurrence of trauma, also, the ability to discontinue topical steroid at an earlier stage compared to PK has ultimately reduced the risk of steroid-induced glaucoma and cataract progression.2–4 Most importantly, performing DALK eliminates the risk of endothelial rejection which is one of the most dreaded complication following PK.3 Due to the higher reported complications associated with PK, a study has also proven that although DALK is a more expensive procedure, the overall incremental cost of management was lower for DALK, making it a more cost effective procedure for patients.5
Thus far, most of the published literature has focused on the outcomes of primary keratoplasty, and little data exist on the outcomes of repeat keratoplasty. Few studies have reported the outcomes of repeat penetrating keratoplasty in patients with primary diagnosis of corneal ectasia and it was confirmed that the overall prognosis for was excellent, however, the rate of rejection following re-PKP was found to be high (75%), necessitating closer follow-up.6,7 However, to the best of our knowledge, this is the largest case series reporting the outcomes of repeat deep anterior lamellar keratoplasty in Keratoconus patients. This study aims to assess the incidence, patient demographics, causes of graft failure and clinical outcomes of repeat DALK in keratoconus patients.
Methods
This retrospective study included all repeat DALK procedures for keratoconus performed at King Khaled Eye Specialist Hospital (KKESH) between 2016 and 2024. Patient demographics, surgical techniques, complications, and outcomes were analyzed.
Eyes with a primary diagnosis other than keratoconus and patients with ocular comorbidities such as glaucoma, uveitis, cataract, or other conditions that could affect surgical outcomes were excluded.
The decision between performing a graft exchange alone versus further stromal dissection was guided by intraoperative assessment of the host bed. If the recipient stromal bed appeared smooth and regular without residual scarring, graft exchange was performed without additional dissection. In contrast, further stromal dissection was undertaken when the host bed showed surface irregularity or residual stromal scarring, to improve graft-host interface quality. All surgeries were performed by experienced corneal surgeons. A standardized postoperative regimen was applied to all patients, including topical corticosteroids tapered over 9 months and prophylactic topical antibiotics for 2 weeks.
Patient demographics, clinical characteristics, surgical details, and postoperative outcomes were collected from medical records. Data included baseline characteristics such as age, sex, laterality, and preoperative best-corrected visual acuity (BCVA), along with indications for repeat DALK, donor characteristics, intraoperative details, and postoperative complications.
The primary outcome measure was final BCVA following repeat DALK. Secondary outcome measures included the incidence of repeat DALK in keratoconus patients within the study period, indications for repeat DALK, second graft survival, and postoperative complication rates. Graft survival was defined as the presence of a clear graft at the last follow-up visit.
Descriptive statistics were used to summarize patient demographics and clinical characteristics. The incidence of repeat DALK was calculated as a proportion of total keratoplasties performed for keratoconus during the study period. Graft survival was reported as the percentage of grafts remaining clear at the last follow-up. A paired t-test was used to compare pre and postoperative BCVA and keratometry readings. Statistical significance was set at P < 0.05.
Informed consent was obtained from all patients including consent for publication of their clinical details. The study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Research Board of King Khaled Eye Specialist Hospital (KKESH, RP 23039-R).
Results
This study included 14 eyes from 14 patients with keratoconus who underwent repeat deep lamellar keratoplasty (DALK) at King Khaled Eye Specialist Hospital (KKESH) between 2016 and 2024. During this period, a total of 2136 DALKs were performed for keratoconus, with an incidence of repeat DALK of 0.66%. Details of the eyes included in this study is shown in Table 1.
 |
Table 1 Characteristics of Eyes with Repeated Lamellar Keratoplasty |
The indications for repeat grafting varied among patients. High irregular astigmatism was the cause in two eyes (n = 2, 14.3%), while lipid keratopathy secondary to corneal neovascularization was identified in four eyes (n = 4, 28.6%). Two eyes had persistent epithelial defects with severe immune reactions to sutures (n = 2, 14.3%). One eye had poor graft quality with stromal scarring (n = 1, 7.1%), and another was found intraoperatively to have a donor cornea with a Laser-assisted in situ keratomileusis (LASIK) flap (n = 1, 7.1%). One eye developed keloid formation following PRK on the first DALK (n = 1, 7.1%), while another had high irregular astigmatism and a graft scar following trauma that required graft re-suturing (n = 1, 7.1%). One case had a scarred graft post microbial keratitis (n = 1, 7.1%), and another developed a stromal scar due to rejection (n = 1, 7.1%).
The mean age at the time of repeat DALK was 32 ± 8.7 years. The majority of patients were male (n = 9, 64%), and all were medically free. A history of vernal keratoconjunctivitis (VKC) was present in 36% of eyes (n = 5).
The primary DALK was performed using a manual dissection technique in 78.5% of eyes (n = 11), while the big-bubble technique was used in 21.5% of eyes (n = 3). The mean time to failure of the first LKP was 60.6 ± 65.34 months. Postoperative complications following the first DALK included persistent epithelial defect (n = 2, 14%), high intraocular pressure (n = 2, 14%), corneal neovascularization (n = 4, 28.5%), and loose sutures (n = 4, 28.5%), while 50% of patients had no reported complications (n = 7).
During the second DALK, the most commonly performed technique was graft exchange alone (n = 9, 64%), followed by larger trephination with further dissection (n = 3, 22%) and further dissection alone (n = 2, 14%). Intraoperative complications were uncommon, with Descemet membrane perforation occurring in two eyes.
Postoperative complications following the repeat DALK were observed in 43% of eyes (n = 6). The most common complications were loose sutures (n = 5, 36%), high intraocular pressure (n = 1, 7%), corneal neovascularization (n = 1, 7%), and cataract formation (n = 1, 7%). Subconjunctival Avastin injection was administered in 36% of eyes (n = 5), and cautery for corneal neovascularization was performed in one eye.
The mean preoperative BCVA was 0.65 ± 0.27 logMAR, which improved to 0.43 ± 0.42 logMAR postoperatively. This improvement was found to be not statistically significant (P = 0.1).
At the final follow-up, BCVA improved to 20/40 or better in 57% of eyes (n = 8), while 43% had a final visual acuity worse than 20/40 (n = 6). The mean postoperative keratometry values were 43.1 ± 3.6 D (K1) and 47.1 ± 2.4 D (K2), demonstrating a reduction from preoperative values (46.5 ± 9.04 D (K1) and 53.4 ± 10 D (K2)). The decrease in K2 was statistically significant (P = 0.03), while the change in K1 did not reach statistical significance (P = 0.1), based on paired t-test analysis.
The overall success rate of repeat DALK was 93% (n = 13), with failure occurring in 1 eye only at a mean of 5.7 months postoperatively. Subsequent surgical interventions were required in 14% of cases (n = 5), including re-suturing (two eyes), amniotic membrane transplantation (one eye), cataract surgery (one case), and deep sclerectomy (one eye). The mean follow-up duration after the second DALK was 29.8 ± 25.8 months.
Discussion
As DALK continues to gain widespread acceptance as the preferred surgical approach for keratoconus,4 the management of failed DALK cases has become an important clinical challenge. While PK has traditionally been the standard option for regrafting, repeat DALK has emerged as a viable alternative, offering the advantage of endothelial preservation and reducing the long-term risk of endothelial failure. However, despite these advantages, there is limited literature on the outcomes of repeat DALK, particularly in keratoconus patients.6–8 This study represents the largest series to date investigating the outcomes of repeat DALK in keratoconus, demonstrating a high graft survival rate (93%), favorable visual outcomes, and a low risk of rejection.
Our study found that out of 2136 DALK procedures performed for keratoconus at KKESH between 2016 and 2024, only 0.66% required repeat keratoplasty, which is significantly lower than previously reported failure rates for DALK and more than 12 times lower than the 8% failure rate observed after PK in keratoconus.9 The need for regrafting in our series arose from a variety of indications, reflecting the complex nature of graft failure mechanisms. Lipid keratopathy was the most common cause (28.6%), followed by persistent epithelial defect with severe immune reaction to sutures (14.3%) and high irregular astigmatism (14.3%). Other causes included poor graft quality, trauma-related complications, and microbial keratitis, each accounting for 7.1% of cases. These findings suggest that while primary DALK failure is uncommon, it can occur due to diverse and sometimes unexpected factors, necessitating individualized surgical approaches.
Among the cases in this study, one patient developed stromal scarring in the first graft, which was noted immediately postoperatively and is illustrated in Figure 1. This suggests that poor graft quality or intraoperative factors may have contributed to early opacification, reinforcing the need for meticulous donor selection and intraoperative assessment. Additionally, two young male patients, with a known history of vernal VKC, experienced severe conjunctival injection, persistent epithelial defect, and early stromal opacity soon after their initial DALK surgeries (Figures 2 and 3). These findings led to their classification as early graft failures, necessitating repeat DALK within 1–3 months. However, before proceeding with regrafting, both patients were prepped with intensified topical steroid therapy and systemic oral steroids to control the severe immune response observed postoperatively. The presence of VKC in these cases may have contributed to the heightened inflammatory reaction and need for more aggressive perioperative immunosuppression. This pattern of early postoperative immune reaction aligns with findings from Hos et al10 who described stromal and subepithelial immune reactions following lamellar keratoplasty. Their study highlights that while DALK eliminates endothelial rejection, it does not prevent immune responses within the stroma and epithelium, particularly in younger patients with heightened immune activity. Our experience suggests that aggressive early intervention with intensified steroid therapy may help stabilize high-risk cases and potentially improve graft survival before considering repeat transplantation.
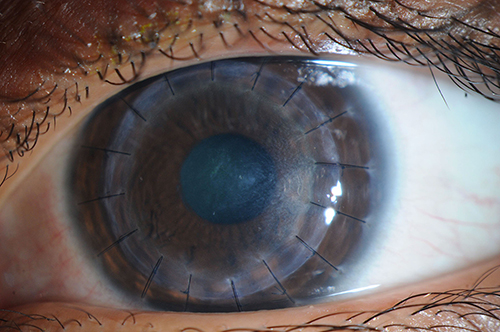 |
Figure 1 Slit-lamp photograph of Patient 1 who developed stromal scarring in the first graft, which was noted immediately postoperatively after primary DALK. The image demonstrates temporal stromal opacity. |
 |
Figure 2 Slit-lamp photograph of Patient 3, a young male patient, who developed a persistent epithelial defect (PED) and severe immune reaction soon after primary DALK. The image shows conjunctival injection, persistent epithelial breakdown, and early stromal melt. |
 |
Figure 3 Slit-lamp photograph of Patient 13, who similarly presented with severe conjunctival injection, and stromal opacity shortly after primary DALK. |
In our cohort, graft exchange was the most frequently performed surgical approach (64%), followed by larger trephination with further dissection (22%) and further dissection alone (14%), depending on the specific nature of the primary graft failure. We found that in most cases, graft exchange alone was sufficient, and we were able to bluntly detach the failed graft using a Sinskey hook, minimizing trauma to the underlying host tissue. Larger trephination and further dissection were performed only when residual stromal scarring, uneven dissection, or host rim ectasia was identified, ensuring a smoother recipient bed for the new graft. Our approach aligns with Scorcia et al11,12 who described a technique for repeat DALK where the donor lamella was bluntly detached without requiring pneumatic dissection, allowing for a straightforward graft exchange while preserving the host endothelium. In contrast to their study, which primarily addressed stromal opacity-related failures, our series included a broader range of failure mechanisms, reinforcing the versatility of graft exchange in managing various complications following primary DALK.
In cases with progressive peripheral corneal neovascularization, subconjunctival Avastin (bevacizumab) was administered during the early postoperative period to help suppress vessel growth and support graft clarity. Although its precise impact could not be conclusively evaluated in our limited sample, previous studies have demonstrated its efficacy in reducing corneal neovascularization and improving graft survival in high-risk settings.12
The overall success rate of repeat DALK was 93%, with only one case (7%) experiencing graft failure after a mean of 5.7 months. This failure occurred in a patient with poor compliance to postoperative steroid use and irregular follow-up visits, highlighting the critical role of adherence to postoperative care. This high survival rate aligns with previous reports suggesting that repeat DALK, when carefully planned and executed, can achieve comparable outcomes to primary DALK.6–8 Visual recovery was favorable, with 57% of eyes achieving a final best spectacle-corrected visual acuity (BCVA) of 20/40 or better. Only one eye had a final BCVA of 20/200, which was attributed to cataract formation following trauma. Additionally, postoperative keratometry values demonstrated an improvement in corneal curvature, with K1 decreasing from 46.5 ± 9.04 D to 43.1 ± 3.6 D and K2 from 53.4 ± 10 D to 47.1 ± 2.4 D. These findings confirm that repeat DALK not only restores graft clarity but also improves corneal shape and refractive outcomes in keratoconus patients.
While postoperative complications were observed in 43% of cases, they were predominantly non-immune in nature. The most common complication was loose sutures (36%), followed by high intraocular pressure (7%), corneal neovascularization (7%), and cataract formation (7%). Notably, none of the graft failures were due to rejection, emphasizing the critical role of proper postoperative care, adherence to immunosuppressive therapy, and patient education on recognizing early signs of graft failure.
This study supports repeat DALK as the preferred approach for failed primary DALK when the host endothelium remains viable, offering a graft-preserving alternative to penetrating keratoplasty (PK) while minimizing immune-mediated complications. The findings highlight the critical role of patient compliance, consistent follow-up, and extended postoperative steroid use in optimizing graft survival, as underscored by the single case of graft failure due to noncompliance.
With a high graft survival rate of 93% and favorable visual outcomes, these results reinforce the safety and efficacy of repeat DALK. Future directions should include prospective or multicenter studies comparing repeat DALK with repeat PK, as well as long-term monitoring of endothelial cell density and functional visual outcomes. Developing standardized surgical and postoperative management protocols—including the potential use of adjunctive therapies such as anti-VEGF agents—may further enhance outcomes in this patient population.
This study is limited by its retrospective design, small sample size, and lack of a control group. Nonetheless, the data provide a strong foundation for positioning repeat DALK as a viable, tissue-sparing strategy in keratoconus patients requiring regrafting.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Amayem AF, Hamdi IM, Hamdi MM. Refractive and visual outcomes of penetrating keratoplasty versus deep anterior lamellar keratoplasty with hydrodissection for treatment of keratoconus. Cornea. 2013;32:e2–5. doi:10.1097/ICO.0B013E31825CA70B
2. Liu H, Chen Y, Wang P, et al. Efficacy and safety of deep anterior lamellar keratoplasty vs. penetrating keratoplasty for keratoconus: a meta-analysis. PLoS One. 2015;10:e0113332. doi:10.1371/JOURNAL.PONE.0113332
3. Tan DTH, Dart JKG, Holland EJ, et al. Corneal transplantation. Lancet. 2012;379:1749–1761. doi:10.1016/S0140-6736(12)60437-1
4. Reinhart WJ, Musch DC, Jacobs DS, et al. Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty a report by the American academy of ophthalmology. Ophthalmology. 2011;118:209–218. doi:10.1016/J.OPHTHA.2010.11.002
5. Koo TS, Finkelstein E, Tan D, et al. Incremental cost-utility analysis of deep anterior lamellar keratoplasty compared with penetrating keratoplasty for the treatment of keratoconus. Am J Ophthalmol. 2011;152:40–47.e2. doi:10.1016/J.AJO.2011.01.017
6. Woo JH, Tan YL, Htoon HM, et al. Outcomes of repeat anterior lamellar keratoplasty. Cornea. 2019;39(2):200–206. doi:10.1097/ICO.0000000000002167
7. Feizi S, Javadi MA, Khajuee-Kermani P, et al. Repeat keratoplasty for failed deep anterior lamellar keratoplasty in keratoconus: incidence, indications, and outcomes. Cornea. 2017;36(5):535–540. doi:10.1097/ICO.0000000000001169
8. Arora R, Sanoria A, Jain P, et al. Repeat deep anterior lamellar keratoplasty (DALK) for failed primary DALK. Indian J Ophthalmol. 2023;71:2462–2465. doi:10.4103/IJO.IJO_2505_22
9. Kelly TL, Coster DJ, Williams KA. Repeat penetrating corneal transplantation in patients with keratoconus. Ophthalmology. 2011;118:1538–1542. doi:10.1016/J.OPHTHA.2011.01.002
10. Hos D, Matthaei M, Bock F, et al. Immune reactions after modern lamellar (DALK, DSAEK, DMEK) versus conventional penetrating corneal transplantation. Prog Retin Eye Res. 2019;73:100768. doi:10.1016/J.PRETEYERES.2019.07.001
11. Scorcia V, Beltz J, Lucisano A, et al. Surgical technique for graft exchange after big-bubble deep anterior lamellar keratoplasty. Cornea. 2015;34:486–489. doi:10.1097/ICO.0000000000000365
12. Chang JH, Garg NK, Lunde E, et al. Corneal neovascularization: an anti-VEGF therapy review. Surv Ophthalmol. 2012;57:415. doi:10.1016/J.SURVOPHTHAL.2012.01.007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.