")
Back to Journals » International Medical Case Reports Journal » Volume 17
Partial Detachment of an ILM Inverted Flap After a Successful Closure of a Full-Thickness Traumatic Macular Hole
Authors Al Taisan AA
Received 15 September 2024
Accepted for publication 10 December 2024
Published 12 December 2024 Volume 2024:17 Pages 1025—1028
DOI https://doi.org/10.2147/IMCRJ.S495427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Abdulaziz A Al Taisan
Department of Surgery, King Faisal University, Al-Ahsa, Saudi Arabia
Correspondence: Abdulaziz A Al Taisan, Department of Surgery, College of Medicine, King Faisal University, Al-Ahsa, Saudi Arabia, Email [email protected]
Purpose: To report a case of partial detachment of an inverted internal limiting membrane (ILM) flap following a successful closure of a full-thickness traumatic macular hole.
Observations: A 24-year-old male patient presented with a history of a blunt trauma and a full-thickness macular hole. Visual acuity was (20/50) then deteriorated to (20/100) prior to surgery. He underwent pars plana vitrectomy with an inverted ILM flap and gas tamponade. Postoperatively, successful closure of the hole was noted with a visible hinged ILM flap observed over the retina in optical coherence tomography (OCT). Three months later, the patient presented with a complaint of a central floater. Visual acuity was (20/30) and a partially detached ILM flap was noted in the OCT.
Conclusions and Importance: Inverted ILM flap might detach from the retinal surface after gas resolution and successful closure of a full-thickness macular hole.
Keywords: ILM flap, ILM inverted flap, full thickness macular hole, macular hole
Introduction
Internal limiting membrane (ILM) flaps have been used in the management of full-thickness macular holes (FTMH) since 2010.1 For small and medium macular holes, ILM peeling and inverted ILM flaps have a high success rate. However, for large macular holes, inverted ILM flaps appear superior in achieving hole closure.2 More recently, Romano et al3 described the viscoelastic-assisted inverted ILM flap technique. Here, we report a case of an inverted flap that has detached after a successful closure of a full-thickness macular hole, done in Al jabr Eye and ENT Hospital in Hofuf (IRB approval was aquired; Al jabr Eye and ENT Hospital, Hofuf).
Case Report
A 24-year-old male patient presented to our clinic in November 2023 with a history of blunt trauma to the right eye in October 2023. He had a hyphema at the time of the trauma, so a proper fundus exam was not performed at that time. Upon examination, visual acuity was (20/50), anterior segment examination was unremarkable, and fundus exam revealed a full-thickness macular hole. OCT revealed a full-thickness macular hole with a diameter of 320 um and a base diameter of 925 um (Figure 1). Surgery was offered, but the patient was reluctant, and a one-month follow-up was given to reconsider surgery. Two months later, he presented with a visual acuity of (20/100), and OCT showed an enlargement of the macular hole with a diameter of 368 um and a base diameter of 1233 um (Figure 2). Pars plana vitrectomy (PPV) was performed in January 2024, posterior vitreous detachment (PVD) induction followed by staining with trypan blue (Membrane blue dual, DORC, Netherlands). ILM peeling was initiated inferotemporally and advanced nasally then superiorly and concluded with an inverted temporal ILM flap over the hole. At this stage, the flap was not stable over the hole; it was tucked gently with a soft tip cannula, and a dispersive viscoelastic was applied over the flap; careful fluid-air exchange was performed at 30 mmHg with the flap observed flat over the hole, and SF6 20% flush was performed. After the surgery, the patient was instructed to maintain a face-down position. At two weeks postoperatively, the patient reported maintaining a strict face-down position and came with an improved visual acuity to (20/50). OCT showed successful hole closure, and the flap could be seen bridging the fovea (Figure 3). At three months postoperatively, the patient came back to the clinic with a complaint of a very faint central floater. Visual acuity was (20/30), and fundus exam revealed a clear vitreous cavity and a closed hole. OCT showed a partially detached flap that is still hinged temporally to the fovea (Figure 4). No intervention was offered to the patient since the floater is very minimal.
 |
Figure 1 Pre op OCT at the time of presentation showing a full-thickness macular hole with a diameter of 320 um. |
 |
Figure 2 Pre op OCT one month after the initial presentation showing a full-thickness macular hole with an enlarged diameter to 368 um. |
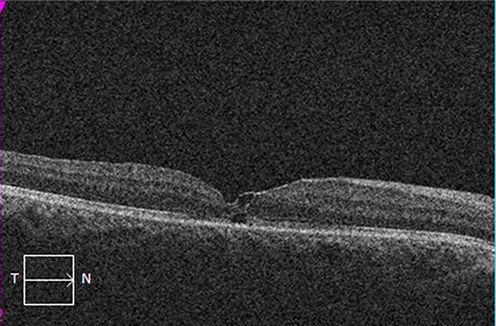 |
Figure 3 An OCT taken two weeks postoperatively showing a closed FTMH with a visible ILM flap attached to the retinal surface bridging the fovea. |
 |
Figure 4 An OCT taken three months postoperatively showing a closed FTMH and a partially detached ILM flat with an intact hinge temporally. |
Discussion
FTMH surgery classically involves PPV with ILM peeling and gas tamponade, which is successful in most cases ranging between 250 and 650 um.4 However, for larger holes, many techniques have been described with a higher success rates than ILM peeling alone, including ILM flaps, free ILM grafts, and amniotic membrane grafts.5 ILM flaps are hypothesized to provide a scaffold for Muller cells to induce enough gliosis and promote hole closure.6 In this case, we elected to perform an inverted ILM flap, however due to the instability of the flap, viscoelastic was utilized to aid in the stability of the flap before performing fluid–air exchange. In Romano’s technique,3 a cohesive viscoelastic is injected into the hole, with subsequent small flaps lying into the viscoelastic in petal flower-like flaps. However, in our case, since the use of viscoelastic was not originally planned and the fear that further manipulation of the flap might lead to its disinsertion from the temporal edge of the hole, we elected to apply the viscoelastic on top of the flap. Early displacement of the ILM inverted flap might occur during fluid–air exchange or soon after surgery due to improper positioning or incomplete tamponade.1 Hinge location might also play a role in flap stability and closure rate. Inferiorly hinged ILM flaps might have better results than the classical nasally hinged flaps.7 Partial detachment of the ILM flap occurred late in our case after the hole was closed. It was expected that glial tissue that formed and helped close the hole would keep the flap attached to the inner retina. Kawamata et al8 reported a case of an early partial detachment of an ILM flap soon after the gas tamponade resolved with spontaneous reattachment of the flap and hole closure. A better understanding of the gliosis process is needed to fully understand the cause of ILM flap detachment in our case.
Patient Consent
Written consent to publish this case has been obtained from the patient himself.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding or grant support.
Disclosure
No conflict of interests, no financial disclosures.
References
1. Michalewska Z, Michalewski J, Adelman RA, et al. Inverted internal limiting membrane flap technique for large macular holes. Ophthalmology. 2010;117:2018–2025. doi:10.1016/j.ophtha.2010.02.011
2. Guohai C, Radouil T, Fangzheng J, et al. Inverted ILM flap technique versus conventional ILM peeling for idiopathic large macular holes: a meta-analysis of randomized controlled trials. PLoS One. 2020;15(7):e0236431. doi:10.1371/journal.pone.0236431
3. Romano M, Alfredo B, Raffaele R. Viscoelastic-assisted inverted cover and free ILM flap techniques. Eur J Ophthalmol. 2021;14:11206721211016976.
4. Ch’ng SW, Patton N, Ahmed M, et al. The Manchester large macular hole study: is it time to reclassify large macular holes? Am J Ophthalmol. 2018;195:36–42. doi:10.1016/j.ajo.2018.07.027
5. Ittarat M, Somkijrungroj T, Chansangpetch S, et al. literature review of surgical treatment in idiopathic full-thickness macular hole. Clin Ophthalmol. 2020;14:2171–2183. doi:10.2147/OPTH.S262877
6. Tam ALC, Yan P, Gan NY, et al. The current surgical management of large, recurrent, or persistent macular holes. Retina. 2018;38:1263–1275. doi:10.1097/IAE.0000000000002020
7. Ghassemi F, Khojasteh H, Khodabande A, et al. Comparison of three different techniques of inverted internal limiting membrane flap in treatment of large idiopathic full-thickness macular hole. Clin Ophthalmol. 2019;27(13):2599–2606. doi:10.2147/OPTH.S236169
8. Yuto K, Takayuki B, Hirotaka Y, Shuichi Y. Partial detachment of internal limiting membrane flap and spontaneous re-covering of macular hole by flap. Am J Ophthalmol Case Rep. 2021;14(22):101089.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preoperative Peripapillary Retinal Nerve Fiber Layer Thickness as the Prognostic Factor of Postoperative Visual Functions After Endoscopic Transsphenoidal Surgery for Pituitary Adenoma
Thammakumpee K, Buddawong J, Vanikieti K, Jindahra P, Padungkiatsagul T
Clinical Ophthalmology 2022, 16:4191-4198
Published Date: 15 December 2022
Case of Spontaneous Closure and Recurrence of Macular Hole in Vitrectomized Eye
Komi Y, Katsumoto T, Yoshikawa Y, Shibuya M, Shoji T, Makita J, Shinoda K
International Medical Case Reports Journal 2023, 16:641-645
Published Date: 2 October 2023
Fovea-Sparing Internal Limiting Membrane (ILM) Peeling and ILM Plug: A Novel Approach for Managing Optic Disc Pit Maculopathy

Chakraborty S, Sheth JU
Clinical Ophthalmology 2024, 18:3343-3351
Published Date: 19 November 2024