")
Back to Journals » Clinical Ophthalmology » Volume 19
Patient Perspectives on Home Tonometer Usage for Glaucoma
Authors Thaprawat P, Dugan SP, Zhang AD
Received 6 November 2024
Accepted for publication 9 January 2025
Published 21 January 2025 Volume 2025:19 Pages 199—207
DOI https://doi.org/10.2147/OPTH.S501234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pariyamon Thaprawat,1 Sarah P Dugan,1,2 Amy D Zhang1
1Department of Ophthalmology and Visual Sciences, W. K. Kellogg Eye Center, University of Michigan Medical School, Ann Arbor, MI, USA; 2Department of Ophthalmology, Casey Eye Institute, Oregon Health and Science University, Portland, OR, USA
Correspondence: Amy D Zhang, Department of Ophthalmology and Visual Sciences, W. K. Kellogg Eye Center, University of Michigan Medical School, 1000 Wall Street, Room 215 Kellogg Tower, Ann Arbor, MI, 48105, USA, Tel +1 734-615-2479, Fax +1 734-232-0864, Email [email protected]
Purpose: To understand patient experiences using the iCare HOME tonometer through assessing ease of use, device usage patterns, proficiency, and patient comments.
Methods: We conducted a prospective survey-based cohort study of 19 patients (35 eyes) with glaucoma or glaucoma suspect diagnoses. Patients received training on home tonometer usage and were loaned the device for one week to measure intraocular pressure at home multiple times daily. Participants completed a journal and survey at the end of the study period.
Results: On average, participants measured intraocular pressure ≥ 4 times per eye each day (4.19± 1.54 OD and 4.06± 1.41 OS). Most found the home tonometer moderately or very easy to use (75% total, 31% and 44% respectively) and would be happy to use the device in the future (94%). The home tonometer was deemed comfortable to use (94%). Most participants were able to use the device without assistance from another person (88%). Many felt that they became proficient at using the home tonometer (94%) and proficiency was achieved typically by day 3 of usage. Patient comments provided insight into sources of difficulty in usage and motivations for home tonometry.
Conclusion: Home tonometry was easy to use and comfortable for most patients with proficiency in usage quickly achieved by day 3. Surveying patient perspectives revealed sources of difficulties in home tonometer usage. Patients were eager to obtain home intraocular pressure measurements that could help with disease management.
Keywords: glaucoma, home tonometry, rebound tonometry, ease of use, proficiency
Introduction
Glaucoma is a chronic disease and one of the leading causes of blindness worldwide.1 Vision loss in glaucoma is mainly due to optic nerve damage from increased intraocular pressure (IOP), a significant risk factor that needs to be monitored and carefully controlled.2 Monitoring and management of IOP is therefore a primary goal for patient care. Current therapeutics for glaucoma also target IOP reduction. It is essential for patients to regularly obtain accurate IOP measurements as they serve as key data points in determining disease status, assessing therapeutic efficacy, and guiding treatment decisions. Most commonly, in-person testing and evaluation of IOP are required in the clinic or hospital settings. As glaucoma is a lifelong disease, this places a large burden on many patients due to the frequency of IOP testing that is required for proper management. Additionally, IOP measurements can undergo diurnal fluctuations that may not be accurately captured from a single measurement taken in the clinic or hospital.3–5
The current gold standard for measuring IOP is Goldmann applanation tonometry (GAT) due to its reliability and reproducibility.6 However, GAT requires a trained professional for proper IOP measurement and can only be performed in the clinic or hospital setting. Home tonometry offers a promising solution that may lead to more robust glaucoma patient care with an increasing number of devices that have been developed for measuring IOP at home including rebound tonometry devices such as the iCare HOME tonometer (HT) approved by the Food and Drug Administration for home use.7,8 Comparisons of IOP measurements obtained with GAT and HT have shown moderate to high agreement in accuracy.9–12 Multiple studies have also demonstrated that home tonometry with the HT is feasible and reliable.13,14 However, few studies have comprehensively reviewed patient reports regarding ease or difficulty of use, which has direct implications for patient compliance in using the HT device.
The purpose of this pilot study was to better understand the patient’s perspective on using a HT by assessing ease of use, device usage patterns, and proficiency ratings. Patients were able to take home the HT for one week. The longer duration allowed patients to fully familiarize themselves with the HT and assess its ease of use over this period. While other studies have mainly focused on validating the accuracy of IOP measurements taken with the HT or the feasibility of training and usage,9–15 our study places greater emphasis and focus on the patient experience using the HT device. Gaining a better understanding of the patient’s perspective will allow for potential improvements in training, device design, and an overall wider acceptance and integration of home tonometry in glaucoma patient care.
Materials and Methods
This was a prospective survey-based cohort study involving 19 patients with glaucoma or glaucoma suspect diagnoses recruited from Kellogg Eye Center, Ann Arbor, MI, USA. Institutional Review Board (IRB) approval was obtained for this study. This study adhered to the tenets of the Declaration of Helsinki.
Participants were recruited from a subset of patients with glaucoma or glaucoma suspect diagnoses who previously expressed interest in using HT (iCare HOME, (TA022, Icare Oy, Vanda, Finland). Patients for whom the HT device was clinically indicated were scheduled for an appointment to receive the device and receive device training regardless of their participation in the study. A study team member reviewed the medical records of patients scheduled to receive HT to screen for eligibility in the study. Patients with a history of LASIK, corneal surgery, severe dry eye, or recent cataract and other ocular surgery (within 3 weeks) were excluded as these conditions may impair IOP measurement acquisition with the HT and use may introduce unsafe conditions. Other exclusion criteria included patients with corneal pathology, including keratoconus and Fuch’s dystrophy. Patients with diseases that significantly limited mobility, such as severe arthritis, Parkinson’s disease, or other movement disorders were excluded, as these patients may have difficulty manipulating the HT device. Those without any exclusionary criteria were contacted by phone by a study team member for recruitment to participate in the study. Informed consent was obtained over the phone.
Enrolled patients underwent standardized training prior to device use. Patients were loaned an iCare HOME device for one week and were instructed to measure their IOP multiple times throughout the day. At their appointment to receive the HT, enrolled patients were also given a journal template to help keep responses consistent in formatting and organization, a copy of the consent form for their records, directions on how to participate in the study, and a survey to be filled out at the end of the study period. All documents were pre-labeled with a unique study ID. The medical record number (MRN) that correlated with a patient’s ID was saved in a document separate from the main database of patient information and stored on an encrypted document in a HIPAA-compliant, secure DropBox folder. iCare HOME automatically uploaded IOP data onto a HIPAA-compliant database as part of its design.
The survey asked participants to respond to 16 questions as follows:
- How easy was it to use iCare HOME? (5-point Likert scale) and comments.
- If you found it difficult to use iCare HOME, which steps were challenging?
- Did you require assistance from another person to use the device?
- Were there any barriers to obtaining regular measurements (4–6x a day)?
- How comfortable was it to take measurements with iCare HOME? (5-point Likert scale) and comments.
- How happy would you be to use this device in the future? (5-point Likert scale) and comments.
- Did you feel that you became more proficient at using iCare HOME as the week went by? Around what day after receiving the device did you feel fully proficient?
- Which part of the training to use the iCare HOME did you find most helpful?
- Have you had experience with home medical devices in the past? Please list.
- What changes would you make to the device?
- Did you take your measurements before or after taking eye drops?
- What is your race/ethnicity?
- What is your highest level of education?
- What is your dominant hand?
- Which eye did you measure the pressure in?
- Which hand did you use to hold iCare HOME when measuring your IOP?
Results
Study participants were 50% men and 50% women, with a mean age of 60.75 years and a range of 42 to 82 years. Our study recruited 19 patients who received a HT device loan, of which 16 completed the end of study survey and 12 completed the home journal. As the end of study survey was our main outcome, we excluded the three patients with incomplete surveys. The full demographics and clinical characteristics of study participants are listed in Table 1.
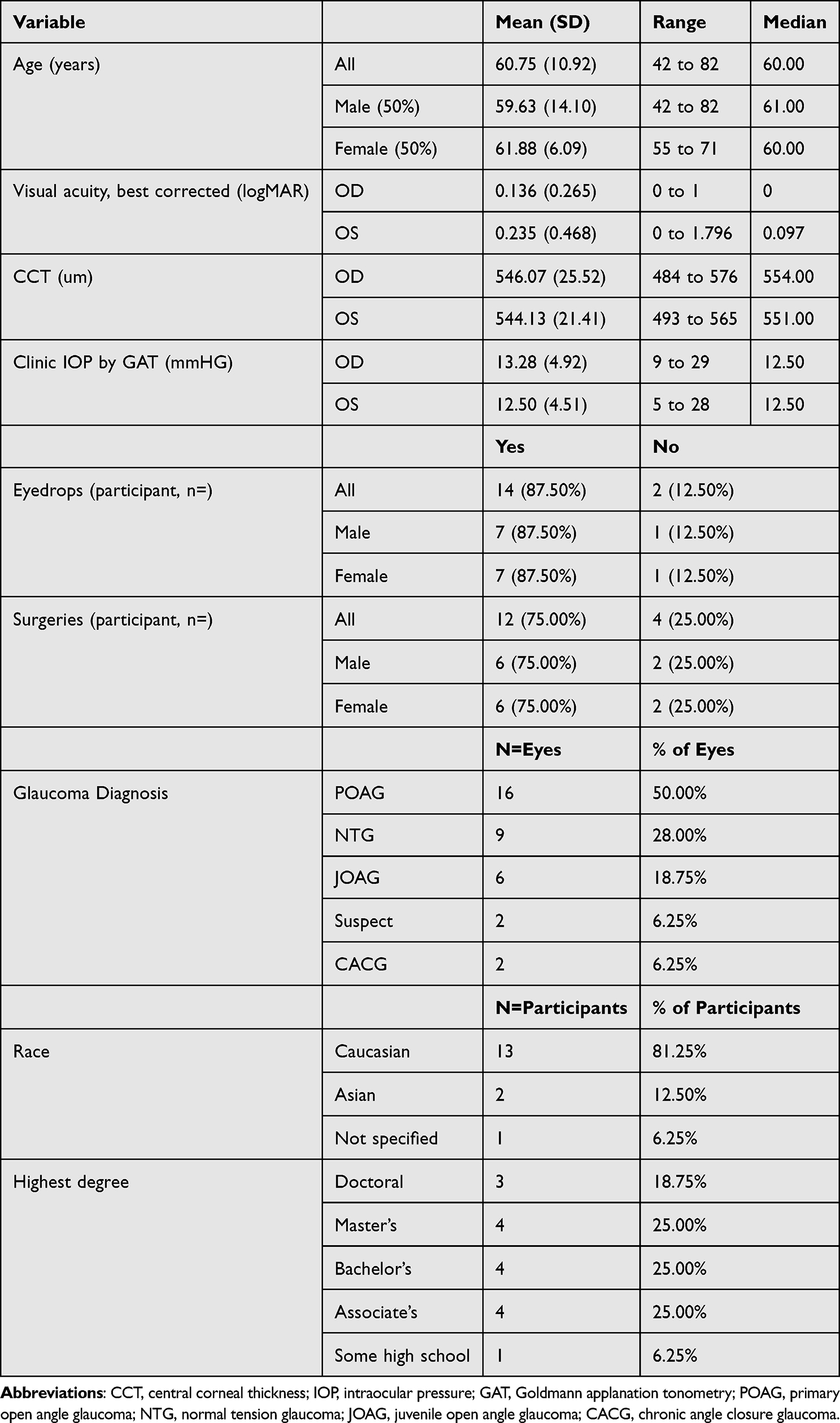 |
Table 1 Demographics and Clinical Characteristics of Participants |
Characteristics of Device Usage
Regarding characteristics and patterns of HT device usage, 100% of participants took IOP measurements in both eyes. While 87.5% reported right hand dominance, 56% used their right hand only to hold the device, 38% used both hands, and 6% used their left hand only (Figure 1A). In relation to eye medications, 88% reported that measurements were taken both before and/or after eyedrops (Figure 1B). While patients were instructed to try to take multiple measurements each day using the HT device, a barrier noted by many patients included remembering to do so, especially on busy days working, running errands, or at nighttime. Some noted that it was difficult to bring the device with them when not at home, which decreased the total number of measurements obtained each day. Nonetheless, patients obtained on average at least four IOP measurements in each eye per day (4.19±1.54 OD and 4.06±1.41 OS) (Figure 1C).
 |
Figure 1 Characteristics of patient usage of home tonometer (HT) device. (A) Descriptions of handedness when using device and eyes in which measurements were obtained. Inset values represent percentages (%). (B) Pie chart visual representation of when measurements were obtained in relation to medications or eyedrops. (C) Average number of intraocular pressure (IOP) measurements taken per day, per eye ± standard deviation. |
Perspectives on Ease of Use
We surveyed patient perspectives on general HT device ease of use and 75% reported a rating of “moderately easy” or “very easy” (31% and 44%, respectively) (Figure 2A). Specific comments listed in survey responses and journal entries highlighted issues aligning the device for proper measurements or adjusting the forehead and cheek sliders to sit properly. Other patients reported trouble seeing the light cues emitted from the device when trying to take measurements, especially in an eye with low vision. Additionally, the beeping sounds from the device were not intuitive to understand for some patients. The device emits normal short or long beeps when measurements are being taken, however various combinations of light flashes and long or short beeps indicate a specific error depending on the combination. For example, when the probe base light is flashing red accompanied by 3 long beeps, this indicates that the probe is positioned too far from the eye while 5 short beeps paired with the same light flashes indicates that the probe is too close to the eye. In terms of comfort when taking measurements, 94% reported a rating of “moderately comfortable” or “very comfortable” (25% and 69%, respectively) (Figure 2B). A large majority of patients (94%) reported that they would be “moderately happy” to “very happy” to use the HT device in the future (13% and 81%, respectively) (Figure 2C). While the majority reported high comfort in device usage, sources of discomfort included the bright lights from the device, especially with nighttime use. Additionally, prolonged attempts at measurement led to patient discomfort if the first measurement attempt was unsuccessful. Most patients (88%) were able to use the device independently without the need for assistance from another person (Figure 2D). A recurring theme from survey and journal entries was patient appreciation for getting more data points for their IOP measurements and its role in disease management. However, many were curious about the actual IOP measurements obtained and would have liked to see the readings in real-time displayed on the device itself. A few patients would have also liked a mechanism to improve probe stability on the device along with a cover for the probe.
 |
Figure 2 Patient perspectives on ease-of-use of home tonometer (HT) device. Pie chart visual representations of participants’ survey answers to ease-of-use related survey questions. (A) Responses regarding ease of use of HT based on a 5-point Likert scale. (B) Responses regarding comfort of HT based on a 5-point Likert scale. (C) Responses regarding use of HT in the future based on a 5-point Likert-scale. (D). Responses regarding requirement of assistance to use HT. |
Training and Proficiency
In-person training with an ophthalmic technician was most often reported as the most helpful part of HT device training, with many patients commenting on its essential role in gaining familiarity with using the device. Notably, a trained technician was helpful for obtaining the correct forehead and cheek measurements to ensure correct device alignment for some patients. Additional training materials deemed helpful included printed handouts with written and photographic instructions and other resources such as online videos (Figure 3A). Most patients (94%) reported that they became more proficient at using the HT device over their loan period (Figure 3B). Most patients reported proficiency by day 3 after receiving training with the HT device, with some gaining proficiency slightly earlier or later (Figure 3C). One patient reported in journal entries that it took about 20–30 minutes to obtain measurements the first few days with the device, but this process only took 5 minutes after multiple uses over time a few days later, demonstrating a common pattern of how patients gained proficiency in device usage over time. Most patients (62%) reported prior experience with home medical devices, while 38% had never used another home medical device (Figure 3D). The most commonly used devices were blood pressure monitors, CPAP machines, or glucose monitors.
 |
Figure 3 Training and proficiency of home tonometer (HT) device. Visualization of participant responses to survey questions related to training on device usage, proficiency, and experiences using other home medical equipment. (A) Responses regarding training helpfulness. (B) Responses regarding perceived proficiency after usage of HT over time. (C) Depiction of time to self-reported proficiency after receiving HT device. (D) Responses regarding prior experience with home medical devices. |
Discussion
Our small cohort study demonstrated that glaucoma patients were generally receptive to the use of HT in their disease management. Most patients found that the HT was relatively easy to use (75%), comfortable (94%) and would be happy to use the device in the future (94%). There is a need for more robust measurements of patient IOP data in glaucoma management and positive patient experiences with HT highlight its potential role in more comprehensive care. Relying only on clinic or hospital based IOP measurements places a burden on patients to have easy and reliable access to these settings, which is not feasible for certain patient demographics such as those with high travel burden to the nearest glaucoma care provider, those more likely to be lost to follow-up, and those with a lack of glaucoma education or awareness.16–19 Home tonometry can address this gap and add to the growing field of teleophthalmology, decreasing the frequency of in-person visits that are required by patients.20
Regarding patient device usage patterns, we found that some patients preferred to hold the device with only their dominant hand (56% right hand only or 6% left hand only) while others were more comfortable using both hands to hold the device (38%) while taking IOP measurements. Examples of barriers that prevented consistent usage of the device included forgetting the device when patients left their homes or inconvenience at nighttime. Despite this, we found that patients on average took at least 4 IOP measurements per day which is beneficial in capturing any diurnal fluctuations in their IOPs. From patient responses in our study, we can derive potential suggestions on HT design that could improve the overall patient experience. First, most patients are highly curious to learn about their IOP measurements, however, the device does not display IOP readings and there is no easy way for patients to access this information. The rationale behind this feature is to decrease unnecessary patient anxiety from IOP measurements, although few studies have directly shown negative impacts of patient knowledge of IOP.8 Our study highlights the potential motivating role of real-time IOP display for more consistent patient adherence to HT usage. If patients can readily know their IOP measurements, they may be more likely to also adhere to their glaucoma medication regimen. While there is not a clear solution to this design concern, we offer potential changes that can better balance patient and manufacturer concerns rather than full omission of IOP data to patients. One suggestion includes a dichotomous display of either “normal” or “abnormal” based directly from patient data points obtained by their HT device. If the HT can integrate patient data and analyze their diurnal patterns, perhaps it could compute an acceptable range of IOPs that would be considered that patient’s norm, while alerting them if their IOP falls outside this range. Alternatively, IOP data could be easily accessed in a mobile application or portal-based system that would still provide patient agency in management of their data. These small changes would greatly promote active patient participation in management of their disease. In fact, while our study was being conducted, an updated version of HT was released (iCare HOME 221) that now allows patients to directly visualize their IOP trends in a mobile app. Additionally, physicians can directly work with patients to set a pre-determined limit for IOP that would trigger Email notifications to their provider if their HT readings exceeded the limit. An additional design feature that our study participants wanted to improve included the sometimes-confusing beeping alerts that indicated some type of error when obtaining measurements. In the new version of HT, the device now possesses a digital display that accompanies the beeps emitted for easier interpretation with clear indications of measurement quality. One of our study participants commented on the brightness of the light from the HT as a source of discomfort while taking measurements, especially at night. The new version of HT now comes equipped with a way for users to adjust the brightness settings. A common source of measurement error is a misaligned device when held for use against the patient’s face. Many of our study participants found it difficult to get the proper alignment while holding the device, which would prompt error messages. The new version of HT has an alternate design for forehead and cheek placement adjusters that are slightly more angled than the previous version, which could improve alignment issues. While there is no clear reminder system in place to prompt patients to measure IOPs at home, implementing such a system would help with more accurate data collection and visualization of true IOP trends throughout the course of a day, which is known to fluctuate in a diurnal pattern.3–5 We suggest that this feature could easily be integrated into the mobile app that would send alerts to patients to remember to take measurements at regular intervals throughout the day.
Over the course of one week, most of our participants reported proficiency in using the HT by day 3 after receiving training to use the device. To our knowledge, this is the first report of temporal data in patient proficiency trends using HT. This supports our data on patient ease of use and is an important consideration when training patients to use the HT for the first time. Some patients may find that there is a learning curve to using the HT and should be reassured that repeated practice can lead to proficiency. Interestingly, our study highlights the critical role of in-person based training with a knowledgeable technician or provider, which was regarded as the most helpful part of training on HT usage. While printed or online resources may be available, in-person teaching will likely remain a key factor in patient success with using the HT. While our study did not include this form of teaching, the use of a remote video link has also been shown to be successful in teaching home tonometry.22 While some of our study participants had experience using other home medical devices (62%) such as blood pressure monitors, CPAP machines, or glucose monitors, others had never used another home medical device (38%).
Home tonometry is overall a positive experience for glaucoma patients with high ratings on ease of use and proficiency. Understanding the patient’s perspective in home tonometry is essential to increase acceptance, adherence, and wider integration of this technology in disease management. With a relatively fast timeline to proficiency in using the HT device, many patients would benefit from home tonometry for better monitoring of their chronic disease.
Study Limitations
Our study has some limitations including its small sample size and relatively homogenous patient population. Participants were recruited from a group of patients who had previously expressed interest in using the HT device, therefore our study results could be skewed towards higher acceptance or more inviting answers of using the HT device. While our end-of-study survey design had a 5-point Likert scale for most questions, we also solicited responses in the form of comments to better understand a specific rating given by a participant. Some participants were more descriptive and detailed in their responses, while others did not provide comments. Similarly, the journaling portion of our study had inconsistencies in the number of entries and descriptions. This may have limited our interpretation of patient experiences in using their HT devices. In-person training was provided by a set of trained technicians, which may lead to variable degrees of support in device training depending on the teaching style of the technician. This is a limitation as it may directly influence the level of proficiency or time to proficiency for our participants.
Acknowledgments
The authors thank all the technicians at Kellogg Eye Center Glaucoma Clinic that provided training to patients on device usage and for their help in supporting study participant recruitment.
Funding
There is no funding to report.
Disclosure
Sarah P Dugan was affiliated with University of Michigan Medical School at the time the study was conducted. The authors report no conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Leske MC. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003;121(1):48. doi:10.1001/archopht.121.1.48
3. Leidl M, Choi CJ, Syed ZA, Melki SA. Intraocular pressure fluctuation and glaucoma progression: what do we know? Br J Ophthalmol. 2014;98(10):1315–1319. doi:10.1136/bjophthalmol-2013-303980
4. Caprioli J, Kim J. Intraocular pressure fluctuation: is it important? J Ophthalmic Vis Res. 2018;13(2):170. doi:10.4103/jovr.jovr_35_18
5. LiGHT China Trial Study Group; Yang Y, Zhang X, Chen Z, et al. Intraocular pressure and diurnal fluctuation of open-angle glaucoma and ocular hypertension: a baseline report from the LiGHT China trial cohort. Br J Ophthalmol. 2023;107(6):823–827. doi:10.1136/bjophthalmol-2021-320128
6. Goldmann H, Schmidt T. Über Applanationstonometrie. Ophthalmologica. 1957;134(4):221–242. doi:10.1159/000303213
7. Aziz K, Friedman DS. Tonometers—which one should I use? Eye. 2018;32(5):931–937. doi:10.1038/s41433-018-0040-4
8. Liu J, De Francesco T, Schlenker M, Ahmed II. Icare home tonometer: a review of characteristics and clinical utility. Clin Ophthalmol. 2020;14:4031–4045. doi:10.2147/OPTH.S284844
9. Dabasia PL, Lawrenson JG, Murdoch IE. Evaluation of a new rebound tonometer for self-measurement of intraocular pressure. Br J Ophthalmol. 2016;100(8):1139–1143. doi:10.1136/bjophthalmol-2015-307674
10. Takagi D, Sawada A, Yamamoto T. Evaluation of a New Rebound Self-tonometer, Icare HOME: comparison with Goldmann applanation tonometer. J Glaucoma. 2017;26(7):613–618. doi:10.1097/IJG.0000000000000674
11. Mudie LI, LaBarre S, Varadaraj V, et al. The Icare HOME (TA022) Study. Ophthalmology. 2016;123(8):1675–1684. doi:10.1016/j.ophtha.2016.04.044
12. Quérat L, Chen E. iCare® home vs Goldmann applanation tonometry: agreement of methods and comparison of inter-observer variation at a tertiary eye centre. European J Ophthalmol. 2022;33(1):312–318. doi:10.1177/11206721221099252
13. Cvenkel B, Velkovska MA, Jordanova VD. Self-measurement with Icare HOME tonometer, patients’ feasibility and acceptability. European J Ophthalmol. 2019;30(2):258–263. doi:10.1177/1120672118823124
14. Hu GY, Prasad J, Chen DK, Alcantara-Castillo JC, Patel VN, Al-Aswad LA. Home monitoring of glaucoma using a home tonometer and a novel virtual reality visual field device: acceptability and feasibility. Ophthalmol Glaucoma. 2022;6(2):
15. McGlumphy EJ, Mihailovic A, Ramulu PY, Johnson TV. Home self-tonometry trials compared with clinic tonometry in patients with glaucoma. Ophthalmol Glaucoma. 2021;4(6):569–580. doi:10.1016/j.ogla.2021.03.017
16. Altangerel U, Nallamshetty HS, Uhler T, et al. Knowledge about glaucoma and barriers to follow-up care in a community glaucoma screening program. Can J Ophthalmol. 2009;44(1):66–69. doi:10.3129/i08-175
17. Rothman AL, Stoler JB, Vu DM, Chang TC. A geodemographic service coverage analysis of travel time to glaucoma specialists in Florida. J Glaucoma. 2020;29(12):1147–1151. doi:10.1097/IJG.0000000000001648
18. Foot B, MacEwen C. Surveillance of sight loss due to delay in ophthalmic treatment or review: frequency, cause and outcome. Eye. 2017;31(5):771–775. doi:10.1038/eye.2017.1
19. Varma R, Lee PP, Goldberg I, Kotak S. An assessment of the health and economic burdens of glaucoma. Am J Ophthalmol. 2011;152(4):515–522. doi:10.1016/j.ajo.2011.06.004
20. Faes L, Bachmann LM, Sim DA. Home monitoring as a useful extension of modern tele-ophthalmology. Eye. 2020;34(11):1950–1953. doi:10.1038/s41433-020-0964-3
21. iCare HOME2. iCare. Available from: https://www.icare-world.com/us/product/icare-home2/.
22. Barbour-Hastie CC, Tatham AJ. Teaching home tonometry using a remote video link. Eye. 2022;37(3):501–505. doi:10.1038/s41433-022-01966-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.