")
Back to Journals » Clinical Ophthalmology » Volume 18
Pattern and Prevalence of Retinal Vein Occlusion in Bhutan: A 3-Year National Survey at Vitreoretinal Clinics
Authors Rai BB , Dorji P , Maddess T
Received 9 May 2024
Accepted for publication 7 October 2024
Published 17 October 2024 Volume 2024:18 Pages 2939—2949
DOI https://doi.org/10.2147/OPTH.S477559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr John Miller
Bhim B Rai,1,2 Phuntsho Dorji,2 Ted Maddess1
1John Curtin School of Medical Research, Australian National University, Canberra, ACT, Australia; 2Department of Ophthalmology, JDW National Referral Hospital, Thimphu, Bhutan
Correspondence: Bhim B Rai, Building 131, Garran Road, John Curtin School of Medical Research, Australian National University, Canberra, ACT, 2601, Tel +61 2 61259253, Email [email protected]
Purpose: We conducted this study to determine the pattern and prevalence of retinal vein occlusion (RVO) in Bhutan to inform national health policy as no data has been compiled previously.
Methods: A retrospective cross-sectional survey was conducted over 3 years, including all new RVO cases. For patients with bilateral RVO, one eye was chosen randomly. Demographic, clinical, and diagnostic details, including optical coherence tomography, fluorescein angiography, and fundus photography, were collected.
Results: Of 141 RVO new patients included, aged 50.5 ± 20.2 years, there were more males (62.4%) than females (37.6%) significantly (p = 0.031), and 59.6% of total patients were from an urban setting. Farmers were the most affected group (44, 31.2%), followed by housewives (34, 24.1%), and the working group (33, 23.4%). Blurry vision (64, 45.5%), sudden loss of vision (17, 12.1%), including unsatisfactory cataract surgery (8, 5.7%) were common presenting complaints. Systemic hypertension (HT) (36, 25.5%), and diabetes mellitus (DM) (17, 12.1%), were associated systemic diseases. The prevalence of RVO was 4.8% (141/2913 all new retinal patients over the survey). Branch RVO (BRVO) was the most common type (77, 54.6%), followed by central RVO (CRVO) 56, (39.7%), and hemi-central RVO (HCRVO) (8, 5.7%). Superotemporal BRVO was the most common subtype (30, 39%) followed by inferotempoal (19, 24.7%). Best correct visual acuity (BCVA) was worse than 6/60 in 38 eyes (25.5%). BCVA was not significantly different between BRVO and CRVO eyes. Intraocular pressure was significantly lower in HCRVO eyes (p = 0.015) compared to BRVO and CRVO eyes.
Conclusion: In Bhutan, 8.5% of RVO patients were bilateral. HT was associated significantly as a risk factor. Incidental findings of RVO during routine eye check-up and evaluating for unsatisfactory cataract surgery were common. Therefore, Bhutan needs to control noncommunicable diseases such as diabetes and HT to reduce RVO, and RVO-related blindness and complications.
Keywords: anti-VEGF, avoidable blindness, complications of diabetes and hypertension, retinal vein occlusion in Bhutan, risk factors of retinal vein occlusion, vitreoretinal disease in Bhutan
Introduction
Retinal vascular diseases are the major causes of visual impairment and loss of central vision.1 Among these, retinal vein occlusion (RVO) is one of the most common causes of acquired retinal vascular abnormality and is the second leading cause of retinal vascular blindness after diabetic retinopathy (DR).2 It is an obstruction of the retinal venous system by a thrombus or an embolism. It progresses by two major disease mechanisms: first, alteration to the inner blood-retinal barrier with resultant increased vascular permeability and oedema; and second, vessel closure with resultant ischaemia leading to the development of abnormal neovascularisation. Major risk factors for RVO include arterial hypertension, atherosclerosis, diabetes mellitus (DM), an increased body mass index, and cardiovascular disease.3 Risk of RVO was decreased by high-density lipoprotein cholesterol and alcohol consumption.3 RVO is divided into two main types: Central RVO (CRVO) and branch RVO (BRVO). In CRVO, the main retinal vein is occluded behind the lamina cribrosa of the optic nerve and is typically caused by thrombosis. CRVO is further divided into two categories: non-ischaemic (perfused) and ischaemic (nonperfused) types. BRVO is a blockage of one of the tributaries of the central retinal vein.4 A two-trunked central retinal vein may persist in the anterior part of the optic nerve as a congenital abnormality. One trunk may get occluded to produce hemi-central RVO (HCRVO), which is pathogenically and clinically a distinct entity closely related to CRVO, but not related to BRVO. CRVO occurs at the site where the CRV crosses the lamina cribrosa and is almost always thrombo-embolic in origin.5 It may involve the central, hemi-central or branch retinal vein resulting CRVO, HCRVO, and BRVO, respectively. A population-based study reported an incidence of symptomatic RVO at 2.14 per 1000 among the population aged 40 years or more, with a significant increase with age.6 The Beaver Dam Eye Study reported an incidence of 0.6%, and additionally found the RVO was associated with hypertension, DM, pulse pressure, ocular perfusion pressure, arteriovenous nicking, and focal arteriolar narrowing.7 A population-based study in Nepal reported an RVO prevalence of 2.95% in a population group of 65 to 95 years,8 and RVO was the fourth most common vitreoretinal (VR) disease presenting to a tertiary eye care centre.9 In Bhutan, RVO was the fifth most common VR disorder presenting to the national referral hospital,10 the second most common reason for retinal laser therapy11 as well as intravitreal injections of anti-vascular endothelial growth factor (anti-VEGF).12
The aim of the current study was to report on the pattern and prevalence of RVO in Bhutan. Since this is the first study of this kind in the country, the results have impacts for policy making in Bhutan. The data from this study will guide the development of national health programs to understand, screen and manage RVO in Bhutan. The information will be useful to other developing countries in the region, and globally for planning and implementation of robust blindness control measures.
Methods
The current article reports on the datasets of the national survey of VR diseases in Bhutan, which has generated several publications.10,11,13–17 Therefore, the description of methods section may overlap with these reports.
Study Design and Ethics
This was a retrospective cross-sectional observational study approved by the Research Ethics Board of Health (REBH) (REBH/Approval/2016/083), Ministry of Health, Royal Government of Bhutan, Thimphu, Bhutan. This study adhered to the principles of the Declaration of Helsinki. Informed consent was waived by REBH because this retrospective study collected only de-identified data.
Setting
The Jigme Dorji Wangchuck (JDW) national referral hospital is the apex national referral and teaching hospital and the only hospital with subspecialty eye-care services. Regular VR surgical and interventional services in the country are provided only at the JDW national referral hospital. All such VR patients across the country are referred there for management. Occasionally the VR surgeon visits Eastern Regional Referral Hospital (ERRH) in Mongar and Central Regional Referral Hospital (CRRH) in Gelephu when the treatment is provided there. The sites for the current study included mainly JDW national referral hospital, and ERRH and CRRH. The VR patients from the entire country are referred to and managed in these three hospitals, mainly at the JDW national referral hospital, making this study the first national survey on RVO in Bhutan. However, all referred patients might not have reported to the VR clinics due to inconvenience in transport or referral services. To mitigate this bias, screening of RVO cases was conducted regularly in association with the diabetes and hypertension clinics in district hospitals and peripheral health centres. All diagnosed RVO cases were referred properly and transport facilities were provided to the patients and an attendant. The VR clinics of the jurisdiction were informed about the referrals and contact details of the patients.
Participants
Inclusion criteria included new RVO patients, presenting to the VR sub-speciality clinic (VRSC) at the JDW national referral hospital, and VR clinics in ERRH and CRRH, and within the study period (01 May 2013 until 30 April 2016). Exclusion criteria included RVO patients who presented for follow-up. The demographic characteristics of patients represent the entire citizenry.
Clinical Examination
The clinical workup in the out-patient department (OPD) included taking detailed medical histories of presenting symptoms and diseases, associated systemic diseases, and prior surgical or laser interventions done. Best corrected visual acuity (BCVA) at presentation was measured using a Snellen chart and Tumbling E for illiterate patients. Intraocular pressure (IOP) was measured by Goldmann applanation tonometry or an iCare tonometer. The anterior and posterior segments were examined under slit-lamp biomicroscopy (BM 900, Haag-Streit, Switzerland) and 90D bio-microscopy. The funduscopic findings were confirmed by binocular indirect ophthalmoscope (Model 125, Welch Allyn, USA). Macular and retinal nerve fibre (RNFL) scans were measured using a Spectral Domain Optical Coherence Tomography (OCT) (Cirrus-HD 4000, Carl Zeiss Germany). OCT was performed to note the severity of the macular oedema (MO) for documentation, to explain to the patients and for prognostic evaluation following treatment. Fundus photographs were taken by a VISUCAM-524 (Carl Zeiss, Germany) for similar reasons. Fundus fluorescein angiograms (FFA) and B-ultrasonogram scans were performed when necessary (Sonomed Escalon, Model: VUPAD A/B, USA). FFA was done to differentiate between the ischaemic and non-ischaemic type of RVO to decide the management approach. B-ultrasound was mainly performed among patients with media opacity such as vitreous haemorrhage to rule out retinal detachment. Visual field tests (VFTs) were performed with Humphrey Field Analyzer (HFA 3, Carl Zeiss, Germany), and Frequency Doubling Technology (FDT) perimetry (Carl Zeiss Meditec, Dublin, California USA). When indicated, imaging diagnostics such as magnetic resonance imaging (MRI) scans were performed to diagnose or rule out intracranial and orbital pathologies. The results of these imaging diagnostics were provided by the qualified radiologists. Other tests included chest X-rays and Mantoux skin tests to rule out tuberculosis among RVO cases with associated retinal vasculitis. Grading of hypertensive retinopathy has already been reported in an earlier publication.10 Therefore, it is not described in detail in here.
The diagnosis of RVO was based on the clinical findings inferenced by the VR specialist from retinal photographs, OCT reports, and the FFA patterns. For this study, the classification of RVO was mainly based on clinical findings and the retinal photographs providing anatomical classification.
Data Collection and Management
For the current study, the patient registers maintained in the VRSC, and the patient files were reviewed for the data collection. The data collected included demographic information such as age and gender, residential settings, BCVA, diagnostic tests performed, and diagnoses. The collected data were entered into a password protected XLSX spreadsheet by a trained VR assistant with good knowledge of VR diseases and different terminologies. This was counterchecked by the VR specialist (Rai BB).
Statistical Analysis
The data were analysed using MATLAB (2020b, The MathWorks, Natick, MA, USA). Comparisons of the expected and observed frequencies used Chi-squared tests. Other comparisons used paired or unpaired t-tests as applicable. Our main comparison was the relative prevalence of BRVO vs CRVO. We used G*Power (University of Kiel) to examine the power to detect a difference from equal prevalence using a Chi-squared test. To obtain p = 0.05 at a power of 0.95 required a Non-centrality Parameter of 13. Preliminary examination of the data indicated a value >13.
Results
Demographic Characteristics
A total of 141 new patients with RVO presented during the study period. The mean age of presentation was 50.5 ± 20.2 years. Majority of them were males (88, 62.4%), and from urban setting (84, 59.6%). Compared to an expectation of 50% males their rate was significantly higher (p = 0.031, χ2=6.13) (Chi-squared test). Farmers were the most affected group (44, 31.2%), followed by housewives (34, 24.1%), and employees or the working group (33, 23.4%). Other demographic characteristics are shown in Table 1.
 |
Table 1 Demographic Characteristics of Patients |
Presenting Complaints
Blurry vision was the most common presenting complaints (64, 45.4%), followed by sudden loss of vision (17, 12.1%). Other details are shown in Table 2.
 |
Table 2 Presenting Complaints |
Associated Systemic Diseases
Sixty-one patients did not have any associated systemic diseases. In the remaining 80 patients the associated systemic diseases were found as shown in Table 3.
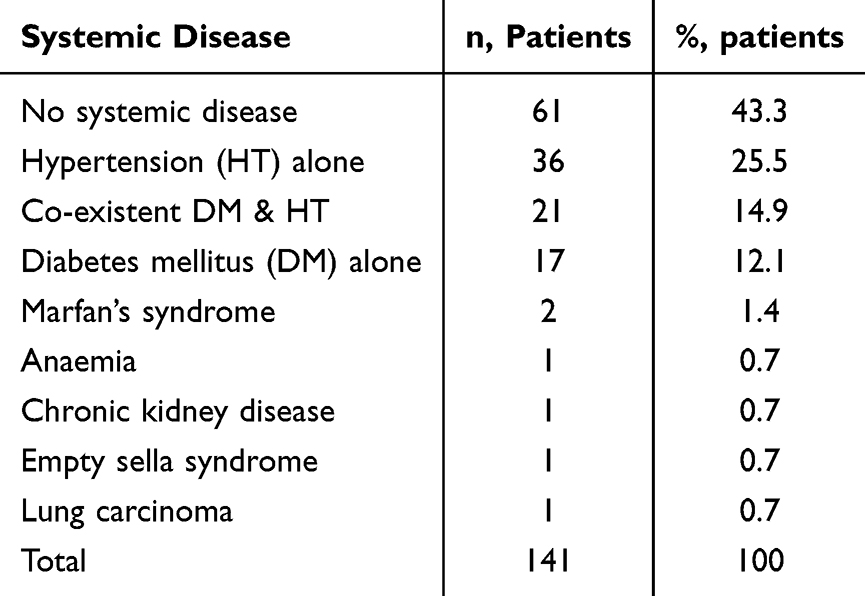 |
Table 3 Associated Systemic Diseases |
Prior Interventions
Before the presentation to the VRSC or VR clinics for consultation, 9 patients had received cataract operation with intraocular lens implantations, 3 patients each had received retinal laser therapy, and retinal detachment surgery. Two patients received primary corneal tear repair.
Visual Acuity
The number of eyes with BCVA worse than 6/60 was 38% or 25.5%, 19 persons bilaterally and so legally blind. The number with 6/12 or better was 70% or 47.0%. The distributions of the number of eyes according to the level of BCVA is depicted in Figure 1A. Figure 1B shows the probability of a given BCVA. These were only computed for BRVO and CRVO because there were insufficient number of HCRVO eyes to reliably estimate the probabilities. The differences in probabilities for BRVO and CRVO were not statistically significant.
 |
Figure 1 Best corrected visual acuity in the eyes with retinal vein occlusion. (A) the number of eyes for each condition. (B) the probability of encountering a given BCVA outcome for BRVO and CRVO. Abbreviations: CF, Counting fingers; HM, Hand movement; NA, Not accessible; NPL, No perception of light; PL, Perception of light. |
Diagnostic Tests
Haematological tests for blood sugar, lipid profile and total blood counts were the most common diagnostic tests in 74 patients (52.5%), followed by OCT in 70 patients (49.6%), retinal photography in 26 patients (18.4%), fundus fluorescein angiogram (FFA) in 23 patients (16.3%), ocular B-scan ultrasound in 18 patients (12.8%), refraction in 12 patients (8.5%), magnetic resonance imaging in 8 patients (5.7%), visual field test in 7 patients (5.0%), X-ray skull in 3 patients (2.1%), Mantoux skin test for tuberculosis in 2 patients (1.4%), X-ray chest in 2 patients (1.4%), and CT-scan in one patient (0.7%). We compared the IOP in the BRVO and CRVO eyes. They were not significantly different at 14.3 ± 2.06 mm Hg and 14.5 ± 2.20 mm Hg, respectively (mean ± SE, p = 0.243) (t-test). When the combined BRVO and CRVO cases were compared with HCRVO, the latter had significantly lower IOP at 12.6 ± 2.76 mm Hg (p = 0.015) (t-test). However, one eye with an IOP of 74 mm Hg with neovascular glaucoma secondary to HCRVO had been excluded for this analysis, leaving only 7 cases.
Retinal Vein Occlusion: Types and Sub-Types
The prevalence of RVO among the patients presenting to the VR clinics was 4.8% (141 new RVO patients divided by 2913 all new retinal patients examined in the VR clinics over the study period). Here, we have classified the RVO according to the morphological types. BRVO was the most common type of RVO affecting 77 patients (54.6%), followed by CRVO with 56 patients (39.7%), and hemi-central RVO with 8 patients (5.7%). Within the sub-group of BRVO cases, superotemporal BRVO (ST BRVO) was the most common involving 30 eyes, followed by inferotemporal BRVO (IT BRVO) with 19 eyes, and 3 eyes had inferonasal BRVO (IN BRVO). An example of ST BRVO is shown in Figure 2 and 3 shows an example of CRVO. Other details are shown in Table 4. In 21 cases, the type of BRVO was not recorded.
 |
Table 4 Types and Sub-Types of Retinal Vein Occlusion |
 |
Figure 2 Superotemporal branch retinal vein occlusion with macular oedema in right eye. Left) Coloured Fundus photograph, Right) Corresponding Optical Coherence Tomography image showing macular oedema. |
 |
Figure 3 Central Retinal Vein Occlusion with macular oedema in left eye. Top row) Coloured fundus photograph and corresponding Optical Coherence Tomography image showing macular oedema. Bottom row) Red-free fundus photograph showing retinal haemorrhages more prominently. |
Bilaterality of RVO
There were 12 cases of RVO occurring bilaterally: 6 of them had BRVO in both eyes, 3 of them had CRVO in one eye and BRVO in the other, 2 of them had CRVO in both eyes and one patient had HCRVO in one eye and BRVO in the other eye. In 10 of these patients HT was the associated systemic disease, while 2 of them did not have associated systemic disease.
Ocular Co-Morbidities and Sequelae
Hypertensive retinopathy was found in 28 patients in the affected eyes, followed by age-related macular degeneration in 5 patients, non-proliferative diabetic retinopathy in 3 patients, and one patient each was found with optic atrophy, retinal vasculitis, and vitreous degeneration. Other 102 patients did not have any associated ocular co-morbidity.
As sequelae to RVO, vitreous haemorrhage in the affected eyes was seen in 14 patients: 9 associated with BRVO and 5 with CRVO. Neovascular glaucoma was seen in 5 cases: 4 associated with CRVO and one case with HCRVO. Shunt vessels were seen in 4 cases: 3 associated with CRVO and one with BRVO. NVD was diagnosed in 3 cases and NVE was seen in 11 cases.
Management of RVO
General Management
Health education was an integral part of the management of RVO. The patients were advised to consult their general or medical internist physician for controlling hypertension, DM, dyslipidaemia, and other associated systemic diseases. Living a healthy lifestyle with dietary modification, avoiding alcohol consumption and tobacco use, and maintaining physical activities were advised. Finally, the importance of medical adherence and proper follow-up was highlighted.
Retinal Laser Therapy
During the study period 91 patients of RVO received retinal laser therapy (RLT).11 This account might not be a one RLT session per study patient here. The CRVO patients might have at least 2 RLT sessions. RVO was the second most common indication for RLT in Bhutan, only next to the DR.
Anti-VEGF Injection
Intravitreal anti-VEGF injection was received by 132 patients of RVO over the study period.12 RVO was the second most common indication for anti-VEGF injection in Bhutan, only next to the neovascular AMD.
Vitreoretinal Surgery
During the study period, 32 cases of vitreous haemorrhage received pars-plana vitrectomy (PPV), and 11 cases received PPV with epiretinal membrane peeling.14 At least some of these patients must have been the cases of RVO.
Discussion
Demographically, 23.4% of the affected patients were employees or from the working group and relatively younger mean age of presentation. Bhutan is largely an agriculture-based country – agriculture, livestock and forest sectors provide livelihood for about 57% of the total population.18 Farmers and housewives were the major groups affected in the study by RVO, which is concerning for a country with a small population and a handful of workforces. Higher male presentation in the study needs further exploration with a population-based study to find out if the RVO is truly more prevalent among males, or females are not coming forward for medical consultation and treatment despite having the disease. Similar higher male representation was reported by other studies on VR diseases in Bhutan.10,11,13–17 Studies conducted in the region of Indian subcontinent on retinal diseases also report male predominance in Bangladesh,19 India,20 Nepal,9,21 and Pakistan,22 except Sri Lanka, where the female preponderance is reported.23,24
Incidental findings of RVO during routine eye check-up and evaluating for unsatisfactory cataract surgery were common. This may be an indication of poor knowledge of the public on diseases and strongly suggests the need for community screening programs and health advocacy to diagnose VR diseases early and prevent complications.
The current study, as well as previous studies, have shown a high prevalence of non-communicable diseases such as diabetes, hypertension, and their co-existence.10,17 This is attributed to unhealthy Bhutanese diets high in salt and oil, alcohol consumption, and tobacco use.25
The current prevalence of RVO among patients presenting to the VR clinics in Bhutan at 4.8% is marginally lower than that reported by a similar study in Nepal reported at 5.4%.9 Similarly, in India the RVO prevalence was reported at 3.4%, 67.6% of them being BRVO.26 The prevalence reported among the general population worldwide is at 0.77%.27 The Beaver Dam Eye Study reported the 5-year incidence and prevalence of RVO at 0.6%, prevalence of CRVO at 0.1%.7 Bhaktapur Retina Study, a population-based study conducted in Nepal reported an overall population prevalence of RVO at 2.95%, BRVO at 2.74%, and CRVO at 0.21%.8 Similarly, a population-based Central India Eye and Medical Study reported that the prevalence of overall RVO at 0.76%, BRVO at 0.66%, and CRVO at 0.11%.28 Bhutan is yet to conduct a population-based study to quantify the prevalence of RVO among the general population. The current data will serve as a baseline for the more aligned future and population-based studies which are very much needed to know the actual prevalence of RVO among the Bhutanese population.
The pathology of BRVO is different from CRVO by being a mechanical obstruction – in 99% the BRVO occurs at the arterio-venous crossings and the arterioles were located anterior to the vein at the obstruction sites.29 Among the BRVO cases, ST BRVO was the most common type. This higher subtype of BRVO is explained by its mechanical origin because ST retinal vessels travel the furthest and have more arterio-venous crossings.7,29 This is also supported by the topographical distributions of temporal retinal vessels as risk factors to the BRVO - the distribution of superior and inferior temporal retinal arteries were closer to the foveal centre being at the highest risk of developing BRVO.30
We found that HT was associated in 10 of the 12 cases of bilateral RVO. There are studies reporting HT as a known risk factor for RVO.31,32 This may explain why most bilateral cases of RVO in our study had significant association with HT. Grading of hypertensive retinopathy have been already reported in an earlier publication.10 Therefore, it was not described in detail here.
The complications and sequelae of RVO are sight-threatening. The most common complications of RVO described are macular oedema, retinal vascular sheathing, retinal neovascularisation, vitreous haemorrhage, and retinal detachment.33 In our study, vitreous haemorrhage was the most common, seen both in BRVO and CRVO cases. The neovascular glaucoma was seen only with the CRVO and HCRVO, and the shunt vessels more common with CRVO than BRVO. Although the IOP was higher in CRVO compared to BRVO, it was not significantly higher. Raised IOP and therefore the development of neovascular glaucoma is closely associated with the degree of ocular non-perfusion.34 In our study, the weak association perhaps arose because we did not categorise the CRVO into ischaemin or non-ischaemic types. Our finding of lower IOP in HCRVO may just be spurious findings. Numerous factors such as VEGF and cytokines are produced proportional to the area of the retinal ischaemia causing macular oedema and neovascularisation and further complications.35
The mainstays in the management are directed at the consequences of the pathophysiology rather than re-establishing normal venous circulation. Other two treatments are the steroids and the anti-VEGF.36 In the current study, retinal laser therapy was delivered for resorption of retinal swelling and bleeds,11 rather than for creating chorioretinal anastomoses.37 Anti-VEGF injections were administered,12 and VR surgeries were performed to relieve complications of RVO such as vitreous haemorrhage, fibrovascular bands, tractional retinal detachment, and epiretinal membranes.14 There was a high percentage of RVO patients receiving RLT in the study because this study was conducted right after the establishment of VR unit and RLT facility in Bhutan. There were several RVO patients waiting for the RLT in the country. They were referred ex-country to India or Nepal for treatment but refused to go due to language barrier.
Co-existing diabetes and hypertension, and even hypercholesterolemia, are common in Bhutan.38 All these are attributed risk factors for RVO.39 Therefore, Bhutan needs to take strong step in controlling and treating non-communicable diseases such as diabetes, hypertension, dyslipidaemia and obesity. There should be restrictions on the alcohol consumption, salt intake, and tobacco use because studies have unhealthy diets among the Bhutanese population.25
Overall, the first national survey on VR disease reported that 51.9% of participants did not attend modern education, and a majority of them presented only after 15 days of symptom onset.10 This is also supported by the fact that half of AMD cases were in late stage and one-third of neovascular AMD had disciform scars,15 high prevalence of diabetic macular oedema and proliferative diabetic retinopathy,17 total optic atrophy from several causes,16 in their first presentation. Thus, effective community screening, flawless referral systems and health education to public are keys to successful patient management in Bhutan as the public has poor knowledge of diseases, treatment options and prognosis and late presentation is so common. Currently, there is a practice of mobile eye clinics and surgical camps in the district hospitals and peripheral health centres. These activities are mainly focused on anterior segment eye diseases such as refractive errors, cataract, and pterygium. Patients with incidentally diagnosed VR disorders are referred to higher centres, but many of them do not report or are lost to follow-ups and return later with blinding complications. To avoid such incidents, there is need for strengthening screening programs for VR diseases like RVO, and to improve referral systems and patient transportation, ensuring the referred patients report to the higher centre and get proper and timely management. For economic reasons, such screening and referral programs for VR disorders can be clubbed with the existing mobile eye clinics and surgical camps, and with the diabetes and hypertension clinics. Thus, the people who have high risk of getting RVO, such as patients living with diabetes and hypertension, identified as high-risk populations, can be assessed easily. Such targeted screening programs will help make early diagnosis, timely management and prevent complications.
The study has some limitations. This study included only those patients presenting to the VR clinics. The study was a retrospective cross-sectional type. Therefore, it does not have data on the follow-up and treatment outcomes of the included patients. The RVO cases were classified morphologically only, so ischaemic or non-ischaemic types are not discussed, which would be more useful for the management point. Although the FFAs were performed the findings were not recorded on the clinical registers. In the follow-up study, we will address all these limitations.
Conclusions
In Bhutan, 8.5% of RVO patients presented with bilateral. HT was associated significantly as the risk factor for RVO. Incidental findings of RVO during routine eye check-up and evaluation for unsatisfactory cataract surgery was common. Risk factors for RVO such as diabetes, HT and dyslipidaemia are prevalent among the Bhutanese population.10 Therefore, Bhutan needs to control noncommunicable diseases such as diabetes and HT to reduce RVO, and RVO-related blindness and other complications. Currently, regular VR service is provided only at the national referral hospital, which needs to be extended to ERRH and CRRH for regionally balanced VR services.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethical Approval, Informed Consent and Consent for Publication
The study was approved by the Research Ethics Board of Health (REBH) (REBH/Approval/2016/083), Ministry of Health, Royal Government of Bhutan, and was conducted as per the REBH guidelines and tenets of the Declaration of Helsinki. The informed consent and the consent for publication were waived by REBH as the retrospective study collected only the de-identified data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the John Curtin School of Medical Research at the Australian National University under grant number 669/2014.
Disclosure
Author BBR declares that he has received a PhD scholarship from the Australian National University for the current study. Author PD declares that he has no conflict of interest. Author TM declares that he has no conflict of interest.
References
1. Yau JW, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
2. Ip M, Hendrick A. Retinal vein occlusion review. Asia Pac J Ophthalmol. 2018;7(1):40–45. doi:10.22608/APO.2017442
3. Group TEDC-cS. Risk factors for branch retinal vein occlusion. The eye disease case-control study Group. Am J Ophthalmol. 1993;116(3):286–296. doi:10.1016/S0002-9394(14)71345-5
4. Blair K, Czyz CN. Central Retinal Vein Occlusion. StatPearls; 2022.
5. Chopdar A. Hemi-central retinal vein occlusion. Pathogenesis, clinical features, natural history and incidence of dual trunk central retinal vein. Trans Ophthalmol Soc UK. 1982;102(pt 2):241–248.
6. David R, Zangwill L, Badarna M, Yassur Y. Epidemiology of retinal vein occlusion and its association with glaucoma and increased intraocular pressure. Ophthalmologica. 1988;197(2):69–74. doi:10.1159/000309923
7. Klein R, Klein BE, Moss SE, Meuer SM. The epidemiology of retinal vein occlusion: the Beaver dam eye study. Trans Am Ophthalmol Soc. 2000;98:133–141.
8. Thapa R, Bajimaya S, Paudyal G, et al. Prevalence, pattern and risk factors of retinal vein occlusion in an elderly population in Nepal: the Bhaktapur retina study. BMC Ophthalmol. 2017;17(1):162. doi:10.1186/s12886-017-0552-x
9. Rai BB, Shresthra MK, Thapa R, Essex RW, Paudyal G, Maddess T. Pattern and presentation of vitreo-retinal diseases: an analysis of retrospective data at a tertiary eye care centre in Nepal. Asia-Pac J Ophthalmol. 2019;8(6):481–488. doi:10.1097/01.APO.0000604400.50700.2d
10. Rai BB, Morley MG, Bernstein PS, Maddess T. Pattern of vitreo-retinal diseases at the national referral hospital in Bhutan: a retrospective, hospital-based study. BMC Ophthalmology. 2020;20(1). doi:10.1186/s12886-020-01335-x
11. Rai BB, Morley MG, Zangmo P, et al. Retinal laser services in Bhutan: a 3-year national survey. BMC Ophthalmol. 2020;20(1):404. doi:10.1186/s12886-020-01675-8
12. Rai BB, Rai D, Maddess T. Profile of patients treated with intravitreal anti-vascular endothelial growth factor injections in Bhutan. Clin Ophthalmol. 2023;17:1565–1573. doi:10.2147/opth.s414621
13. Rai BB, Ashby RS, French AN, Maddess T. Rural-urban differences in myopia prevalence among myopes presenting to Bhutanese retinal clinical services: a 3-year national study. Graefes Arch Clin Exp Ophthalmol. 2021;259(3):613–621. doi:10.1007/s00417-020-04891-6
14. Rai BB, Morley MG, Zangmo P, et al. Surgical management of vitreo-retinal diseases in Bhutan: a 3-year national study. New Front Ophthalmol. 2020;6:1–6. doi:10.15761/NFO.1000251
15. Rai BB, Morley MG, Bernstein PS, Maddess T. Severity of age-related macular degeneration at first presentation in Bhutan: a 3-year national study. BMC Ophthalmology. 2022;22(1). doi:10.1186/s12886-022-02520-w
16. Rai BB, Sarac O, van Kleef JP, Maddess T. Incidence and pattern of neuro-ophthalmological disorders presenting to vitreoretinal clinics in Bhutan: a 3-year national study. Clin Ophthalmol. 2023;17:107–114. doi:10.2147/OPTH.S396879
17. Rai BB, Essex RW, Morley MG, Bernstein PS, van Kleef JP, Maddess T. Prevalence and severity of diabetic retinopathy at first presentation to vitreoretinal services in Bhutan: a 3-year national study. J Ophthalmology. 2023;2023:1.
18. CIAT, WorldBank. Climate-Smart Agriculture in Bhutan. CSA Country Profiles for Asia Accessed 2019 January. Available from: http://sdwebx.worldbank.org/climateportal/doc/agricultureProfiles/CSA-in-Bhutan.pdf.
19. Ahmed KR, Karim MN, Bhowmik B, et al. Incidence of diabetic retinopathy in Bangladesh: a 15-year follow-up study. J Diabetes. 2012;4(4):386–391. doi:10.1111/j.1753-0407.2012.00208.x
20. Singh HV, Das S, Deka DC, Kalita IR. Prevalence of diabetic retinopathy in self-reported diabetics among various ethnic groups and associated risk factors in North-East India: a hospital-based study. Indian J Ophthalmol. 2021;69(11):3132–3137. doi:10.4103/ijo.IJO_1144_21
21. Thapa R, Bajimaya S, Sharma S, Rai BB, Paudyal G. Systemic association of newly diagnosed proliferative diabetic retinopathy among type 2 diabetes patients presented at a tertiary eye hospital of Nepal. Nepal J Ophthalmol. 2015;7(1):26–32. doi:10.3126/nepjoph.v7i1.13163
22. Jokhio AH, Talpur KI, Shujaat S, Talpur BR, Memon S. Prevalence of diabetic retinopathy in rural Pakistan: a population based cross-sectional study. Indian J Ophthalmol. 2022;70(12):4364–4369. doi:10.4103/ijo.IJO_126_22
23. Katulanda P, Waniganayake YC, Ranasinghe P, et al. Retinopathy among young adults with Diabetes Mellitus from a tertiary care setting in Sri Lanka. BMC Endocr Disord. 2014;14:20. doi:10.1186/1472-6823-14-20
24. Katulanda P, Ranasinghe P, Jayawardena R. Prevalence of retinopathy among adults with self-reported diabetes mellitus: the Sri Lanka diabetes and Cardiovascular Study. BMC Ophthalmol. 2014;14:100. doi:10.1186/1471-2415-14-100
25. Pelzom D, Isaakidis P, Oo MM, Gurung MS, Yangchen P. Alarming prevalence and clustering of modifiable noncommunicable disease risk factors among adults in Bhutan: a nationwide cross-sectional community survey. Bmc Public Health. 2017;17. doi:10.1186/s12889-017-4989-x
26. Bhattacharjee H, Barman M, Misra D, et al. Spectrum of Eye Disease in Diabetes (SPEED) in India: a prospective facility-based study. Report # 3. Retinal vascular occlusion in patients with type 2 diabetes mellitus. Indian J Ophthalmol. 2020;68(Suppl 1):S27–S31. doi:10.4103/ijo.IJO_1934_19
27. Song P, Xu Y, Zha M, Zhang Y, Rudan I. Global epidemiology of retinal vein occlusion: a systematic review and meta-analysis of prevalence, incidence, and risk factors. J Glob Health. 2019;9(1):010427. doi:10.7189/jogh.09.010427
28. Jonas JB, Nangia V, Khare A, Sinha A, Lambat S. Prevalence and associations of retinal vein occlusions: the Central India eye and medical study. Retina. 2013;33(1):152–159. doi:10.1097/IAE.0b013e318260246f
29. Zhao J, Sastry SM, Sperduto RD, Chew EY, Remaley NA. Arteriovenous crossing patterns in branch retinal vein occlusion. The eye disease case-control study group. Ophthalmology. 1993;100(3):423–428. doi:10.1016/s0161-6420(93)31633-7
30. Oztas Z, Akkin C, Nalcaci S, Ilim O, Afrashi F. Branch retinal vein occlusion: the importance of the topographical distribution of retinal vessels among risk factors. Eye. 2017;31(5):726–731. doi:10.1038/eye.2016.318
31. Kondo M, Noma H, Shimura M, et al. Background factors affecting visual acuity at initial visit in eyes with central retinal vein occlusion: multicenter study in Japan. J Clin Med. 2021;10(23). doi:10.3390/jcm10235619
32. Ponto KA, Scharrer I, Binder H, et al. Hypertension and multiple cardiovascular risk factors increase the risk for retinal vein occlusions: results from the Gutenberg Retinal Vein Occlusion Study. J Hyperten. 2019;37(7):1372–1383. doi:10.1097/Hjh.0000000000002057
33. Jaulim A, Ahmed B, Khanam T, Chatziralli IP. Branch retinal vein occlusion: epidemiology, pathogenesis, risk factors, clinical features, diagnosis, and complications. An update of the literature. Retina. 2013;33(5):901–910. doi:10.1097/IAE.0b013e3182870c15
34. Chan CK, Ip MS, Vanveldhuisen PC, et al. SCORE Study report #11: incidences of neovascular events in eyes with retinal vein occlusion. Ophthalmology. 2011;118(7):1364–1372. doi:10.1016/j.ophtha.2010.11.020
35. Rehak M, Storch MW, Hattenbach LO, Feltgen N. [Ischemia and laser photocoagulation in retinal vein occlusion]. Ischamie und Lasertherapie bei retinalen venosen Verschlussen. Ophthalmologie. 2022;119(11):1121–1128. doi:10.1007/s00347-022-01750-z
36. Schmidt-Erfurth U, Garcia-Arumi J, Gerendas BS, et al. Guidelines for the management of retinal vein occlusion by the European society of retina specialists (EURETINA). Ophthalmologica. 2019;242(3):123–162. doi:10.1159/000502041
37. McAllister IL, Gillies ME, Smithies LA, et al. The central retinal vein bypass study: a trial of laser-induced chorioretinal venous anastomosis for central retinal vein occlusion. Ophthalmology. 2010;117(5):954–965. doi:10.1016/j.ophtha.2009.10.026
38. Giri BR, Sharma KP, Chapagai RN, Palzom D. Diabetes and hypertension in urban Bhutanese men and women. Indian J Community Med. 2013;38(3):138–143. doi:10.4103/0970-0218.116349
39. Kolar P. Risk factors for central and branch retinal vein occlusion: a meta-analysis of published clinical data. J Ophthalmol. 2014;2014:724780. doi:10.1155/2014/724780
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.