")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Perceived Credibility of Public Health Campaigns and Its Impact on Infection Control Behaviors: Mediating Roles of Health Literacy and Motivation
Authors Alotaibi KA
Received 2 February 2025
Accepted for publication 28 May 2025
Published 3 June 2025 Volume 2025:18 Pages 3153—3163
DOI https://doi.org/10.2147/JMDH.S520357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Khalid Abdullah Alotaibi
College of Education, Department of Psychology, Prince Sattam bin Abdulaziz University, Al-Kharj, 11942, Saudi Arabia
Correspondence: Khalid Abdullah Alotaibi, College of Education, Department of Psychology, Prince Sattam bin Abdulaziz University, Al-Kharj, 11942, Saudi Arabia, Email [email protected]
Background: Public health campaigns are vital in promoting infection control behaviors, particularly during health crises. The effectiveness of such campaigns can be influenced by various factors, including the perceived credibility of the messages, health literacy, and motivation to adopt health behaviors. Understanding the relationships between these factors is crucial for enhancing the impact of health campaigns. This study aimed to examine the effect of the perceived credibility of public health campaigns on infection control behaviors, with health literacy and motivation serving as mediators in Riyadh, Saudi Arabia.
Methods: A cross-sectional survey was conducted between November and December 2024 with 393 participants in Riyadh. Structural equation modeling (SEM) and path analysis were used to assess perceived credibility’s direct and indirect effects on infection control behaviors through health literacy and motivation while controlling for age, gender, and education.
Results: The results showed that perceived credibility had a significant direct effect on adherence to preventive behaviors (β = 0.44, p < 0.001) and motivation significantly mediated this relationship (indirect effect: β = 0.08, p < 0.01). However, no significant indirect effect was found through health literacy (indirect effect: β = 0.006, p > 0.05).
Conclusion: This study emphasizes the critical roles of perceived credibility and motivation in driving infection control behaviors. The findings suggested that public health campaigns should focus on enhancing the credibility of health messages and fostering motivation to improve adherence to preventive measures. These insights have practical implications for designing more effective public health strategies in regions like Riyadh, Saudi Arabia.
Keywords: perceived credibility, health literacy, motivations, adherence to preventive behaviors, public health campaigns, Riyadh
Introduction
Public health campaigns play a vital role in shaping public behavior,1 particularly in infection control, which has become increasingly critical during health crises such as the COVID-19 pandemic.2 In Saudi Arabia, as in many regions, public health interventions are central to promoting mask-wearing, physical distancing, and proper hygiene practices.3 However, the success of these campaigns depends not only on the clarity of the messages but also on various psychological and cognitive factors,4 including the perceived credibility of the messages,5 health literacy,6 and motivation to adopt health behaviors.7 Understanding the relationships among these variables can help refine public health strategies to enhance adherence to infection control measures and improve overall health outcomes.
Perceived credibility refers to the degree to which individuals trust and believe in the information provided by public health campaigns.8 It has been consistently shown that when people perceive health messages as credible, they are more likely to engage in the recommended behaviors.9 Researchers emphasized that the perceived credibility of health messages influences individuals’ likelihood of acting on those messages.5,10 Odunsi and Farris 2023,11 found that source credibility significantly predicted college students’ compliance with COVID-19 preventive behaviors, particularly when coupled with health literacy and perceived threat levels. Similarly, Niu et al 2022,12 demonstrated that trust in media sources and message credibility were strong predictors of adherence to infection control practices among high-risk individuals in China. In regions like Riyadh, where trust in health authorities and communication channels varies,13–16 perceived credibility is crucial in shaping the effectiveness of public health messages. Ensuring that public health campaigns are perceived as credible can lead to increased engagement and adherence to preventive health measures, thus making this factor an important focal point for health communication strategies. Given this evidence, the present study hypothesizes that perceived credibility may have a direct positive effect on individuals’ adherence to infection control behaviors among Saudi participants (H1).
Health literacy is another essential factor in adopting health behaviors.17 It refers to an individual’s ability to understand, interpret, and apply health information to promote well-being.18 Health literacy has been linked to improved health outcomes19 and adherence to health recommendations.20,21 However, the relationship between health literacy and adherence to infection control behaviors is complex. Studies have suggested that while individuals with higher health literacy are generally more likely to follow health recommendations,22 other factors, such as motivation23 and social influences,24 may play a more significant role in shaping behavior,25 especially in the context of preventive health measures. The influence of health literacy on behavior might also depend on the context in which it is assessed, suggesting that additional factors such as health beliefs and external motivators must be considered when studying its effects.26 Recent research by Hassanien et al 2022,27 found that electronic health literacy mediated the relationship between pandemic fatigue and adherence to COVID-19 preventive behaviors, highlighting its role in helping individuals assess and respond to public health messages. Similarly, Zhao et al 2022,28 demonstrated that health literacy significantly influenced individuals’ engagement with health information, which in turn promoted preventive practices, underscoring its mediating role in behavioral adoption. Building on this evidence, the present study proposes that health literacy may serve as a mediator between the perceived credibility of public health messages and individuals’ adherence to infection control behaviors among Saudi participants (H2).
Motivation is a key psychological driver of health behavior change.29 It refers to the willingness to engage in health-promoting behaviors, which various intrinsic and extrinsic factors can influence.30 Motivation to adopt health behaviors has been found to strongly predict the likelihood of behavior change, particularly when individuals feel that the behaviors align with their values and health goals.31 For instance, intrinsic motivation, driven by personal satisfaction and well-being, has led to sustained behavior change.32 Motivation is particularly relevant in infection control behaviors, where individuals may need to continuously adopt and maintain practices like physical distancing and hand hygiene.33 Public health campaigns that foster motivation—by emphasizing personal benefits or communal well-being—can enhance the likelihood of adherence to infection control measures. Recent studies further highlight the mediating role of motivation in public health behavior change. For example, Martela et al 2021,34 demonstrated that autonomous motivation significantly mediated the impact of health messaging on behavioral compliance during COVID-19, supporting a self-determination framework for message effectiveness. Similarly, Oyibo 2021,35 found that motivational beliefs mediated the relationship between perceived message effectiveness and behavioral intentions in digital health campaigns. Based on this evidence, the current study hypothesizes that motivation mediates the relationship between perceived credibility of public health campaigns and adherence to preventive behaviors among Saudi participants (H3).
This study contributes significantly to the existing literature by examining the combined effects of perceived credibility, health literacy, and motivation on adherence to infection control behaviors, particularly within Riyadh, Saudi Arabia. While prior research has often focused on these variables in isolation, this study explores how they interact, providing a deeper understanding of the mechanisms that drive health behavior change. This study aims to investigate the direct effect of the perceived credibility of public health awareness on adherence to preventive behaviors and the mediating roles of motivation to adopt health behaviors and health literacy in this relationship. Focusing on the mediating roles of health literacy and motivation, this research offers new insights into how public health messages’ perceived credibility influences individuals’ motivation to adopt health behaviors and their ability to act on them. This study highlights that motivation is crucial in directly predicting adherence to preventive behaviors and mediating the influence of perceived credibility. Additionally, it challenges the traditional view that health literacy alone directly impacts behavior change, suggesting its effect may be more context-dependent. By integrating these variables, the study provides a more comprehensive model for understanding adherence to infection control behaviors, offering practical implications for designing public health campaigns that are credible, motivational, and tailored to diverse literacy levels. The findings encourage future research to explore these dynamics further and emphasize the importance of creating health messages that are not only informative but also engaging and motivating for the public. This research contributes innovative perspectives for improving public health strategies, particularly in the Saudi context, and can be applied to similar cultural settings globally.
Methodology
Research Design and Study Participants
This study employed a quantitative cross-sectional design to examine the relationships between the perceived credibility of public health awareness campaigns and citizens’ adherence to infection control behaviors in Riyadh, Saudi Arabia, with the mediating roles of health literacy and motivation in these relationships. Four hundred twenty-three participants were initially recruited from Riyadh using stratified random sampling. This approach ensured that different subgroups within the population, such as age, gender, and exposure to public health campaigns, were adequately represented. The inclusion criteria required participants to be 18 years or older and residents of Riyadh who had been exposed to at least one public health awareness campaign. After screening for missing data, 393 valid responses were retained for analysis. A total of 30 cases were excluded due to missing data exceeding the 5% threshold. The potential for non-response bias was examined by comparing the demographic characteristics of excluded versus retained participants. No statistically significant differences were found in age, gender, or education level between the two groups (all p-values > 0.10), suggesting that non-response bias is unlikely to have affected the representativeness of the final sample (Supplementary File: Table S1).
Although a power analysis for a multiple regression model with six predictors and a medium effect size (f² = 0.15) indicates that a minimum sample of 98 would be sufficient (power = 0.80, α = 0.05), structural equation modeling (SEM) requires larger samples due to model complexity and the estimation of multiple fit indices. In line with best practices, a sample size of 300–500 is considered adequate for SEM involving latent variables and mediation. Our final sample of 393, therefore, meets these recommended criteria and ensures robust model estimation.36,37 Additionally, the stratified sampling approach ensures that the sample is representative of Riyadh’s demographic population, enhancing the generalizability of the findings. With a sufficiently powered sample, the study can detect meaningful relationships between the variables and provide reliable insights into the mediating roles of health literacy and motivation. The final sample (n = 393) had a mean age of 34.4 years (SD = 4.8; range = 18–65), with 52.4% identifying as female.
Data Collection Procedure
Data collection was conducted in December 2024 using self-administered paper-based questionnaires delivered in person by trained enumerators. This method enabled real-time support if participants required clarification while preserving the integrity of self-reporting. Enumerators provided standardized instructions and remained available to assist if needed but did not influence participants’ responses. Surveys were completed by respondents in semi-private areas of public spaces and community centers across Riyadh, helping to ensure participation from a broad demographic cross-section.
Questionnaire Translation and Pilot Testing
All measurement instruments used in this study were originally developed in English. The full questionnaire was translated into Arabic by two bilingual experts following best practices in cross-cultural research. The translation emphasized semantic equivalence and cultural appropriateness while retaining the original item structure and meaning. No rewording, substitution, or conceptual modifications were made to the content of any item beyond necessary grammatical adjustments in the translation process. A pilot test was conducted with a sample of 35 Arabic-speaking participants from Riyadh to evaluate the clarity, linguistic accuracy, and comprehension of all items. Feedback from the pilot confirmed that the translated questionnaire was clearly understood and required no further modification. This step ensured that all items retained their intended meaning and were culturally accessible to the study population. The questionnaire is presented in the Supplementary File: Questionnaire items).
Ethical Considerations
The research was conducted in accordance with the ethical guidelines of the Declaration of Helsinki. Prior to data collection, approval was obtained from the Institutional Review Board (IRB) of the Prince Sattam bin Abdul Aziz University (SCBR-395/2024). All participants provided informed consent prior to completing the questionnaire. Participation was voluntary, and confidentiality was maintained throughout the study.
Measures
Demographic Variables
Participants were asked to provide basic demographic information, including age, gender, education level, marital status, employment status, residential region, household income, and self-reported health status.
Perceived Credibility of Public Health Awareness Campaigns
Perceived credibility was measured using a 10-item version of the original 15-item Source Credibility Scale developed by Ohanian 1990,38 The original instrument assesses three dimensions of source credibility: expertise, trustworthiness, and attractiveness, with five items per dimension. For this study, the attractiveness dimension and its associated five items were removed, as it was not conceptually relevant to evaluating the credibility of public health campaigns rather than individual endorsers. Additionally, slight modifications to the wording of certain items were made to better align with the study’s focus on public health campaigns and infection control behaviors. These modifications were aimed at ensuring clarity and relevance to the target population while retaining the original conceptual structure. The adapted scale, therefore, included 5 items for expertise and 5 items for trustworthiness. Participants responded to each item using a 5-point Likert scale (1 = Strongly Disagree to 5 = Strongly Agree). A composite credibility score was calculated as the mean of all 10 items, with higher scores indicating greater perceived credibility of the public health messages. The scale was translated into Arabic and pilot-tested for clarity and cultural relevance.
Health Literacy
Health literacy was assessed using a 16-item short-form version of the European Health Literacy Survey Questionnaire (HLS-EU-Q16).39 This validated instrument measures individuals’ perceived ease or difficulty in accessing, understanding, appraising, and applying health-related information across the domains of health care, disease prevention, and health promotion. Slight modifications to the wording of certain items were made to better align with the study’s focus on public health campaigns and infection control behaviors. These modifications ensured clarity and relevance for the target population while maintaining the original conceptual structure of the scale. Participants responded using a 4-point scale ranging from “Very difficult” to “Very easy”. The health literacy score was calculated as the mean of all items, with higher scores indicating greater health literacy. HLS-EU proficiency categories (eg, inadequate, problematic, sufficient, excellent) were not applied in this study.
Motivation to Adopt Health Behaviors
Motivation to adopt infection control behaviors was assessed using a 10-item scale adapted from the Theory of Planned Behavior (TPB).40 The items were tailored to reflect key preventive health actions promoted during the COVID-19 pandemic, including mask-wearing, hand hygiene, physical distancing, and participation in health campaigns. Statements covered personal motivation, perceived value, behavioral intention, and a sense of social responsibility (eg, “I feel personally responsible for helping prevent the spread of infection through my behavior”). Responses were collected using a 5-point Likert scale ranging from Strongly Disagree (1) to Strongly Agree (5). A composite motivation score was computed by taking the mean of all 10 items, with higher scores indicating greater motivation to adopt and maintain infection control behaviors. Slight modifications to the wording of certain items were made to better align with the study’s focus on infection control behaviors and the context of public health campaigns. These modifications ensured that the items were clear, relevant, and applicable to the target population while maintaining the integrity of the original TPB constructs.
Adherence to Preventive Behaviors
Adherence was measured using an 8-item scale adapted from the behavioral guidelines of the World Health Organization (WHO)41 and the Centers for Disease Control and Prevention (CDC) for infection control during pandemics such as COVID-19.42 The selected items were chosen based on their practical relevance to the study context and reflected widely recommended preventive practices, including hand hygiene, mask-wearing, social distancing, and avoiding large gatherings. Participants were asked to indicate how frequently they had engaged in each behavior over the past month using a 5-point Likert scale (1 = Never to 5 = Always). A composite adherence score was calculated as the mean of all eight items, with higher scores reflecting greater adherence to recommended infection control behaviors.
Analytical Approach
Confirmatory factor analysis (CFA) and model fitting were conducted using AMOS 24.0 to assess the validity and reliability of this study’s structural models and measurement scales. Descriptive statistics and correlation analyses were performed with SPSS 26.0. To estimate the mediating effects, 95% confidence intervals were calculated using a bias-corrected percentile bootstrap method with 5000 resamples.
Results
To assess the potential impact of Common Method Variance (CMV), Harman’s single-factor test was conducted. All measurement items were entered into an unrotated exploratory factor analysis using principal axis factoring. The results revealed that the first factor accounted for 31.4% of the total variance, which is well below the 40% threshold commonly used to indicate problematic CMV.43 This suggests that CMV is unlikely to be a significant concern in this dataset.
The reliability and validity analyses demonstrated strong internal consistency across all measures (Table 1), with Cronbach’s alpha (α) values ranging from 0.82 to 0.89, indicating good reliability for each construct. The composite reliability (CR) values ranged from 0.83 to 0.88, confirming the constructs’ reliability. The average variance extracted (AVE) values were generally acceptable, ranging from 0.58 to 0.67, supporting the measures’ convergent validity.
 |
Table 1 Reliability, Validity, and Model Fit Analyses |
Multicollinearity was assessed using variance inflation factors (VIF), which ranged from 1.12 to 2.01, suggesting no significant multicollinearity concerns. Model fit indices indicated that the model had a good fit, with RMSEA values between 0.041 and 0.052, SRMR values between 0.039 and 0.055, and CFI values ranging from 0.95 to 0.96, all of which fell within acceptable thresholds. TLI ranged from 0.93 to 0.95, also supporting the adequacy of the model fit.
The results of bivariate correlation among the study variables are presented in Table 2. Perceived credibility of public health awareness campaigns was positively correlated with motivation to adopt health behaviors (r = 0.40, p < 0.001) and adherence to preventive behaviors (r = 0.52, p < 0.001). Health literacy showed a small but significant negative correlation with adherence to preventive behaviors (r = −0.13, p < 0.05), suggesting that higher health literacy might be associated with slightly lower adherence, although the effect was weak. Motivation to adopt health behaviors was positively correlated with adherence to preventive behaviors (r = 0.29, p < 0.001), indicating that individuals more motivated to adopt health behaviors were more likely to engage in preventive behaviors.
 |
Table 2 Descriptive and Correlational Analysis |
Table 3 demonstrates several key findings for regression analysis. The perceived credibility of public health awareness campaigns significantly influenced both motivations to adopt health behaviors and adherence to preventive behaviors. Specifically, the credibility of public health campaigns had a strong positive effect on adherence (β = 0.442, p < 0.001) and motivation (β = 0.352, p < 0.001). Age was a significant predictor for all three dependent variables: health literacy (β = 0.005, p < 0.05), motivation (β = 0.008, p < 0.01), and adherence to preventive behaviors (β = 0.012, p < 0.01). This suggested that older individuals reported higher levels of motivation and adherence and slightly higher health literacy. In contrast, gender and educational level did not significantly affect the outcomes. In addition, motivation to adopt health behaviors significantly mediated this relationship. Perceived credibility positively predicted motivation (β = 0.35, p < 0.001), which in turn predicted adherence (β = 0.22, p < 0.01). The indirect effect of perceived credibility on adherence through motivation was statistically significant (β = 0.08, p < 0.01). This suggested that motivation is a key psychological mechanism through which credible health messages influence behavior. Although perceived credibility was hypothesized to indirectly influence adherence through health literacy, this indirect path was not supported. Perceived credibility did not significantly predict health literacy (β = −0.12, p > 0.05), and health literacy also did not have a significant direct effect on adherence to preventive behaviors (β = −0.05, p > 0.05). As both segments of the pathway were non-significant, there was no evidence of an indirect effect from perceived credibility to adherence via health literacy alone (Figure 1).
 |
Table 3 Regression Results (Controlling for Age, Sex, and Educational Level) |
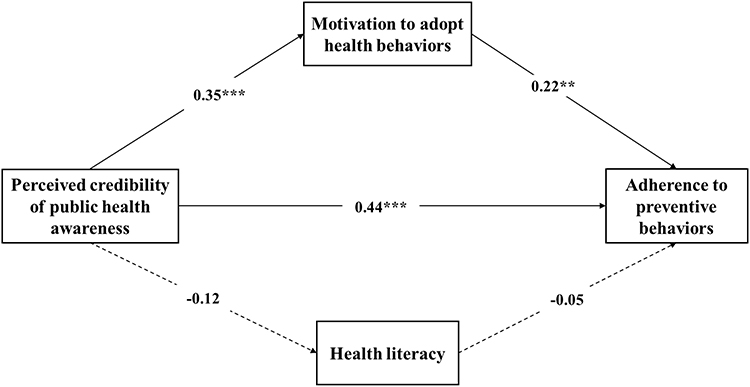 |
Figure 1 Path analysis. Solid lines show significant paths (***p < 0.01, **p<0.01). Dashed lines represent insignificant paths (p ≥ 0.05). |
Discussion
This study explored the relationships between the perceived credibility of public health awareness campaigns, health literacy, motivation to adopt health behaviors, and adherence to preventive behaviors. It is original in its focus on the role of perceived credibility and motivation in influencing adherence, addressing a critical gap in existing research on health behavior promotion. The results indicated that perceived credibility was significantly associated with motivation and adherence to preventive behaviors, with motivation also playing a key role in driving adherence. However, health literacy did not show a significant direct effect on adherence. This study contributes to the literature by highlighting the importance of perceived credibility and motivation in shaping health behaviors, offering insights for improving public health campaign strategies.
The direct effect of the perceived credibility of public health awareness campaigns on adherence to preventive behaviors in this study was found to be significant, supporting the initial study hypothesis (H-I). This finding is consistent with previous research highlighting credibility’s importance in health communication.44–46 Evidence suggests that individuals are more likely to adhere to health recommendations when they perceive the information to be credible,47,48 which aligns with the results of the current study. Additionally, studies by Xu et al 2021,5 and Zhao et al 2021,10 have also reported that perceived credibility influences health behavior compliance by fostering trust in health messages and increasing the likelihood of behavioral change. Our findings also echo recent work by Odunsi and Farris 2023,11 who showed that source credibility significantly predicted COVID-19 preventive behaviors among college students in the US, particularly when coupled with perceived risk and health literacy. Likewise, Niu et al 2022,12 found that the credibility of health information sources strongly influenced compliance among high-risk individuals in China, emphasizing the universal role of message trustworthiness in behavior adoption. The significant relationship observed in this study can be attributed to individuals being more likely to engage in behaviors endorsed by sources they trust, which is crucial in public health campaigns, especially during health crises like the COVID-19 pandemic.49 Furthermore, the alignment with prior studies suggests that the credibility of the source of information plays a central role in motivating individuals to act following recommended preventive measures.50 This finding underscore health campaigns’ need to ensure that their messages are clear and informative and emanate from credible sources to drive behavior change effectively.
Contrary to the second hypothesis (H2), the current study found that health literacy did not exhibit a significant direct effect on adherence to preventive behaviors, nor did it show a significant indirect effect through motivation. This contrasts with prior research suggesting that higher health literacy is associated with better adherence to health recommendations. For instance, Nutbeam 2008,22 and Ferguson et al 2011,19 found that individuals with higher health literacy are more likely to understand and act upon health information, improving health behaviors. However, the lack of significant findings in the present study may be explained by the complex nature of health literacy, which is not solely about the ability to understand health information but also involves factors like individual motivation,51 health beliefs,52 and social contexts.53 Additionally, the current study’s sample may have already had a certain baseline level of health knowledge, diminishing the variation in health literacy needed to detect a stronger effect. In contrast, health literacy did not directly influence adherence or act as a mediator; its potential indirect influence through other factors, such as motivation, warrants further exploration.
Further, motivation to adopt health behaviors demonstrated a significant positive effect on adherence to preventive behaviors, supporting the third hypothesis of this study. This finding aligns with existing research highlighting motivation as a key psychological driver of health behavior change. Studies by Ryan and Deci 2000,31 and Hardcastle et al 2015,54 have shown that motivated individuals are more likely to engage in health-promoting behaviors, particularly those requiring sustained effort, such as adherence to preventive measures. Intrinsic motivation enhances personal commitment to following health guidelines, especially when individuals perceive the behaviors as personally meaningful. In health campaigns, fostering motivation is critical to ensuring both initial compliance and continued adherence.55 Additionally, the indirect effect of perceived credibility on adherence, mediated by motivation, was also significant. This suggested that motivation plays an essential role in translating external influences, such as the perceived credibility of health messages, into actual behavior change. Consistent with prior studies, including Slater and Rouner, 2002,9 this mediation effect emphasizes that credible information alone may not suffice to drive behavior change unless it also motivates individuals to take action. The findings support the notion that health campaigns should focus not only on delivering credible information but also on fostering motivation to ensure sustained behavior change.56–59
Study Implications
The findings of this study contribute significantly to the existing literature on health behavior change, particularly in the context of public health campaigns. The study reinforces the importance of perceived credibility and motivation as critical drivers of adherence to preventive behaviors, aligning with prior research that emphasizes the role of trusted information sources in influencing health behaviors. This is particularly important in global health crises, where effective communication strategies are essential for behavior change. In this study, the direct effect of perceived credibility on both motivation and adherence highlights the essential role that trustworthy, credible messages play in shaping public health behaviors, especially in regions like Riyadh, Saudi Arabia, where health literacy and trust in public health authorities can vary across different population groups.
From a practical perspective, the findings suggest that public health campaigns in Riyadh and similar regions should focus on delivering clear and informative messages and ensuring that these messages come from credible, trusted sources. Health authorities should consider partnerships with reputable organizations, local influencers, and community leaders to enhance the credibility of public health information. Moreover, fostering motivation to adopt health behaviors could improve adherence, especially in regions where cultural and social factors influence individuals’ willingness to take preventive measures. Interventions that address intrinsic motivation, such as framing health behaviors as aligned with personal values or community well-being, could lead to more sustained behavior change.
The implications of these findings extend beyond local health campaigns in Riyadh to global public health challenges, particularly in pandemic management and long-term health behavior interventions. As seen in COVID-19 health campaigns around the world, motivation plays a crucial role in increasing compliance with preventive measures. This study suggests that health communication strategies worldwide should focus on both credibility and motivation to ensure engagement and sustained adherence.
Furthermore, while health literacy was not a significant mediator in this study, it remains an essential component of effective health communication. Improving health literacy in Riyadh—and, by extension, other regions with diverse literacy levels—can support the effective delivery and understanding of public health messages. However, the findings suggest that strategies to increase motivation and enhance the perceived credibility of health messages should accompany efforts to improve health literacy, ensuring higher engagement and compliance with preventive health measures. These insights provide a roadmap for future public health interventions in Riyadh, and more broadly, they emphasize the multifaceted nature of health behavior change. An integrated approach that considers both cognitive and motivational aspects of behavior is essential to achieving lasting behavior change and improving health outcomes on a global scale.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, its cross-sectional design prevents causal inference, limiting conclusions to associations rather than directionality. Future longitudinal studies would help clarify temporal relationships and causal pathways. Second, the data were self-reported, which may introduce social desirability bias and recall inaccuracies, particularly in reporting adherence behaviors. Incorporating objective or behavioral measures in future research could strengthen validity. Third, the sample—though drawn from Riyadh—may not fully represent the broader Saudi population, especially rural or marginalized groups with potentially different health literacy levels or public health perceptions. As a result, generalizability may be limited. Fourth, although Harman’s single-factor test indicated that common method variance (CMV) was not a major concern, reliance on self-reporting still presents the risk of response bias, which could be mitigated in future studies through multi-source or longitudinal data collection. Fifth, the non-significant role of health literacy as a mediator may reflect limitations in how it was measured. Future studies should examine multidimensional health literacy constructs (eg, functional, interactive, critical literacy) to explore their behavioral relevance. Additionally, the study did not include other potential mediators, such as emotional or social factors, which may further illuminate the complexities of health behavior adoption. Finally, external contextual influences (eg, media exposure, public health policies, political climate) were not controlled for, though they may shape behavioral responses to public health campaigns. Including these variables in future research would offer a more comprehensive understanding of what drives adherence in diverse settings.
Conclusion
This study provides preliminary evidence that perceived credibility and motivation may play important roles in influencing adherence to preventive behaviors, particularly in the context of public health campaigns in Riyadh, Saudi Arabia. While motivation emerged as a significant mediator, health literacy did not show a direct or indirect effect in this model, suggesting that its influence may be more complex or context-dependent. Given the study’s cross-sectional design and reliance on self-reported data, these findings should be interpreted with caution. Nonetheless, the results offer practical considerations for developing public health messages that prioritize credibility and strategies that enhance motivation. Future research using longitudinal or experimental designs, and incorporating additional mediators and external contextual factors, is needed to better understand the dynamics of health behavior adoption.
Data Sharing Statement
The raw data supporting this study’s findings are available upon reasonable request from the author.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board (IRB) of Prince Sattam bin Abdul Aziz University (SCBR-395/2024), and all methods were carried out in accordance with the relevant guidelines and regulations of the Declaration of Helsinki. All participants provided informed consent and were assured of confidentiality and anonymity when handling their data. Participation was entirely voluntary, and participants retained the right to withdraw from the study at any stage without any repercussions.
Funding
This study is supported via funding from Prince Sattam bin Abdulaziz University project number (2024/03/31747).
Disclosure
The author reports no conflicts of interest in this work.
References
1. Baqir R. Assessing the effectiveness of public health campaigns: strategies, impacts, and challenges. Law Res J. 2023;1(2):54–63.
2. Al-Dmour H, Masa’deh R, Salman A, Al-Dmour R, Abuhashesh M. The role of mass media interventions on promoting public health knowledge and behavioral social change against COVID-19 Pandemic in Jordan. Sage Open. 2022;12(1):21582440221082124. doi:10.1177/21582440221082125
3. F MA, A MA, M MA, H HA, H HA. Effect of facemask, handwashing, and social distancing on contracting COVID-19 infection in Saudi Arabia: a case-control study. F1000Research. 2023;12:323. doi:10.12688/f1000research.129255.1
4. Renner B, Schwarzer R. Social‐cognitive factors in health behavior change. Soc Psychol Found Heal Illn. 2003;2003:169–196.
5. Xu X, Li H, Shan S. Understanding the health behavior decision-making process with situational theory of problem solving in online health communities: the effects of health beliefs, message credibility, and communication behaviors on health behavioral intention. Int J Environ Res Public Health. 2021;18(9):4488. doi:10.3390/ijerph18094488
6. Jhummon-Mahadnac ND, Knott J, Marshall C. A cross-sectional study of pandemic influenza health literacy and the effect of a public health campaign. BMC Res Notes. 2012;5:1–8. doi:10.1186/1756-0500-5-377
7. Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet. 2010;376(9748):1261–1271. doi:10.1016/S0140-6736(10)60809-4
8. Yoo S-W, Kim J, Lee Y. The effect of health beliefs, media perceptions, and communicative behaviors on health behavioral intention: an integrated health campaign model on social media. Health Commun. 2018;33(1):32–40. doi:10.1080/10410236.2016.1242033
9. Slater MD, Rouner D. Entertainment—education and elaboration likelihood: understanding the processing of narrative persuasion. Commun theory. 2002;12(2):173–191.
10. Zhao Y, Zhang L, Zeng C, Chen Y, Lu W, Song N. Factors influencing online health information credibility: a meta-analysis. Aslib J Inf Manag. 2024. doi:10.1108/AJIM-05-2023-0155
11. Odunsi IA, Farris KL. Predicting college students’ preventative behavior during a pandemic: the role of the health belief model, source credibility, and health literacy. Am Behav Sci. 2023;2023:00027642231164044.
12. Niu Z, Qin Z, Hu P, Wang T. Health beliefs, trust in media sources, health literacy, and preventive behaviors among high-risk Chinese for COVID-19. Health Commun. 2022;37(8):1004–1012. doi:10.1080/10410236.2021.1880684
13. Al-Shehri B, Gormley K, Mccutcheon K, Prue G. Communication and information exchange between Emergency Medical Teams during emergency situations in Riyadh, the Kingdom of Saudi Arabia: an explorative qualitative study. 2022.
14. Almutairi AF, BaniMustafa A, Alessa YM, Almutairi SB, Almaleh Y. Public trust and compliance with the precautionary measures against COVID-19 employed by authorities in Saudi Arabia. Risk Manag Healthc Policy. 2020;Volume 13:753–760. doi:10.2147/RMHP.S257287
15. Alsulaiman SA. Health Crisis in the Kingdom of Saudi Arabia: A Study of Saudis’ Knowledge of Coronavirus, Attitudes Toward the Ministry of Health’s Coronavirus Preventive Campaigns, and Trust in Coronavirus Messages in the Media. Bowling Green State University; 2018.
16. Elnasieh AM, Alturki AT, Alhadlaq R, et al. Health education resources favored by out-patients attending King Saud Medical City, Riyadh. Cureus. 2024;16(8):e67089. doi:10.7759/cureus.67089
17. Fleary SA, Joseph P, Pappagianopoulos JE. Adolescent health literacy and health behaviors: a systematic review. J Adolesc. 2018;62:116–127. doi:10.1016/j.adolescence.2017.11.010
18. Berkman ND, Davis TC, McCormack L. Health literacy: what is it? J Health Commun. 2010;15(S2):9–19. doi:10.1080/10810730.2010.499985
19. Ferguson LA, Pawlak R. Health literacy: the road to improved health outcomes. J Nurse Pract. 2011;7(2):123–129. doi:10.1016/j.nurpra.2010.11.020
20. Kwon MS, Noh G-Y, Jang JH. A study on relationships between health literacy, disease-related knowledge and compliance to medical recommendations in patients with hypertension. J Korean Public Heal Nurs. 2013;27(1):190–202. doi:10.5932/JKPHN.2013.27.1.190
21. Miller TA. Health literacy and adherence to medical treatment in chronic and acute illness: a meta-analysis. Patient Educ Couns. 2016;99(7):1079–1086. doi:10.1016/j.pec.2016.01.020
22. Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67(12):2072–2078. doi:10.1016/j.socscimed.2008.09.050
23. Juul L, Rowlands G, Maindal HT. Relationships between health literacy, motivation and diet and physical activity in people with type 2 diabetes participating in peer-led support groups. Prim Care Diabetes. 2018;12(4):331–337. doi:10.1016/j.pcd.2018.02.005
24. Christy SM, Gwede CK, Sutton SK, et al. Health literacy among medically underserved: the role of demographic factors, social influence, and religious beliefs. J Health Commun. 2017;22(11):923–931. doi:10.1080/10810730.2017.1377322
25. Riemann L, Lubasch JS, Heep A, Ansmann L. The role of health literacy in health behavior, health service use, health outcomes, and empowerment in pediatric patients with chronic disease: a systematic review. Int J Environ Res Public Health. 2021;18(23):12464. doi:10.3390/ijerph182312464
26. Ghorbani-Dehbalaei M, Loripoor M, Nasirzadeh M. The role of health beliefs and health literacy in women’s health promoting behaviours based on the health belief model: a descriptive study. BMC Women's Health. 2021;21(1):421. doi:10.1186/s12905-021-01564-2
27. Hassanien NS, Adawi AM, Alzahrani TA, Adawi EA, Adawi A, Adawi E. The mediating role of resilience and electronic health literacy in the relationship between pandemic fatigue and adherence to preventive behaviours against COVID-19. Cureus. 2022;14(9):1.
28. Zhao YC, Zhao M, Song S. Online health information seeking among patients with chronic conditions: integrating the health belief model and social support theory. J Med Internet Res. 2022;24(11):e42447. doi:10.2196/42447
29. Michaelsen MM, Esch T. Motivation and reward mechanisms in health behavior change processes. Brain Res. 2021;1757:147309. doi:10.1016/j.brainres.2021.147309
30. Berdud M, Cabasés JM, Nieto J. Incentives and intrinsic motivation in healthcare. Gac Sanit. 2016;30(6):408–414. doi:10.1016/j.gaceta.2016.04.013
31. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68. doi:10.1037/0003-066X.55.1.68
32. Deci EL, Ryan RM. Facilitating optimal motivation and psychological well-being across life’s domains. Can Psychol Can. 2008;49(1):14. doi:10.1037/0708-5591.49.1.14
33. Lee MH, Park Y-H. The effectiveness of the information-motivation-behavioral skills model-based intervention on preventive behaviors against respiratory infection among community-dwelling older adults. Patient Educ Couns. 2021;104(8):2028–2036. doi:10.1016/j.pec.2021.01.016
34. Martela F, Hankonen N, Ryan RM, Vansteenkiste M. Motivating voluntary compliance to behavioural restrictions: self-determination theory–based checklist of principles for COVID-19 and other emergency communications. Eur Rev Soc Psychol. 2021;32(2):305–347. doi:10.1080/10463283.2020.1857082
35. Oyibo K. The relationship between perceived health message motivation and social cognitive beliefs in persuasive health communication. Information. 2021;12(9):350. doi:10.3390/info12090350
36. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis. Cengage Learning EMEA; 2019.
37. Kline P. A Handbook of Test Construction (Psychology Revivals): Introduction to Psychometric Design. Routledge; 2015.
38. Ohanian R. Construction and validation of a scale to measure celebrity endorsers’ perceived expertise, trustworthiness, and attractiveness. J Advert. 1990;19(3):39–52. doi:10.1080/00913367.1990.10673191
39. Sørensen K, Pelikan JM, Röthlin F, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25(6):1053–1058. doi:10.1093/eurpub/ckv043
40. Ajzen I. The Theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
41. Organization WH. Infection prevention and control [Internet]. WHO. [cited 2025 Nov 11]. Available from: https://www.who.int/teams/integrated-health-services/infection-prevention-control.
42. Centers for Disease Control and Prevention (CDC). How to protect yourself and others [Internet]. CDC. 2023 [cited 2025 Nov 11]. Available from: https://archive.cdc.gov/#/details?url=https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html.
43. Podsakoff PM, MacKenzie SB, Lee J-Y, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879. doi:10.1037/0021-9010.88.5.879
44. Snyder LB. Health communication campaigns and their impact on behavior. J Nutr Educ Behav. 2007;39(2):S32–40. doi:10.1016/j.jneb.2006.09.004
45. Carpenter CJ. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010;25(8):661–669. doi:10.1080/10410236.2010.521906
46. Jones CJ, Smith H, Llewellyn C. Evaluating the effectiveness of health belief model interventions in improving adherence: a systematic review. Health Psychol Rev. 2014;8(3):253–269. doi:10.1080/17437199.2013.802623
47. Jia X, Pang Y, Liu LS. Online Health Information Seeking Behavior: a Systematic Review. Healthc. 2021;9(12). doi:10.3390/healthcare9121740
48. Li H, Sakamoto Y. Social impacts in social media: an examination of perceived truthfulness and sharing of information. Comput Human Behav. 2014;41:278–287. doi:10.1016/j.chb.2014.08.009
49. Melki J, Tamim H, Hadid D, et al. Media exposure and health behavior during pandemics: the mediating effect of perceived knowledge and fear on compliance with COVID-19 prevention measures. Health Commun. 2022;37(5):586–596. doi:10.1080/10410236.2020.1858564
50. Wathen CN, Burkell J. Believe it or not: factors influencing credibility on the Web. J Am Soc Inf Sci Technol. 2002;53(2):134–144. doi:10.1002/asi.10016
51. Peerson A, Saunders M. Health literacy revisited: what do we mean and why does it matter? Health Promot Int. 2009;24(3):285–296. doi:10.1093/heapro/dap014
52. Soones TN, Lin JL, Wolf MS, et al. Pathways linking health literacy, health beliefs, and cognition to medication adherence in older adults with asthma. J Allergy Clin Immunol. 2017;139(3):804–809. doi:10.1016/j.jaci.2016.05.043
53. McKenna VB, Sixsmith J, Barry MM. The relevance of context in understanding health literacy skills: findings from a qualitative study. Heal Expect. 2017;20(5):1049–1060. doi:10.1111/hex.12547
54. Hardcastle SJ, Hancox J, Hattar A, Maxwell-Smith C, Thøgersen-Ntoumani C, Hagger MS. Motivating the unmotivated: how can health behavior be changed in those unwilling to change? Frontiers in Psychology. Frontiers Media SA. 2015;6:835.
55. Gillison FB, Rouse P, Standage M, Sebire SJ, Ryan RM. A meta-analysis of techniques to promote motivation for health behaviour change from a self-determination theory perspective. Health Psychol Rev. 2019;13(1):110–130. doi:10.1080/17437199.2018.1534071
56. Heideker S, Steul-Fischer M. The effects of message framing and ad credibility on health risk perception. Mark ZFP–Journal Res Manag. 2017;39(2):49–64.
57. Snyder LB, Hamilton MA, Mitchell EW, Kiwanuka-Tondo J, Fleming-Milici F, Proctor D. A meta-analysis of the effect of mediated health communication campaigns on behavior change in the United States. J Health Commun. 2004;9(S1):71–96. doi:10.1080/10810730490271548
58. Ahadzadeh AS, Wu SL, Ong FS, Deng R. The mediating influence of the unified theory of acceptance and use of technology on the relationship between internal health locus of control and mobile health adoption: cross-sectional study. J Med Internet Res. 2021;23(12):e28086. doi:10.2196/28086
59. Pelletier LG, Sharp E. Persuasive communication and proenvironmental behaviours: how message tailoring and message framing can improve the integration of behaviours through self-determined motivation. Can Psychol Can. 2008;49(3):210. doi:10.1037/a0012755
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.