")
Back to Journals » Journal of Pain Research » Volume 17
Perioperative Pain Observation of Hip Fracture Surgery Patients with Cheek Acupuncture
Authors Xu X, Zhao L, Li Y, Zhan L, Zheng L, Wang J
Received 15 August 2024
Accepted for publication 6 November 2024
Published 12 November 2024 Volume 2024:17 Pages 3719—3727
DOI https://doi.org/10.2147/JPR.S491669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Xingmei Xu, Libin Zhao, Yue Li, Li Zhan, Lidong Zheng, Jingxian Wang
Department of Anesthesiology, Lu’an Hospital of Anhui Medical University, Luan, 237000, People’s Republic of China
Correspondence: Li Zhan, Department of Anesthesiology, Lu’an Hospital of Anhui Medical University, Luan, 237000, People’s Republic of China, Email [email protected]
Background: The objective of this study is to investigate the impact of cheek acupuncture on perioperative pain in patients with hip fracture.
Methods: A random number table was utilized to allocate the patients into three distinct cohorts: Only spinal anesthesia was performed (group S), cheek acupuncture was performed before spinal anesthesia (group C), and ultrasound-guided fascia iliaca block was performed before spinal anesthesia (group F). The primary outcome measure was the Visual Analogue Scale (VAS) score within 24 hours post-surgery, as well as the level of beta-endorphin. The secondary outcome measures included intraoperative mean arterial pressure (MAP), heart rate (HR), length of hospital stay, postoperative complications, levels of interleukin-6 (IL-6), and degree of motor block.
Results: Compared to Group S, patients in group C and group F exhibited significantly lower Visual Analog Scale (VAS) scores at the following endpoints: when the patient is positioned in the spinal anesthesia position (T2); 12 hours post-surgery (T5); and 24 hours post-surgery (T6). And patients in group C and group F demonstrated a decreased beta-endorphin level at the T6. Compared to Group S, patients in group C and group F displayed reduced Mean Arterial Pressure (MAP) levels at T2.
Conclusion: The application of cheek acupuncture therapy in hip fracture surgery can effectively reduce the Visual Analog Scale (VAS) score, enhance perioperative safety, facilitate postoperative recovery, and optimize the overall medical experience for patients.
Clinical Trial: ChiCTR2100043194.
Keywords: cheek acupuncture, hip fracture, VAS score
Background
The term “pain” refers to an unpleasant sensory and emotional experience that is associated with actual or perceived noxious stimuli, encompassing various dimensions including sensory, emotional, cognitive, and social aspects.1 The presence of pain can result in compromised postoperative comfort, increased risk of wound infection, prolonged hospitalization, and other adverse outcomes.2 Moreover, it exerts significant physical and psychological impacts on patients while imposing a substantial financial burden on their families.
The experience of pain is always subjective and can be influenced to different extents by biological, psychological, and social factors.1 The occurrence of pain is significantly attributed to surgical procedures. Approximately 27% of patients who underwent hip surgery experienced persistent pain even six months post-surgery.3 The innervation of fascia and soft tissues may contribute to the occurrence of postoperative pain following hip surgery.4 Therefore, the alleviation of pain in patients undergoing hip surgery is currently a prominent focus in clinical research. Commonly employed clinical methods include spinal anesthesia, nerve block, non-steroidal anti-inflammatory drugs, and postoperative analgesic pumps.
Cheek acupuncture is a novel micro-needle technique developed by Professor WANG Yongzhou, which integrates modern anatomy, biological holography, and mind-body theory to achieve optimal therapeutic outcomes. The cheek acupuncture are typically crafted from specialized, ultra-fine and short filiform needles measuring 0.14–0.20mm in diameter and 7–30mm in length. Cheek acupuncture therapy is a painless and innovative treatment method that utilizes specific points on the cheek for acupuncture and moxibustion to effectively address systemic diseases.5 The therapeutic targets consist of 16 specific acupoints located in the cheek region. Cheek acupuncture is characterized by its convenient selection of acupoints, painless needling technique, high safety profile, rapid analgesic effects, and wide range of applications.6
The theory of cheek acupuncture therapy posits the existence of a holographic micro-system encompassing the entire human body within the cheek. By targeting specific acupoints in this area, the pain of hip fracture surgery can be achieved. The lumbar point can alleviate symptoms such as lower back pain, sciatica pain, and herniated disc.5 The hip point can alleviate symptoms such as sciatica pain and hip osteoarthritis caused by piriformis muscle injury.5 Additionally, the sacral point can provide relief for conditions including sacrospinous muscle strain and injuries of sacroiliac ligament.5 Therefore, the lumbar, hip, and sacral points were chosen for cheek acupuncture treatment in patients undergoing hip fracture surgery.
In this study, patients were categorized into three groups to investigate the potential disparity in analgesic effects between nerve block and cheek acupuncture among individuals undergoing hip fracture surgery. The Visual Analog Scale (VAS) score as well as the levels of IL-6 and beta-endorphin were monitored.
Materials and Methods
Study Design
This three-arm parallel randomized clinical study was conducted from December 2020 to October 2021 in accordance with the principles of the Declaration of Helsinki. The study received approval from the Ethics Committee for Clinical Trials of Lu’an Hospital, Anhui Medical University, China (approval no: 2020LL031). Prior to patient enrollment, the trial was registered in the Chinese Clinical Trial Registry (ChiCTR2100043194), and all patients provided written informed consent.
The study included patients who had undergone elective posterior approach hip fracture surgery and had an American Society of Anesthesiologists (ASA) physical status II or III, as well as a New York Heart Association Functional Classification (NYHA) class II or III. All patients aged between 60 and 90 years were excluded from the study if they met any of the following criteria: a history of mental disorders or communication problems within six months prior to admission, current use of psychotropic drugs; presence of heart, lung, liver or kidney dysfunction, hematopoietic system disease; known allergies to any drugs used in the study; contraindications to spinal anesthesia; refusal to participate by patients. Patients were divided into 3 groups: Only spinal anesthesia was performed (group S), cheek acupuncture was performed before spinal anesthesia (group C), and ultrasound-guided fascia iliaca block was performed before spinal anesthesia (group F).
Management of Anesthesia Process and Analgesia
Prior to the initiation of anesthesia, all patients observed an 8-hour fasting period and abstained from receiving any analgesic medications. Upon arrival in the operating room, intravenous access was established for administration purposes, while lactated Ringer’s solution was administered at a rate of 6–7mL/kg/h to maintain fluid levels. Continuous monitoring of vital parameters such as non-invasive blood pressure, electrocardiogram readings, heart rate, pulse oximetry levels, and respiratory rate was conducted using appropriate medical equipment (model: 866066, Philips Medizin Systeme Boeblingen, Germany). Given the majority of patients’ advanced age, this study utilized Stroke Volume Variation (SVV) for non-invasive hemodynamic monitoring (TL-400 model, Zhejiang Shashi Biological Instrument Co)., aiming to alleviate excessive volume burden.
After administering 100% oxygen via a mask, dexmedetomidine was intravenously injected using a micropump within a 15-minute timeframe at a dosage of 0.5 µg kg−1 if the patient’s heart rate exceeded 65 beats/min and mean arterial pressure (MAP) was above 70mmHg prior to anesthesia.
The patients in all three groups underwent spinal anesthesia. The patient was positioned in the lateral decubitus position at the L2-L3 or L3-L4 interspace. The patient grasped their knees while flexing their head downwards, maximizing spinal elongation. After disinfecting and covering the skin, a local infiltration anesthesia was performed in the puncture space using 4mL of lidocaine solution with a concentration of 2%. Subsequently, all patients in the three groups underwent spinal anesthesia utilizing a 25 gauge Quincke needle (Mekon Medical Devices Co. Shanghai, China) at the L2-L3 or L3-L4 space. After performing Cerebrospinal Fluid (CSF) aspiration, a solution of 0.5% ropivacaine (2mL) with an injection of 10% glucose (1mL) was administered into the subarachnoid space. Subsequently, the patient was promptly positioned in the supine posture.
Before spinal anesthesia, patients in group C received cheek acupuncture therapy. The administration of cheek acupuncture was performed by the same skilled physician. After disinfecting the skin with alcohol, the Cheek acupuncture was used to needle the lumbar, hip, and sacral points (Bond Medical Instrument Co., Ma’anshan, China). The hip point was located at the masseter tuberosity and 1 inch anterior to the mandibular angle. The scalar point was located at the masseter tuberosity and 0.5 inch anterior to the mandibular angle. Lumbar point was located at the middle of the connecting line between dorsal and sacral points. The position of dorsal point was in the cross of the lower edge of the zygomatic arch and the inferior capsule of the temporomandibular joint (Figure 1). The depth and direction of needling needed to be adjusted or additional needles closer to the acupoint were required until complete or significant pain relief was achieved, if the pain did not fully alleviate or only partially alleviated. The Cheek acupuncture is usually left in place for 40 minutes.
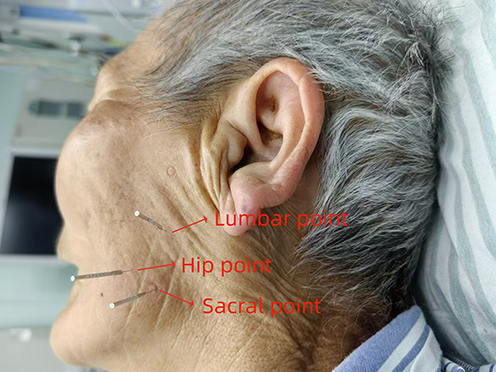 |
Figure 1 Acupoints of cheek acupuncture. |
Before spinal anesthesia, patients in group F underwent ultrasound-guided fascia iliaca block. Patients were placed in the supine position. After disinfecting and covering the skin, the linear US probe (Mindray Bio-medical Electronics Co., Shenzhen, China) with a frequency range of 5–10 MHz was positioned in a parasagittal orientation, medial to the anterosuperior iliac spine for acquiring the “bow-tie” sign.7 The sartorius, iliacus, and internal oblique muscles were identified. Utilizing an in-plane technique with a caudad to cephalad direction, the block needle was advanced until its tip was positioned between the internal oblique and iliacus muscles beneath the fascia iliaca. Subsequently, 30 mL of 0.25% ropivacaine was injected into the space within the iliac fascia.
The patients were administered intravenous patient-controlled analgesia (IV-PCA) for 48 hours postoperatively. The IV-PCA regimen included 1.5 g kg−1 of sufentanil and 100 mg of flurbiprofen axetil, with a total volume of 150 mL including 0.9% normal saline. The basal rate was set at 3 mL/h, with a bolus dose of 2 mL and a lockout time of 30 minutes.
Intraoperative Hemodynamic Monitoring and Management
The hemodynamic fluctuation range of elderly patients following spinal anesthesia is substantial, typically characterized by a decline in intraoperative blood pressure. Therefore, a single injection of 40 ug of norepinephrine or 6 mg of ephedrine was given when blood pressure decreased. Norepinephrine 0.08 µg kg−1 min−1 was pumped intraoperatively as blood pressure continued to decrease.8 When the heart rate was less than 50 beats/min, atropine was given 5–10 µg kg−1 to increase the heart rate; when the heart rate was more than 100 beats/min, esmolol was given 0.5–1 mg kg−1 to reduce the heart rate until the heart rate was in the normal range.
Outcome Measures
The primary endpoint was the achievement of pain remission within 24 hours post-surgery. We evaluated pain relief based on the visual analogue scale (VAS) and measured serum beta-endorphin levels.9,10 The VAS measurements were recorded at the following time points: 1 minute after admission to the operating room (T1); when the patient is positioned in the spinal anesthesia position (T2); at the conclusion of surgery (T3); 6 hours post-surgery (T4); 12 hours post-surgery (T5); and 24 hours post-surgery (T6). Serum samples were collected at T1 and T3.
Mean arterial pressure (MAP) and heart rate (HR) were measured at T1, T2, and T3. In addition, preoperative waiting time, Hamilton Anxiety Scale (HAMA) score before surgery, length of hospital stay, postoperative complications, IL-6 levels, and degree of motor block were recorded.
Detection of Serum Samples
Serum IL-6 level was detected by ELISA (kit was purchased from Shenzhen Jingmei Biotechnology Co. Shenzhen, China). Serum beta-endorphin level was detected by ELISA (kit was purchased from ImmunoWay Biotechnology Company, Suzhou, China). The operation process is carried out in strict accordance with SOP documents.
Randomization and Blinding
Once consent was received, participants were assigned by the research assistant to three groups according to a random allocation sequence. An online random list generation was utilized to perform blocked randomization in a 60:60:60 ratio. The anesthesiologist was not blinded to the trials because the anesthesiologist should choose the appropriate anesthesia method for the patient according to the grouped results. Outcome assessment and statistical analyses were performed by independent researchers. Outcome assessors and the surgical team were blinded to the study allocation status of participants.
Sample Size and Statistical Analyses
The sample size for the present study was determined using PASS 2008 software (NCSS, LLC., Kaysville, Utah, USA). The degrees of freedom and effect size for the incidence of pain among the three groups as a primary outcome were set at 2 and 0.3, respectively. A sample size of 50 patients per group would provide sufficient statistical power (80%) to detect a significant difference at an α-coefficient level of significance equaling 0.05 when considering potential dropout rates up to ten percent while aiming for increased statistical power, thus resulting in sixty patients per group being deemed necessary.
Statistical analyses were conducted using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). The measurement data were assessed for normal distribution using the Kolmogorov–Smirnov test and tested for homogeneity of variances using the Levene test. Normally distributed continuous data were presented as mean ± standard deviation, while non-normally distributed data were expressed as median (25th-75th percentile). Categorical variables were expressed as number (%). Categorical variables including sex, ASA classification, type of surgery, and postoperative complications were analyzed using χ2 test. Group comparisons of age, body mass index, preoperative waiting time, preoperative IL-6 and BNP, and hospital stay, VAS score and blood pressure, and CAM-CR score were performed using one-way analysis of variance (ANOVA). Post-hoc analysis in ANOVA with Bonferroni correction was performed.
For intraoperative hemodynamic parameters (MAP, HR), univariate analysis was performed using Independent-sample t test was employed to compare continuous variables between the two groups, and repeated measures one-way ANOVA was adopted for in-group comparisons.
Results
The CONSORT diagram is shown in Figure 2. Finally, 169 patients were randomly assigned to the following three groups: Only spinal anesthesia was performed (group S), cheek acupuncture was performed before spinal anesthesia (group C), and ultrasound-guided fascia iliaca block was performed before spinal anesthesia (group F).
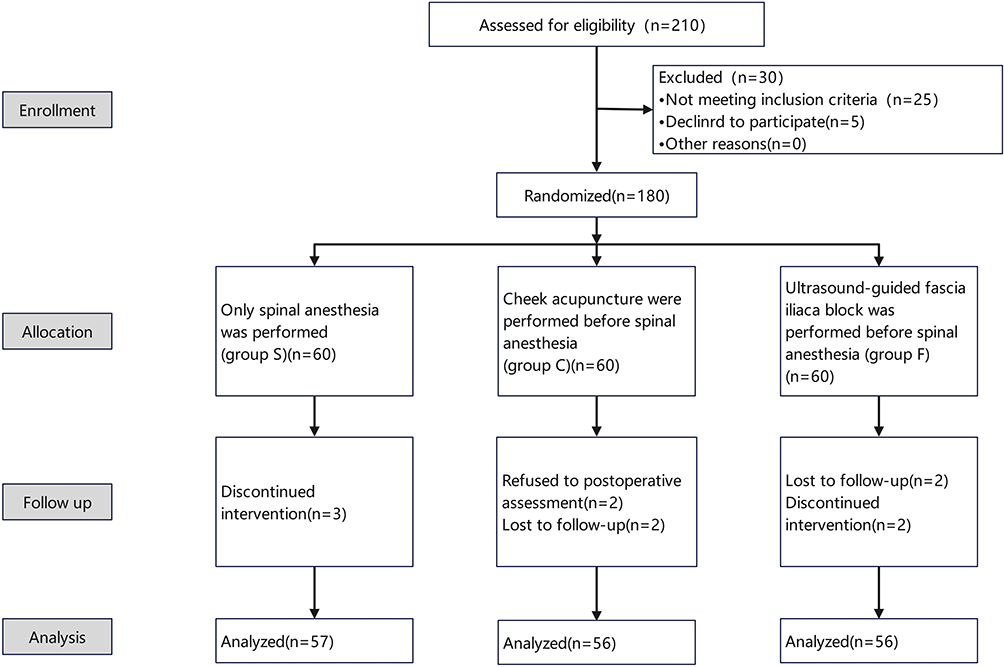 |
Figure 2 CONSORT flowchart. |
Patients’ Characteristics and Operative Data
No significant differences in age, gender, BMI, ASA, types of surgery, comorbidities, preoperative waiting time (from admission to surgery), or preoperative HAMA scale scores were observed among the three groups (Table 1). Additionally, there were no significant differences in surgery duration and hospital stay among the three groups.
 |
Table 1 Patient Characteristics and Operative Profiles |
Primary Endpoint
Compared to Group S, patients in group C and group F exhibited lower VAS scores at the following endpoints: when the patient is positioned in the spinal anesthesia position (T2); 12 hours post-surgery (T5); and 24 hours post-surgery (T6) (Table 2). Additionally, patients in group C and group F demonstrated lower beta-endorphin levels at T6 (Table 2).
 |
Table 2 The Data of VAS Score and Beta-Endorphin Level |
Secondary Endpoints and Postoperative Characteristics
Compared to Group S, patients in group C and group F exhibited significantly lower MAP levels at T2 (Table 3). Compared to Group S, patients in group C and group F demonstrated a significant decrease in IL-6 levels 24 hours after surgery (Table 4).
 |
Table 3 Intraoperative Hemodynamics |
 |
Table 4 Postoperative Data |
Discussion
The present prospective randomized study investigates the potential association between cheek acupuncture therapy and pain relief in elderly patients undergoing hip arthroplasty surgery. It is found that administering cheek acupuncture before spinal anesthesia effectively alleviates patient discomfort.
The surgical procedure of hip replacement is commonly performed in elderly patients, particularly among the majority of women. Postoperative pain following hip replacement can significantly impact the patient’s emotional well-being and, in severe cases, may necessitate a revision surgery while also increasing the risk of hospital readmission.11 The subjects of this study were elderly patients undergoing hip arthroplasty, who were specifically chosen to examine the impact of cheek acupuncture therapy on pain.
The impact of cheek acupuncture therapy on pain remains inconclusive. The analgesic mechanism of cheek acupuncture may involve the excitation of class II and III afferent nerve fibers, with subsequent interaction between the afferent signal and central nervous system processing and integration to produce an analgesic effect.12
The application of cheek acupuncture may potentially modulate the levels of monoamine neurotransmitters, such as serotonin, thereby exerting analgesic effects.13 Some studies have shown that the efficacy of cheek acupuncture in increasing the β-EP content in the cerebrospinal fluid of a rheumatoid arthritis rabbit model has been demonstrated, thereby exerting analgesic effects.14 Other studies have shown that mast cells may be the target of cheek acupuncture.15 In our study, compared to Group S, patients in group C and group F exhibited lower VAS scores at T2, T5 and T6 (Table 2). The β-EP level was found to be lower in patients belonging to group C and group F at T6 (Table 2). The application of cheek acupuncture when the patient is positioned in the spinal anesthesia position (T2) has been found to effectively alleviate pain, and our study demonstrates that its analgesic effect is comparable to iliac fascia block. Importantly, there was no statistically significant difference observed in motor block among the three groups, suggesting that cheek acupuncture has no impact on postoperative motor function (Table 4).
Studies have demonstrated that cheek acupuncture can elicit anti-inflammatory effects by inhibiting the synthesis of cyclooxygenase in both peripheral and central nociceptive sites.16 In this study, the postoperative IL-6 levels of patients in group C and F were found to be significantly lower than those in group S, indicating that both iliac fascia and cheek acupuncture have the potential to effectively mitigate inflammatory response (Table 4). The mechanism may involve mast cells inducing an antagonistic response in blood vessels and the nervous system, as well as local infiltration of inflammatory cells.17
Compared to Group S, patients in group C and group F exhibited significantly lower mean arterial pressure (MAP) levels at T2 (Table 3). This observation may be attributed to the potential mechanisms of enhancing blood flow in the vertebrobasilar artery or mitigating painful stimulation.18
However, the following are a few limitations of our study: (1) a small sample size, (2) a relatively short observation time for postoperative pain in the three groups, and (3) an absence of further clarification on the underlying principles of cheek acupuncture analgesia.
Conclusion
Therefore, the application of cheek acupuncture is convenient and carries a low risk of infection while also providing a good analgesic effect. Consequently, it can be safely utilized in elderly patients undergoing hip replacement surgery.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The study received approval from the Ethics Committee for Clinical Trials of Luan Hospital, Anhui Medical University, China (approval no: 2020LL031). Prior to patient enrollment, the trial was registered in the Chinese Clinical Trial Registry (ChiCTR2100043194), and all patients provided written informed consent. The study was carried out in accordance with the applicable guidelines and regulations.
Acknowledgments
We acknowledge that the first and second authors had equal contributions to write and finalize this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present study was financially supported by the Basic and Clinical Research Promotion Program of Anhui Medical University (2021xkjT041) and the Surface Item of Luan Hospital, Anhui Medical University (2021kykt02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
2. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/s0140-6736(21)00393-7
3. Wang HY, Xiao Q, Luo ZY, Pei FX, Wang D, Zhou ZK. A new cocktail formula with diprospan of local infiltration analgesia in primary total Hip arthroplasty: a prospective, randomized, controlled, observer-blinded study. Orthopaedic Surg. 2022;14(8):1799–1807. doi:10.1111/os.13288
4. Fede C, Porzionato A, Petrelli L, et al. Fascia and soft tissues innervation in the human Hip and their possible role in post-surgical pain. J Orthopaedic Res. 2020;38(7):1646–1654. doi:10.1002/jor.24665
5. Wang Y, Yang L, Wu Y. Case report: cheek acupuncture exhibits an immediate effect in relieving severe pain associated with nerve compression or damage of central nervous system and its potential mechanism of action. Front Neurosci. 2023;17:1211361. doi:10.3389/fnins.2023.1211361
6. Lin JG, Kotha P, Chen YH. Understandings of acupuncture application and mechanisms. Am J Transl Res. 2022;14(3):1469–1481.
7. Desmet M, Vermeylen K, Van Herreweghe I, et al. A Longitudinal Supra-Inguinal Fascia Iliaca Compartment Block Reduces Morphine Consumption After Total Hip Arthroplasty. Reg Anesth Pain Med. 2017;42(3):327–333. doi:10.1097/aap.0000000000000543
8. Fu F, Xiao F, Chen W, et al. A randomised double-blind dose–response study of weight-adjusted infusions of norepinephrine for preventing hypotension during combined spinal–epidural anaesthesia for Caesarean delivery. Br J Anaesth. 2020;124(3):e108–e114. doi:10.1016/j.bja.2019.12.019
9. Ye W, Hackett S, Vandevelde C, Twigg S, Helliwell PS, Coates LC. Comparing the Visual Analog Scale and the Numerical Rating Scale in Patient-reported Outcomes in Psoriatic Arthritis. J Rheumatol. 2021;48(6):836–840. doi:10.3899/jrheum.200928
10. Ahn H, La JH, Chung JM, et al. The Relationship Between β-Endorphin and Experimental Pain Sensitivity in Older Adults With Knee Osteoarthritis. Biol Res Nurs. 2019;21(4):400–406. doi:10.1177/1099800419853633
11. Fernández-de-Las-Peñas C, Florencio LL, de-la-Llave-Rincón AI, et al. Prognostic Factors for Postoperative Chronic Pain after Knee or Hip Replacement in Patients with Knee or Hip Osteoarthritis: an Umbrella Review. J Clin Med. 2023;12(20):6624. doi:10.3390/jcm12206624
12. Jie W The Proteomics Study on the Rheumatoid Arthritis Rabbit Models Induced by Egg Albumin After Buccal Acupuncture Intervention [Doctor Thesis]. Lanzhou: Gansu University of Chinese Medicine. 2017;72.
13. Pu R, Fang X, Jie W-J, Liu D-L, Su C-H. Experimentally investigating the effect of buccal acupuncture on analgesic time—effect characteristics and monoamine neumtransmitters. J Acupunct Tuina Sci. 2018;16(4):229–235. doi:10.1007/s11726-018-1055-x
14. Jie W, Fang X, Pu R, et al. Analgesic effect of buccal acupuncture on acute arthritis in rabbits and underlying mechanisms. J Central South Univ Med Sci. 2017;42(5):517–521. doi:10.11817/j.issn.1672-7347.2017.05.006
15. Yin N, Yang H, Yao W, Xia Y, Ding G, Duann J-R. Mast Cells and Nerve Signal Conduction in Acupuncture. eCAM. 2018;2018:3524279. doi:10.1155/2018/3524279
16. Yi Y, Huijun YE, Huiling Z, Lihua J. Clinical observation on 90 cases of primary dysmenorrhea treated by buccal acupuncture therapy: a randomized controlled study. J Tradition Chin Med. 2024;44(1):172–181. doi:10.19852/j.cnki.jtcm.20231110.001
17. Mukai K, Tsai M, Starkl P, Marichal T, Galli SJ. IgE and mast cells in host defense against parasites and venoms. Semin Immunopathol. 2016;38(5):581–603. doi:10.1007/s00281-016-0565-1
18. Takemoto Y, Ramirez RJ, Yokokawa M, et al. Galectin-3 Regulates Atrial Fibrillation Remodeling and Predicts Catheter Ablation Outcomes. JACC. 2016;1(3):143–154. doi:10.1016/j.jacbts.2016.03.003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.