")
Back to Journals » Nature and Science of Sleep » Volume 17
Persisting Short or Long Sleep Duration Predicts Post-Stroke Depression One year After Stroke and Transient Ischemic Attack
Authors Hu Y, Zuo L, Pan Y, Yan H , Wang Y, Zhao X
Received 5 September 2024
Accepted for publication 26 April 2025
Published 27 June 2025 Volume 2025:17 Pages 1507—1519
DOI https://doi.org/10.2147/NSS.S492838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yang Hu,1,* Lijun Zuo,1,* Yuesong Pan,2 Hongyi Yan,2 Yongjun Wang,1 Xingquan Zhao1
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xingquan Zhao, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, No. 119, South Fourth Ring West Road, Fengtai District, Beijing, People’s Republic of China, 100070, Tel +0086-010-59978350, Fax +0086-010-59973383, Email [email protected]
Objective: Disrupted sleep duration is associated with the risk of stroke, and abnormal sleep duration predicts depression. However, the association of changes in sleep duration with functional outcome and depression after acute ischemic stroke (AIS) or transient ischemic attack (TIA) is still unclear.
Methods: All patients diagnosed with AIS or TIA in the impairment of cognition and sleep (ICONS) from the China National Stroke Registry III were included. Post-stroke depression (PSD) was defined as a value on the Patient Health Questionnaire-9 (PHQ-9) ≥ 5. Sleep duration was classified as normal (7– 8 hours), short (< 7 hours), or long (≥ 9 hours). According to the sleep duration, patients were divided into four groups: group A (persisting normal), group B (changed from long or short to normal), group C (changed from normal to long or short), and group D (persisting long or short). Logistic regression was performed to evaluate the effects of sleep duration changes on PSD, quality of life, and functional outcome at 1-year follow-ups.
Results: A total of 1450 AIS or TIA patients at baseline with a mean age of 60.73± 10.82 years were followed for 1-year. The group with persisting long or short sleep duration exhibited a significantly higher risk of PSD [OR 1.58(95% CI (1.06~2.33)] and poor quality of life [OR 1.42(95% CI 1.04~1.94)] than those in the persisting normal group at 1-year after AIS and TIA when adjusted for covariates. Patients with a decreased sleep duration of > 1 hour had more risk of moderate to severe PSD [OR 2.26(95% CI 1.13~4.53)] than the persisting normal group. Patients with newly developed abnormal sleep duration (changed from normal to long or short) had a higher risk of poor functional outcome [OR 2.82(95% CI 1.33~5.96)] than the persisting normal group.
Conclusion: The alterations in sleep duration were independently associated with PSD, poor quality of life, and adverse outcomes at 1-year, suggesting that inadequate sleep quantity plays an important role in 1-year depression, quality of life, and adverse outcomes after AIS or TIA.
Keywords: mild stroke, persisting cognitive impairment, Montreal cognitive assessment-Beijing, functional dependence
Introduction
Stroke is the leading cause of death in China1-3 and many stroke survivors experience neurological impairments and mood disorders that affect their daily functioning and work capacity.4 Among the mood disorders, post-stroke depression (PSD) is the most common complication of acute ischemic stroke (AIS), with a prevalence of 24%–31%.5,6 PSD after stroke significantly reduces patient quality of life and increases the risk of mortality,7–9 where a meta-analysis showed a 1.59-fold increased risk of mortality in PSD patients.10
Sleep disorders are reported to be associated with a worsening functional outcome and increased risk of depression after stroke. Previous studies have indicated that up to 90% of patients with depression have sleep complaints11 and that sleep disorders were secondary manifestations of depression, suggesting that impaired sleep is a major risk factor.12 Studies have also demonstrated a U-shaped relationship between sleep duration and depression.13 Longitudinal studies showed that self-reported sleep issues represent a greater risk of developing depression.14 Sleep duration of <7 hours has been shown to be closely related to the development of depression and stroke.15 Sleep duration of shorter than 6 hours is, however, predictive of depression after ischemic stroke at 3 months.16 According to the American Heart Association, nightly sleep duration is one of the eight essential components for optimal cardiovascular health17 and it recommends, an appropriate nightly sleep duration for adults of 7 to 9 hours.15 Adequate sleep duration plays a vital role in maintaining physical and psychological health. Excessively long (>9 hours) or short sleep duration (<7 hours) has been identified as risk of adverse outcomes.18 A prior study showed that prolonged sleep was associated with lower scores of stroke-related quality of life (QOL).19 And some studies have reported that shorter or longer sleep duration was associated with increased mortality compared with participants with a sleep duration of 7–8 hours/night.20,21 Several studies have established an association between both self-reported short and long sleep duration and increased stroke risk22,23 and also found that both short and long sleep durations could be predictive of mortality risk.20,24 Previous studies on the relationship between sleep duration and PSD, quality of life, and stroke outcome were mostly conducted at one time point and lacked the metric of alterations in sleep duration. Whether the alterations in sleep duration, such as transitioning from normal to shorter or excessive sleep, affect PSD, quality of life, and adverse outcomes after stroke remains uncertain.
In this study, we seek to investigate the associations between changes in sleep duration after stroke, with depression, functional disability, and quality of life at 1-year post-stroke in patients from a Chinese national registry.
Materials and Methods
Subjects
Patients were enrolled from the Impairment of Cognition and Sleep after AIS or transient ischemic attack (TIA) in Chinese patients (ICONS) study. The ICONS study is one subgroup of the Chinese National Stroke Registry-III (CNSR-III), which is a multicenter prospective registry for patients presented to hospitals with AIS or TIA (within 7 days of onset) between August 2015 and March 2018, from 201 hospitals.25 Patients were eligible if they met all the following criteria: age over 18 years; completed the baseline and follow-up tests.
The exclusion criteria were as follows: (1) stroke mimics (ie, seizures, migraine); (2) illiteracy; (3) prior diagnosis of dementia (as diagnosed by physicians), or any major mental conditions; (4) neurological disorders that could not cooperate to evaluate cognition or sleep questionnaire, for example, aphasia, hemispatial neglect, disturbance of consciousness, or limb dyskinesia.
A total of 2625 patients enrolled in the ICONS subgroup. We excluded 281 patients with missing data for bedtime or waketime at 2 weeks or 3 months, and 894 patients without Health Questionnaire-9 (PHQ-9), General Anxiety Disorder-7 (GAD-7), or Modified Rankin Scale (mRS) data at 1-year. Finally, 1450 patients with TIA/minor stroke were enrolled in this study (Figure 1).
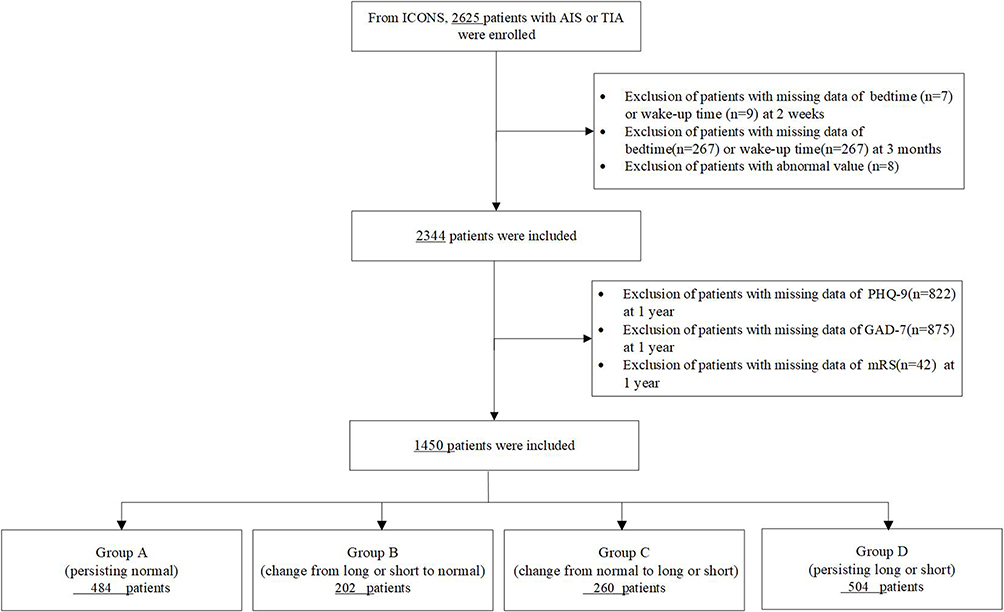 |
Figure 1 Flowchart of study participants. |
The data collection was approved by the ethics committee of Beijing Tiantan Hospital (KY2015-001-01). The study protocol has been conducted in accordance with the Declaration of Helsinki. Prior to data collection, all participants signed written informed consents.
Data Collection
The baseline demographic information and characteristics for all participants were noted, including age, gender, body mass index (BMI) [weight (kg)/height2 (m2)], current smoking habits, current drinking habits, systolic blood pressure (SBP), diastolic blood pressure (DBP), monthly income, marital status, medical history, and medication history. The medical history included previous stroke, hypertension, diabetes mellitus, hyperlipidemia, atrial fibrillation, heart failure, coronary heart disease, and peripheral vascular disease. The medication history contains antiplatelet or anticoagulant therapy, antihypertensive therapy, lipid-lowering therapy, and hypoglycemic therapy. Etiologic subtypes of ischemic stroke were classified by the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification criteria.26 The National Institutes of Health Stroke Scale (NIHSS) was used to evaluate stroke severity.27 Functional outcomes were evaluated using mRS and the quality of life was evaluated using the Stroke Impact Scale (SIS)-16 questionnaire.28 The SIS-16 measures 8 domains – strength, memory, emotion, communication, activities of daily living, mobility, hand function, and social participation. It has been widely used to assess the impact of stroke on quality of life in stroke patients.29
Sleep Duration
Sleep duration was defined as the time interval between bedtime and wake-up in the Pittsburgh Sleep Quality Index (PSQI).30 Sleep duration was classified as short sleep (<7 hours), normal sleep (≥7 and <9 hours) and long sleep (≥9 hours). Because of changes in sleep duration from 2 weeks to 3 months, we divided patients into four groups as mentioned above: group A (persisting normal); group B (Change from long or short to normal); group C (Change from normal into long or short); group D (persisting long or short). We also performed a secondary evaluation for the changes of sleep duration as follows: 1) >-1 hour (decrease in sleep duration of >1 hour); 2) −1 hour (decrease in sleep duration of 0.1 to 1 hour); 3) 0 (stable sleep duration, reference); 4) >1 hour (increase in sleep duration of ≥1 hour). The Epworth Sleeping Scale (ESS) was used to evaluated excessive daytime sleepiness.31
Outcome Assessment
Patients were asked standardized follow-up questions at 3 months and 1-year after stroke onset and outcome data included 1-year PSD, functional outcome, and quality of life after stroke. Evaluation of PSD was collected by face-to-face interviews at 2 weeks or discharge, 3 months, and 1-year. PHQ-9 was used to evaluate depression with a total score of 27 points. PSD was defined as a PHQ-9 score of ≥5, and moderate and severe PSD was defined as ≥10.32 GAD-7 was used to assess the severity of anxiety, with a total score of 21 points (whereby ≤4 represents no anxiety and 5–9, 10–14, and 15–21 represent mild, moderate, and severe anxiety).33 A poor functional outcome was defined as a score of 3 to 6 on the mRS.34 Poor quality of life was defined as a percentage of SIS-16<25%.35,36
Statistical Analyses
All statistical analyses were conducted with SAS 9.4 software (SAS Institute Inc, Cary, NC). The differences in baseline demographic and clinical features among the four groups were tested for continuous variables with normal distribution using ANOVA test and with skewed distribution using a nonparametric test. The χ2 or Fisher exact test was used for categorical variables.
Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile ranges (IQRs) and analyzed using the Kruskal–Wallis test. Categorical variables were described as frequencies (percentages) and tested with the χ2 or Fisher’s exact probability test.
We analyzed the associations between clinical outcomes including PSD, quality of life, and functional outcomes. For PSD, quality of life, poor functional outcome, and odds ratios (ORs) with 95% CIs were estimated by logistic regression models and fitted three adjusted models. Model 1 was adjusted for age and gender. Model 2 was further adjusted for PHQ-9, GAD-7, NIHSS, and mRS scores at admission, hypertension, diabetes, coronary heart disease, and stroke recurrence at 3 months, antiplatelets, antihypertensive therapy, lipid-lowering therapy and hypoglycemic therapy. Model 3 was additionally adjusted for history of sleep apnea, antiplatelets, antihypertensive therapy, lipid-lowering therapy, hypoglycemic therapy, sleep medicine usage(≥3 time a week). We determined that a two-tailed p values less than 0.05 was statistically significant.
Results
Baseline Characteristics of TIA/AIS Patients Categorized by Different Alterations of Sleep Duration
Among 2625 patients with ischemic stroke or TIA enrolled in the ICONS subgroup (CNSR-III study), 1175 patients were excluded (Figure 1). Finally, 1450 patients (mean age, 60.73±10.82 years), and 1055 (72.76%) were male. Participants included in the study had general characteristics similar to subjects who were excluded (Supplementary Table S1). Included participants had lower income, higher percentage of history of lipid metabolism disorders, antiplatelet or anticoagulant therapy, and lipid-lowering therapy sever anxiety and lower percentage of intravenous thrombolysis than patients excluded. (Supplementary Table S1).
According to their sleep duration, patients were divided into four groups: group A (persisting normal), group B (changed from long or short to normal), group C (changed from normal to long or short), and group D (persisting long or short). The baseline characteristics of the four groups are summarized in Table 1. In group D (persisting long or short), the proportion of patients that smoked was significantly lower and the average age, NIHSS score and GAD-7 scores were significantly higher when compared to those in group A (persisting normal). No significant differences were detected for sex, income, marital status, BMI, SBP, DBP, TOAST subtype, mRS score at admission, medication history, subjective sleep quality, the proportions of patients currently drinking, previous stroke, hypertension, diabetes, lipid metabolism disorders, atrial fibrillation, heart failure, coronary heart disease, sleep apnea or peripheral vascular disease. As for the use of sleep medication, 1358(94.17%) patients did not use any sleep medication, while 36(2.5%),17(1.18%) and 31 (2.15%) patients used sleep medicine once, twice and three or more times a week for the whole population. And there were no significant differences in the use of sleep medication among the 4 groups.
 |
Table 1 Baseline Characteristics of Study Participants by Sleep Duration Change Category |
At the 3-month assessment, 484 (33.38%) patients had persisting normal sleep duration, 260 (17.93%) patients had altered sleep duration transitioning from normal to long or short, 202 (13.93%) patients had altered sleep duration transitioning from long or short to normal, and 504 (34.76%) patients had persisting short or long sleep duration.
Association Between Different Sleep Duration Changes and 1-year Depression, Quality of life, and Functional Outcomes After Stroke
During the 1-year follow-ups, 252 (17.4%) of patients had PSD and 87 (6.0%) had moderate and severe PSD (Table 2). Patients with persisting long or short sleep duration (group D) had a higher risk of PSD (22.02% vs 12.6%, p<0.05), functional outcome (6.94% vs 3.10%, p<0.05), and quality of life (36.71% vs 24.59%, p<0.05) when compared to those with persisting normal sleep duration. Patients with persisting long or short sleep duration (group D) and patients with newly developed long or short sleep duration (group C) had higher risks of poorer functional outcome (6.94% vs 3.10%,7.31% vs 3.10%, p<0.05) when compared to those with persisting normal sleep duration (group A). The distribution of changes in sleep duration and the functional outcomes of AIS are shown in Figure 2.
 |
Table 2 Associations of Sleep Duration Change Category with Depression, Poor Functional Outcomes, Quality of Life After Stroke at 1 year |
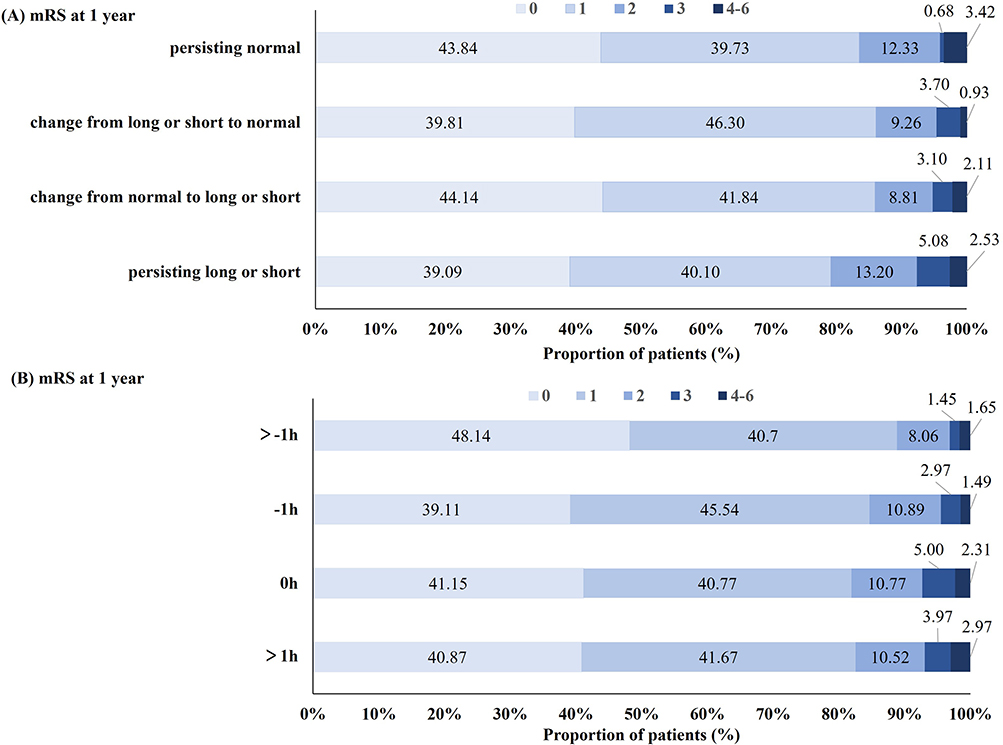 |
Figure 2 (A) Distribution of modified Rankin scale score at 12 months among different groups according to changes in sleep duration as mentioned above: group A (persisting normal); group B (Change from long or short to normal); group C (Change from normal into long or short); group D (persisting long or short); (B) Distribution of modified Rankin scale score at 12 months among different groups according to other changes of sleep duration as mentioned above: 1) >-1 h (decrease in sleep duration of >1 hour); 2) −1 h (decrease in sleep duration of 0.1 to 1 hour); 3) 0 (stable sleep duration, reference); 4) >1 h (increase in sleep duration of ≥1 hour). |
The association of sleep duration changes with 1-year PSD, quality of life, and functional outcomes after stroke is shown in Table 2. We found that compared with the patients with persisting normal sleep duration, those with persisting long or short sleep duration had an increased risk of PSD (PHQ-9≥5) (adjusted OR, 1.58; 95% CI, 1.06~2.33; p=0.01) and poorer quality of life (SIS-16<25%) after adjustment (adjusted OR, 1.42; 95% CI, 1.04~1.94; p=0.03), and those with newly developed long or short sleep duration had a poorer functional outcome after adjustment (adjusted OR, 2.82; 95% CI, 1.33~5.96; p=0.01), and those with persisting long or short sleep duration had a trend towards poor functional outcomes after adjustment (adjusted OR, 1.80; 95% CI, 0.92~3.52; p=0.09) (Table 2). A decrease in sleep duration of >1 hour was more likely to be associated with an increased risk of moderate and severe PSD (adjusted OR, 2.26; 95% CI, 1.13~4.53; p=0.02) (Table 3). The prolonged sleep duration of >1 hour trended towards a high risk for moderate and severe PSD (adjusted OR, 2.05; 95% CI, 1.04~4.04; p=0.04) (Table 3).
 |
Table 3 Associations of Sleep Duration Changes with Depression, Poor Functional Outcomes, Quality of Life After Stroke at 1 year |
Discussion
In this prospective cohort study, we investigated the effects of altered sleep duration on PSD, quality of life, and functional outcome after AIS/TIA at 1-year. Our findings revealed that patients with persisting short or long sleep duration were associated with 1-year PSD and poor quality of life after stroke. Especially, decreased sleep duration of >1 hour was associated with moderate to severe PSD. Altered sleep duration transitioning from normal to short or long was associated with an increased risk of 1-year poor functional outcome after AIS/TIA, even after adjusting for age, gender, medical histories, and sleep medicine usage. No significant associations were found between changes of sleep duration and others factors, including heart failure, sleep apnea and usage of sleep medicine. While other studies showed that heart failure, sleep apnea37 and usage of sleep medicine have impacts on sleep duration.38
According to the dynamic changes of sleep duration, we classified them into 4 groups. Both short and long sleep durations are reported to be related to adverse health outcomes. A meta-analysis containing seven prospective studies concluded that both short and long sleep durations are risk factors for depression.39 However, most studies were cross-sectional, and few longitudinal studies have investigated the effects of changed sleep duration on depression.40 Little is known about the impact of changes in sleep duration over time on the risk of PSD. Our study expands previous work in stroke patients by providing data on the role of altered sleep duration on the development of 1-year PSD. In this study, during 1-year follow-ups, the risk of PSD was significantly higher in those with persisting long or short sleep duration than in stroke survivors with persistently normal sleep duration (Table 2). Our findings are similar to existing evidence from the UK Household Longitudinal Study where reduced sleep duration was associated with depression.18 Furthermore, we found that a reduction in sleep duration >1 hour or prolonged sleep duration >1 hour had a higher risk of moderate to severe PSD than patients with no changed sleep duration, especially for patients with reduced sleep duration>1 hour. A prior study suggested that acute reduction in sleep duration was associated with various adverse health effects.41 Evidence suggests that >1 hour reduction in sleep duration for only a short period (approximately four days) could result in poorer emotional functioning42 and a decreased sleep duration of more than one hour might be a sensitive indicator of moderate to severe PSD. In a different study with young adults, results revealed that short sleep duration was associated with the incidence of depression.40 Reduced sleep duration might be associated with increased daytime sleepiness and fatigue, likely resulting in decreased social activity and increased social withdrawal and loneliness,43 both of which are risk factors for depression.40 Sleep deficiency results in endothelial dysfunction and an increase in inflammatory cytokine levels, such as interleukin-6 and tumor necrosis factor,12 and these inflammatory markers may contribute to the onset of depression. The increased inflammatory response can activate the kynurenine pathway, decrease serotonin synthesis, and affect other factors involved in the pathophysiology of neuropsychiatric conditions. Persisting long or short sleep duration might lead to alterations in sleep patterns, circadian rhythms, sleep self-balancing mechanisms, as well as levels and patterns of sleep-related hormone secretion.44 Sleep and depression are both associated with the activation of the hypothalamic-pituitary-adrenal axis. Moreover, sleep disorders and depression can change the gut microbiota and alter the microbiota-gut-brain axis.45 These mechanisms may partly explain the correlation between short or long sleep duration and depression.
Another study proposed a U-shaped association between sleep duration and the incidence of depression.46 An increased sleep duration (>9 hours) is associated with depression46,47 and prolonged sleep may lead to reduced physical activity, possibly decreasing the production of key hormones that regulate mood, such as serotonin or dopamine, or weakening self-efficacy and sense of well-being.48 Alternatively, excessive sleep has been suggested to be associated with poor socioeconomic status and increased social isolation, such as living alone, unemployment, or an unhealthy lifestyle, which can have a negative influence on psychological health, leading to depression.46,48 Persisting long or short sleep duration serves as a consequential predictor for PSD. There was a negative bidirectional relationship between sleep duration and psychological resilience.49 Good-quality sleep may enhance resilience and reduce symptoms of depressive symptom, thereby enhancing mental health.49
In this study, we also found that persisting short or long sleep duration was associated with a higher risk of poor quality of life at 1-year after stroke. In general, individuals with a sleep duration of 7~8 hours have lower morbidity risks and better quality of life than those without.50 Changes in sleep patterns resulted in the dysfunction of sleep-related hormone secretion, substantial changes in the brain, and were related to poor quality of life.44 A prior study assessing the quality of life(SIS-16) showed that the most impacted domains were strength, hand function, participation, and overall recovery.51
A prolonged sleep duration (>9 hours) was significantly associated with less time standing and a lower number of sit-to-stand transitions and steps, which might hinder stroke rehabilitation, and eventually result in a poor quality of life.51 Another study revealed that stroke patients without optimal sleep duration were associated with emotional instability and a lower score of health-related quality of life52 and this is inconsistent with our findings. Similarly, one cross-sectional study showed that most stroke survivors had emotional disorders, which are associated with a decline in life quality. Furthermore, sleep duration was reported to partially mediate the association between emotional disorders and quality of life.52 Stroke patients should be educated and supported to reach their optimal sleep duration, which is an important determinant of health.
Furthermore, we found that the changes in sleep duration from normal to long or short were associated with poor functional outcomes at 1-year after stroke and patients with persistent long or short sleep duration were also at a higher risk of 1-year poor functional outcomes, but this association weakened and did not reach statistical significance after adjustment for covariance, which may be related to its small sample size. Accumulating evidence suggests that sleep duration is related to stroke risk. Some have reported a J-shape relationship between long or short sleep duration and stroke,53,54 while other studies reported a U-shape relationship.55,56 One longitudinal study showed that individuals with a short-stable sleep duration (<7 hours) were significantly associated with a higher risk of stroke.57 Conversely, there is evidence showing that older adults who sleep for 9 or more hours have a higher prevalence of stroke55 and a prolonged sleep duration is associated with cardiovascular morbidity and mortality. One study reported that long sleep was associated with greater odds of the presence of carotid plaques relative to plaque absence and larger total plaque area after adjustment for covariance.58 The association between long sleep and subclinical carotid atherosclerosis may partially explain the associations between long sleep and stroke. Long sleep is also reported to be associated with inflammatory markers and white matter hyperintensity, which might be associated with adverse outcomes. Prolonged sleep duration may be an epiphenomenon of comorbidity,59 which is usually associated with adverse outcomes. Relative to prior studies that defined short sleep as <5 hours, our study’s categorization of sleep duration as short (<7 hours), intermediate (≥7 and <9 hours), and long (≥9 hours) are more consistent with consensus recommendations.
Sleep duration, mood, and stroke interact with each other, and sleep disorders and depression are not only considered risk factors for stroke but also predict adverse outcomes. Abnormal sleep duration, while increasing the risk of depression after stroke, together with psychosocial factors, will affect the quality of life and functional prognosis in AIS/TIA patients. Therefore, the results of this study have highlighted that AIS/TIA patients with persisting short or long sleep duration or with transitioning from normal to long or short should be given prioritized attention, and, if necessary, early intervention. As sleep duration is modifiable, it may serve as a target for interventions that could mitigate depression, quality of life and poor functional outcomes after stroke.
To the best of our knowledge, this study is the first to investigate the effects of altered sleep duration on PSD, quality of life, and functional outcomes after stroke. However, our study has some limitations. Firstly, sleep duration was assessed using a self-reported questionnaire. This study did not obtain polysomnography, which objectively measures sleep activity. Although previous studies suggested that self-reported sleep assessment correlates well with actigraphy,60,61 the self-reported sleep status may not reflect what it was in reality. Further study needs partial polysomnography recordings and validates the self-reported sleep duration. Although we record and adjust the history of sleep apnea in the regression model, it maybe more accuracy to use the polysomnography to record the sleep-disordered breathing and clarify whether the association between long sleep and functional outcomes was independent of sleep-disordered breathing. Thirdly, because of this study design, the causal relationships could not be established.
Conclusions
This study showed that AIS/TIA patients with persisting long or short sleep duration are associated with a higher risk of 1-year depression, as well as poor quality of life. Patients transitioning from normal to long or short sleep duration had a higher risk of poor functional outcome at 1-year follow-ups. Our findings highlight the importance of improving sleep duration and establishing healthy sleep habits to prevent emotional symptoms and poor functional outcomes. Thus, stroke education should offer sleep health education to stroke survivors, thereby increasing their awareness regarding healthy sleep. Targeted interventions are needed to address those with persistently long or short sleep duration or with transitioning from normal to short or long sleep duration in this population.
Acknowledgments
The authors would like to thank all participants for their involvement. This work was performed at Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
Funding
This work was supported by the following institutions: the National Natural Science Foundation of China (81870905, U20A20358) and the Capital Medical University Cultivation Fund (PYZ23117).
Disclosure
The authors declare no conflicts of interest related to this study.
References
1. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2019;394:1145–1158. doi:10.1016/S0140-6736(19)30427-1
2. Wang W, Jiang B, Sun H, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017;135:759–771. doi:10.1161/CIRCULATIONAHA.116.025250
3. Wang Y, Zhao X, Jiang Y, et al. Prevalence, knowledge, and treatment of transient ischemic attacks in China. Neurology. 2015;84:2354–2361. doi:10.1212/WNL.0000000000001665
4. Medeiros GC, Roy D, Kontos N, Beach SR. Post-stroke depression: a 2020 updated review. Gen Hosp Psychiatry. 2020;66:70–80. doi:10.1016/j.genhosppsych.2020.06.011
5. Guo J, Wang J, Sun W, Liu X. The advances of post-stroke depression: 2021 update. J Neurol. 2022;269:1236–1249. doi:10.1007/s00415-021-10597-4
6. Castilla-Guerra L, Fernandez Moreno MDC, Esparrago-Llorca G, Colmenero-Camacho MA. Pharmacological management of post-stroke depression. Expert Rev Neurother. 2020;20:157–166. doi:10.1080/14737175.2020.1707666
7. Bartoli F, Lillia N, Lax A, et al. Depression after stroke and risk of mortality: a systematic review and meta-analysis. Stroke Res Treat. 2013;2013:862978. doi:10.1155/2013/862978
8. House A, Knapp P, Bamford J, Vail A. Mortality at 12 and 24 months after stroke may be associated with depressive symptoms at 1 month. Stroke. 2001;32:696–701. doi:10.1161/01.STR.32.3.696
9. Unsworth DJ, Mathias JL, Dorstyn DS. Preliminary screening recommendations for patients at risk of depression and/or anxiety more than 1 year poststroke. J Stroke Cerebrovasc Dis. 2019;28:1519–1528. doi:10.1016/j.jstrokecerebrovasdis.2019.03.014
10. Fan XW, Yang Y, Wang S, et al. Impact of persistent poor sleep quality on post-stroke anxiety and depression: a national prospective clinical registry study. Nat Sci Sleep. 2022;14:1125–1135. doi:10.2147/NSS.S357536
11. Tsuno N, Besset A, Ritchie K. Sleep and depression. J Clin Psychiatry. 2005;66:1254–1269. doi:10.4088/JCP.v66n1008
12. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23:2324–2332. doi:10.1111/jcmm.14170
13. Liu Q, He H, Yang J, Feng X, Zhao F, Lyu J. Changes in the global burden of depression from 1990 to 2017: findings from the global burden of disease study. J Psychiatr Res. 2020;126:134–140. doi:10.1016/j.jpsychires.2019.08.002
14. Riemann D, Voderholzer U. Primary insomnia: a risk factor to develop depression? J Affect Disord. 2003;76:255–259. doi:10.1016/S0165-0327(02)00072-1
15. Watson NF, Badr MS, Belenky G, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of sleep medicine and sleep research society. Sleep. 2015;38:843–844. doi:10.5665/sleep.4716
16. Liu F, Yang Y, Wang S, et al. Impact of sleep duration on depression and anxiety after acute ischemic stroke. Front Neurol. 2021;12:630638. doi:10.3389/fneur.2021.630638
17. Lloyd-Jones DM, Allen NB, Anderson CAM, et al. Life’s essential 8: updating and enhancing the American heart association’s construct of cardiovascular health: a presidential advisory from the American heart association. Circulation. 2022;146:e18–e43. doi:10.1161/CIR.0000000000001078
18. Tang NK, Fiecas M, Afolalu EF, Wolke D. Changes in sleep duration, quality, and medication use are prospectively associated with health and well-being: analysis of the UK household longitudinal study. Sleep. 2017;40.
19. Kasai A, Saitou H, Takano M, et al. Pre-stroke habitual prolonged sleep as a predictor for post-stroke sleep quality, stroke-related quality of life, and lifestyle values. J Clin Neurosci. 2021;90:26–31. doi:10.1016/j.jocn.2021.05.018
20. Yh W, Wang J, Chen SH, et al. Association of longitudinal patterns of habitual sleep duration with risk of cardiovascular events and all-cause mortality. JAMA Network Open. 2020;3:e205246. doi:10.1001/jamanetworkopen.2020.5246
21. Diao T, Zhou L, Yang L, et al. Bedtime, sleep duration, and sleep quality and all-cause mortality in middle-aged and older Chinese adults: the dongfeng-Tongji cohort study. Sleep Health. 2023;9:751–757. doi:10.1016/j.sleh.2023.07.004
22. Yin J, Jin X, Shan Z, et al. Relationship of sleep duration with all-cause mortality and cardiovascular events: a systematic review and dose-response meta-analysis of prospective cohort studies. J Am Heart Assoc. 2017;6.
23. Akinseye OA, Ojike NI, Akinseye LI, Dhandapany PS, Pandi-Perumal SR. Association of sleep duration with stroke in diabetic patients: analysis of the national health interview survey. J Stroke Cerebrovasc Dis. 2016;25:650–655. doi:10.1016/j.jstrokecerebrovasdis.2015.11.023
24. Cappuccio FP, D’Elia L, Strazzullo P, Miller MA. Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep. 2010;33:585–592. doi:10.1093/sleep/33.5.585
25. Wang Y, Jing J, Meng X, et al. The third China national stroke registry (cnsr-iii) for patients with acute ischaemic stroke or transient ischaemic attack: design, rationale and baseline patient characteristics. Stroke Vasc Neurol. 2019;4:158–164. doi:10.1136/svn-2019-000242
26. Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. toast. trial of org 10172 in acute stroke treatment. Stroke. 1993;24:35–41. doi:10.1161/01.STR.24.1.35
27. Adams HP Jr, Davis PH, Leira EC, et al. Baseline nih stroke scale score strongly predicts outcome after stroke: a report of the trial of org 10172 in acute stroke treatment (toast). Neurology. 1999;53:126–131. doi:10.1212/WNL.53.1.126
28. Duncan PW, Lai SM, Bode RK, Perera S, DeRosa J. Stroke impact scale-16: a brief assessment of physical function. Neurology. 2003;60:291–296. doi:10.1212/01.WNL.0000041493.65665.D6
29. Duncan PW, Lai SM, Tyler D, Perera S, Reker DM, Studenski S. Evaluation of proxy responses to the stroke impact scale. Stroke. 2002;33:2593–2599. doi:10.1161/01.STR.0000034395.06874.3E
30. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. the Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi:10.1016/0165-1781(89)90047-4
31. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14:540–545. doi:10.1093/sleep/14.6.540
32. Negeri ZF, Levis B, Sun Y, et al. Accuracy of the patient health questionnaire-9 for screening to detect major depression: updated systematic review and individual participant data meta-analysis. BMJ. 2021;375:n2183. doi:10.1136/bmj.n2183
33. Löwe B, Decker O, Müller S, et al. Validation and standardization of the generalized anxiety disorder screener (gad-7) in the general population. Med Care. 2008;46:266–274. doi:10.1097/MLR.0b013e318160d093
34. Weisscher N, Vermeulen M, Roos YB, de Haan RJ. What should be defined as good outcome in stroke trials; a modified rankin score of 0-1 or 0-2? J Neurol. 2008;255:867–874. doi:10.1007/s00415-008-0796-8
35. Moran GM, Fletcher B, Feltham MG, Calvert M, Sackley C, Marshall T. Fatigue, psychological and cognitive impairment following transient ischaemic attack and minor stroke: a systematic review. Eur J Neurol. 2014;21:1258–1267. doi:10.1111/ene.12469
36. Liao X, Zuo L, Dong Y, et al. Persisting cognitive impairment predicts functional dependence at 1 year after stroke and transient ischemic attack: a longitudinal, cohort study. BMC Geriatr. 2022;22:1009. doi:10.1186/s12877-022-03609-z
37. Türoff A, Thiem U, Fox H, et al. Sleep duration and quality in heart failure patients. Sleep Breath. 2017;21:919–927. doi:10.1007/s11325-017-1501-x
38. Wang J, Wang Z, Wang X, et al. Combination of alprazolam and bailemian capsule improves the sleep quality in patients with post-stroke insomnia: a retrospective study. Front Psychiatry. 2019;10:411. doi:10.3389/fpsyt.2019.00411
39. Zhai L, Zhang H, Zhang D. Sleep duration and depression among adults: a meta-analysis of prospective studies. Depress Anxiety. 2015;32:664–670. doi:10.1002/da.22386
40. Um YJ, Kim Y, Chang Y, et al. Association of changes in sleep duration and quality with incidence of depression: a cohort study. J Affect Disord. 2023;328:64–71. doi:10.1016/j.jad.2023.02.031
41. Roenneberg T, Allebrandt KV, Merrow M, Vetter C. Social jetlag and obesity. Curr Biol. 2012;22:939–943. doi:10.1016/j.cub.2012.03.038
42. Vriend JL, Davidson FD, Corkum PV, Rusak B, Chambers CT, McLaughlin EN. Manipulating sleep duration alters emotional functioning and cognitive performance in children. J Pediatr Psychol. 2013;38:1058–1069. doi:10.1093/jpepsy/jst033
43. Holding BC, Sundelin T, Schiller H, Åkerstedt T, Kecklund G, Axelsson J. Sleepiness, sleep duration, and human social activity: an investigation into bidirectionality using longitudinal time-use data. Proc Natl Acad Sci U S A. 2020;117:21209–21217. doi:10.1073/pnas.2004535117
44. Li J, Vitiello MV, Gooneratne NS. Sleep in normal aging. Sleep Med Clin. 2022;17:161–171. doi:10.1016/j.jsmc.2022.02.007
45. Manosso LM, Duarte LA, Martinello NS, Mathia GB, Réus GZ. Circadian rhythms and sleep disorders associated to major depressive disorder: pathophysiology and therapeutic opportunities. CNS Neurol Disord Drug Targets. 2024;23:1085–1100. doi:10.2174/0118715273254093231020052002
46. Dong L, Xie Y, Zou X. Association between sleep duration and depression in us adults: a cross-sectional study. J Affect Disord. 2022;296:183–188. doi:10.1016/j.jad.2021.09.075
47. Supartini A, Honda T, Basri NA, et al. The impact of sleep timing, sleep duration, and sleep quality on depressive symptoms and suicidal ideation amongst Japanese freshmen: the equsite study. Sleep Disord. 2016;2016:8737654. doi:10.1155/2016/8737654
48. Salmon P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: a unifying theory. Clin Psychol Rev. 2001;21:33–61. doi:10.1016/S0272-7358(99)00032-X
49. Arora T, Grey I, Östlundh L, et al. A systematic review and meta-analysis to assess the relationship between sleep duration/quality, mental toughness and resilience amongst healthy individuals. Sleep Med Rev. 2022;62:101593. doi:10.1016/j.smrv.2022.101593
50. Ren Y, Miao M, Yuan W, Sun J. Sleep duration and all-cause mortality in the elderly in China: a population-based cohort study. BMC Geriatr. 2020;20:541. doi:10.1186/s12877-020-01962-5
51. Ezeugwu VE, Manns PJ. Sleep duration, sedentary behavior, physical activity, and quality of life after inpatient stroke rehabilitation. J Stroke Cerebrovasc Dis. 2017;26:2004–2012. doi:10.1016/j.jstrokecerebrovasdis.2017.06.009
52. Liu W, Liu X, Wang J, et al. Predicting the relationship between anxiety and health-related quality of life in post-stroke patients: the role of sleep duration. J Stroke Cerebrovasc Dis. 2023;32:107368. doi:10.1016/j.jstrokecerebrovasdis.2023.107368
53. Zhou L, Yu K, Yang L, et al. Sleep duration, midday napping, and sleep quality and incident stroke: the dongfeng-Tongji cohort. Neurology. 2020;94:e345–e356. doi:10.1212/WNL.0000000000008739
54. Zhu G, Cassidy S, Hiden H, et al. Exploration of sleep as a specific risk factor for poor metabolic and mental health: a UK biobank study of 84,404 participants. Nat Sci Sleep. 2021;13:1903–1912. doi:10.2147/NSS.S323160
55. Titova OE, Michaëlsson K, Larsson SC. Sleep duration and stroke: prospective cohort study and Mendelian randomization analysis. Stroke. 2020;51:3279–3285. doi:10.1161/STROKEAHA.120.029902
56. Fang Y, He Y, Huang Y, et al. Sleep duration, daytime napping, and risk of incident stroke: nuances by metabolic syndrome from the China health and retirement longitudinal study. Front Cardiovasc Med. 2022;9:976537. doi:10.3389/fcvm.2022.976537
57. Fang Y, Yang MJ, Ning D, et al. Associations between sleep duration trajectories and risk of cardio-metabolic disease among middle-aged and older Chinese adults. J Affect Disord. 2024;362:126–133. doi:10.1016/j.jad.2024.06.114
58. Agudelo C, Ramos AR, Gardener H, et al. Sleep duration is associated with subclinical carotid plaque burden. Stroke. 2023;54:2347–2355. doi:10.1161/STROKEAHA.122.041967
59. Stranges S, Dorn JM, Shipley MJ, et al. Correlates of short and long sleep duration: a cross-cultural comparison between the United Kingdom and the United States: the Whitehall ii study and the western New York health study. Am J Epidemiol. 2008;168:1353–1364. doi:10.1093/aje/kwn337
60. Signal TL, Gale J, Gander PH. Sleep measurement in flight crew: comparing actigraphic and subjective estimates to polysomnography. Aviat Space Environ Med. 2005;76:1058–1063.
61. Patel SR, Ayas NT, Malhotra MR, et al. A prospective study of sleep duration and mortality risk in women. Sleep. 2004;27:440–444. doi:10.1093/sleep/27.3.440
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Sleep Duration and Stroke in Different Status of Metabolic Syndrome: A Cross-Sectional Study in Shanghai Adult Residents
Wu H, Zheng Y, Liu DN, Liu XX, Yang QD, Su QY, Wang YQ, Wang YZ, La XN, Shi Y, Fu C
Nature and Science of Sleep 2023, 15:639-652
Published Date: 9 August 2023
The Correlation Between Caregivers Burden and Quality of Life Among Family Caregivers of Stroke Survivors: The Mediating Role of Resilience
Handayani F, Kusumaningrum NSD, Dwidiyanti M
Nursing: Research and Reviews 2024, 14:91-102
Published Date: 19 June 2024
Gender and Age Differences in the Relationship Between Smartphone Addiction and Sleep Duration in Korean Children: A Panel Quantile Regression Study
Jeong K, Cho S, Song D, Li R, Han S, Cho HJ, Kim J
Psychology Research and Behavior Management 2024, 17:4183-4192
Published Date: 8 December 2024