")
Back to Journals » Patient Preference and Adherence » Volume 19
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Authors Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Received 29 August 2024
Accepted for publication 4 December 2024
Published 25 January 2025 Volume 2025:19 Pages 215—234
DOI https://doi.org/10.2147/PPA.S486553
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Sonia Roldan Munoz,1 Peter GM Mol,1 Femke de Vries,2 Peter R van Dijk,3 Hans Hillege,4 Douwe Postmus,4 Sieta T de Vries1
1Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Center Groningen, Groningen, Netherlands; 2Faculty of Beta Science, Vrije Universiteit Amsterdam, Amsterdam, Netherlands; 3Division of Endocrinology, Department of Internal Medicine, University of Groningen, University Medical Center Groningen, Groningen, Netherlands; 4Department of Epidemiology, University of Groningen, University Medical Center Groningen, Groningen, Netherlands
Correspondence: Sieta T de Vries, Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Center Groningen, Groningen, Netherlands, Email [email protected]
Background: Treatment guidelines recommend metformin as initial drug in many people with type 2 diabetes (T2D) and low risk of cardiovascular disease, with the possibility to switch to or add other drug classes. A decision aid (DA) could be useful to incorporate a patient’s preferences in the decision of which drug class to choose. We developed such a DA and assessed the perspectives of people with T2D towards its comprehensibility and usability.
Methods: The DA consists of a paper-based leaflet followed by a web-based preference elicitation exercise. The leaflet aims at informing patients about drug characteristics (eg, efficacy, safety). The relative importance of these drug characteristics for each participant are then assessed in a web-based exercise, which results in a ranking of the preferred drug classes. A qualitative study using semi-structured interviews was conducted among Dutch patients with T2D who were or had ever been under pharmacological treatment for T2D. The audio-recorded interviews were transcribed verbatim. Thematic analysis was conducted.
Results: Fifteen patients participated (median age 64 years, nine women, and most had T2D > 10 years). Risk of hypoglycaemia was most often the characteristic to which patients attached the highest importance (n=5). A glucagon-like peptide-1-antagonist weekly injection fitted best the preferences of most patients (n=8). The interviews revealed improvements for text, pictograms and figures, and formatting, and increased comprehension of how patients completed the DA. Regarding usability, missing information was identified, as well as patients’ perspectives about the usefulness of the DA and its role in shared-decision making.
Conclusion: The DA was considered promising for shared-decision making but further improvements regarding its comprehensibility and usability are needed, for which this study provides clear guidance.
Keywords: decision aid, diabetes mellitus, type 2, qualitative research, participant preference
Introduction
People with type 2 diabetes mellitus (T2D) have an increased risk of micro- and macrovascular complications.1 Therefore, adequate management of the disease and associated risk factors for cardiovascular diseases, such as hypertension and smoking, is crucial. Guidelines for the management of T2D recommend starting with lifestyle changes (eg, adjusting food intake and increasing physical activity) and initiating pharmaceutical treatment if there is insufficient glycaemic control.2 Metformin is considered the first-line pharmaceutical treatment for many patients, in particular in those with low risk of cardiovascular and renal diseases.3–5 A switch to or addition of other drug classes, such as dipeptidyl peptidase-4 (DPP-4) inhibitors, sulfonylureas, and sodium-glucose cotransport-2 (SGLT-2) inhibitors, is possible in case glycated haemoglobin (HbA1c) targets are not met or metformin is not well-tolerated.2,6
Although these drug classes are all marketed for the treatment of diabetes, there are differences in their characteristics, such as in their mode and frequency of administration, efficacy, and profile of possible adverse drug reactions (ADRs).7 Previous studies have shown heterogeneity in preferences among patients towards such drug characteristics,8 and, in addition to clinical characteristics, treatment guidelines advise to incorporate patient preferences at the time of clinical decision-making.2,9 Involving patients in treatment decisions may increase commitment, satisfaction, and adherence, which may ultimately lead to better outcomes.10–12 A decision aid (DA) could be a useful tool when deciding on treatments in this so-called shared-decision making process between the healthcare professional (HCP) and the patient.13–16 A DA is a tool that provides information about clinical decisions, and helps patients on communicating the personal values they attach to the characteristics of the treatment options.17
In the field of diabetes, review studies have identified randomized controlled trials testing the effects of various DAs.16–18 These studies aimed, mainly, at testing the development of new DAs, exploring whether a DA improved communication with HCPs, enhanced informed clinical decisions, and/or improved treatment outcomes, among people with T2D or people in need to add preventive therapies, such as statins. In this paper, we describe a DA to elicit participants’ preferences towards specific treatment characteristics and drug classes to use in addition to or as a replacement of metformin. Also, we present the results of a pilot study that assessed the perspectives of people with T2D regarding the comprehensibility of the DA and its usability in clinical practice.
Materials and Methods
The DA contains five steps (Figure 1) and consists of a paper-based leaflet and web-based preference elicitation exercise in the Dutch language.
 |
Figure 1 Overview of the decision aid. Abbreviations: T2D, Type 2 diabetes; HCP, Healthcare professional. |
The leaflet (Figure 1-step 1) provides some basic information about T2D and the different treatment steps based on guidelines,2,6 and gives information about several drug characteristics using text, pictograms, and figures. The included drug characteristics are “mode and frequency of administration”, “effect on blood glucose”, “effect on cardiovascular risk reduction”, “effect on body weight”, “risk of hypoglycaemia”, and “risk of diarrhoea, nausea and vomiting”. These characteristics, so-called attributes, were selected because they were found important to patients in their preferences towards pharmacological treatments for T2D.8,19,20 For each attribute, there are two or three options, so-called levels, which are based on the actual attributes of the included drug classes in the DA (Table 1). The included drug classes are those currently marketed and mentioned in guidelines as options to treat high HbA1c levels when metformin (alone) is insufficient or causes intolerable ADRs, ie, DPP-4 inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, SGLT-2 inhibitors, sulfonylureas, and insulin.2,4,6 Internists specialised in diabetes were consulted to finalize the included attributes and levels. An overview of the drug classes with their effects classified in the attribute levels21–25 is available in Supplementary Table 1. At the end of the leaflet, four multiple-choice questions are presented to assess the reader’s understanding of the provided information.
 |
Table 1 Attributes and Attribute Levels Included in the Decision Aid |
The web-based preference elicitation exercise (Figure 1-step 3) contains the attributes and attribute levels described in the leaflet. The exercise starts with a short explanation (Supplementary Figure 1A). Subsequently, patients have to respond to eight pairwise comparison questions in which they are asked to choose between two treatments (labelled as treatment A and treatment B) (Supplementary Figure 1B). The treatments are described by two attributes with different levels each time. The exercise is adaptive, meaning that the pairwise comparison questions change for each participant according to their answers. The question tree for this adaptive exercise was generated in R (version 4.0.2 R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/) using an entropy-based approach to find a sequence of pairwise comparison questions that maximizes the information gained at each node of the question tree.26 For most attributes, a ranking in the levels is assumed in the question tree; for instance for “effect on blood glucose”, the largest and lowest decreases are considered the best and worst options, respectively. For the attributes “mode and frequency of administration” and “effect on body weight”, however, the best and worst levels may vary from person to person. Therefore, participants are asked about their preferred ranking for these attribute levels before starting the exercise (Figure 1-step 2). This variability in rankings could lead to nine possible combinations. However, we assumed that weekly injection would always be preferred over daily injection, reducing the number of possible combinations to six. To cover the six combinations, we generated six question trees, with the only variation of the best to worst attribute levels according to these previous choices. The question trees were implemented in the web application Research Electronic Data Capture 10.0.23 (REDCap – www.projectredcap.org). After completing the exercise, an R-script has to be run to generate the results (Figure 1-step 4). The outcome of the exercise is an overview of the person’s importance attached to the attributes via a radar plot, a ranking of the drug classes in a bar chart based on the importance attached to the attributes, and a general overview of the attribute levels of each drug class. An explanation of how to interpret the results is provided on top of the radar plot and the bar chart. The results can then be used to come to a shared decision (Figure 1-step 5).
We aimed to restrict the text of the DA to the B1 language level as advised in communication recommendations, and we considered the information in guidelines and tools for presenting the text, risks, pictograms, and figures.27–30
Pilot Study
Design and Participants
We conducted a qualitative study using semi-structured interviews among people with T2D who were 18 years or older, were or had ever been under pharmacological treatment for T2D, and were able to speak and read the Dutch language. Participants were recruited through various means: general practitioners (GPs) and flyers distributed in community pharmacies in the north of the Netherlands, messages on social media and on the Dutch website for patients with diabetes (www.diabetesfonds.nl), emails to patients who had participated in a previous study of the Department of Clinical Pharmacy and Pharmacology at the University Medical Center Groningen (UMCG) and had agreed to be contacted for future studies, and via-via. Participants received a link to a digital letter with information about eg, the study aim, duration, compensation for participation (ie, a voucher of 25€), and the consent form which included agreement with the use of the provided information and anonymized data (Supplementary Text 1). After providing informed consent, participants were contacted to schedule a face-to-face interview at the UMCG or their home depending on their preference. A waiver for full ethical approval was obtained from the medical ethical committee of the UMCG (METc UMCG) (reference number M22.29778), who evaluated this study as not being a clinical research with human subjects as defined in the Medical Research Involving Human Subjects Act (WMO). The study was performed in line with the principles of the Declaration of Helsinki.
Procedure
Before the interview, participants completed a short web-based questionnaire with questions about demographic characteristics (eg, gender, age, educational level), health (eg, diabetes duration, current and previous treatments used for diabetes), perceptions regarding shared-decision making (two statements adapted from Levinson et al 2005)31 and self-reported health literacy (three items adapted to the Dutch language from Chew et al 2004).32,33 The semi-structured interviews (Figure 2) were conducted in Dutch and took place between June 15 and November 9 2022. The duration of the interviews ranged from 50 to 90 minutes. Two to three researchers (SRM, FdV and/or STdV) were present at the interview; one (FdV or STdV) was in the lead and the others took notes, asked additional questions when relevant, and ran the R script to generate the results of the exercise (SRM). The DA was adapted in an iterative process in which changes to notified issues, comments, and suggestions were implemented. Interviews were conducted until we reached saturation in identified topics. An English translation of the final version of the leaflet and an example of the results of the elicitation exercise are available in Supplementary Text 2.
 |
Figure 2 Outline of the semi-structured interviews. Abbreviations: T2D, Type 2 diabetes; DA, Decision aid. |
Analyses
Descriptive analyses in R were conducted to assess the answers of the questionnaire completed before the interviews, the multiple-choice questions at the end of the leaflet, and the outcome of the preference elicitation exercise. The interviews were audio-recorded and transcribed verbatim by FdV or STdV. The texts were then coded using Atlas.ti (2002–2023–ATLAS.ti Scientific Software Development GmbH version 4.15.2–2023-04-26) by one researcher and a second researcher went through the coding to add any further possible codes. Further analyses of the codes were done using Microsoft Excel® 2010 (Microsoft Corp., Redmond, WA, USA). We applied thematic analysis using both a deductive and inductive approach. For the deductive approach, we used the alpha testing phase for patients from the model of the development process for DAs and, therefore, assessed comprehensibility and usability.34 Subsequently, the inductive approach was used for the identification of the themes within these concepts.
Results
Interviews were conducted among 15 people. Their median age was 64 years (interquartile range (IQR) 57–70), nine were women, and eight were higher educated. Most participants (n=9) had a self-reported T2D duration of more than ten years. The participants were in favour of shared-decision making and were health literate (Table 2). The multiple-choice questions at the end of the leaflet were answered correctly by all participants except two, who both answered one question incorrectly. For the ranking of the levels of the attribute “mode and frequency of administration” and “effect on body weight”, the most often chosen order was respectively weekly injection, daily tablet and daily injection, and decrease in body weight over a stable body weight (N=7) (Supplementary Table 2).
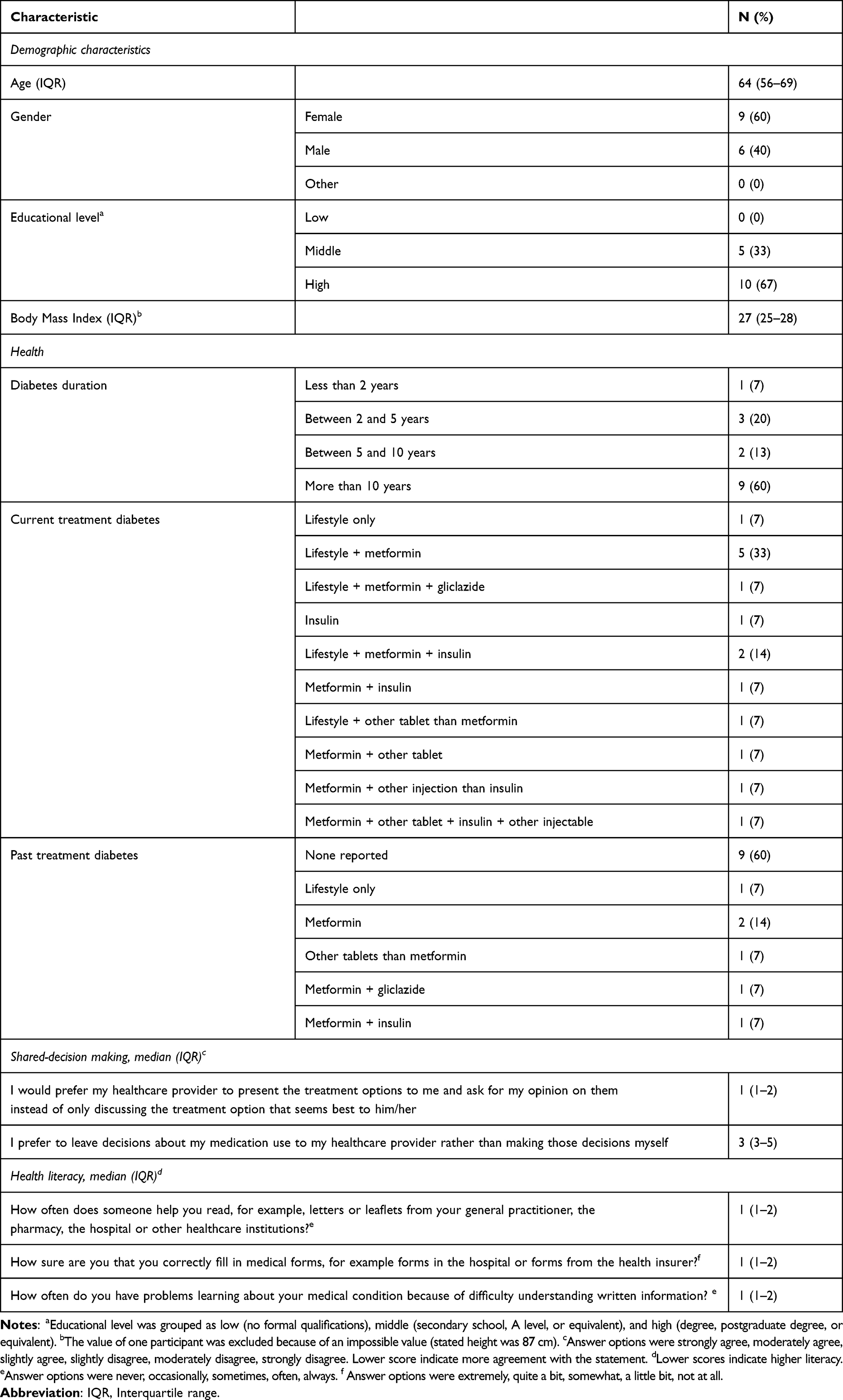 |
Table 2 Characteristics of the Participants (N=15) |
Based on the exercise in the DA, the risk of hypoglycaemia was most often the attribute to which patients attached the highest importance (n=5), followed by the risk of gastrointestinal complaints (N=4), and the effect on blood glucose level (N=3). None of the patients attached the highest importance to the effect on body weight (Figure 3A). The importance attached to the drug characteristics resulted in a GLP-1 agonist weekly injection being the preferred drug class for most participants (N=8) followed by an SGLT-2 inhibitor (N=5), and a GLP-1 daily tablet (N=2) (Figure 3B). Results at individual level are presented in Supplementary Figure 2.
 |
Figure 3 Outcome of the elicitation exercise with (A) the radar plot showing the scores by preferred attribute of each participant (with each color representing a different participant) and (B) an overview of the participants’ top 3 drug classes best fitting their preferences. Abbreviations: DPP-4, Dipeptidyl peptidase 4 inhibitor; GLP-1, Glucagon-like peptide-1 receptor agonist; INS, Insulin; SGLT-2, Sodium-glucose co-transporter-2; SU, Sulphonylurea. |
Comprehensibility
The concept of comprehensibility is used for two themes; participants’ comprehensibility of the DA and comprehension about how the participants completed the DA.
Participants’ Comprehensibility of the DA
The DA was generally considered clear and understandable, with an appropriate font size (leaflet: format A5, font Calibri, size 15.9, lines double spaced; exercise: font Open Sans, adaptable size), and well-explained information. Nevertheless, some difficulties were identified and mentioned by the participants, and suggestions were made to further improve the comprehensibility of the text, pictograms and figures, and formatting of the DA. Details are provided in Supplementary Information 1. An important finding was unclarity with the aim of the leaflet and the link between the leaflet and the exercise (Table 3; quote (Q)01). Some participants thought that the leaflet was providing general information about diabetes rather than more details about the drug characteristics used in the exercise (Table 3; Q02), or they identified the link between the leaflet and the exercise while reading the leaflet (Table 3; Q03). Unclarity with the aim of the leaflet may have contributed to a different interpretation of the levels of attributes (Table 3; Q04). Some participants also had difficulties interpreting the exercise (Table 3; Q05). After a short explanation, all participants were able to complete the exercise.
 |
Table 3 Quotes Supporting the Results |
Comprehension About How the Participants Completed the DA
During the interviews, more insights were obtained about how participants completed the DA. These are grouped into application to current/own situation, interpretation of risks, and rationale for the choices made in the exercise.
Application to Current/Own Situation
It was not always clear to participants that the DA was about drug attributes in general and aimed at eliciting participants’ preferences for drug attributes and drug classes other than metformin, instead of gathering knowledge about what the participant was currently doing or using (Table 3; Q06). The expected focus on metformin also resulted in discrepancies between the expectations and the content of the leaflet and the exercise (Table 3; Q07). A specific example of the application to the own situation and the focus on metformin was a participant who tried to relate the presented levels of the attribute “effect on blood glucose” to the participant’s own effect of metformin (Table 3; Q08). Also, a participant mentioned being content even towards the least favourable level of this attribute since the “low decrease” was better than the participant’s current glucose level (Table 3; Q09), and the level “intermediate decrease” was interpreted as a person’s own average glucose (HbA1c) level (Table 3; Q10).
Interpretation of Risks
The use of both text and pictograms influenced participants’ interpretation of risks (Table 3; Q11). Some unrealistic optimism was noticed with the interpretation of pictograms (Table 3; Q12-Q13). Moreover, the wording of the level “additional effect proven” of the attribute “additional effect on cardiovascular risk reduction” was in the participants’ opinion not in line with the risk reduction described, since the wording suggested to them a large effect (Table 3; Q14), whereas the actual additional effect on cardiovascular risk reduction from 10% to 8% was considered very low. In general, the interpretation of percentages might be difficult for patients (Table 3; Q15). A suggested easier way was to present risks of the individual participant instead of at a population level (Table 3; Q16).
Rationale for the Choices Made in the Exercise
Several themes were identified when participants’ reasoned out loud about the choices they had to make between drug attributes and attribute levels in the exercise (Table 4). The themes varied widely, from heredity to general beliefs and from quality of life to the interpretation of the presented risks. Most of the themes came up for several attributes, such as (the lack of) experience with the drug characteristics and the (lack of) other options to manage drug effects. Other themes came up for a specific attribute only, eg, (non)adherence and ease of use for mode of administration. Participants were aware that preferences could differ between people (Table 3; Q17).
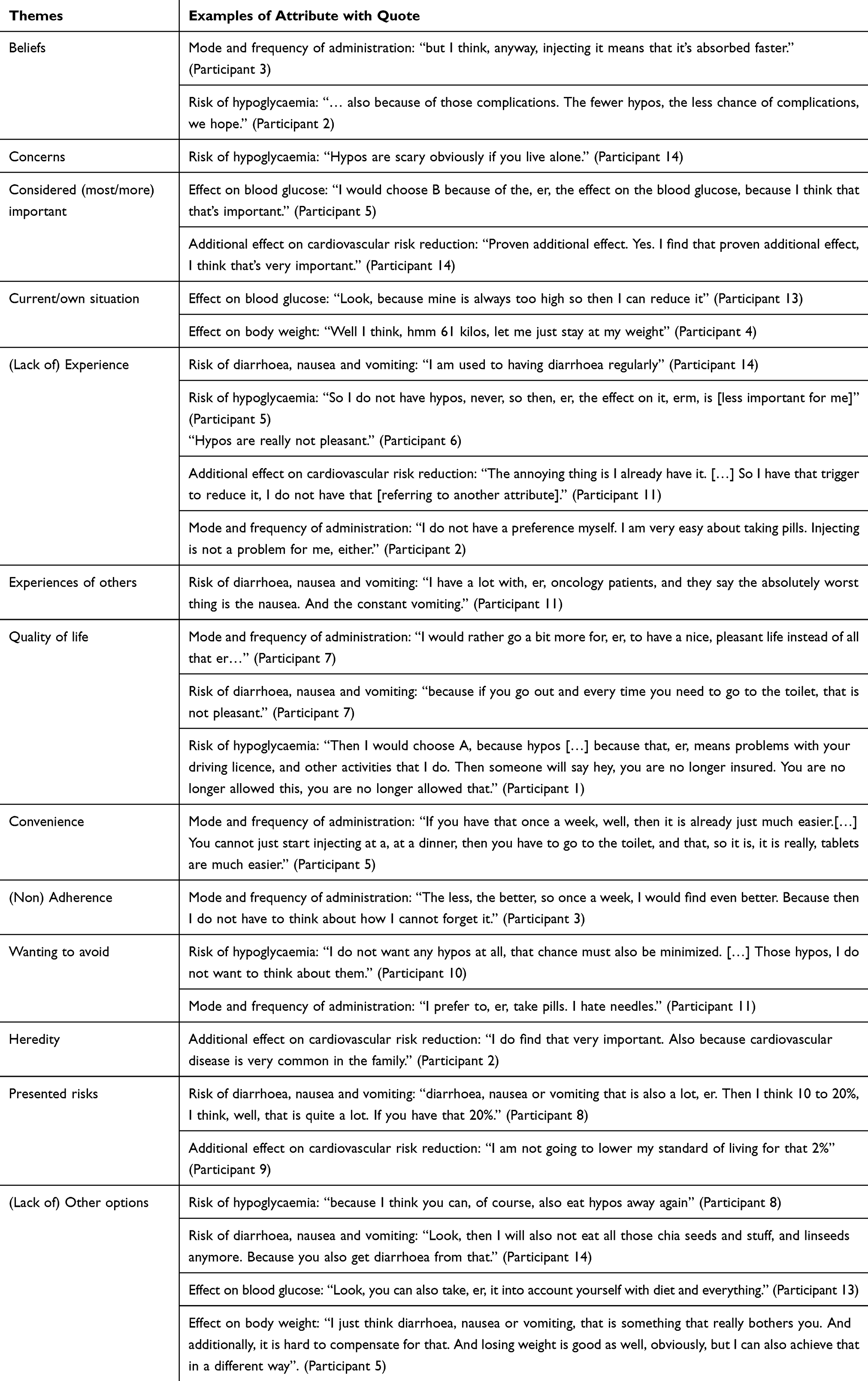 |
Table 4 Overview of Identified Themes in Participants’ Considerations for Evaluating the Various Drug Characteristics or Levels |
Usability
Regarding the usability of the DA, the following overarching themes were identified from the interviews: missing information, usability of the elicitation exercise, usefulness of the DA, shared-decision making, and where to use the DA.
Missing Information
During the interviews, participants mentioned several things that they felt were missing in the DA (eg, information about neuropathy, kidney function, hyperglycemia, costs [particularly the amount rather than whether or not a patient would need to pay for a drug]) but they also preferred a short leaflet. The current leaflet was considered to have an adequate length, and more information could be provided in different ways (Table 3; Q18). The use of QR codes to reliable sources of information was considered a useful possibility, although not all participants knew how to use QR codes and therefore preferred a web-link. It was also mentioned that the importance of lifestyle changes for the treatment of diabetes could be further emphasized. Another participant, however, mentioned that in general information about lifestyle as an option to treat diabetes makes you feel like you are doing insufficient yourself (Table 3; Q19).
With regard to the attribute “effect on body weight”, some participants were surprised that an increase in body weight was not among the effects. Providing more details of the currently included attributes was also considered relevant, such as the role of food for the attribute “mode and frequency of administration” (eg, any food restrictions) and details of the attribute “risk of diarrhoea, nausea and vomiting” (eg, information about transiency, or options to manage the ADR) (Table 3; Q20).
Participants expressed interest in receiving details on the effects per drug class. Although some participants were not interested in such details, an overview of the drug effects per drug class – which was initially not included in the DA – was added to the outcome of the exercise. Some participants, however, preferred to have the overview in the leaflet already instead of at the end of the DA. Many participants had never heard of all the different drug classes and it was questioned why metformin was not included as one of the possible preferred drugs.
Usability of the Elicitation Exercise
The length of the elicitation exercise was considered adequate (Table 3; Q21). Also, it was appreciated that the number of choice sets was mentioned beforehand (Table 3; Q22) and that each choice set was presented on a separate page (Table 3; Q23). Nevertheless, participants considered it difficult to choose between the two treatment options in the exercise (Figure 4). These difficulties were partly due to the forced choice nature of the exercise, ie, no possibility of skipping a question or choosing none of the alternatives. The forced choice of the ranking of the levels of the attributes “mode and frequency of administration” and “effect on body weight” before starting the exercise was also considered difficult for some people. Another reason for the experienced difficulties with making the choices in the exercise was participants’ willingness to answer consistently (Table 3; Q24). Similarly, some participants asked whether a choice set was repeated during the exercise, and a participant specifically mentioned that it is common in questionnaires that consistency is assessed with a control question. Participants also questioned the independence between some of the attributes when completing the exercise (Table 3; Q25-Q26). Furthermore, few participants initially selected the treatment that was not in line with their out loud stated preference. This was partly due to some initial difficulties in the wording or due to incorrect reading (Table 3; Q27).
 |
Figure 4 Examples of quotes illustrating the difficulties participants experienced when having to choose between the two treatment options in the elicitation exercise of the decision aid. |
The outcome of the exercise in terms of the importance attached to the drug effects was generally in line with participants’ expectations. One participant, however, was slightly surprised about the results (Table 3; Q28). Also, some participants expressed feelings of insecurity with the results shown in the radar plots (Table 3; Q29). The bar chart showing the order of the preferred drug classes was appreciated by the participants but there were discrepancies in their preferences towards the number of drug classes presented (ie, preferences for an overview of all drug classes versus an overview of only those drug classes most related to the preferences) (Table 3; Q30).
Usefulness of the DA
The difficulties in choosing between the alternatives and the sometimes mistakenly selected alternative in the exercise introduced the discussion about the added value of the exercise – and the DA in general – compared to an overview of the characteristics per drug class only. Some participants expected that an overview would be sufficient for them (Table 3; Q31). This might specifically apply to participants who are focusing (primarily) on one drug characteristic (Table 3; Q32). Other participants saw an added value of the exercise as it made them actively think (Table 3; Q33). When presenting an example of an overview with drug characteristics only, mentioned disadvantages were the large amount of information at once with still the requirement of making a decision (Table 3; Q34).
There was discussion about the added value of having a leaflet and an exercise in the DA. A participant mentioned that it would have been possible to complete the exercise without the leaflet but that the leaflet is a nice addition. It was suggested to add an overview of the characteristics of the drug classes at the end of the leaflet and offer the exercise as an optional next step for assessing the preferred drug class (Table 3; Q35).
Shared-Decision Making
Taking a patient’s perspective into account when making treatment decisions was generally considered appropriate and important. A participant mentioned being often involved in the decision but lacking knowledge. The DA would increase participants’ knowledge about possible treatment options and their characteristics, improving the control over their own treatment, which might result in being taken more seriously. The DA could also be an advantage for the HCP since it would facilitate the conversation with the patient, not only by identifying preferences, but also supporting the patient anamnesis and understanding the rationale of their preferences for a specific treatment (Table 3; Q36-Q37).
Nevertheless, a DA might not be necessary for everyone and could be relevant for specific patients, such as those who are modest and do not dare to ask for other treatment options or those who are not yet used to be involved in treatment decisions. Also, other patients might still prefer to leave the decision to the HCP (Table 3; Q38). Furthermore, it was mentioned that the DA should be used with help from a HCP since they have more knowledge and should always be involved in the decision-making. A concern raised was that not all included drug classes might fit an individual and that the HCP therefore might have reasons not to prescribe a drug class included in the DA (Table 3; Q39). Other remarks related to personalized medicine were that the effects of the drugs may differ between participants as well as within an individual over time (Table 3; Q40).
Regarding which HCP should be involved in the DA, participants had the impression that GPs will not have the time to use the DA. Discussing the DA with a nurse practitioner was therefore considered a better option, although this might not work with all nurse practitioners (Table 3; Q41).
Where to Use the DA
Participants mentioned that the preference for completing the DA at home or during a consultation with an HCP would depend, for instance, on whether people were recently diagnosed with diabetes or had little experience with computers. Differences in preferences between participants were indeed identified. Some preferred to complete the DA at home with the advantage of HCPs having more time to look at the outcome of the exercise (Table 3; Q42). Others mentioned that it would be possible to complete the DA at home although some instructions beforehand might be needed (Table 3; Q43) and that the results would still need to be discussed with a HCP (Table 3; Q44). Nonetheless, many participants preferred to complete the DA together with an HCP. Several advantages were mentioned for both parties; patients, eg, having the possibility to ask questions and discuss further with their HCP, and HCPs gathering knowledge about the dilemmas a patient faces while making the choices, information about the rationale of the choices, or the possibility to explain or clarify certain information to the individual patient (Table 3; Q45).
Discussion
This study assessed the comprehensibility and usability of a DA developed to elicit preferences of people with T2D towards drugs that may be prescribed in addition to or as a replacement of metformin. The DA was generally considered comprehensible and usable, however, concrete aspects regarding the text, pictograms and figures, and formatting to further improve the comprehensibility were identified. Also, it became clear that factors like the participants’ current/own situation, their interpretation of risks, and their rationale for the choices made in the exercise influence how people complete the DA. Finally, insights about missing information, the usability of the exercise, the usefulness of the DA, shared-decision making in general, and where to use the DA should be considered to further improve the usability of the DA.
With regard to the results of the elicitation exercise, the most relevant attribute was the risk of hypoglycaemic events, followed by gastrointestinal complaints. The importance of these two attributes has also been shown in previous patient preference studies.35–37 Nevertheless, it should be noted that participants in our study mentioned that to be fully capable of making choices in the elicitation exercise, essential information about the presented ADRs (eg, its severity or duration) was missing. Some of such information, however, is not systematically reported in public reports from clinical trials.38 The inclusion of patients’ perspectives in the set-up of clinical trials could be a way forward to ensure that all relevant information to patients is collected during the trials.
The effect of the drug on weight change was never elicited as the most important drug characteristic in our study. This result differs from previous studies showing that the effect on body weight is a highly influencing factor at the time of choosing among treatments for T2D.8,39 Some of the reasons of the discrepancy might be differences in the included population (ie, a mean body mass index of 27 kg/m2 in our study versus >30 kg/m2 in others), and differences in the included attribute levels (ie, weight reduction and no effect on weight versus the additional level of weight gain). The drug classes most frequently aligning with the participants’ preferences in our study were GLP-1 weekly injectables and SGLT-2 inhibitors. This is supporting the latest guideline recommendations, which position these drug classes as the first step at the time of treating people with T2D and high risk of cardiovascular diseases.2,5,6,40 However, currently in the Netherlands, whether SGLT-2 inhibitors and GLP-1 weekly injectables are reimbursed depend on patient factors such as body mass index (www.medicijnkosten.nl/). Reimbursement rules may, however, change over time (eg, when new evidence becomes available). This relates to the findings related to personalised medicine, as participants mentioned that not all drug classes might fit an individual patient and that drug effects may differ between individuals. In general, the result of the DA for an individual patient should not be seen as binding for the decision-making but rather as support in the conversation between the HCP and the patient to come to a shared decision.
A personalised approach also seems to be useful for the design and content of the DA, as there was variation in participants’ perspectives with regard to, eg, the use of figures and pictograms, and the content and quantity of information included. With regard to the latter, guidelines for the development of DAs recommend including information that is directly related to the aim of the DA and relevant to patients.34,41 Nevertheless, the leaflet in our DA also contains some additional information about diabetes in general. For some patients, this was indeed redundant information, which may have caused confusion about the aim of the DA, but others considered this a nice and useful introduction.
Differences about how participants interpreted the presented risks were noted. Most participants stated that they understood the information but it became clear that there were incorrect interpretations. Difficulties with the understandability and interpretation of risks have been shown previously, and it is influenced by factors such as an individual’s numeracy.42–44 This is in general concerning as patients have increasing access to information and are more often involved in treatment-related decisions, but do not necessarily have the skills to understand it,45 impairing the possibility of making proper informed decisions.
A specific case of an identified incorrect risk interpretation was unrealistic optimism. Unrealistic optimism is defined as the prediction of a personal outcome being more positive than the one suggested by objective data46 and has been previously shown in the context of T2D; for instance, a large number of people believe that other persons are at higher risk of developing diabetes than themselves.47,48 While this effect might be psychologically protective, it can also lead to accentuated risk behaviours.49 Our study suggests that unrealistic optimism might also influence patients’ preferences when interpreting risks. The influence of how risks are presented (eg, via text or pictograms) and the best way to present risks in a DA should be further assessed.
Besides the possible role of unrealistic optimism, our study showed that several other factors influenced the participants’ choices in the exercise, including experiences and beliefs. This is in line with previous studies assessing patient preferences as well as actual behavior showing, for instance, higher treatment acceptability when health is declining,50 differences in the preferences for the mode and frequency of administration based on experiences with injectable treatments,36 and an effect of beliefs about the necessity of medicines and expectations of ADRs on the use of medicines.51–53 These results show that preferences are influenced by factors that may change over time, making them dynamic. A discussion of patient preferences, possibly with the use of a DA, should therefore be considered at several moments during the treatment.
It was mentioned that the reasoning for the choices made in the exercise could be useful background information for the HCP. Nevertheless, participants had the impression that GPs might not have the time to use the DA or might not want to discus treatment options with patients. In the Netherlands, patients with T2D without complications are treated in primary care,54 where relative short consultation times are allocated.55 Suggestions were proposed by participants to optimise its implementation, such as the use of the DA only in those patients who struggle with eg, treatment satisfaction or adherence, the use of the DA with other HCPs than GPs (eg, diabetes nurses), or a further improved version of the DA that can be used by patients at home. Nevertheless, we found again differences between participants regarding their preferences about where to complete the DA.
Taken together, the observed heterogeneity among the participants pleads for a personalised approach in both the design and content of the DA and its use in clinical practice. While it is challenging to develop such DAs (eg, adjusting the formatting or quantity of information per person), the increasing progresses made in the field of artificial intelligence could be useful in their further development. Although the use of artificial intelligence is in its infancy,56 there are indications of its usefulness.57 Until such personalised tools are available, the use of DAs that provide patients with comprehensible information and that trigger the interaction between the patient and the HCP seems usable to elicit patient preferences in clinical practice.
Strengths and Limitations
A diverse sample of participants with regard to their gender and age was included in this study. Although we conducted interviews until saturation in identified topics, the sample size was small. The views of the participants might not represent those of the overall T2D population, as in our study participants considered shared-decision making highly important and self-reported health-literacy was high. Similarly, digital resources were part of this study (ie, a digital information letter and consent form) and are included in the DA (ie, a web-based preference elicitation exercise) which restricts participation to individuals who have access to and are comfortable using digital devices. Also, it should be noted that not all participants reasoned out-loud when making the choices in the exercise, or not necessarily did this for each of the choice sets. This implies that the themes identified for the rationale for the choices made in the exercise might not be exhaustive. Another limitation is that only patients were included in this study. Future studies are needed to assess the perspectives of HCPs.
A general limitation of preference elicitation exercises is that the elicited preferences can vary depending on the included attributes and attribute levels. To address this limitation, we aimed at including the most relevant attributes and accurate levels, basing the decisions on literature and the input of internists specialised in diabetes.2,21–25 Nonetheless, other possibly relevant attributes and attribute levels were mentioned by the participants (eg, costs), and should be considered in the further development of DAs. The inclusion of additional attributes and/or attribute levels will, however, increase the number of choice sets to be completed and its feasibility should, therefore, be examined. Finally, the DA distinguished treatment options by drug class instead of by specific drugs. Although there are some differences between drugs within a class,2 the use of all specific drugs would have substantially increased the number of choice sets to be completed, lowering the feasibility of the exercise.
Conclusion
In this study, we identified factors related to the comprehensibility and usability of a DA developed to elicit the preferences of a person with T2D towards drug classes to be prescribed in addition to or as a replacement of metformin. Aspects regarding the text, pictograms and figures, and the formatting were identified and applied to further improve the comprehensibility of the DA. Information about how participants relate the given information to their current/own situation, their interpretation of risks, and their rationale for the choices made in the exercise increased the comprehension of how people complete the DA. Regarding the usability, we obtained insights about relevant information being missing, about the usability of the exercise, the usefulness of the DA, shared-decision making in general, and about where to use the decision aid. Although this type of DA was considered a potentially useful tool to incorporate individual patient preferences in treatment decisions, the identified factors indicate that a personalized approach with regard to both the content and the formatting of the DA should be considered in its further development and/or implementation.
Acknowledgments
The authors would like to thank the people who participated in this study by being interviewed or collaborating in the recruitment of volunteers.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Financial support for this study was provided entirely by a grant from the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement number 754425. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Disclosure
All authors have declared no conflicts of interest relevant to the contents of this study.
References
1. Dal Canto E, Ceriello A, Ryden L, et al. Diabetes as a cardiovascular risk factor: an overview of global trends of macro and micro vascular complications. Eur J Prev Cardiol. 2019;26(2_suppl):25–32. doi:10.1177/2047487319878371
2. Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41(2):255–323. doi:10.1093/eurheartj/ehz486
3. Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2022;65(12):1925–1966. doi:10.1007/s00125-022-05787-2
4. ElSayed NA, Aleppo G, Aroda VR, et al. 6. glycemic targets: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S97–S110. doi:10.2337/dc23-S006
5. ElSayed NA, Aleppo G, Aroda VR, et al. 9. pharmacologic approaches to glycemic treatment: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S140–S157. doi:10.2337/dc23-S009
6. Barents E, Bilo H, Bouma M, et al. NHG-standaard. Diabetes Mellitus Type. 2009;2(M01): 160–191.
7. Chaudhury A, Duvoor C, Dendi VSR, et al. Clinical review of antidiabetic drugs: implications for type 2 diabetes mellitus management. Front Endocrinol. 2017;8. doi:10.3389/fendo.2017.00006
8. Purnell TS, Joy S, Little E, Bridges JF, Maruthur N. Patient preferences for noninsulin diabetes medications: a systematic review. Diabetes Care. 2014;37(7):2055–2062. doi:10.2337/dc13-2527
9. Seidu S, Cos X, Brunton S, et al. 2022 update to the position statement by primary care diabetes Europe: a disease state approach to the pharmacological management of type 2 diabetes in primary care. Prim Care Diabetes. 2022;16(2):223–244. doi:10.1016/j.pcd.2022.02.002
10. Saheb Kashaf M, McGill ET, Berger ZD. Shared decision-making and outcomes in type 2 diabetes: a systematic review and meta-analysis. Patient Educ Couns. 2017;100(12):2159–2171. doi:10.1016/j.pec.2017.06.030
11. Wang MJ, Hung LC, Lo YT. Glycemic control in type 2 diabetes: role of health literacy and shared decision-making. Patient Prefer Adherence. 2019;13:871–879. doi:10.2147/PPA.S202110
12. Losi S, Berra CCF, Fornengo R, Pitocco D, Biricolti G, Federici MO. The role of patient preferences in adherence to treatment in chronic disease: a narrative review. Drug Target Insights. 2021;15:13–20. doi:10.33393/dti.2021.2342
13. Will A. Drug and therapeutics bulletin editorial office. an introduction to patient decision aids. BMJ. 2013;347:f4147. doi:10.1136/bmj.f4147
14. Bailey RA, Pfeifer M, Shillington AC, et al. Effect of a patient decision aid (PDA) for type 2 diabetes on knowledge, decisional self-efficacy, and decisional conflict. BMC Health Serv Res. 2016;16:10. doi:10.1186/s12913-016-1262-4
15. Stacey D, Legare F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4). doi:10.1002/14651858.CD001431.pub5
16. Wieringa TH, Rodriguez-Gutierrez R, Spencer-Bonilla G, et al. Decision aids that facilitate elements of shared decision making in chronic illnesses: a systematic review. Syst Rev. 2019;8(1):121. doi:10.1186/s13643-019-1034-4
17. International patient decision aid standards (IPDAS) collaboration. Available from: http://ipdas.ohri.ca/what.html.
18. Karagiannis T, Andreadis P, Manolopoulos A, et al. Decision aids for people with type 2 diabetes mellitus: an effectiveness rapid review and meta-analysis. Diabet Med. 2019;36(5):557–568. doi:10.1111/dme.13939
19. Sims TJ, Boye KS, Robinson S, Kennedy-Martin T. Treatment-related attributes of diabetes therapies and how people with type 2 diabetes report their impact on indicators of medication-taking behaviors. Patient Prefer Adherence. 2022;16:1919–1939. doi:10.2147/PPA.S367046
20. Toroski M, Kebriaeezadeh A, Esteghamati A, Karyani AK, Abbasian H, Nikfar S. Patient and physician preferences for type 2 diabetes medications: a systematic review. J Diabetes Metab Disord. 2019;18(2):643–656. doi:10.1007/s40200-019-00449-4
21. Feingold KR. Oral and injectable (non-insulin) pharmacological agents for the treatment of type 2 diabetes. In: Feingold KR, Anawalt B, Blackman MR, editors.Endotext.South Dartmouth (MA);2000:1.
22. Tsapas A, Avgerinos I, Karagiannis T, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med. 2020;173(4):278–286. doi:10.7326/M20-0864
23. Alfayez OM, Al Yami MS, Alshibani M, et al. Network meta-analysis of nine large cardiovascular outcome trials of new antidiabetic drugs. Prim Care Diabetes. 2019;13(3):204–211. doi:10.1016/j.pcd.2019.01.003
24. Kramer CK, Ye C, Campbell S, Retnakaran R. Comparison of new glucose-lowering drugs on risk of heart failure in type 2 diabetes: a network meta-analysis. JACC Heart Fail. 2018;6(10):823–830. doi:10.1016/j.jchf.2018.05.021
25. Maruthur NM, Tseng E, Hutfless S, et al. Diabetes medications as monotherapy or metformin-based combination therapy for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med. 2016;164(11):740–751. doi:10.7326/M15-2650
26. van Valkenhoef G, Tervonen T. Entropy-optimal weight constraint elicitation with additive multi-attribute utility models. Omega-Int J Manag Sci. 2016;64:1–12. doi:10.1016/j.omega.2015.10.014
27. Council of Europe. The CEFR Levels. Available from: https://www.coe.int/en/web/common-european-framework-reference-languages/level-descriptions.
28. Dienst publiek en communicatie. Ministerie van Algemene Zaken. Themaonderzoek taalniveaus. [Public and communication service. Ministry of General Affairs. Theme research language levels]. Available from: https://www.communicatierijk.nl/documenten/publicaties/2021/01/21/themameting-taalniveaus.
29. Methodiek P – Begrijpelijke medische informatie in woord en beeld. [Methodology P – Understandable medical information in words and images]. Available from: https://www.pharos.nl/kennisbank/methodiek-begrijpelijke-medische-informatie-in-woord-en-beeld/.
30. College ter Beoordeling van Geneesmiddelen. Toolkit voor een begrijpelijke bijsluiter. [Dutch Medicines Evaluation Board. Toolkit for an understandable package leaflet]. Available from: https://www.cbg-meb.nl/onderwerpen/hv-patientenbijsluiter/toolkit-voor-een-begrijpelijke-bijsluiter.
31. Levinson W, Kao A, K A, Thisted R. Not all patients want to participate in decision making. a national study of public preferences. J GEN INTERN MED. 2005;20:531–535. doi:10.1111/j.1525-1497.2005.0088.x
32. Schlatmann FWM, Hofmeester I, van Balken MR. Met “Ik geef u onze folder mee” heeft een op de tien nóg geen idee. Tijdschrift voor Urologie. 2016;6(6–7):94–96. doi:10.1007/s13629-016-0131-6
33. Chew L, Bradley K, Boyko E. Brief questions to identify patients with inadequate health literacy. Fam Med. 2004;36(8):588–594.
34. Coulter A, Stilwell D, Kryworuchko J, Mullen PD, Ng CJ, van der Weijden T. A systematic development process for patient decision aids. BMC Med Inform Decis Mak. 2013;13 Suppl 2(Suppl 2):S2. doi:10.1186/1472-6947-13-S2-S2
35. Roldan Munoz S, Postmus D, de Vries ST, et al. Differences in Importance attached to drug effects between patients with type 2 diabetes from the Netherlands and Turkey: a preference study. Front Pharmacol. 2020;11:617409. doi:10.3389/fphar.2020.617409
36. Mansfield C, Sikirica MV, Pugh A, et al. Patient preferences for attributes of type 2 diabetes mellitus medications in Germany and Spain: an online discrete-choice experiment survey. Diabetes Ther. 2017;8(6):1365–1378. doi:10.1007/s13300-017-0326-8
37. Boland BS, Edelman SV, Wolosin JD. Gastrointestinal complications of diabetes. Endocrinol Metab Clin North Am. 2013;42(4):809–832. doi:10.1016/j.ecl.2013.07.006
38. European Medicines Agency. European public assessment reports: background and context. Available from: https://www.ema.europa.eu/en/medicines/what-we-publish-when/european-public-assessment-reports-background-context.
39. Mohamed AF, Zhang J, Johnson FR, et al. Avoidance of weight gain is important for oral type 2 diabetes treatments in Sweden and Germany: patient preferences. Diabetes Metab. 2013;39(5):397–403. doi:10.1016/j.diabet.2013.06.001
40. Buse JB, Wexler DJ, Tsapas A, et al. 2019 update to: management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2020;43(2):487–493. doi:10.2337/dci19-0066
41. NICE. NICE Decision Aids: Process Guide. NICE; 2018.
42. Naik G, Ahmed H, Edwards AG. Communicating risk to patients and the public. Br J Gen Pract. 2012;62(597):213–216. doi:10.3399/bjgp12X636236
43. Fajardo MA, Balthazaar G, Zalums A, Trevena L, Bonner C. Favourable understandability, but poor actionability: an evaluation of online type 2 diabetes risk calculators. Patient Educ Couns. 2019;102(3):467–473. doi:10.1016/j.pec.2018.10.014
44. Sinayev A, Peters E, Tusler M, Fraenkel L. Presenting numeric information with percentages and descriptive risk labels: a randomized trial. Med Decis Making. 2015;35(8):937–947. doi:10.1177/0272989X15584922
45. Kreps GL. Promoting patient comprehension of relevant health information. Isr J Health Policy Res. 2018;7(1):56. doi:10.1186/s13584-018-0250-z
46. Shepperd JA, Waters E, Weinstein ND, Klein WM. A primer on unrealistic optimism. Curr Dir Psychol Sci. 2015;24(3):232–237. doi:10.1177/0963721414568341
47. Reyes-Velazquez W, Sealey-Potts C. Unrealistic optimism, sex, and risk perception of type 2 diabetes onset: implications for education programs. Diabetes Spectr. 2015;28(1):5–9. doi:10.2337/diaspect.28.1.5
48. Gassen J, Nowak TJ, Henderson AD, Weaver SP, Baker EJ, Muehlenbein MP. Unrealistic optimism and risk for COVID-19 disease. Front Psychol. 2021;12:647461. doi:10.3389/fpsyg.2021.647461
49. Salgado S, Berntsen D. ”It won’t happen to us”: unrealistic optimism affects COVID-19 risk assessments and attitudes regarding protective behaviour. J Appl Res Mem Cogn. 2021;10(3):368–380. doi:10.1016/j.jarmac.2021.07.006
50. Fried T, Byers A, Gallo W, et al. Prospective study of health status preferences and changes in preferences over time in older adults. Arch Intern Med. 2006;166:890–895. doi:10.1001/archinte.166.8.890
51. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/s0022-3999(99)00057-4
52. Colloca L, Miller FG. The nocebo effect and its relevance for clinical practice. Psychosom Med. 2011;73(7):598–603. doi:10.1097/PSY.0b013e3182294a50
53. Smith LE, Webster RK, Rubin GJ. A systematic review of factors associated with side-effect expectations from medical interventions. Health Expect. 2020;23(4):731–758. doi:10.1111/hex.13059
54. Campmans-Kuijpers MJ, Lemmens LC, Baan CA, et al. Defining and improving quality management in Dutch diabetes care groups and outpatient clinics: design of the study. BMC Health Serv Res. 2013;13:129. doi:10.1186/1472-6963-13-129
55. Schafer WLA, van den Berg MJ, Groenewegen PP. The association between the workload of general practitioners and patient experiences with care: results of a cross-sectional study in 33 countries. Hum Resour Health. 2020;18(1):76. doi:10.1186/s12960-020-00520-9
56. Abbasgholizadeh Rahimi S, Cwintal M, Huang Y, et al. Application of artificial intelligence in shared decision making: scoping review. JMIR Med Inform. 2022;10(8):e36199. doi:10.2196/36199
57. Jayakumar P, Moore MG, Furlough KA, et al. Comparison of an artificial intelligence-enabled patient decision aid vs educational material on decision quality, shared decision-making, patient experience, and functional outcomes in adults with knee osteoarthritis: a randomized clinical trial. JAMA Network Open. 2021;4(2):e2037107. doi:10.1001/jamanetworkopen.2020.37107
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Pattern of Dyslipidemia and Its Associated Factors Among Patients with Type 2 Diabetes Mellitus in Jordan: A Cross-Sectional Study
Al Quran TM, Bataineh ZA, Al-Mistarehi AH, Zein Alaabdin AM, Allan H, Al Qura'an A, Weshah SM, Alanazi AA, Khader YS
International Journal of General Medicine 2022, 15:7669-7683
Published Date: 4 October 2022
Decreased Serum Osteocalcin is an Independent Risk Factor for Metabolic Dysfunction-Associated Fatty Liver Disease in Type 2 Diabetes
Wang YJ, Jin CH, Ke JF, Wang JW, Ma YL, Lu JX, Li MF, Li LX
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3717-3728
Published Date: 29 November 2022
Diabetes Distress and Illness Perceptions in Tunisian Type 2 Diabetes Patients
Masmoudi R, Hadj Kacem F, Bouattour M, Guermazi F, Sellami R, Feki I, Mnif M, Masmoudi J, Baati I, Abid M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3547-3556
Published Date: 6 November 2023
Age at Diagnosis of Diabetes in Young Men is Associated with Albuminuria
Zhang Q, Cheng L, Li B, Lu Y, Yang S, Wu Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1543-1549
Published Date: 4 April 2024
Support Vector Machine for Stratification of Cognitive Impairment Using 3D T1WI in Patients with Type 2 Diabetes Mellitus
Xu Z, Zhao L, Yin L, Cao M, Liu Y, Gu F, Liu X, Zhang G
Diabetes, Metabolic Syndrome and Obesity 2025, 18:435-451
Published Date: 13 February 2025