")
Back to Journals » Infection and Drug Resistance » Volume 18
Phenotyping Nontuberculous Mycobacterial Lung Disease: Comparative Analysis of Clinical and Imaging Features in a TB-Endemic Setting
Authors Feng Y, Guo J, Luo S, Zhang Z
Received 20 March 2025
Accepted for publication 4 July 2025
Published 14 July 2025 Volume 2025:18 Pages 3527—3534
DOI https://doi.org/10.2147/IDR.S529466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor M. Mora-Montes
Yinping Feng, Jing Guo, Shuirong Luo, Zunjing Zhang
Department of Tuberculosis, Lishui Hospital of Traditional Chinese Medicine Affiliated to Zhejiang University of Traditional Chinese Medicine, Lishui Tuberculosis Clinical Medical Research Center, Lishui, Zhejiang, People’s Republic of China
Correspondence: Zunjing Zhang, Email [email protected]
Objective: To systematically analyze clinical features and imaging characteristics of nontuberculous mycobacterial pulmonary disease (NTM-PD) patients in a tuberculosis specialty setting, establishing diagnostic and management references.
Methods: We conducted a retrospective analysis of 204 NTM-PD cases admitted to our tuberculosis department from January 2018 to December 2023, evaluating clinical manifestations, mycobacterial speciation, and radiological patterns.
Results: The cohort comprised 118 males and 86 females (mean age 65.34 ± 13.23 years), predominantly rural residents (63.24%). Common comorbidities included previous pulmonary tuberculosis (58.33%), chronic obstructive pulmonary disease (41.67%), and bronchiectasis (36.76%). Primary clinical manifestations were productive cough (78.92%), dyspnea (25.98%), and hemoptysis (24.5%). Mycobacterium avium complex (MAC) accounted for 59.80% of isolates, followed by Mycobacterium abscessus (MABS) (16.67%). Radiological analysis revealed right upper lobe (86.54%) and left upper lobe (82.69%) predominance, with multilobar involvement (≥ 3 lobes) in 73.08% cases. Characteristic imaging features included nodular opacities, pleural thickening (63.46%), cavitary lesions (54.81%), and bronchiectasis (51.92%).
Conclusion: NTM-PD primarily affects elderly populations with chronic respiratory symptoms, demonstrating extensive pulmonary involvement across multiple lobes. The disease exhibits characteristic radiological triad of nodules, cavitations, and bronchiectasis, with MAC being the predominant pathogen in this cohort.
Keywords: nontuberculous mycobacteria, pulmonary infection, chronic respiratory disease, mycobacterial diagnosis, chest imaging
Introduction
Non-tuberculous mycobacteria (NTM) comprise a heterogeneous group of acid-fast bacilli distinct from Mycobacterium tuberculosis complex and Mycobacterium leprae. These environmentally ubiquitous organisms include over 190 identified species, predominantly existing as environmental saprophytes or transient colonizers, with only a subset demonstrating pathogenic potential in humans.1 While historically regarded as less virulent than tuberculosis, emerging evidence highlights specific NTM species capable of causing rapidly progressive, life-threatening infections with substantial mortality risks.2 Clinically, NTM manifests most frequently as pulmonary disease (NTM-PD), though extrapulmonary involvement—including lymphadenitis, cutaneous lesions, and osteoarticular infections—constitutes approximately 30% of reported cases.3 Despite increasing recognition, NTM-PD epidemiology remains poorly characterized due to diagnostic complexities, contributing to diagnostic delays, therapeutic resistance, and intricate treatment protocols that significantly compromise patient prognoses. This study systematically examines clinical and radiological profiles of NTM-PD cases at a tertiary referral center, aiming to enhance diagnostic precision and inform evidence-based management strategies.
Materials and Methods
Study Design and Population
This retrospective cohort study analyzed clinical records of patients diagnosed with NTM-PD at our tertiary referral center from January 2018 to December 2023. Collected data included demographic characteristics (age, sex, rural/urban residence, BMI), comorbidities, clinical manifestations, and radiological findings. Two radiologists independently reviewed CT images; discrepancies were resolved by a third radiologist. Ethical approval was granted by the Institutional Review Board of Lishui Hospital of Traditional Chinese Medicine (Approval No. LW-2024021), with waived informed consent due to retrospective anonymized data analysis. The study was conducted at LishuiTCM Hospital (Zhejiang, China), a tertiary TB referral center serving rural/suburban populations.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Confirmed NTM-PD diagnosis per 2020 ATS/ERS/ESCMID/IDSA guidelines;1 (2) Complete clinical documentation including microbiological confirmation and thoracic CT imaging. Exclusion criteria: (1) Concurrent active pulmonary tuberculosis; (2) Incomplete clinical records (>20% data missing); (3) Immunocompromised status (HIV positivity or solid-organ transplantation).
Records with >20% missing core variables (CT findings, speciation) were excluded. All eligible NTM-PD cases were included via total sampling.
Statistical Analysis
Data processing utilized SPSS 26.0 (IBM Corp.) with two-tailed significance testing. Categorical variables were expressed as frequencies (%) and analyzed by Chi-square test or Fisher’s exact tests. Normality-tested continuous variables (Shapiro–Wilk, P>0.05) were reported as mean±SD and compared via independent t-tests. Nonparametric data were presented as median (IQR) and evaluated using Mann–Whitney U-tests. A threshold of P<0.05 defined statistical significance.
Results
Patient Age and Gender Distribution
The study cohort comprised 204 patients (mean age 65.34 ± 13.23 years) with bimodal age distribution, peaking in the 50–80 year range (72.1% of cases). A male predominance was observed (male: female ratio 1.37:1, 118 vs 86), though gender distribution did not reach statistical significance (P>0.05) (Figure 1).
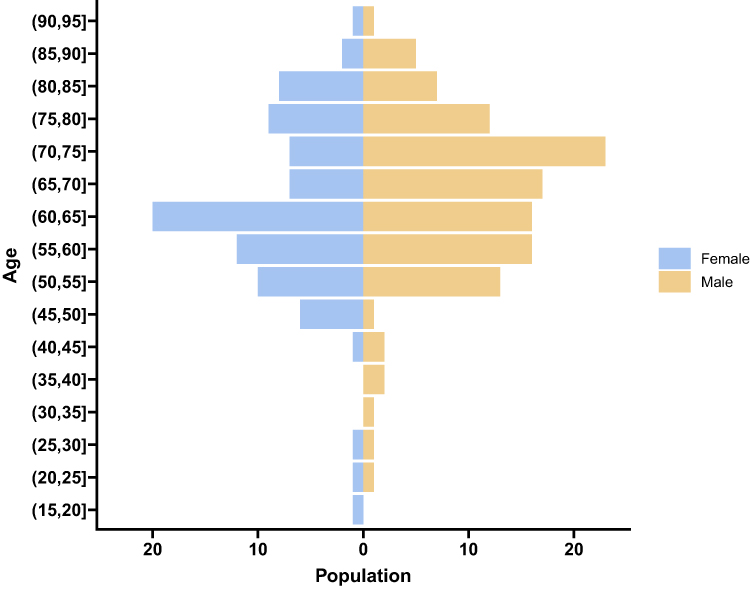 |
Figure 1 Patient age and gender distribution. |
Comparison of Clinical General Information for Patients of Different Genders
Among the total of 204 patients included in the study, the majority (129 individuals, 63.24%) were found to reside in rural areas. Analysis of the data showed no significant difference in body mass index between male and female patients (P>0.05). However, there was a statistically significant difference in the rates of smoking and alcohol consumption, with a higher prevalence among male patients compared to female patients (P<0.05). Furthermore, the historical data revealed a higher incidence of bronchiectasis in women and diabetes in men, both of which displayed significant disparities (P<0.05) (Table 1).
 |
Table 1 Comparison of Clinical General Information for Patients of Different Genders |
Clinical Manifestation
Out of the 204 patients studied, the predominant clinical symptoms reported were cough and phlegm in 161 cases (78.92%). Following this, dyspnea was observed in 53 cases (25.98%), hemoptysis in 50 cases (24.51%), asymptomatic presentation in 34 cases (16.67%), and fatigue in 10 cases (4.90%) (Table 2).
 |
Table 2 Clinical Manifestation |
Distribution of NTM Pathogens
In the study involving 204 patients, there is one case of non tuberculous mycobacteria whose specific strain cannot be identified. The most commonly identified bacterial group was Mycobacterium avium complex, found in 122 cases (59.80%). Following this, there were 34 cases (16.67%) of Mycobacterium abscess, 15 cases (7.35%) of M. malmoense, 10 cases (4.90%) of M. kansasii, 8 cases (3.92%) of M. gordonae, 6 cases (2.94%) of M. scrofulaceum, 3 cases (1.47%) of M. fortuitum, 3 cases (1.47%) of M. terrae, and 2 cases (0.98%) of M. gilvum (Table 3).
 |
Table 3 Distribution of NTM Pathogens |
Analysis of Imaging Characteristics of MAC and MABS Pulmonary Disease
The chest imaging findings revealed the presence of lesions in a total of 133 cases (86.54%) in the upper right lobe, 82 cases (52.56%) in the middle right lobe, 57 cases (36.54%) in the lower right lobe, 129 cases (82.69%) in the upper left lobe, and 77 cases (49.36%) in the lower left lobe. Analysis showed no statistically significant difference (P>0.05) in the number of lesions involving three or more lobes. Notably, 98 cases (80.33%) of MAC pulmonary disease exhibited a higher number of lesions compared to 16 cases (47.06%) of MABS pulmonary disease, indicating a significant difference (P<0.05). Furthermore, the evaluation of lesion morphology did not demonstrate significant variations in terms of nodules, bronchiectasis, lymphnode enlargement, and calcification. However, there was a higher prevalence of pleural thickening in MAC pulmonary disease, with 65 cases (53.28%) compared to only 9 cases (26.47%) in MABS pulmonary disease. Additionally, cavities MAC pulmonary disease was more frequently observed in 76 cases (62.30%) compared to 3 cases (8.82%) in MABS pulmonary disease, highlighting statistically significant differences (P<0.05) (Table 4).
 |
Table 4 Analysis of Imaging Characteristics of MAC and MABS Pulmonary Disease |
Discussion
Non-tuberculous mycobacteria (NTM), as opportunistic pathogens prevalent in the environment, demonstrate global ubiquity.4 Infections primarily occur through respiratory inhalation or direct environmental exposure. Meta-analyses of culture samples reveal a worldwide annual increase in NTM disease incidence at 4.1 cases per 100,000 population.5 This upward trend stems not only from enhanced clinical recognition and diagnostic advancements but also reflects the growing population of immunocompromised hosts and widespread environmental colonization of NTM.6 Epidemiological data show significant geographical variations: The United States reports annual NTM pulmonary disease (NTM-PD) incidence rates of 1–15 cases per 100,000 person-years,7 while South Korea’s prevalence surged from 9.4/100,000 in 2009 to 36.1/100,000 in 2016.8 Germany witnessed an increase from 2.3/100,000 in 2009 to 3.3/100,000 in 2014.9 Notably, high-prevalence regions in North America, Japan, and Europe contrast with lower incidence areas, a disparity attributable to complex interactions between genetic predisposition, environmental factors, and healthcare infrastructure.10 Pulmonary manifestations dominate NTM infections (≈90%), with rare extrapulmonary involvement in cerebrospinal fluid, synovial fluid, and musculoskeletal systems.11 Global NTM-PD incidence ranges 1–5/100,000.3 Distinct from tuberculosis’ predilection for young healthy individuals, NTM-PD predominantly affects elderly populations in communal living settings, frequently comorbid with bronchiectasis and chronic obstructive pulmonary disease.12,13 This study also revealed that the average age of onset for NTM-PD is 65.34 ± 13.23 years, with the majority affecting elderly individuals living in communal settings. Older individuals are at an increased risk of NTM infection, possibly due to age-related changes in the immune system and a higher prevalence of underlying diseases. Age-related decline in immune function can lower the body’s ability to resist NTM bacteria, making older individuals more vulnerable to these infections.14 Smoking also heightens the risk of NTM-PD, particularly in those with pre-existing lung conditions. Smoking damages the respiratory epithelium, compromises the lungs’ natural defense mechanisms, and creates a favorable environment for NTM colonization and infection.15 Patients with chronic lung diseases, such as bronchiectasis, COPD, or cystic fibrosis, are particularly susceptible to pulmonary NTM infection. These lung conditions provide a conducive environment for NTM bacterial growth, leading to chronic and potentially severe respiratory infections.16 NTM-PD itself can result in fibrous bronchiectasis, characterized by abnormal bronchiectasis and the formation of pulmonary nodules, leading to persistent respiratory symptoms.17 Diabetes can impair cell-mediated immune responses, increasing the likelihood of NTM-PD.12
The clinical presentations of NTM-PD are diverse, with respiratory symptoms being the most common. Some cases may be asymptomatic and only identified through physical examinations. Research indicates that cough are the primary symptoms of NTM-PD, followed by breathlessness and coughing up blood.18,19 Among the 204 individuals studied, the most prevalent symptoms were cough and phlegm in 161 cases (78.92%), dyspnea in 53 cases (25.98%), and hemoptysis in 50 cases (24.51%). The predominant bacteria responsible for NTM-PD was the MAC in 122 cases (59.80%), followed by MABS in 34 cases (16.67%). In a comprehensive nationwide research conducted in Japan, it was found that MAC emerged as the most prevalent pathogen.20 Similarly, a study focusing on NTM-PD in China revealed that MAC accounted for the majority (52.6%), however, a distinct pattern was observed in the northwest region, where M. kansasii stood out as the dominant species, highlighting regional variations.21 In South Korea, a study showcased the distribution of NTM as follows: MAC> MABS > M. malmoense.22 In the United States, approximately 80% of NTM-PD cases are caused by the MAC.23 In the UK, the proportion is 43%, while in Asia, the MAC proportion stands at 56%, followed by MABS at 35%.24 Additionally, an important NTM species to consider is Mycobacterium kansasensis, which is anticipated to be widespread in Europe and certain areas of North America, this species exhibits clinical and imaging features that closely mimic tuberculosis, presenting a diagnostic challenge.25 MABS is another notable NTM species that presents a substantial hurdle in treatment due to its resistance to multiple drugs. This resistance can result in a range of infections including lung infections, skin and soft tissue infections, as well as disseminated diseases.26
The imaging manifestations of NTM-PD are important for the diagnosis, treatment, and prognosis of the disease, as well as for research purposes. While the imaging of NTM-PD may bear similarities to tuberculosis, there are also distinct differences.27 The imaging manifestations of NTM-PD are varied and lack specificity, including nodules, patches, and cavities, with lesions often spanning multiple lung lobes. This study reveals that regardless of the bacterial strain, nodular manifestations are the most common in NTM-PD (84.62%), followed by pleural thickening, cavities, and bronchiectasis. The manifestation of NTM-PD as bronchiectasis is prevalent, and the relationship between NTM-PD and bronchiectasis, as a cause or consequence, remains unclear and can often coexist.28 NTM infection can also lead to cavities, characterized by the formation of cavities in the lung parenchyma, which may result in hemoptysis, while another subset of patients may develop fibrocavitary diseases.29 The presence of cavities indicates disease progression, and NTM-PD patients with cavity lesions necessitate long-term and intensified treatment. Evaluating the location, size, and quantity of cavities is crucial in determining the disease prognosis and the potential need for surgical intervention.30 High-resolution computed tomography (HRCT) examination results play a critical role in the diagnosis of NTM-PD, providing detailed images of the lung structure and aiding in the identification of characteristic abnormalities associated with NTM infection. It is generally believed that manifestations such as bronchiectasis, cavities, and nodules should raise suspicion of NTM infection.31,32 Presently, AI machine learning can be employed in the early differential diagnosis of pulmonary tuberculosis and NTM-PD imaging, coupled with T-SPOT detection to significantly enhance accuracy, CT images of pulmonary tuberculosis typically exhibit lung consolidation, thick-walled cavities, and pleural effusion, whereas NTM-PD often presents with bronchiectasis, cystic changes, and thin-walled cavities.33 Slow-growing MAC lung disease is more commonly observed on imaging due to its low virulence, protracted course, and the presence of cavities and pleural thickening.
Our other study shows that, bronchiectasis exacerbation occurring at least twice a year, involvement of three or more lung lobes with bronchiectasis, hypoalbuminemia, and the NLR index (= Neutrophils (*109/L)/Lymphocytes (*109/L)) were significant risk factors for NTM-PD in individuals with bronchiectasis.34 The aim of this study is to examine the clinical features and imaging findings of individuals diagnosed with at a specialized tuberculosis hospital, it has better novelty.
Conclusions
In summary, the clinical and imaging presentations of NTM-PD are varied, lack specificity in clinical practice, and are generally considered to be more common in the elderly. Patients with a history of smoking, pulmonary tuberculosis, bronchiectasis, COPD, and diabetes are at a more prevalent. The main clinical symptoms include cough and sputum production, followed by hemoptysis and dyspnea, although some patients may be asymptomatic. Upon radiological assessment, lesions are typically found to be widely distributed, often involving more than three lung lobes, with nodules, pleural thickening, cavities, and bronchiectasis observed. The imaging findings are associated with the specific bacterial species involved. Future research efforts should focus on exploring additional laboratory testing markers, as well as investigating drug treatment options and resistance patterns, to enhance our understanding of clinical management practices.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Informed Consent Statement
Written informed consent was obtained from all participants.
Institutional Review Board Statement
This study was conducted with approval from the Ethics Committee of Lishui Hospital of Traditional Chi- nese Medicine. This study was conducted in accordance with the declaration of Helsinki.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Zhejiang Province Elderly Pulmonary Tuberculosis Diagnosis and Treatment Traditional Chinese Medicine Multidisciplinary Interdisciplinary Innovation Team. Key Medical Disciplines in Lishui City.
Disclosure
The authors declare no competing interests.
References
1. Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J. 2020;56(1):2000535. doi:10.1183/13993003.00535-2020
2. Wassilew N, Hoffmann H, Andrejak C, et al. Pulmonary disease caused by non-tuberculous mycobacteria[J]. Respiration. 2016;91(5):386–402. doi:10.1159/000445906
3. Sharma SK, Upadhyay V. Epidemiology, diagnosis & treatment of non-tuberculous mycobacterial diseases. Indian J Med Res. 2020;152(3):185–226. doi:10.4103/ijmr.IJMR_902_20
4. Falkinham JO. Environmental sources of nontuberculous mycobacteria. Clin Chest Med. 2015;36(1):35–41. doi:10.1016/j.ccm.2014.10.003
5. Dahl VN, Mølhave M, Fløe A, et al. Global trends of pulmonary infections with nontuberculous mycobacteria: a systematic review. Int J Infect Dis. 2022;125:120–131. doi:10.1016/j.ijid.2022.10.013
6. Shah NM, Davidson JA, Anderson LF, et al. Pulmonary mycobacterium avium-intracellulare is the main driver of the rise in non-tuberculous mycobacteria incidence in England, Wales and Northern Ireland, 2007-2012. BMC. Infect Dis. 2016;16:195.
7. Kendall BA, Winthrop KL. Update on the epidemiology of pulmonary nontuberculous mycobacterial infections. Seminars in Respiratory and Critical Care Medicine. 2013;34(01):87–94. doi:10.1055/s-0033-1333567
8. Jeon D. Infection source and epidemiology of nontuberculous mycobacterial lung disease. Tuberc Respir Dis. 2019;82(2):94–101. doi:10.4046/trd.2018.0026
9. Ringshausen FC, Wagner D, de Roux A, et al. Prevalence of nontuberculous mycobacterial pulmonary disease, Germany, 2009-2014. Emerg Infect Dis. 2016;22(6):1102–1105. doi:10.3201/eid2206.151642
10. Maurya AK, Nag VL, Kant S, et al. Prevalence of nontuberculous mycobacteria among extrapulmonary tuberculosis cases in tertiary care centers in Northern India. Biomed Res Int. 2015;2015:465403. doi:10.1155/2015/465403
11. Smith GS, Ghio AJ, Stout JE, et al. Epidemiology of nontuberculous mycobacteria isolations among central North Carolina residents, 2006-2010. J Infect. 2016;72(6):678–686. doi:10.1016/j.jinf.2016.03.008
12. Henkle E, Winthrop KL. Nontuberculous mycobacteria infections in immunosuppressed hosts. Clin Chest Med. 2015;36(1):91–99. doi:10.1016/j.ccm.2014.11.002
13. Rawson TM, Abbara A, Kranzer K, et al. Factors which influence treatment initiation for pulmonary non-tuberculous mycobacterium infection in HIV negative patients; a multicentre observational study. Respir Med. 2016;120:101–108. doi:10.1016/j.rmed.2016.10.001
14. Li Y, Wang C, Peng M. Aging immune system and its correlation with liability to severe lung complications. Front Public Health. 2021;9:735151. doi:10.3389/fpubh.2021.735151
15. Jiang C, Chen Q, Xie M. Smoking increases the risk of infectious diseases: a narrative review. Tob Induc Dis. 2020;18(July):60. doi:10.18332/tid/123845
16. Wyrostkiewicz D, Opoka L, Filipczak D, et al. Nontuberculous mycobacterial lung disease in the patients with cystic Fibrosis-A challenging diagnostic problem. Diagnostics. 2022;12(7):1514. doi:10.3390/diagnostics12071514
17. Rao R, Sheshadri S, Patil N, et al. Lady Windermere syndrome: a very rare entity in Indian medical scenario. J Clin Diagn Res. 2016;10(1):OD01–2. doi:10.7860/JCDR/2016/17540.7024
18. Liu Q, Du J, An H, et al. Clinical characteristics of patients with non-tuberculous mycobacterial pulmonary disease: a seven-year follow-up study conducted in a certain tertiary hospital in Beijing. Front Cell Infect Microbiol. 2023;13:1205225. doi:10.3389/fcimb.2023.1205225
19. Hu C, Huang L, Cai M, et al. Characterization of non-tuberculous mycobacterial pulmonary disease in Nanjing district of China. BMC Infect Dis. 2019;19(1):764. doi:10.1186/s12879-019-4412-6
20. Morimoto K, Hasegawa N, Izumi K, et al. A laboratory-based analysis of nontuberculous mycobacterial lung disease in Japan from 2012 to 2013. Ann Am Thorac Soc. 2017;14(1):49–56. doi:10.1513/AnnalsATS.201607-573OC
21. Tan Y, Deng Y, Yan X, et al. Nontuberculous mycobacterial pulmonary disease and associated risk factors in China: a prospective surveillance study. J Infect. 2021;83(1):46–53. doi:10.1016/j.jinf.2021.05.019
22. Kim YJ, Kim S, Ham H, et al. Trend of nontuberculous mycobacteria species and minimal inhibitory concentration in a referral laboratory in Korea from 2013 to 2019. J Infect Public Health. 2024;17(2):212–216. doi:10.1016/j.jiph.2023.11.028
23. Prevots DR, Shaw PA, Strickland D, et al. Nontuberculous mycobacterial lung disease prevalence at four integrated health care delivery systems[J]. Am J Respir Crit Care Med. 2010;182(7):970–976. doi:10.1164/rccm.201002-0310OC
24. Simons S, Van Ingen J, Hsueh PR, et al. Nontuberculous mycobacteria in respiratory tract infections, Eastern Asia[J]. Emerg Infecti Dis. 2011;17(3):343–349. doi:10.3201/eid170310060
25. Matveychuk A, Fuks L, Priess R, et al. Clinical and radiological features of mycobacterium kansasii and other NTM infections. Respir Med. 2012;106(10):1472–1477. doi:10.1016/j.rmed.2012.06.023
26. Lee MR, Sheng WH, Hung CC, et al. Mycobacterium abscessus complex infections in humans. Emerg Infect Dis. 2015;21(9):1638–1646. doi:10.3201/2109.141634
27. Gopinath K, Singh S. Non-tuberculous mycobacteria in TB-endemic countries: are we neglecting the danger? PLoS Negl Trop Dis. 2010;4(4):e615. doi:10.1371/journal.pntd.0000615
28. Griffith DE, Aksamit TR. Bronchiectasis and nontuberculous mycobacterial disease. Clin Chest Med. 2012;33(2):283–295. doi:10.1016/j.ccm.2012.02.002
29. Johnson MM, Odell JA. Nontuberculous mycobacterial pulmonary infections. J Thorac Dis. 2014;6(3):210–220. doi:10.3978/j.issn.2072-1439.2013.12.24
30. Jhun BW, Moon SM, Jeon K, et al. Prognostic factors associated with long-term mortality in 1445 patients with nontuberculous mycobacterial pulmonary disease: a 15-year follow-up study. Eur Respir J. 2020;55(1):1900798. doi:10.1183/13993003.00798-2019
31. Pathak K, Hart S, Lande L. Nontuberculous mycobacteria lung disease (NTM-LD): current recommendations on diagnosis, treatment, and patient management. Int J Gen Med. 2022;15:7619–7629. doi:10.2147/IJGM.S272690
32. Polverosi R, Guarise A, Balestro E, et al. High-resolution CT of nontuberculous mycobacteria pulmonary infection in immunocompetent, non-HIV-positive patients. Radiol Med. 2010;115(2):191–204. doi:10.1007/s11547-009-0479-2
33. Ying C, Li X, Lv S, et al. T-SPOT with CT image analysis based on deep learning for early differential diagnosis of nontuberculous mycobacteria pulmonary disease and pulmonary tuberculosis. Int J Infect Dis. 2022;125:42–50. doi:10.1016/j.ijid.2022.09.031
34. Feng Y, Guo J, Luo S, et al. A case-control study on the risk factors associated with the occurrence of non-tuberculous mycobacteria pulmonary disease in bronchiectasis patients. BMC Pulm Med. 2023;23(1):451. doi:10.1186/s12890-023-02768-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.