")
Back to Journals » Clinical Ophthalmology » Volume 18
Population Prevalence, Pattern and Associated Factors for Retinal Diseases at High Altitude in Nepal
Authors Thapa R, Ruit S , Poudel MP, Neupane P, Banjara P, Duwal S, Gurung E, Tabin G
Received 2 May 2024
Accepted for publication 11 July 2024
Published 6 September 2024 Volume 2024:18 Pages 2555—2565
DOI https://doi.org/10.2147/OPTH.S457153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Raba Thapa,1 Sanduk Ruit,2 Manish Prasad Poudel,3 Pratibha Neupane,3 Pradeep Banjara,3 Sushma Duwal,4 Elena Gurung,4 Geoffrey Tabin5
1Department of Vitreo-Retina and Research, Tilganga Institute of Ophthalmology, Kathmandu, Nepal; 2Department of Cataract and Cornea, Tilganga Institute of Ophthalmology, Kathmandu, Nepal; 3Department of Research, Tilganga Institute of Ophthalmology, Kathmandu, Nepal; 4Department of Vitreo-Retina, Tilganga Institute of Ophthalmology, Kathmandu, Nepal; 5Department of Cornea, Byers Eye Institute, Stanford University, Palo Alto, CA, USA
Correspondence: Raba Thapa, Department of vitreo-retina and Research, Tilganga Institute of Ophthalmology, Kathmandu, Nepal, Email [email protected]
Background: Retinal diseases are common at high altitudes due to a cascade of changes caused by hypoxia. The aim of this study is to assess the population prevalence, pattern and associated factors of retinal disorders at high altitude in Nepal.
Methodology: A cross-sectional study was conducted at three selected high-altitude districts (over 2500 meters) of Nepal. Subjects were at least 40 years old, and the target sample size was 309. A detailed history was taken. Visual acuity, blood sugar, blood pressure, and oxygen saturation were measured. Anterior and posterior ocular evaluations were conducted by retina specialists using slit lamp and indirect ophthalmoscopy.
Results: A total of 338 participants were recruited, with nearly equal numbers from the three districts with mean age of 57.0 (S.D 11.1) years. Two-thirds (63.9%) were females; 38.2% were illiterate, and 46.7% were farmers. Average blood oxygen saturation was 87.2% (S.D 4.1%). Systemic hypertension and diabetes mellitus were found in 58% and 11%, respectively. Retinal diseases were found in 176 (52.5%), with bilateral involvement in 157 (46.9%). The major retinal diseases were hypertensive retinopathy (32.2%), high-altitude retinopathy (10.4%), age-related macular degeneration (AMD) (8.1%), branch vein occlusion (BRVO) (2.1%), and diabetic retinopathy (DR) (1.8%). The multivariate analysis showed significant association of retinal diseases with age and hypertension. Best corrected visual acuity better than 6/18 was present in 96.7%.
Conclusion: Over half of the study participants had retinal diseases, with hypertensive retinopathy, AMD, and high-altitude retinopathy as the most common retinal problems. A significant association of retinal diseases was found with ageing, and hypertension. Access to eye care services and control of systemic hypertension along with patient education should be emphasized among people living at high-altitude.
Keywords: prevalence, pattern, risk factors, high-altitude retinopathy, Nepal
Introduction
Retinal disorders are the leading cause of blindness in Nepal.1,2 A study from Nepal reported a prevalence of retinal disorders in one or both eyes among 52% of the study participants age 60 years and above, which increased with ageing.2 Retinal problems were found in 56.8% in a study conducted at high altitude in individuals 40 years and above among participants at an eye camp.3
Low level of oxygen and pressure of high altitude (HA) cause various physiological and psychological dysfunctions in the body leading to many systemic disorders. Total cholesterol and triglycerides were found to be elevated at high altitude mainly because of the residential settings and associated lifestyle practices.4 This could also be a reason for the high prevalence of retinal disorders at high altitude.4
Retinal problems are a major feature of high-altitude sickness (HAS). High-altitude retinopathy (HAR) is characterized by engorgement of retinal veins with occasional papilledema, cotton wool spots, vitreous haemorrhage, and retinal haemorrhages.5 The major pathogenic factor underlying HAR is thought to be hypoxia at high altitude, which leads to various changes in the retinal blood vessels.5,6
Several studies and case series have reported retinal and neurological problems after HA exposure.7–15 Timely precautions and treatment could save from many HA-related ocular and systemic conditions.10 In Nepal, 15% of the land is highly mountainous. Almost 7% of the national population live in mountains, and many people live in the hilly districts at altitudes greater than 2500 meters.4 Due to difficult geographical terrain, transportation and eye care services are limited. As there are limited population-based studies on retinal problems, this study explores the prevalence, pattern, and associated factors for retinal diseases among populations residing at high altitudes in Nepal. These findings will help intervention programs to reduce blindness in remote regions.
Materials and Methods
Ethical approval was taken from Ethical Review Board of Nepal Health Research Council (NHRC) to conduct the study (Protocol Registration Number 199/2023; Reference number 3058). The study approval of NHRC was taken as per the rule of Government of Nepal. The study was conducted as per the declaration of Helsinki. The study design was a population-based, cross-sectional study conducted at high altitude in three districts of Nepal: the Manang, Mustang, and Solukhumbu districts. These districts were selected based on the availability of eye examination facilities at community eye centers and general hospitals. An altitude of over 2500 meter was taken as demarcation for high altitude where people generally experience adverse symptoms above this altitude.4 A list of municipalities and wards of the three study districts was prepared, and one municipality from each district was selected using simple random sampling. Based on the proportion of the population, wards were selected from each municipality. From these districts, the local study sites selected randomly were Chame Rural Municipality from Manang, Lo-Ghekar Damodarkunda Rural municipality from Upper Mustang and Khumbu Pasanglhamu rural municipality from Solukhumbu. In these areas, there are community eye centers with facilities for eye evaluations. Similarly, in Lukla Solukhumbu, there is an eye care facility with available ophthalmic equipment in a general hospital.
Subjects age 40 years and older residing in Chame Rural Municipality from Manang, Lo-Ghekar Damodarkunda Rural municipality from Upper Mustang and Khumbu Pasanglhamu rural municipality from Solukhumbu were enrolled in the study. Assuming retinal problem prevalence (P) 56.8%, 95% confidence and 10% tolerable error, the sample size was 293. With assuming 5% non-response rate, the target sample for the study was 309, with a minimum sample of 103 for each district.
The exclusion criteria were participants whose retinal evaluation was not possible due to various causes such as media opacity or participants who were unable to comply with the history, examination, and investigation protocols of the study.
All study participants were from the geographical areas above 2500 meters. Informed written consent was taken before enrollment in the study. Demographic information, history of alcohol, smoking, systemic history, non-fasting blood sugar levels, height, weight, and blood pressure (BP) were measured using a questionnaire designed and finalized by the study team and experts. Body Mass Index (BMI) was calculated as weight in kilogram divided by height in meter square from the collected weight and height data.
In case of mountain climbers, details of average of height climbed and frequency in a year were recorded. Awareness of major eye diseases like DR, AMD, hypertensive retinopathy, and high-altitude retinal diseases was assessed.
Presenting and best corrected visual acuity was taken using a Snellen’s chart. The anterior and posterior segments ocular evaluations were conducted using a slit lamp and an indirect ophthalmoscope both using 90 D lens and 20 D lens after mydriasis. Fundus photographs of each participant were captured using a portable fundus camera (Nidek Versacam DS-20) under mydriasis by a trained ophthalmic technician. Three fellowship trained retina specialists were involved for eye evaluation of all study participants at each site. The discussion was done to ensure accurate diagnosis whenever needed.
Diabetes mellitus was diagnosed if using oral hypoglycaemic agents or use of insulin or a random blood sugar level of 200 mg/dl or greater.1,2,16 Hypertension was diagnosed if participant has systolic BP 140 mmHg or more, or if diastolic BP 90 mmHg or more, or if they are using oral antihypertensive medicines.1,2 Early Treatment Diabetic Retinopathy Study (ETDRS) criteria were used to diagnose various grades of diabetic retinopathy (DR) and macular edema.17 Classification of AMD as early and late AMD, further subdivided as wet and dry types, was based on the International Age-related Maculopathy (ARM) Epidemiological Study Group.18 Modified Scheie Classification was used to grade hypertensive retinopathy from grade 0 to grade 4.20 Presence of any retinal disease in one eye or both eyes were considered to diagnose retinal disease in person. Oxygen saturation was assessed using pulse oximetry among all the study participants. The World Health Organization (WHO) (WHO) criteria were used for grading of blindness and low vision.1,2,19
Data Analysis
Data collection was done using electronic software (Open Data kit) and transferred to Microsoft Excel for cleaning and coding. Statistical Package for the Social Science (SPSS) V20 was used for statistical analysis. The mean, percentage, tables, and figures were prepared for descriptive analysis. For association of categorical data, Chi square test was used, and if the expected cell count was less than 5, Fisher's exact test was used. For the comparison of numerical data, independent t test was used. All the statistically significant variables found during bivariate analysis were used for multiple logistic regression using Enter method to quantify the outcome. Results were considered statistically significant if the P-value was less than 0.05. The data collected are stored in password-protected computer, ensuring the confidentiality of patients’ data.
Results
Total 338 participants were enrolled from three districts. Among them, 109 (32.3%) were from Manang district, 110 (32.5%) were from Mustang district and 119 (35.2%) were from Solukhumbu district. The mean age of all participants was 57.0 years (S.D 11.1 years), whereas the mean age for Solukhumbu was 58.3 years (S.D 11.5 years), Mustang 58.6 years (S.D 10.0 years), and Manang 54.0 years (SD 11.2 years).
The average oxygen saturation level among participants was 87.2% (S.D 4.1%), range 72% to 96%. The mean highest saturation oxygen level was in the Solukhumbu district (87.9%), while it was the lowest in the Mustang district (85.2%).
Three study participants were excluded from the retinal disease analysis because retinal evaluation was not possible in one eye due to hazy media, and fellow eye was normal. One eye of each three cases had thick posterior capsular opacification with corneal scar, mature cataract, and mature cataract with corneal scar, respectively.
Demographic Characteristics
Among the total study participants, 216 (63.9%) were females. This trend of female predominance was similar in all three districts. Three-fifth of the study participants (60%) were between 40 and 60 years of age. Patients 70+ years comprised 16.6%. A total of 129 participants (38.2%) were illiterate, which was highest in Solukhumbu (58%). A total of 158 (46.7%) were farmers, followed by business people 69 (20.4%). By religion, the majority 296 (87.6%) were Buddhists (Table 1).
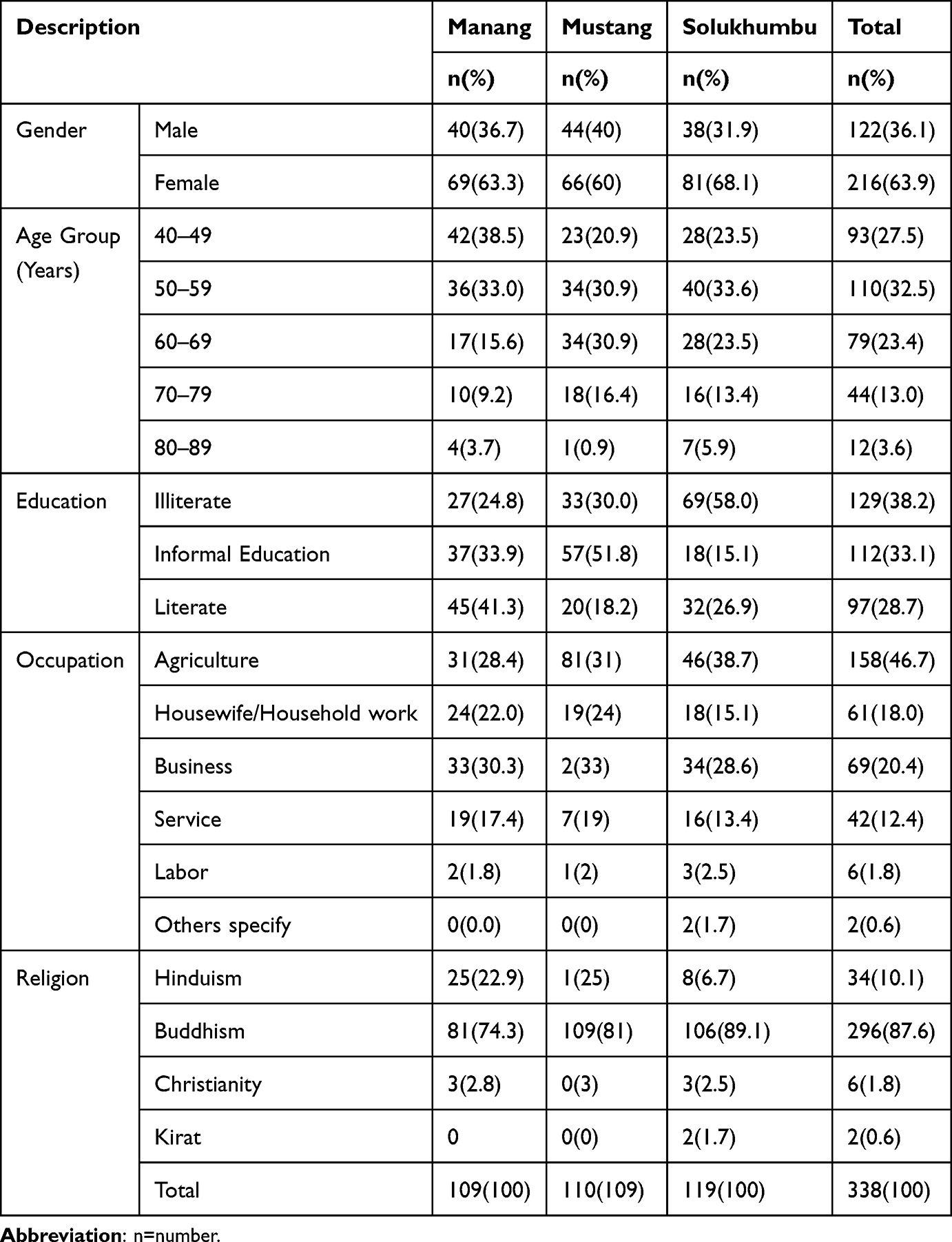 |
Table 1 Demographic Characteristics of Study Population |
Prevalence of Retinal Diseases, Systemic Hypertension, and Diabetes Mellitus in Three Study Sites
Among the study participants, retinal diseases were present in 176 (52.5%). The highest prevalence of retinal diseases was found in Mustang district 72 (66.1%), followed by Solukhumbu district 63 (53.8%) and Manang district 41 (37.6%). Bilateral involvement of retinal diseases was found in 157 (46.9%) and unilateral involvement in 19 (5.7%).
Among the total study participants, systemic hypertension was found in 58.0%, out of which over one-fifth of total (28.1%) were newly diagnosed during the study. The highest proportions were found in Solukhumbu and lowest in Mustang.
A total of 37 (11.0%) of study participants were diagnosed with diabetes mellitus. Among these, 9 (2.7%) were newly diagnosed during the study. The mean blood sugar level was 100.2 mg/dl (S.D 30.8) (Table 2).
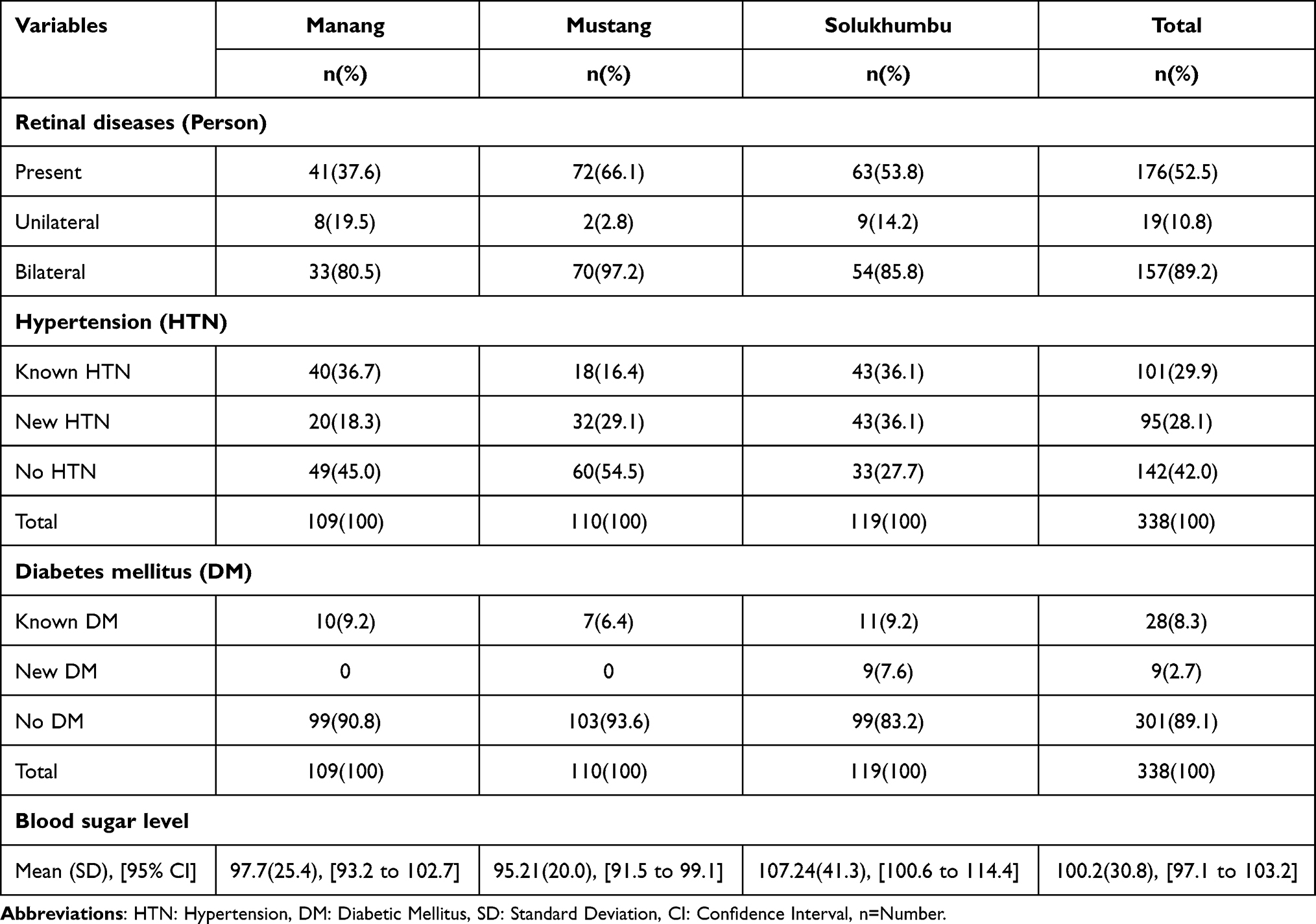 |
Table 2 Prevalence of Retinal Diseases, Hypertension and Diabetes Mellitus Among Study Population at Three Study Sites |
Pattern of Retinal Diseases
Among the various retinal diseases, hypertensive retinopathy was highest at 32.2%, followed by high altitude retinopathy at 10.7%, AMD at 8.1% and retinal vein occlusion at (2.1%) (Table 3).
 |
Table 3 Pattern of Various Retinal Diseases Among the Study Population |
Classification of Hypertensive Retinopathy, Diabetic Retinopathy, and AMD
Among the cases of hypertensive retinopathy, four-fifth eyes (81.9%) were having grade one and 2.8% were having grade three hypertensive retinopathy. Nearly one-third of eyes had mild non-proliferative diabetic retinopathy (NPDR), and proliferative DR with macular edema comprised one-tenth of the eyes. Wet AMD comprised 8.7% of eyes, and geographic atrophy was found in 2.4%. Majority were having mild and intermediate dry AMD (97.5%) among the eyes having dry AMD (Table 4).
 |
Table 4 Classification of Hypertensive Retinopathy, Diabetic Retinopathy, and AMD (Eyes) |
Factors Associated with Retinal Diseases Among the Study Participants (Univariate Analysis)
Among the various factors in univariate analysis, there was significant association of retinal diseases with increase in ageing (p=<0.001), smoking use (p=0.047), alcohol consumption (p=<0.001), presence of systemic hypertension (p=<0.001), and low partial pressure of oxygen (p=0.004). However, there was no significant association with education, gender, religion, diabetes mellitus, visual acuity, or with a history of trekking or blood sugar levels (Table 5).
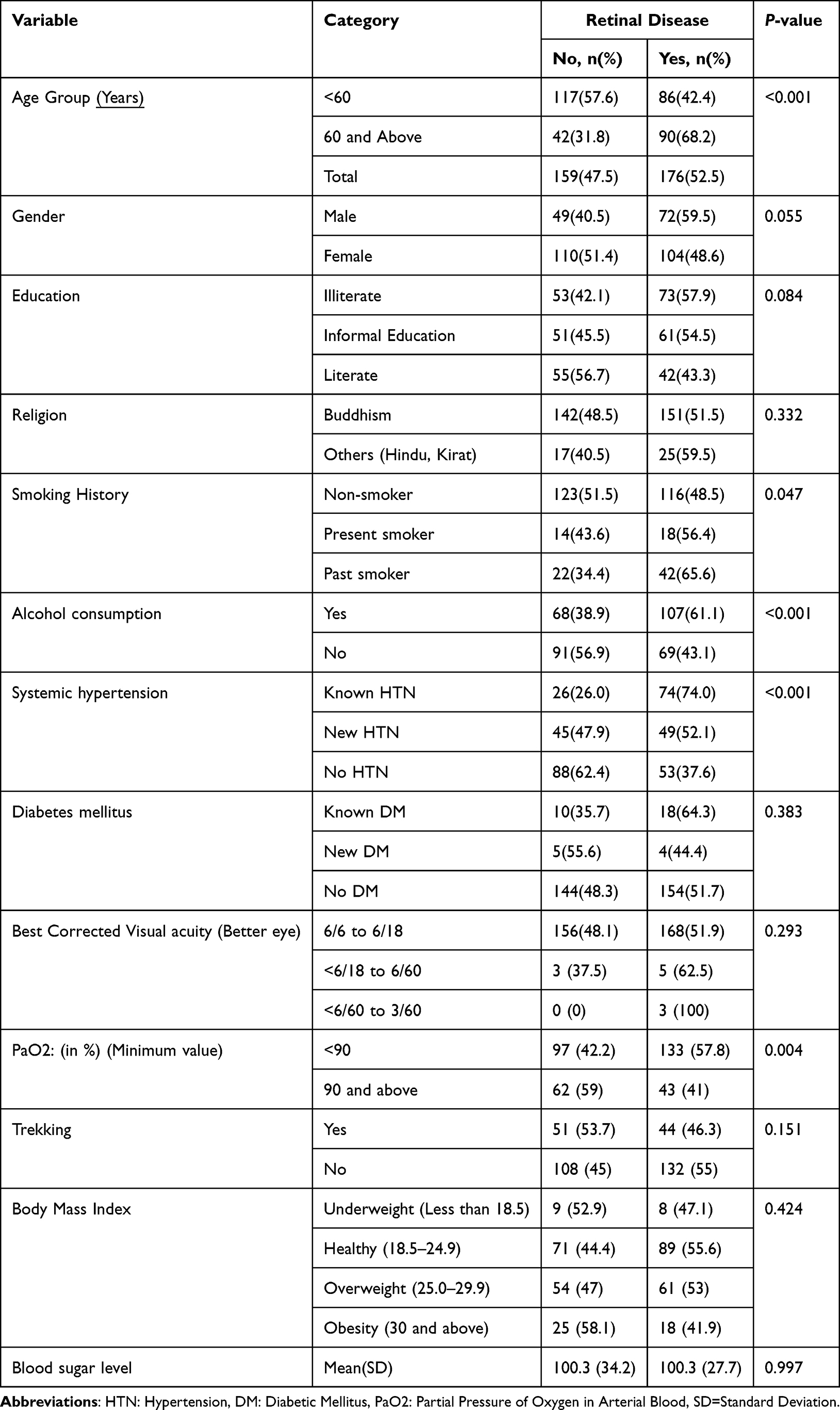 |
Table 5 Factors Associated with Retinal Diseases Among the Study Participants (Univariate Analysis) |
Multiple logistic regressions were carried out to quantify the retinal diseases with statistically significant variables. Age group and hypertension were found to be statistically significant variables in multiple logistic regressions. Age 60 years and above had a 2.19-fold increase in risk of having retinal diseases as compared to those less than 60 years of age. Patients having a known history of hypertension had 5.4-fold increased risk, and new hypertension had 1.8-fold increased risk of retinal disease (Table 6).
 |
Table 6 Factors Associated with Retinal Diseases in Multivariate Analysis |
Visual Status Among the Study Participants
A presenting visual acuity and best corrected visual acuity of 6/6 to 6/18 in the better eye among the study participants were found in 89.1% and 96.7%, respectively. The visual acuity status was almost similar in all three districts. As per the WHO criteria, none of the cases were blind and 3.9% had low vision.
Discussion
Posterior segment problems are an important cause of visual impairment in Nepal.1,2,19 High altitude retinopathy is specific to people residing in high altitude regions or climbing high mountains.3,6–9
Over half (52.5%) of study participants were diagnosed with retinal disease. The highest prevalence was in Mustang (66.1%), then Solukhumbu (53.8%), then Manang (37.6%). About 47% of participants had bilateral retinal disease and 5.7% had unilateral disease. Retinal diseases in this study were consistent with other high altitude studies of retinal disease in Nepal, despite the fact that this study was not conducted on a population presenting to an eye camp, which would be expected to contain a greater proportion of individuals with retinal pathology. This emphasizes the need for regular eye check-ups in these geographically remote areas. The Mustang site was the highest altitude site and also had the highest prevalence of retinal disease (66%). An increase in altitude could be the possible cause for high prevalence of retinal diseases.6
The retinal disease prevalence was quite higher as compared to the population-based study conducted in low land population in the same age group.1,2
There were more participants diagnosed with hypertension (58%) in our study compared to the prior high-altitude study in Nepal (28%).3 This could be due to uncontrolled blood pressure and longer duration of hypertension at high altitude. This could be the reason for more hypertensive retinopathy cases in our study.
High altitude retinopathy was found in 10.4% of study participants in our series, but all participants were found to have dilated and tortuous vessels. In a previous study, dilated and tortuous vessels were found in 25.9% of study participants, due to hypoxia. In our series, the average SpO2 among study participants was 87.2% (S.D 4.1%), with a range of 72% to 96%. About 68.8% of patients had a SpO2 less than 90%. The low SpO2 in the majority of the study participants could be the reason for the high number of cases of high altitude retinopathy. Dilated and tortuous vessels have been reported as high altitude retinopathy in other studies.3,12
Among the hypertensive retinopathy, grade one hypertensive retinopathy was found in highest number, consistent with other studies.21 The predominant dry mild AMD and NPDR were also consistent with other studies from low land and previous study conducted at high altitude.2,3
In our study, age and systemic hypertension were significantly associated with retinal disease. This is consistent with other studies of retinal disease, including those conducted at both high altitude and low land populations.1–3,22,23
The best-corrected visual acuity of the vast majority of patients was very good despite the high prevalence of retinal diseases at high-altitude. Not a single participant met the WHO criteria for blindness. This suggests that refractive error services like provision of spectacles could adequately address most cases of decreased vision in this population to improve the quality of life. Regular check-ups, especially for older individuals and those with diagnosis of hypertension and diabetes, are important.2,22
The limitation of our study is that, although the study population was all enrolled from sites over 2500 meters, all three sites were not at the exact same elevation. This could affect the prevalence of retinal diseases in three different districts.
Conclusion
Over half of the study participants had some form of retinal diseases. Hypertensive retinopathy was the most common disorder followed by AMD, then high altitude retinopathy. Retinal diseases were significantly associated with age and systemic hypertension. The findings emphasize the need for enhanced access to eye care services, good control of hypertension and education on major blinding retinal diseases at high altitude in Nepal.
Abbreviations
HA High Altitude; HAS, High-Altitude Sickness; HAR, High-Altitude Retinopathy; DR, Diabetic Retinopathy; ETDRS, Early Treatment Diabetic Retinopathy Study; AMD, Age-Related Macular Degeneration; DM, Diabetes Mellitus; RVO, Retinal Vein Occlusion; BRVO, Branch Retinal Vein Occlusion.
Data Sharing Statement
Data related to the study are all provided in the manuscript. The corresponding author will be responsible for sharing further details as needed.
Ethics Approval and Informed Consent
Study was conducted after the approval of the study by the Ethical Review Board of Nepal Health Research Council (NHRC) (Registration Number 199/2023; Reference number 3058). The study approval of NHRC was taken as per the rule of Government of Nepal. The study was conducted as per the declaration of Helsinki.
Written informed consent was obtained from the study participants after detailed information about the study before enrollment.
Consent for Publication
There is consent for publication from all the investigators.
Acknowledgment
We would like to acknowledge Association of Research in Vision and Ophthalmology (ARVO) Foundation for providing the financial support to conduct the study as part of Collaborative Research Fellowship Award.
We would like to acknowledge Byers Eye Institute, Stanford University, California, USA, for the support of this study as part of the mentorship program for the Collaborative Research Fellowship Award.
We would like to acknowledge Professor Dr Paul S. Bernstein, Moran Eye Center, University of Utah, USA, and Dr Sean Collon from Byers Eye Institute, Stanford University, California, USA, for edits in English language.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
1. Association of Research in Vision and Ophthalmology (ARVO) Foundation, USA 2. Byers Eye Institute, Stanford University, California, USA.
Disclosure
The authors declare that none of them had any competing interests in the study.
References
1. Thapa SS, Thapa R, Paudyal I, et al. Prevalence and pattern of Vitreo-retinal disorders in Nepal: the Bhaktapur glaucoma study. BMC Ophthalmo. 2013;13:9. doi:10.1186/1471-2415-13-9
2. Thapa R, Khanal S, Tan HS, Thapa SS, van Rens GHMB. Prevalence, pattern and risk factors of retinal diseases among an elderly population in Nepal: The Bhaktapur Retina Study. Clin Ophthalmol. 2020;14:2109–2118. PMCID:PMC: 7399464. PMID:32801619. doi:10.2147/OPTH.S262131
3. Thapa R, Paudyal G, Crandall A, Tabin G. Vitreo-retinal disorders at high altitude in Nepal. Nepalese J Ophthal. 2013;5(8):57–62. PMID: 23584648. doi:10.3126/nepjoph.v5i1.7823
4. Aryal N, Weatherall M, Bhatta YKD, Mann S. Lipid profiles, glycated hemoglobin, and diabetes in people living at high altitude in Nepal. Int J Environ Res Public Health. 2017;14(9):1041. doi:10.3390/ijerph14091041
5. Wieldman M, Tabin GC. High altitude retinopathy and altitude illness. Ophthalmology. 1999;106:1924–1927. doi:10.1016/S0161-6420(99)90402-5
6. Morris DS, Somner J, Michael JD, et al. The Eye at Altitude. Hypoxi Exerci. 2007;249–270.
7. Rennie D, Morrossey J. Retinal changes in Himalayan climbers. Arch Ophthalmol. 1975;93:395–400. doi:10.1001/archopht.1975.01010020409001
8. Karki P, Sijapati MJ, Pandey M, Khadka N. Ocular presentations in high altitude sickness: experience of our centre. Nep Med J. 2019;2(1):141. doi:10.3126/nmj.v2i1.23996
9. Mashkovskiy E, Szawarski P, Ryzhkov P, Goslar T, Mrak I. Fulminant high altitude blindness. J Travel Medi. 2016;1–4.
10. Izadi M, Pourazizi M, Alemzadeh-Ansari M. Ocular problems in high-altitude traveling: a review with focus on management. Int J Travel Med Glob Health. 2017;5(2):41–45. doi:10.15171/ijtmgh.2017.09
11. Wiedman M. High altitude retinal hemorrhage. Arch Ophthalmol. 1975;93:401–403. doi:10.1001/archopht.1975.01010020415002
12. Karakucuk S, Mirza GE. Ophthalmological effects of high altitude. Ophthalmic Res. 2000;32:30–40. doi:10.1159/000055584
13. Houston CS. High altitude illness. Disease with protean manifestations. J Am Med Assoc. 1976;236:2193–2195. doi:10.1001/jama.1976.03270200031025
14. Mills J, Luce JM. Incidence of acute mountain sickness at intermediate altitude. J Am Med Associ. 261(5):732–734.
15. Bosch MM, Barthelmes D, Merz TM, et al. High incidence of optic disc swelling at very high altitudes. Arch Ophthalmol. 2008;26(644):50.
16. World Health Organization. Report of World Health Organization/international diabetes federation consultation: Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia. World Health Organ. 2006;1–50.
17. Early Treatment Diabetic Retinopathy Study Research Group. Early photocoagulation for diabetic retinopathy: ETDRS report 9. Ophthalmology. 1981;98:766–785.
18. Bird AC, Bressler NM, Bressler SB. International ARM epidemiological study group. An international classification and grading system for age-related maculopathy and age-related macular degeneration. Surv Ophthalmol. 1995;39:367–374. doi:10.1016/S0039-6257(05)
19. Thapa R, Bajimaya S, Paudyal G, Khanal S, Tan S, Thapa SS. Prevalence and causes of low vision and blindness in an elderly population in Nepal: the Bhaktapur Retina Study. BMC Ophthalmo. 2018;13(1):42. PMID: 29439666.. doi:10.1186/s12886-018-0710-9
20. Scheie HG. Evaluation of ophthalmoscopic changes of hypertension and arteriolar sclerosis. America Med Associa Arch Ophtha. 1953;49(2):117–138. doi:10.1001/archopht.1953.00920020122001
21. Thapa R, Khanal S, Tan H, Thapa S, vanRens GHMB. Prevalence associated factors and awareness of hypertensive retinopathy among an elderly population with hypertension in Nepal: The Bhaktapur retina study. Nepal J Ophthalmol. 2022;14(27):49–58. doi:10.3126/nepjoph.v14i1.35401
22. Thapa R, Bajimaya S, Paudyal G, et al. Prevalence, pattern and risk factors of retinal vein occlusion in an elderly population in Nepal: The Bhaktapur Retina Study. BMC Ophthalmo. 2017;17:162. PMID: 28865424. doi:10.1186/s12886-017-0552-x
23. Nirmalan PK, Katz J, Robin A, et al. Prevalence of vitreoretinal disorders in a rural population of southern India. Arch Ophthalmol. 2004;122:581–586. doi:10.1001/archopht.122.4.581
 © 2024 Nepal Eye Program. This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 Nepal Eye Program. This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.